
Abstract
Meningiomas are dural-based neoplasms derived from meningothelial (arachnoid) cells; they include a wide variety of histologic subtypes, ranging from benign WHO grade I variants to more biologically aggressive meningiomas encompassing WHO grades II and III.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Meningioma
- Atypical meningioma
- Anaplastic meningioma
- Rhabdoid meningioma
- Papillary meningioma
- Chordoid meningioma
- Clear cell meningioma
- Neurofibromatosis type 2
1 Overview
-
Meningiomas are dural-based neoplasms derived from meningothelial (arachnoid) cells; they include a wide variety of histologic subtypes, ranging from benign WHO grade I variants to more biologically aggressive meningiomas encompassing WHO grades II and III.
-
Many pediatric meningiomas are sporadic, but a significant proportion arise in the context of a hereditary cancer predisposition syndrome, especially neurofibromatosis type 2 (NF2).
-
◦Multiplicity of meningiomas is not uncommon in NF2, and the pediatric onset of meningioma should prompt further evaluation for clinical and genetic findings diagnostic of NF2.
-
◦ Meningiomas are infrequently encountered with Gorlin syndrome. Recently, germline mutations involving SWI/SNF chromatic remodeling complex have been implicated in meningiomas. SMARCE1 mutations have been identified as a cause of clear cell meningiomas (both intracranial and spinal), and about 5 % of patients with schwannomatosis (due to SMARCB1 mutations) will also develop meningiomas.
-
-
Exposure to radiotherapy for prior neoplasm is another significant predisposing factor in the development of meningiomas, particularly within the pediatric age group.
2 Clinical Features
-
Though meningiomas are quite common in adults, they infrequently arise in the pediatric population, acco unting for less than 3 % of all intracranial tumors in that age group.
-
Pediatric meningiomas are more common in males, in contrast to the female predominance encountered in adults.
-
Specific manifestations depend on the tumor site and compression of adjacent structures. Signs and symptoms related to chronically elevated intracranial pressure (headaches, vomiting, papilledema), cranial nerve disorders and other focal neurologic deficits, and seizures have been reported in these children. Spinal meningiomas may present with pain, limb weakness and/or paresthesia, or gait disturbance, and are frequently associated with NF2.
3 Neuroimaging
-
In children, meningiomas most frequently arise at intracranial locations, including over the cerebral convexities, in parasagittal or parasellar regions, or at the cerebellopontine angle (Fig. 10.1). Intraventricular and intraparenchymal meningiomas are more frequent in the pediatric age group.
Fig. 10.1 
T1-weighted post-gadolinium (post-Gd) axial (A) and coronal (B) MR images showing homogeneously enhancing pediatric meningiomas arising over the cerebral convexities and within the cerebellopontine angle, respectively. Note the characteristic “dural tail” in both images
-
Pediatric skull base meningiomas tend to be smaller at presentation, but are less likely to undergo complete resection.
-
Spinal meningiomas in children are most frequent at cervical or thoracic levels.
-
By MR imaging, most meningiomas are isointense to hypointense to gray matter on T1, hyperintense on T2 and FLAIR, and are accentuated strongly after contrast administration (Fig. 10.2A–E). The characteristic “dural tail” may be seen in over 50 % of cases. Over 20 % may have a large cystic component.
Fig. 10.2 
This 8-year-old boy had a quite large parasagittal multilobulated, dural-based mass with solid and cystic components in the right posterior parietal lobe. The solid component showed heterogeneous signal intensity, being isointense to hypointense to cortex on T1-weighted MR imaging (A) and hyperintense on T2-weighted MRI (B) and FLAIR (C); it showed heterogeneous enhancement on T1-weighted post-Gd axial MR images (D). Note the accompanying peritumoral edema and midline shift, seen best in B and C. A sagittal T1-weighted post-Gd image (E) shows thickening (hyperostosis) of the overlying calvarial bone and scalp edema. Angiography (F) shows prominent tumor blush, with feeding vasculature arising from the right middle meningeal artery
-
Surrounding vasogenic edema frequently accompanies meningiomas, and is generally proportionate to tumor size (Fig. 10.2B and C); angiomatous, microcystic, or higher-grade variants may have disproportionate edema relative to their size. Intratumoral calcifications, hemorrhage, or necrosis are uncommon findings.
-
Invasion of adjacent cranial bone may cause hyperostosis, readily identifiable on imaging studies (Fig. 10.2E).
-
Angiography (typically performed when embolization is planned) shows a hypervascular tumor blush throughout the arterial phase of the middle meningeal artery injection, persisting into the late venous phase with slow washout (Fig. 10.2F).
-
Tumor seeding along the surgical trajectory, through CSF dissemination, or by metastases outside the CNS is encountered rarely; though more frequent with higher-grade tumors, histologically benign meningiomas have exhibited such behaviors.


4 Pathology
-
Gross pathology
-
◦ Meningiomas are gene rally round or lobulated tan-yellow, firm masses (Fig. 10.3), frequently with dural attachment. Some tumors (usually skull-base lesions) grow in a flat “en plaque” pattern. A granular appearance may indicate psammoma bodies.
Fig. 10.3 
Typical macroscopic appearance of meningioma, arising from the dura as a well-circumscribed, firm mass
-
◦ Encasement of adjacent nerves or blood vessels, or invasion into bone or soft tissue, may be encountered.
-
◦ WHO grade II and III meningiomas are usually larger and may contain areas of necrosis.
-
-
Intraoperative cytologic imprints or smears
-
◦ Cytologic smears or squa sh preparations show cohesive, syncytial clusters of cells with oval to round nuclei (Fig. 10.4A).
Fig. 10.4 
Helpful cytologic features that may be encountered on crush/squash preparations of meningioma inc lude the findings of cohesive syncytial clusters (A), whorls (B), and psammoma bodies (C). Careful inspection often reveals intranuclear cytoplasmic invaginations or pseudoinclusions, as seen here centrally (D). Similar findings are demonstrable on both conventional H&E (A–D) and Diff-Quik stained preparations (E, F)
-
◦ Classic “whorl” formations, intranuclear cytoplasmic invaginations, and psammoma bodies are other helpful diagnostic features (Fig. 10.4B–F).
-
◦ Unfortunately, cytologic preparations from several meningioma variants may pose a significant diagnostic challenge. For instance, the fibrous variant (Fig. 10.5A) with its elongated spindle cells, may mimic glioma, whereas the papillary variant (Fig. 10.5B) may be confused with carcinoma, and the rhabdoid variant (Fig. 10.5C) may be confused with atypical teratoid/rhabdoid tumor (AT/RT). Nuclear anaplasia, macronucleoli, mitoses, and shee ting suggest a higher-grade lesion.
Fig. 10.5 
(A) Squash preparation of a fibr ous meningioma, showing elongated, spindled cells. (B) Papillary structures with multilayered covering of epithelioid cells may be seen in cytologic preparations of papillary meningioma. (C) Squash preparation of rhabdoid meningioma, containing discohesive cells with eccentrically situated nuclei and eosinophilic cytoplasmic “bellies,” may be reminiscent of atypical teratoid/rhabdoid tumor (AT/RT)
-
-
Histology
-
◦ Numerous meningioma histologic variants have been recognized. In general, WHO grade I meningiomas carry a low risk of recurrence and behave in a benign fashion, whereas WHO grade II and III tumors carry an incrementally higher likelihood of recurrence and aggressive behavior.
-
◦ The higher-grade variants are notably more frequent in the pediatric population.
-
Note that pleomorphi c nuclei may be encountered in any of the meningioma variants, most often connoting a degenerative atypia as opposed to higher tumor grade.
-
-
◦ WHO grade I variants
-
Meningothelial meningioma
-
Common variant with lobular architecture; these lobules contain syncytial arrays of cells with uniform, oval nuclei, often with intranuclear-cytoplasmic inclusions. Whorls and psammoma bodies are infrequent (Fig. 10.6A and B).
Fig. 10.6 

Common WHO grade I variants. The meningothelial variant of meningioma is multilobular (A), containing syncytial arrays of cells with imperceptible cell borders and uniform oval nuclei, often containing intranuclear-cytoplasmic inclusions (B). Whorls are uncommon and poorly formed, and psammoma bodies are uncommon. Fibrous meningioma contains interwoven broad fascicles of bland spindle cells (C), often with multiple clear clefts amongst the fascicles (D); collagen content is variable. Transitional meningioma shows features of both the fibrous and meningothelial variants (E), typically containing numerous tight whorl formations (F) and numerous psammoma bodies (G). Striking nuclear pleomorphism may be encountered in any meningioma (H), though in the absence of other histologic features indicative of grade II or III designation, these should be viewed as degenerative in nature
-
-
Fibrous meningioma
-
These contain spindle cells arranged in parallel fascicles with an interwoven collagen matrix, which on occasion may be quite dense.
-
Focal intranuclear cytoplasmic inclusions and psammoma bodies may be seen (Fig. 10.6C and D).
-
-
Transitional (mixed) meningioma
-
By far the most recogniza ble variant, transitional meningiomas display a mixture of both meningothelial and fibrous patterns with numerous whorls and psammoma bodies (Fig. 10.6E–H).
-
-
-
WHO grade I variants uncommon in children
-
Psammomatous meningioma
-
These tumors contain more psammoma bodies than meningothelial tumor cells, the former often coalescing to form large calcified areas.
-
Whorl formations are common (Fig. 10.7A).
Fig. 10.7 

Other WHO grade I variants. ( A ) In psammomatous meningioma, psammoma bodies may be so numerous as to make identification of the neoplastic meningothelium difficult. (B) Angiomatous meningioma contains numerous variably sized blood vessels, sometimes hyalinized, with a tendency for nuclear pleomorphism. (C) In addition to the numerous microcystic spaces, easily recognizable meningothelial cells are seen in this microcystic meningioma. (D) Secretory meningiomas contain islands of obvious epithelial differentiation. (E) Periodic acid–Schiff (PAS)–positive pseudopsammoma b odies are also found in secretory meningiomas. (F) Carcinoembryonic antigen (CEA)–positive pseudopsammoma bodies are another finding. (G) Metaplastic changes may also be seen in meningioma, as in this example with metaplastic bone formation
-
-
Angiomatous meningioma
-
Typified by more vascular structures than tumor cells, these tumors harbor abundant small- to medium-caliber, often hyalinized blood vessels of variable wall thickness.
-
Degenerative nuclear atypia may be marked (Fig. 10.7B).
-
-
Microcystic meningioma
-
Contain numerous intercellular microcystic spaces, sometimes containing eosinophilic mucinous secretions.
-
Similar to the angiomatous variant, nuclear pleomorphism may be a prominent feature (Fig. 10.7C).
-
-
Secretory meningioma
-
This variant is marked by the presence of focal epithelial differentiation consisting of intracellular lumens containing eosinophilic, periodic acid–Schiff (PAS)–positive secretions (pseudopsammoma bodies) (Fig. 10.7D and E).
-
These structures are also positive for carcinoembryonic antigen (CEA) (Fig. 10.7F).
-
Mast cells may be conspicuous.
-
-
Lymphoplasmacyte-rich meningioma
-
In this extremely rare variant, extensive chronic inflammatory cell infiltrate typically overshadows the meningothelial cells.
-
-
Metaplastic meningioma
-
These tumors contain mesenchymal components in the form of bone, cartilage, lipid, or myxoid tissues (Fig. 10.7G). Xanthomatous areas also may be present.
-
-
-
◦ WHO grade II variants
-
Atypical meningioma
-
By definition, this is a meningioma with increased mitotic rate (>4/10 hpf in the area of highest mitotic activity) or at least three of the following histologic findings:
-
Hypercellularity
-
Small cell change
-
Prominent nucleoli
-
Sheet-like growth pattern
-
Foci of spontaneous or geographic necrosis (i.e., not induced by therapeutic embolization) (Fig. 10.8A–D)
Fig. 10.8 
Microscopic feature s of atypical meningioma (WHO grade II) may include elevated mitotic rate and/or three or more of the following features: hypercellularity, small cell chan ge (A), prominent nucleoli (B), sheeting architecture (C), and foci of spontaneous necrosis (D). Brain-invasive meningiomas (E) have a rate of recurrence similar to atypical meningioma
-
-
From a prognostic standpoint, m eningiomas that are histologically benign (grade I) but show definite brain invasion should also be considered WHO grade II, as they have been documented as showing recurrence and mortality rates akin to other grade II meningiomas.
-
Brain-invasive m eningiomas will show tongue-like projections of tumor infiltrating into the underlying brain parenchyma (Fig. 10.8E).
-
-
Chordoid meningioma
-
Chordoid meningiomas are composed of cords and trabeculae of e osinophilic cells, sometimes with cytoplasmic vacuolization, within a mucoid or myxoid background closely mimicking chordoma (Fig. 10.9).
Fig. 10.9 
With its distinctive cordlike a rchitecture (A), chordoid meningioma (WHO grade II) superficially resembles chordoma, but closer inspection reveals that it lacks the bubbly, physaliferous cells of that entity (B)
-
Most show mixing of this chordoid pattern with more typical meningioma morphology; pure examples are quite rare.
-
These tend to be large, supratentorial tumors typified by a high rate of recurrence if not completely resected.
-
-
Clear cell meningioma
-
Clear cell meningioma is a rare, aggressive meningioma variant, more common in children, containing cells with abundant clear glycogen-rich (PAS-positive) cytoplasm.
-
Dense “blocky” accumulations of collagen are a frequent finding (Fig. 10.10).
Fig. 10.10 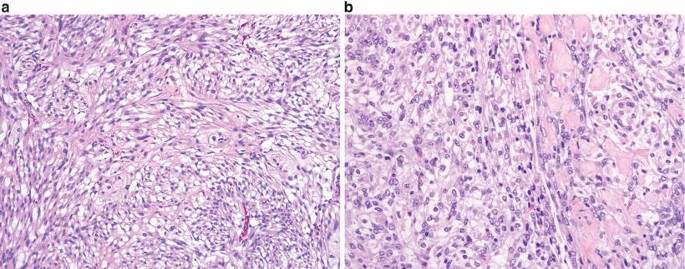
A fascicular architect ure with occasional vague whorls is seen in clear cell meningioma, WHO grade II (A). Dense collagen blocks are a helpful diagnostic clue seen in most cases (B)
-
Psammoma bodies and whorl formations are not typical features.
-
Clear cell meningiomas tend to involve the cerebellopontine angle and spinal or cauda equina region. They frequently recur and may even show CSF dissemination.
-
-
-
◦ WHO grade III variants
-
Anaplastic (malignant) meningioma
-
Anaplastic meningioma contains one or both of these obviously malignant histologic features:
-
Malignant cytol ogy (may resemble carcinoma, sarcoma, or melanoma) (Fig. 10.11A)
Fig. 10.11 
Often barely reco gnizable as meningioma, anaplastic meningioma (WHO grade III) may resemble sarcoma, carcinoma, or melanoma (A) and may have a brisk mitotic index (B)
-
Markedly elevated mitotic index, defined as >20 mitoses/10 hpf (Fig. 10.11B).
-
-
Scattered regions showing at least vaguely recognizable meningioma architecture can be found in most examples, though rarely these lesions prove formidable diagnostic dilemmas necessitating extensive immunohistochemical, ultrastructural, and even molecular workup.
-
Although brain invasion is frequently (though not always) present, this feature alone is not sufficient to warrant a WHO grade III designation. (See note above under “Atypical meningioma”.)
-
-
Papillary meningioma
-
This rare variant, more fre quent in young patients, shows a prominent pseudopapillary pattern (Fig. 10.12A and B)
Fig. 10.12 
(A, B) Papillary meningioma (WHO grade III) contains broad, fibrovascular cores covered by neoplastic meningothelium . A careful search of tissue from these tumors should reveal at least few foci recognizable as meningioma
-
-
Rhabdoid meningioma
-
This uncommon variant, similarly more frequent in children, contains “rhabdoid cells” with eccentrically situated vesicular nuclei that often contain prominent nucleoli, and abundant eosinophilic cytoplasmic “bellies,” many showing obvious globular or whorled inclusions (Fig. 10.13).
Fig. 10.13 
(A, B) Rhabdoid meni ngioma (WHO grade III) characteristically contains discohesive nests of cells with eccentric nuclei, often with vesicular chromatin pattern and prominent nucleoli, in addition to eosinophilic cytoplasmic “bellies.” Areas more r ecognizable as meningioma are usually identifiable elsewhere within these tumors, though this rhabdoid morphology may be the predominant morphology in some cases
-
The cells of this “rhabdoid phenotype” closely mimic those encountered in AT/RT and renal or extrarenal rhabdoid tumors, with definitive differentiation often requiring immunohistochemistry and/or molecular determination of INI1/BAF47 status. (See below for differential diagnosis.)
-
A mixture of rh abdoid cells and papillary/pseudopapillary architecture may be encountered.
-
Rhabdoid meningiomas frequently exhibit a high proliferative index and other aggressive histologic features.
-
-
-













5 Immunohistochemistry
-
Epithelial membrane antigen (EMA) and vimentin are positive in nearly all meningiomas (Fig. 10.14A), but some variants, particularly fibroblastic and higher-grade meningiomas, may show only faint, focal EMA staining.
Fig. 10.14 
(A) Meningiom as are consistently immunopositive for epithelial membrane antigen (EMA). (B) Rhabdoid meningioma shows retained nuclear staining for INI1/BAF47 by immunohistoc hemistry; in true rhabdoid tumor or AT/RT, this nuclear staining is lost. (C) Meningioma ultrastructural findings include intercellular interdigitations and desmosomes
-
Claudin-1, a structural protein found in tight junctions, is detectable in up to 85 % of meningiomas and may be especially useful in diagnostically equivocal cases in which EMA staining is weak.
-
S-100 staining is variable.
-
Strong staining for CEA is typical of the pseudopsammoma bodies of secretory meningioma (Fig. 10.7F).
-
Ki-67, progesterone receptor (PR), and phosphohistone H3 (PHH3, a mitosis-specific antibody) staining may be useful from a prognostic standpoint. (See below.)

6 Electron Microscopy
-
Most meningiomas con tain intercellular complexes including desmosomes and interdigitations, as well as abundant intermediate filaments (Fig. 10.14C).
-
◦ These features may be inconspicuous in the fibrous variant.
-
◦ Microlumina, often with microvilli, are seen in secretory meningiomas.
-
7 Molecular Pathology
-
Alterations of various protei n 4.1 superfamily members are commonplace in meningiomas.
-
◦ Inactivation of the neurofibromatosis 2 (NF2) gene on 22q12 and loss of its protein product merlin are detected in approximately half of sporadic meningiomas and nearly all NF2-associated meningiomas.
-
◦ NF2 alterations are encountered in certain histologic variants (fibrous, transitional, and psammomatous) more frequently than in others (meningothelial).
-
◦ Deletions involving protein 4.1B (DAL-1 or “differentially expressed in adenocarcinoma of the lung”) are seen at a similar frequency overall in meningiomas, including pediatric examples.
-
◦ Though the above alterations have not been shown to have prognostic relevance independent of histologic grading, their detection may be helpful from a diagnostic standpoint in selected cases (see below).
-
-
Multiplicity of the above abnormalities is more frequent in atypical and malignant meningiomas.
-
Deletions of chromosomes 1p and 14q are frequent in pediatric and NF2-associated meningiomas, often accompanying other aggressive histologic features and a tendency for recurrence.
-
A strong association between clear cell meningioma and mutations involving SMARCE1 has been recently reported.
-
In pediatric radiation-induced meningiomas, chromosome 1p deletion and loss of 22q12.2 have also been reported.
8 Differential Diagnosis
-
Spindle-cell lesions such as s chwannoma, solitary fibrous tumor, and hemangiopericytoma may resemble meningiomas, particularly the fibrous variant.
-
◦ Unlike meningiomas, schwannomas are diffusely positive for S-100, and solitary fibrous tumors will be diffusely positive for CD34.
-
◦ Hemangiopericytomas are more variable in their immunolabeling, with possible staining for EMA, vimentin, CD34, and factor XIIIa, to a greater or lesser extent. They will, however, show the ultrastructural feature of pericellular basement membrane material (similar to schwannoma), a feature not present in meningiomas.
-
-
Renal cell carcinoma may be distinguished from clear cell meningioma by virtue of its diffuse immunopositivity for cytokeratin; CD10, RCC-marker antibody, PAX2, and PAX8 may likewise be helpful.
-
◦ Hemangioblastoma, another clear cell lesion, is positive for alpha inhibin and D2-40 and is generally EMA-negative. Careful inspection should divulge characteristic bubbly stromal cells.
-
-
Chordoid meningioma may closely mimic its namesake chordoma, but chordoma will show diffuse S-100 and cytokeratin positivity and contains typical physaliferous cells.
-
Though meningiomas may be quite vascular, they differ from arteriovenous malformations and other vascular lesions in that they contain meningothelial cells.
-
Grade III (anaplastic, rhabdoid, and papillary) meningiomas may frequently prove quite difficult to diagnose, as they may show significant histologic and even immunohistoch emical overlap with other high-grade neoplasms, including sarcomas, hemangiopericytomas, high-grade gliomas, AT/RT, and choroid plexus carcinoma.
-
◦ Detection of deletions of 22q (NF2), 18p (Dal1), 1p, or 14q by fluorescence in situ hybridization (FISH) analysis would provide additional support for classification as meningioma in these instances, as these a lterations are not expected in the other tumors.
-
◦ Immunohistochemical and/or molecular determination of INI1/BAF47 status is specifically helpful for differe ntiating rhabdoid meningioma from AT/RT, as INI1 should be lost (that is, not expressed) in AT/RT. Immunohistochemistry has been found to be a more reliable method in this instance, as deletions involving 22q are common to both tumor types, whereas INI1/BAF47 immunopositivity should be retained in rhabdoid meningiomas but not in AT/RT (Fig. 10.14B).
-
-
Melanocytoma may mimic benign meningioma, and malignant melanoma may mimic anaplastic/malignant meningioma. Unlike anaplastic meningioma, both of the melanocytic tumors are characteristically positive for S-100, HMB-45, and MART1, and negative for EMA.
-
Dural-based metastatic carcinomas, including choroid plexus carcinoma, may be effectively differentiated from meningiomas by virtue of their diffuse cytokeratin positivity.
9 Prognosis
-
Compared with meningiomas in adults, pediatric meningiomas generally have a poorer prognosis. The degree of initial tumor resection (dictated in part by tumor location), pathologic grade, and association with NF2 are the most important factors influencing prognosis in individual children.
-
Recurrence-free survival time is significantly related to WHO grade, but this does not appear to be the case for overall survival.
-
WHO grade III meningiomas, including anaplastic, rhabdoid, and papillary meningiomas, are all notable for markedly aggressive biologic behavior, typified by frequent invasion of brain and other nearby tissue, a higher rate of metastasis outside the CNS, and short recurrence-free and overall survival. Median overall survival is typically less than 2 years for adults with this tumor cohort, but it has not been well established in the pediatric population.
-
Radiation-associated pediatric meningiomas have an increased incidence of multiplicity at first presentation, as well as more frequent aggressive histologic variants.
-
Spinal pediatric meningiomas are frequent in association with NF2 and/or higher WHO grade subtype; they likewise have a higher propensity for recurrence.
Suggested Reading
Arivazhagan A, Devi BI, Kolluri SV, Abraham RG, Sampath S, Chandramouli BA. Pediatric intracranial meningiomas—do they differ from their counterparts in adults? Pediatr Neurosurg. 2008;44:43–8.
Burkhardt JK, Neidert MC, Grotzer MA, Krayenbuhl N, Bozinov O. Surgical resection of pediatric skull base meningiomas. Childs Nerv Syst. 2013;29:83–7.
Cai DX, Banerjee R, Scheithauer BW, Lohse CM, Kleinschmidt-Demasters BK, Perry A. Chromosome 1p and 14 q FISH analysis in clinico-pathologic subsets of meningioma: diagnostic and prognostic implications. J Neuropathol Exp Neurol. 2001;60:628–36.
Elbabaa SK, Gokden M, Crawford JR, Kesari S, Saad AG. Radiation-associated meningiomas in children: clinical, pathological, and cytogenetic characteristics with a critical review of the literature. J Neurosurg Pediatr. 2012;10:281–90.
Gasparetto EL, da Costa Leite C, Lucato LT, Barros CV, Marie SK, Santana P, et al. Intracranial meningiomas: magnetic resonance imaging findings in 78 cases. Arq Neuropsiquiatr. 2007;65:610–4.
Lakhdar F, Arkha Y, El Ouahabi A, Melhaoui A, Rifi L, Derraz S, et al. Intracranial meningioma in children: different from adult forms? A series of 21 cases. Neurochirurgie. 2010;56:309–14.
Liu Y, Li F, Zhu S, Liu M, Wu C. Clinical features and treatment of meningiomas in children: report of 12 cases and literature review. Pediatr Neurosurg. 2008;44:112–7.
Perry A, Scheithauer BW, Stafford SL, Lohse CM, Wollan PC. “Malignancy” in meningiomas: a clinicopathologic study of 116 patients, with grading implications. Cancer. 1999;85:2046–56.
Perry A, Giannini C, Raghavan R, Scheithauer BW, Banerjee R, Margraf L, et al. Aggressive phenotypic and genotypic features in pediatric and NF2-associated meningiomas: a clinicopathologic study of 53 cases. J Neuropathol Exp Neurol. 2001;60:994–1003.
Pinto PS, Huisman TA, Ahn E, Jordan LC, Burger P, Cohen KJ, et al. Magnetic resonance imaging features of meningiomas in children and young adults: a retrospective analysis. J Neuroradiol. 2012;39:218–26.
Raffalli-Ebezant H, Rutherford SA, Stivaros S, Kelsey A, Smith M, Evans DG, et al. Pediatric intracranial clear cell meningioma associated with a germline mutation of SMARCE1: a novel case. Childs Nerv Syst. 2015;31:441–7.
Rushing EJ, Olsen C, Mena H, Rueda ME, Lee YS, Keating RF, et al. Central nervous system meningiomas in the first two decades of life: a clinicopathological analysis of 87 patients. J Neurosurg. 2005;103:489–95.
Siddiqui MT, Mahon BM, Cochran E, Garruso P. Cytologic features of meningiomas on crush preparations: a review. Diagn Cytopathol. 2008;36:202–6.
Smith MJ. Germline and somatic mutations in meningiomas. Cancer Genet. 2015;208:107–14.
Stanuszek A, Piatek P, Kwiatkowski S, Adamek D. Multiple faces of children and juvenile meningiomas: a report of single-center experience and review of literature. Clin Neurol Neurosurg. 2014;118:69–75.
Takei H, Bhattacharjee MB, Rivera A, Dancer Y, Powell SZ. New immunohistochemical markers in the evaluation of central nervous system tumors. A review of 7 selected adult and pediatric brain tumors. Arch Pathol Lab Med. 2007;131:234–41.
Wang XQ, Zeng XW, Zhang BY, Dou YF, Wu JS, Jiang CC, et al. Spinal meningioma in childhood: clinical features and treatment. Childs Nerv Syst. 2012;28:129–36.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing AG
About this chapter
Cite this chapter
Fuller, C.E. (2016). Meningiomas. In: Adesina, A., Tihan, T., Fuller, C., Poussaint, T. (eds) Atlas of Pediatric Brain Tumors. Springer, Cham. https://doi.org/10.1007/978-3-319-33432-5_10
Download citation
DOI: https://doi.org/10.1007/978-3-319-33432-5_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-33430-1
Online ISBN: 978-3-319-33432-5
eBook Packages: MedicineMedicine (R0)