
Abstract
Dr. Joseph Torg made great advances in the diagnosis and understanding of anterior cruciate ligament (ACL) injury in 1976 with the publishing of his landmark paper, “Clinical diagnosis of anterior cruciate ligament instability in the athlete.” This publication defined the proper execution of the Lachman test, which is a variation of the more commonly utilized anterior drawer test, in diagnosing anterior cruciate ligament ruptures. At the time of publication, the ACL was thought to hold little importance, primarily due to an inability to effectively and consistently diagnose isolated rupture patterns and therefore, a lack of understanding of the ACL’s important role in joint stability. Torg purported the Lachman test as a way to overcome the difficulties in accurately diagnosing ACL insufficiency by resolving the problems commonly encountered when performing the anterior drawer test. A decade after initial introduction of the Lachman test, Torg and colleagues further defined a specific grading system for the Lachman test using a knee arthrometer. This allowed for a quantitative assessment of joint instability and, subsequently, outlined specific treatment protocols based on the relative severity of the injury. In the years following these publications, multiple other studies have supported the accuracy of the Lachman test in diagnosing isolated ACL ruptures, solidifying the importance of the test in the clinical setting.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
1 Historical Perspective
The 1970s brought about a drastic shift in the clinical treatment of anterior cruciate ligament (ACL) injuries. Previously, the diagnosis of ACL insufficiency was difficult and not obvious or reproducible during conventional physical examination. During this period, the main technique used to make the clinical diagnosis of an ACL tear was the anterior drawer sign. The anterior drawer test was performed by applying an anterior stress to the tibia with the knee flexed to 90° and the foot placed in internal, external, and neutral rotation. However, this test was often insufficient with a high false-negative rate for isolated ACL injury. The anterior drawer test was often only “positive” when associated with significant meniscal or capsular injury [2].
When a positive anterior drawer sign was demonstrated, conventional treatment of this era was to reduce the drawer at 90° of flexion and attempt to restore tension in the joint capsule [6, 11, 12]. This required a long phase of immobilization and rigorous rehabilitation. At the time, the ACL itself was rarely repaired or reconstructed. Instead, the procedure would render the joint stable through capsular contracture or fibrosis, while the ACL itself remained nonfunctional or absent. As a result, patient function did not typically return to the level of the uninjured knee with an intact ACL [2].
In 1976, Joseph Torg authored “Clinical diagnosis of anterior cruciate instability in the athlete,” which was published in the American Journal of Sports Medicine. This landmark paper provided the first clearly defined description of the Lachman test, a knee examination technique used to determine the status of the ACL in an attempt to improve clinical diagnosis and understanding of ACL instability. In many ways, the theories and perspectives outlined here drove the early phases of developing our current understanding of knee laxity and instability [14].
It is important to put Torg’s work into historical perspective, realizing that his purported view on the importance of proper diagnosis of ACL insufficiency went against mainstream thought at the time. However, it was also clearly acknowledged the “enigma” presented by the ACL. Great diversity of opinion surrounded ACL injury, such as injury mechanisms, efficacy of diagnostic techniques, and treatment and management protocols. This is evident in observations published by Helfet [5] who stated that “occasionally, when operating for a torn medial cartilage, one finds that the anterior cruciate ligament has been torn from its insertions in the tibia… but this knee does not demonstrate anterior-posterior instability preoperatively or postoperatively, and removal of the cartilage cures all symptoms. It is not possible to diagnose the coincidental rupture of the cruciate ligament before operations.” Elsewhere in the publication, Helfet stated that “isolated ruptures of the cruciate ligament are rare and of little clinical significance.”
Furthermore, in 1970, Smillie [13] published on various issues surrounding the use of the drawer sign in clinical examination. He stated, “the drawer sign is ‘minimal’ in isolated ruptures of the anterior cruciate ligament,” and went on to say that “if the sign is ‘maximal,’” it is likely that “the medial ligament has been involved,” therefore defining limitation at the time in diagnosing isolated ACL ruptures on clinical examination. Smillie also recognized that it is difficult to perform the drawer sign following acute injury because of factors such as pain, hemarthrosis, and muscle spasms. Finally, he stated that when an isolated rupture of the ACL occurred, “the anterior cruciate ligament alone is not the factor controlling instability, and a repair does not necessarily improve function. When rupture is associated with a tear of the medial meniscus, treatment is meniscectomy, the ruptured ligament being ignored.”
Helfet and Smillie summarized the thought process at the time, which was a lack of understanding of isolated ruptures of the ACL and their clinical significance due to limitations in diagnosing an isolated ACL tear with intact menisci, capsule, and collateral ligaments. On the other hand, supporters of the Lachman test and its theories challenged this concept and looked further. They believed that the ultimate key to advancing the understanding of ACL injury and subsequent treatment was to improve clinical diagnostic techniques.
Supporters of the Lachman test also rejected the thought process of the previously mentioned authors, believing that the authors’ statements regarding the ACL were a gross oversimplification of the problem. The supporters believed that ACL deficiency posed a greater long-term problem than was understood at the time and pointed to several publications in support of their ideas.
In 1955, O’Donoghue reported on the end results of patients with major ligamentous knee injuries and their progression to medial compartment disease [12]. The study found that 50 out of 69 patients (72 %) had tears of the ACL and based on the analysis of these cases, O’Donoghue concluded that ACL instability ultimately caused significant disability. Surgical repair of the ligament was therefore warranted and recommended.
In addition to O’Donoghue’s study, supporting evidence was found in a study by Kennedy et al. [9] around the same time. Kennedy had recently studied 50 patients with ACL tears and concluded that isolated tears of the ligament do occur. He found that there is a high incidence of associated medial meniscal damage in knees with ACL tears (40 % of patients in his study). However, he still concluded that an acceptable result could be seen in a high percentage of patients with or without ACL repair.
Thirdly, Allman in 1971 [3] was quoted as saying that, in some individuals with ACL tears that are not surgically repaired, the injury begins a cascade of events that causes progressive disability and disruption of integral structures within the knee, leading to “the beginning of the end.” The author goes on to describe the deficit in indications for surgical versus nonsurgical cases that was characteristic of the time, but most importantly the author stressed the functional importance of the ACL.
In turn, Torg clearly believed that a deeper understanding of the ACL was required and would undoubtedly lead to improved management of athletes with traumatic knee injuries. In his paper, he begins with a description of the anterior drawer test, which at that time was the classic clinical examination used to diagnose ACL ruptures. He then describes the Lachman test, the focus of his paper, and the paradigm-shifting clinical test for orthopedic surgeons everywhere.
At the time of Torg’s publication, it differed from other reports in two ways. First, it was understood that the ACL was of great clinical significance, and, second, the necessity of improving clinical diagnostic methods to more accurately and fully understand the entire spectrum of the injury was advocated. In pushing the understanding of the day, Torg was able to emphasize that a better diagnosis and treatment plan was possible by improving one of the most important tools available to physicians everywhere: the clinical examination.
2 The Anterior Drawer Test
In 1976, classic orthopedic teaching relied on the anterior drawer test to make a clinical diagnosis of ACL deficiency. The test was performed with that patient supine and the affected knee at 90° of flexion. The examiner would then attempt to translate the tibia anteriorly with respect to the femur by pulling on the posterior surface of the proximal end of the tibia (Fig. 9.1). A positive anterior drawer sign resulted when anterior translation of the tibia with respect to the femur was observed. This test was unquestionably relied upon, despite the fact that its origins were “obscure.” In “Clinical diagnosis of anterior cruciate instability in the athlete,” clinical experience with 172 ACL ruptures was described. Through that experience, it is concluded that the anterior drawer test was unreliable [14].

The Anterior Drawer Test
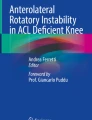
Torg believed there to be three main causes for false-negative anterior drawer tests or scenarios where ACL injury was either unrecognized or underappreciated (Fact Box 1). First, in the setting of acute ACL injury, there are typically an accompanying tense hemarthrosis and reactive synovitis in the joint space. These conditions preclude knee flexion to 90°, thus making it difficult to perform the drawer test with accuracy. Second, acutely following injury, the body experiences protective muscle spasms, such that in “the well-muscled, well-conditioned athlete” this would “generate considerable force” [14]. The resultant problem would be extreme difficulty in attempt to anteriorly translate the tibia against the opposed hamstring spasm. The vector analysis clearly demonstrates this issue. Third, the anatomy of the medial compartment of the knee when flexed to 90° versus relatively extended presents the main barrier to effective anterior translation of the tibia when performing the drawer test. The convex posterior surface of the medial femoral condyle is more congruent with the more concave medial tibial plateau in flexion. In addition, the presence of the posterior horn of the medial meniscus further prevents anterior translation of the tibia due to the supporting effect it produces against the posterior aspect of the medial femoral condyle (Fig. 9.2).

Diagram displaying the relationship between the medial femoral condyle, medial meniscus, and the tibia with the knee in 90° of flexion and viewed in a sagittal plane. Medial meniscus causes a “door stopper” effect preventing efficient anterior translation of the tibia during the anterior drawer test. MM medial meniscus (Reproduced with permission from Torg et al. [14])
Fact Box 1: Causes of False-Negative Anterior Drawer Tests [14]
1. Acute hemarthrosis precluding knee flexion to 90° |
2. Protective muscle spasms preventing anterior tibial translation |
3. Anatomical configuration of knee in flexion preventing effective anterior tibial translation |
Based on these observations, the study by Torg concluded that “significant ‘anterior drawering’ occurred only after peripheral separation of the posterior horn of the medial meniscus or disruption of the medial capsular and/or posterior oblique ligaments” [14]. This observation that combined injury to the ACL and medial meniscus resulted in greater joint instability was novel and began to advance our understanding of the effects produced by combined knee ligament injuries.
3 The Lachman Test
In response to the problems with the anterior drawer test presented above, “Clinical diagnosis of anterior cruciate instability in the athlete” proposed a new method for diagnosing ACL ruptures known as the Lachman test. The test received its name from John W. Lachman, MD, who was chairman and professor of Orthopaedic Surgery at Temple University at the time of the publication. For several years prior to the publication of “Clinical diagnosis of anterior cruciate instability in the athlete,” Lachman had been teaching this “simple, reliable, and reproducible clinical test to demonstrate anterior cruciate ligament instability” [14].
The Lachman test is performed with the patient supine and “the knee held between full extension and 15° of flexion.” The examiner would stabilize the femur with one hand and with the other hand apply firm pressure to the posterior aspect of the proximal tibia, attempting to translate it anteriorly relative to the femur (Fig. 9.3). A positive test, correlating with an anterior cruciate ligament tear, was described as the feeling of a “proprioceptive and/or visual anterior translation of the tibia in relation to the femur with a characteristic “mushy” or “soft” end point.” This is in stark contrast to the “hard” end point characteristic of a negative Lachman test, indicating that the ACL is intact [14].

The Lachman test
Furthermore, visual assessment is a valuable diagnostic indicator of ACL insufficiency. When viewed from the lateral aspect of the knee, anterior translation occurring in the presence of a positive test would eliminate the normal slope of the infrapatellar tendon between the patella and its insertion on the anterior aspect of the proximal tibia [14].
The Lachman test was developed to avert the previously mentioned issues that were associated with anterior drawer test (Fact Box 2). First, the reduced degree of flexion allowed the knee to assume a comfortable position even in the presence of hemarthrosis or reactive synovitis and decreased the likelihood of guarding, which precludes the execution of a proper test. Second, the effect of hamstring spasm is virtually negated as the force required to translate the tibia anteriorly is applied in a vector perpendicular to the pull of the hamstring muscle complex. Third, with the knee in relative extension, the contact area is between the tibial plateau, the medial meniscus, and the distal weight-bearing surface of the femur. Because this surface is relatively flat compared to the posterior femoral condyle, obstruction of anterior tibial translation is greatly reduced (Fig. 9.4). The Lachman test is able to overcome the difficulties associated with performing the anterior drawer test, giving the clinician greater acuity for diagnosing isolated ACL injury [14].

When the knee is in extension, the configuration of the joint components are changed such that the “door stopper” effect caused by the medial meniscus is relieved, allowing anterior tibial translation to occur unobstructed. MM medial meniscus (Reproduced with permission from Torg et al. [14]) (Figures reproduced with permission from: Torg JS, Conrad W, Kalen V. Am J Sports Med Volume 4, Issue 2. Pp. 84–93, ©1976 by SAGE Publications. Reprinted by Permission of SAGE Publications)
Fact Box 2: Benefits of Lachman Test [14]
1. Eliminates effect of acute hemarthrosis on successfully performing exam |
2. Negates force generated by hamstring spasms |
3. Produces optimal anatomical configuration for anterior tibial translation |
3.1 The Grading System
Nearly a decade after initial publication detailing the Lachman exam, Torg and colleagues established a grading system to assess the degree of joint instability for ACL disruption based on the extent of anterior tibial translation. The grading system ranges from I (least severe) to grade IV (most extensive injury and instability). The degree of anterior translation corresponding to each level was quantified using a knee arthrometer [4].
A grade I tear is defined as a positive Lachman test with the proprioceptive detection of a “soft” or “mushy” end point upon anterior tibial translation. Further appreciation of the positive test could be seen when placing the thumb on the joint line during the examination and comparing the difference between the injured leg and the contralateral side. In Torg’s study, grade I tears were associated with an anterior displacement of between 1 and 6 mm. A grade II tear was determined based on detection of the soft end point described above as well as visible anterior tibial translation. A distinguishing characteristic of a grade II tear was the disappearance of the normal slope of the infrapatellar tendon between the patella and its insertion on the anterior aspect of the proximal tibia. Grade II tears involved a displacement between 3 and 9 mm. A grade III tear was seen when the tibia displays passive anterior subluxation without a need for the examiner to provide a force. Placing a 4 × 4 × 6 in. block underneath the tibia just distal to the joint reproduces the same degree of subluxation. Similar to a grade II tear, the slope of the infrapatellar tendon will disappear as well. Grade III tears were associated with tibial translation ranging from 6 to 16 mm. A grade IV injury is defined in patients who were able to actively displace the tibia anteriorly by contracting the quadriceps muscle while either sitting or standing with the knee in flexion. The force produced through the muscle contraction alone is sufficient to translate the tibia anteriorly. Grade IV tears demonstrate anterior displacement ranging from 10 to 20 mm [4].
This grading system was to serve as a basis to guide treatment and management of patients with varying degrees of knee instability. In a proposed algorithm, grade I tears could be treated with a conservative course of bracing and rehabilitation. Grade II tests were generally indicative of injury to a combination of structures, usually one or both menisci in addition to the ACL. In such cases, arthroscopy was suggested as the proper course of treatment, along with bracing and subsequent rehabilitation. In some cases, an extra-articular cruciate substitution procedure was performed. Grade III tears required ACL repair or reconstruction as well as meniscal repair in the young active patient. Finally, a grade IV tear necessitated ACL repair or reconstruction and possibly medial capsular repair or reefing due to the extreme degree of instability [4].
3.2 External Verification
Following the publication of “Clinical diagnosis of anterior cruciate instability in the athlete” in 1976, multiple other authors have validated the Lachman test in clinical application. In 1983, DeHaven [3] found that the Lachman test is “much more reliable” than the anterior drawer test in diagnosing isolated anterior cruciate tears, being positive in 85 % of patients without anesthesia and nearly 100 % in patients with anesthesia. In the same year, Larson [10] also noted that the Lachman test is “one of the most accurate and sensitive tests” used to diagnose ACL injury. Johnson [7] notes that the Lachman test can “greatly increase the accuracy of the clinical examination.”
In 1982 Jonsson et al. [8] reported findings comparing the accuracy of the anterior drawer and Lachman tests performed on unanesthetized patients following acute ACL rupture. Their results showed that the Lachman test had a much higher diagnostic accuracy, with 39 out of 45 patients having a positive Lachman test whereas only 15 out of 45 had a positive anterior drawer test. Jonsson et al. concluded that the Lachman test is a “valuable diagnostic tool” and should be regularly utilized to evaluate the status of the ACL.
More recently, Benjaminse et al. [1] in 2006 concluded that the Lachman test has a high diagnostic accuracy from a meta-analysis of over 2,000 patients. This study pooled results from varied publications between 1980 and 1995. The Lachman test has had great longevity in the accurate clinical diagnosis of ACL injuries worldwide.
4 Conclusions
Four decades ago, “Clinical diagnosis of anterior cruciate instability in the athlete” emphasized the importance of complete and accurate clinical diagnosis, sought to improve exam skills, and opened the door to a greater understanding of combined knee injury patterns. This publication clearly noted differences in knee laxity patterns with various combined knee ligament injuries. The Lachman test has become a key component of the physical examination to effectively and efficiently diagnose varied degrees of knee instability. Treatment algorithms have been developed and advanced throughout the subsequent decades based on the clinical information afforded by the Lachman test.
The “Torg School of Thought” was integral to the advancement of the field of ACL management and surgery. The limitations of conventional wisdom and physical exam testing were challenged. This drove forward our understanding of knee instability, clinical diagnostic testing, and the appreciation for combined knee ligament injuries. Torg’s contributions serve as a strong foundation to our current day understanding of knee laxity and instability.
The Lachman test, originally described in 1976 by Dr. Joseph Torg, has become a key method to diagnose ACL insufficiency. The Lachman test still drives treatment algorithms today. The widespread clinical application of this simple and reproducible test has improved our ability to diagnose and quantify ACL injury. These works represent key advances in the early understanding of knee laxity and rotational instability.
References
Benjaminse A, Gokeler A, van der Schans CP (2006) Clinical diagnosis of an anterior cruciate ligament rupture: a meta-analysis. J Orthop Sports Phys Ther 36(5):267–288
Chambat P, Guier C, Sonnery-Cottet B et al (2013) The evolution of ACL reconstruction over the last fifty years. Int Orthop 37(2):181–186
DeHaven KE (1983) Arthroscopy in the diagnosis and management of the anterior cruciate ligament deficient knee. Clin Orthop Relat Res 172:52–56
Gurtler RA, Stine R, Torg JS (1987) Lachman test evaluated. quantification of a clinical observation. Clin Orthop Relat Res 216:141–150
Helfet A (1974) Disorders of the knee. Lippincott Co, Philadelphia, pp 92–93
Hughston JC, Eilers AF (1973) The role of the posterior oblique ligament in repairs of acute medial (collateral) ligament tears of the knee. J Bone Joint Surg Am 55(5):923–940
Johnson RJ (1983) The anterior cruciate ligament problem. Clin Orthop Relat Res 172:14–18
Jonsson T, Althoff B, Peterson L et al (1982) Clinical diagnosis of ruptures of the anterior cruciate ligament: a comparative study of the lachman test and the anterior drawer sign. Am J Sports Med 10(2):100–102
Kennedy JC, Weinberg HW, Wilson AS (1974) The anatomy and function of the anterior cruciate ligament. As determined by clinical and morphological studies. J Bone Joint Surg Am 56(2):223–235
Larson RL (1983) Physical examination in the diagnosis of rotatory instability. Clin Orthop Relat Res 172:38–44
Nicholas JA (1973) The five-one reconstruction for anteromedial instability of the knee. indications, technique, and the results in fifty-two patients. J Bone Joint Surg Am 55(5):899–922
O’Donoghue DH (1955) An analysis of end results of surgical treatment of major injuries to the ligaments of the knee. J Bone Joint Surg Am 37-A(1):1–13
Smillie I (1970) Injuries of the knee joint. The Williams and Wilkins Co, Baltimore, p 152
Torg JS, Conrad W, Kalen V (1976) Clinical diagnosis of anterior cruciate ligament instability in the athlete. Am J Sports Med 4(2):84–93
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Kropf, E.J., Colón, J.W., Torg, J.S. (2017). Knee Rotation: The Torg School. In: Musahl, V., Karlsson, J., Kuroda, R., Zaffagnini, S. (eds) Rotatory Knee Instability. Springer, Cham. https://doi.org/10.1007/978-3-319-32070-0_9
Download citation
DOI: https://doi.org/10.1007/978-3-319-32070-0_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-32069-4
Online ISBN: 978-3-319-32070-0
eBook Packages: MedicineMedicine (R0)