
Abstract
Approximately 80 % of bladder cancer is diagnosed as “conventional” urothelial carcinoma (UC) with 10–25 % nonurothelial and “variants” of urothelial carcinoma (UC). For the current discussion, variant histology will refer to any bladder malignancy other than pure UC. Furthermore, we have limited our review to the specific histologic variants sarcomatoid, plasmacytoid, and micropapillary bladder cancer. Before we discuss each of these variants in detail, we should mention that each of these histologic descriptions is based on morphologic features from H&E pathologic sections with little insight into their biology. Moreover, mixed histologies are often present (including so-called urothelial and nonurothelial carcinomas), for which the term variant histology is generally used. Figure 6.1 describes the histological classification of tumors arising from the urinary tract and was adapted from the 2004 World Health Organization classification of tumors.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Approximately 80 % of bladder cancer is diagnosed as “conventional” urothelial carcinoma (UC) with 10–25 % nonurothelial and “variants” of urothelial carcinoma (UC) [1, 2]. For the current discussion, variant histology will refer to any bladder malignancy other than pure UC. Furthermore, we have limited our review to the specific histologic variants sarcomatoid, plasmacytoid, and micropapillary bladder cancer. Before we discuss each of these variants in detail, we should mention that each of these histologic descriptions is based on morphologic features from H&E pathologic sections with little insight into their biology. Moreover, mixed histologies are often present (including so-called urothelial and nonurothelial carcinomas), for which the term variant histology is generally used. Table 6.1 describes the histological classification of tumors arising from the urinary tract and was adapted from the 2004 World Health Organization classification of tumors.
Challenges in the Study of Variant Histology
Sampling error and tumor heterogeneity at transurethral resection (TUR) have been reported to detect only 39 % of variant cancers [3, 4]. It has been estimated that up to 44 % of cases of histologic variants are not recognized or documented by community pathologists which further leads to underreporting and potential mismanagement. Initial reports have suggested variant tumors were uniformly present at a high stage with invasion into muscularis propria [1]. However, more recent studies have shown variant histology present within non-muscle-invasive (NMI) tumors [5–10]. In a large bladder cancer patient registry from the Netherlands, 23 % of all variant tumors identified within the registry presented with NMI disease [11].
While this is likely a reflection of increased awareness and recognition within the scientific community, variant histology often carries an aggressive and lethal diagnosis. One early study proposed that up to 20 % variant histology within a bladder specimen was associated with worse survival outcomes [12]. However, no consistency has been shown among subsequent studies, and it has become quite apparent that each bladder cancer variant behaves differently and needs to be addressed individually to assess its impact on the overall biology of the disease. In a recent retrospective study evaluating pathologic and survival outcomes among patients with variant histology, micropapillary and plasmacytoid variants were independently associated with twice the risk of all-cause mortality compared with nonvariant UC [13]. The significance of the extent of each specific variant remains an area of significant interest.
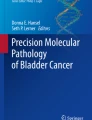
Diagnosing variant histology has been the rate-limiting step at understanding the biology and development of appropriate treatment algorithms. Figure 6.1 illustrates the most common histologic appearances of sarcomatoid, plasmacytoid, and micropapillary bladder cancer. In an effort to combat these challenges, many groups are collaborating to outline standards and guidelines in the identification and reporting of variant histology [4]. With the incorporation of collaborative efforts and centralized pathologic review, further improvements in the identification and treatment of variant bladder cancer will result. Figure 6.2 provides a decision tree utilized for the diagnosis and treatment of non-muscle-invasive variant histology bladder cancer. When feasible in muscle invasive disease, we believe that up-front radical cystectomy is the treatment of choice for reasons we will explain further in this chapter.

Histologic variants: sarcomatoid, plasmacytoid, and micropapillary. (a) Infiltrative urothelial carcinoma. Sarcomatoid variant without heterologous elements showing spindle cell morphology. (b) Infiltrating urothelial carcinoma of the bladder, plasmacytoid variant. (c) Micropapillary urothelial carcinoma (Reference: Eble et al. [50])

Decision tree for the clinical management of variant NMIBC
Significance of Variant Histology
Variant histology often portends to worse oncologic outcomes when compared to conventional urothelial carcinoma. Several retrospective studies suggest to be the result of a higher propensity of locally aggressive disease, higher rates of distant metastasis, and a different response to chemotherapy or radiotherapy as compared to conventional UC. In a study of 448 consecutive TURBT cases with 295 subsequent cystectomies, mixed histology was present in 25 %, and the presence of variant architecture almost uniformly predicted the presence of locally advanced disease at cystectomy [1]. Another study observed that among 600 cystectomy patients, variant histology predicted upstaging at the time of cystectomy with an odds ratio of 2.77 [14]. The presence of variant histology has also been found to be associated with increased rates of pathologic lymph node metastasis leading to worse survival outcomes [15, 16]. In one of the largest multi-institutional studies pertaining to variant histology, identified patients with adenocarcinoma, small cell carcinoma, or other histologic subtypes had worse disease-specific survival compared to conventional UC even adjusting for stage, adjunctive treatment, and lymphovascular invasion on multivariate analyses [17].
However, other studies have presented conflicting evidence that these trends may not be true for all variant types of bladder cancer. The Southwest Oncology Group (SWOG)-randomized trial S8710 showed increased survival for neoadjuvant MVAC (methotrexate, vinblastine, Adriamycin, cisplatin) plus cystectomy over cystectomy alone in patients with locally advanced (cT2-T4a) bladder cancer [18]. In a secondary analysis they demonstrated that patients with mixed histology (squamous and glandular differentiation) had improved survival rates after neoadjuvant MVAC chemotherapy as well as a higher rate of pT0 downstaging (34 %) versus cystectomy alone (4 %). This translated to improved survival rates for patients with mixed histology after neoadjuvant chemotherapy, though statistical significance was not achieved. This secondary analysis challenges the notion that all variant histology leads to a worse overall prognosis and outcome.
Non-muscle-Invasive Variant Bladder Cancer
There is intense controversy regarding non-muscle-invasive bladder cancer with variant histology, both in terms of diagnosis, role of intravesical therapy, and aggressive up-front radical cystectomy. Clinical staging for NMI variant bladder cancer is critical. While this is important for conventional UC, some argue that since variant tumors notoriously are associated with advanced disease, there may be a potentially higher risk of understaging for variant tumors. Thus, intravesical therapy would be less effective and potentially lead to missed opportunity for cancer cure. Several studies for cT1 NMI variant bladder cancer have reported local understaging rates ranging from 27 to 57 % [1, 4, 19]. Rates of occult metastatic disease have also been reported as high as 27–44 % among NMI variant tumors [5] with divergent histology being associated with the presence of lymph node metastasis and decreased survival [20]. Thus, in the setting of NMI variant bladder cancer, a more aggressive treatment strategy might be warranted. However, other studies have reported progression rates of approximately 40 % which is similar to conventional UC with high-risk features [5, 10, 19, 21]. Caution must be made when extrapolating results from these studies as they included tumors with squamous or glandular differentiation, nested variant, and micropapillary disease. The role of intravesical treatment for variant NMIBC should be considered based on the unique subtype and should be weighed against the risk of understaging in order to optimize oncologic outcomes.
Sarcomatoid
Carcinosarcomas (CS) are biphasic malignant neoplasms with morphological evidence of both epithelial (carcinomatous) and mesenchymal (sarcomatous) differentiation. It is different from sarcomatoid carcinoma (SaC) of the bladder, which is a malignant spindle cell neoplasm, in which epithelial differentiation may be demonstrated by immunohistochemical or ultrastructural studies. However, World Health Organization classification system acknowledges the controversy surrounding the terminology and histogenesis of these tumors of the bladder and now includes what used to be called carcinosarcoma together with sarcomatoid UC.
Sarcomatoid variant is a rare variant of UC, which accounts for approximately 0.3 % of all urothelial tumors [22]. A history of radiation and intravesical cyclophosphamide chemotherapy has been associated. Macroscopically, tumors are often polypoid with often advanced large intraluminal masses.
Microscopically, the sarcomatous component is usually a high-grade spindle cell neoplasm, whereas the epithelial component can be in the form of conventional UC, squamous cell carcinoma, adenocarcinoma, small cell carcinoma, or overlying carcinoma in situ. The immunohistochemical profile of the sarcomatoid variant of UC includes positivity for epithelial markers, at least focally, including cytokeratin and epithelial membrane antigen. This immunohistochemical profile distinguishes this entity from pure sarcomas [23].
Similar to other variants, sarcomatoid carcinoma also tends to present with advanced stage, distant metastasis, and local progression [10, 19]. The mean age of presentation is 66 years (50–77) with presentation similar to conventional UC with hematuria as the usual presenting symptom. These tumors are typically diagnosed at advanced local stage, and they often exhibit nodal or distant metastases. The significance of this variant lies in its association with a poor prognosis [24]. After controlling for stage, patients with sarcomatoid disease have a worse survival and higher disease-specific mortality (almost twofold greater) than those with conventional UC [10, 25]. Pathological stage is the best predictor of survival in sarcomatoid variants [24]. Good prognostic factors include negative surgical margins and absence of metastatic disease at the initial presentation; however, even with these favorable prognostic factors taken into account, 2-year mortality is almost 70 %.
Few case reports/series have been reported with few population-based analyses providing further information on this rare variant. Wright et al. presented a SEER database of patients with SaC, CS, and urothelial carcinoma (UC) treated between 1988 and 2003 [10]. It was found that patients with both SaC and CS presented more frequently with locally advanced or metastatic disease. Survival was worse for sarcomatoid variants compared with UC in organ-confined and metastatic disease. Five-year survival was 17 % and 37 % in SaC and CS, respectively, compared with 47 % in UCs.
Appropriate modalities and sequence of administration remain to be defined. However, given the aggressive behavior of the tumor precludes radical therapy whenever possible. A variety of treatment modalities have been described, but optimal treatment requires rather a multimodality approach. The effectiveness of different modalities is not known because of varying rates of usage of adjuvant radiation (15–45 %) and chemotherapy (5–60 %) and varying results of each case [26]. Transurethral resection and partial cystectomy carry the risk of incomplete tumor resection. Radical cystectomy with pelvic lymphadenectomy is the mainstay of treatment, although patients tend to develop local recurrence after surgery [10].
Wang et al. presented SEER databases, which included 221 patients, between 1973 and 2004. Median age of the patients was 75 years (range 41–96) [25]. 72.5 % had a locally advanced or distant stage. 53.9 % of patients underwent transurethral resection only, 35.8 % of patients had radical or partial cystectomy, and 15.8 % of patients received surgery followed by radiation therapy. The median overall survival was 14 months (95 % confidence interval 7–21 months). The overall 1-, 5-, and 10-year survival rates were 53.9 %, 28.4 %, and 25.8 %. The overall 5-year survival rate after cystectomy was only 20.3 %, suggesting a high risk of early dissemination. Cancer-specific survival was significantly better for those who underwent cystectomy instead of transurethral resection.
The rationale for the use of adjuvant chemotherapy in this variant is the aggressive nature of the disease. Probability of metastasis is high (50–70 %). The combination of gemcitabine and cisplatin is an effective and well-tolerated chemotherapy regimen for the treatment of advanced UC. However, no data are available regarding its use in bladder sarcomatoid UC. The use of this chemotherapy regimen in sarcomatoid variants was first reported by Froehner in a single case of metastatic (pulmonary) SC showing durable, complete local, and pulmonary remission, but, the pathological stage, was not reported (pTxNxM1) in this study, and hence no conclusion can therefore be drawn [27]. Other platinum-based regimens have been utilized with varying responses and include methotrexate, vinblastine, doxorubicin, and cisplatin as well as gemcitabine and cisplatin when concerned for nephrotoxicity. As mentioned in most of the studies, favorable outcomes may be explained by good performance status, absence of nodal and metastatic involvement, and delivery of chemotherapeutic agents at the full dose.
The role of adjuvant radiation in SC can be justified on the basis of high chances of local invasion and pelvic lymph node metastasis, known with this variant. Adjuvant radiotherapy to the dose of 50–60 Gy, along with the various combinations of chemotherapy has been used in certain case reports, but has yielded inconsistent results. No definite effect of adjuvant radiation on local control can be concluded in view of limited case studies and high disease-specific mortality.
Plasmacytoid
Plasmacytoid urothelial carcinoma (PUC) is uncommon; however, as with other variant bladder cancers, it exhibits a unique clinical behavior. As is the case with the prior variants, PUC is associated with advanced local and distant disease at presentation in an often younger subset of patients than conventional UC [28]. Morphologically, PUC presents with a discohesive, single cell growth pattern, with eccentrically located nuclei and an abundant eosinophilic cytoplasm [28]. PUC is usually diagnosed at an advanced pathological stage, and survival appears to be more unfavorable to what has been described for conventional UC [3]. PUC often expresses unfavorable molecular features, such as the loss of CK20, high proliferation index, p53 accumulation, and complete loss of membranous E-cadherin expression [29]. Loss of E-cadherin is a sign of epithelial-mesenchymal transition (EMT), and upregulation of transcriptional repressors of E-cadherin may contribute to the aggressiveness of these tumors which may portend to reduced sensitivity to chemotherapeutic agents [29, 30]. Interestingly, even in the setting of negative surgical margins, the peritoneum remains a site of major recurrence. Because of this predisposition for peritoneal metastasis, CEA, CA125, and CA19-9 have been incorporated as potential tumor markers for PUC [31, 32].
While few studies on PUC exist, a 31-patient case series has been published in patients with >50 % PUC at the time of TUR to determine the utility of neoadjuvant chemotherapy [32]. Median overall survival was 17.7 months (stage I–III vs IV; 45.8 vs 13.3). In patients who presented with metastatic disease and were treated with chemotherapy, median survival was 12.6 months. Moreover, no survival difference was noted between those receiving neoadjuvant chemotherapy and those proceeding to up-front cystectomy, though some chemotherapeutic responses were observed. A recent study found therapeutic strategies with radical cystectomy, and cisplatin-based chemotherapy was not as effective for PUC as it was described for locally advanced UC or micropapillary bladder cancer, however, a complete response to adjuvant chemotherapy administering MVAC and neoadjuvant chemotherapy using gemcitabine and cisplatin may occur in a subgroup of PUC patients [33]. Therefore, chemotherapy in a neoadjuvant or adjuvant setting should be included in the treatment paradigm. PUC tumor biology represents a negative prognostic factor for patients suffering from this histologic variant. Because of the aggressive nature of PUC and the high rates of peritoneal metastasis, aggressive therapy incorporating radical cystectomy is likely required for both invasive and NMI forms of PUC.
Micropapillary
Micropapillary bladder carcinoma (MPBC) has been a recent interest of many groups with a majority of variant studies published on this particular variant. MPBC is a distinct variant of conventional UC and resembles papillary serous carcinoma of the ovary. MPBC is typically found in the background of conventional UC to varying degrees of involvement but can also be associated with squamous cell carcinoma of the bladder [34], adenocarcinoma [35], small cell carcinoma [36], and sarcomatoid carcinoma [37]. Studies of MPBC have helped elucidate the void in our understanding variant bladder cancer. Published literature has demonstrated not only that MPBC has a relatively poor recognition in community practices but great heterogeneity even among academic pathologists regarding the histologic diagnosis of micropapillary architecture with only classical cases of MPBC showing consensus [38].
A majority of MPBC studies have consistently shown that muscle invasive MPBC is associated with high rates of locally advanced, metastatic disease associated with limited overall survival [6, 8, 35, 37, 39]. As previously mentioned, MPBC often exists within the background of conventional UC with small amounts of MPBC within the tumor being clinically significant with >10 % MPBC associated with worse clinical outcomes [39, 40]. The largest single institution series to date from MD Anderson Cancer Center demonstrated that the overall prognosis of MPBC was poor with 5- and 10-year OS rates of 54 % and 27 %, respectively [21], despite a relatively high proportion of patients with NMI-MPBC at presentation (44 %). Moreover, there were high rates of upstaging at the time of radical cystectomy (52.7 %) and occult lymph node metastases identified in 27.3 % of patients. Others studies have reported rates of occult metastatic disease as high as 35 and 86 % [6]. In the MD Anderson cohort, the lymph node metastases were often reported to contain micropapillary features, independent of percentage of involvement of MPBC in the primary tumor, suggesting a predisposition of MPBC to spread by lymphatic invasion. Interestingly, case-matched studies with conventional UC have demonstrated that stage for stage, there is no survival difference in MPBC and conventional UC [41, 42].
There remains limited consensus regarding the clinical management of MPBC [43]. The utilization of multimodality treatments including neoadjuvant chemotherapy varies, and the definition of risk stratification groups within the arena of MPBC remains to be elucidated. The MD Anderson experience suggested MPBC might not respond to chemotherapy with worse survival identified among those receiving neoadjuvant chemotherapy after controlling for stage [21]. However, others have argued due to high rates of upstaging at surgery and high rates of lymph node metastasis, systemic chemotherapy should be incorporated [6]. A retrospective cohort reported a 45 % pathologic pT0 downstaging rate among MPBC patients after neoadjuvant chemotherapy compared to 13 % downstaging in those patients who underwent up-front cystectomy. They also noted a survival advantage with neoadjuvant chemotherapy for patients that were downstaged [44]. While there are limitations to all of these studies including retrospective nature, small sample size, relatively short follow-up, and few quality controls for chemotherapy regimens, the role of neoadjuvant chemotherapy for organ-confined MPBC remains controversial.
The initial MD Anderson study was one of the first to help develop an awareness of variant histology among NMI-MPBC as well as diagnostic and therapeutic strategies needed to optimize oncologic outcomes. In one study, 44 patients with NMI-MPBC were treated with intravesical bacillus Calmette-Guérin (BCG) versus up-front radical cystectomy [5]. Cancer progression was 67 % in the BCG group with progression to metastatic disease in 22 %. Patients who underwent delayed cystectomy after BCG failure were found to have worse disease-specific survival rates compared to up-front radical cystectomy. In a follow-up study, patients who received BCG had recurrence, progression, and lymph node metastasis in 75 %, 45 %, and 35 %, respectively [45]. Patients treated with up-front cystectomy had improved survival compared to patients treated with primary BCG (5-year disease-specific survival 100 % vs 60 %, p = 0.006) and patients who underwent delayed cystectomy after recurrence (5-year disease-specific survival 62 %, p = 0.015). Prognosis was especially poor in patients who waited for progression before undergoing radical cystectomy with an estimated 5-year disease-specific survival of only 24 % and a median survival of 35 months. In patients treated with up-front cystectomy, pathological upstaging was done in 27 %, including 20 % with lymph node metastasis. In these studies, the authors concluded that because of the high rates of occult metastatic disease and the poor prognosis associated with BCG failure, up-front radical cystectomy was the treatment of choice for cT1 MPBC. These findings coincide with a recent population-based study which identified 120 patients with MPBC. After controlling for stage, there was no difference in survival between MPBC and conventional UC except among patients with NMI-MPBC where worse survival outcomes was noted [8].
Other authors have suggested intravesical BCG might be an appropriate therapy for NMI-MPBC. In a publication from Memorial Sloan Kettering Cancer Center, they noted equivalent survival outcomes between intravesical BCG and up-front radical cystectomy. While no survival difference was noted, there was a 21 % incidence of metastasis in the BCG cohort with a 27 % rate of occult metastatic disease in those patients who underwent up-front cystectomy [46]. Other reports have made similar conclusions regarding intravesical BCG which have also suggested that BCG might be appropriate in patients with a small percentage of micropapillary component in the tumor [9].
While no universal guidelines exist for the management of MPBC, radical cystectomy is encouraged for invasive disease. Conflicting evidence exists regarding the optimal management for NMI-MPBC; however, many experts still favor up-front radical cystectomy over BCG due to high rates of distant metastasis and the poor survival after BCG failure [45, 47].
Future Therapy
In order to direct appropriate therapy for variant histologies including sarcomatoid, plasmacytoid, and micropapillary bladder cancer, we need precise diagnosis at the onset. Moreover, due to the limited diagnoses made relative to conventional UC, the likelihood of developing randomized controlled trials is dismal, and we must rely on data combined from large centers in order to direct future therapies. It appears aggressive local therapy with radical cystectomy when diagnosis is made and surgically feasible remains the mainstay of treatment. Tissue from these patients can then be studied in order to direct targeted therapies desperately needed among these aggressive histologic variants. Subtyping of bladder cancer has been performed by several groups, including our own [48], suggesting that several distinct classes of bladder cancer exist based on gene expression platform data. It is important that this is performed with tumors showing variant histologies, which would enhance our understanding of the innate biology of these subtypes and establish treatment paradigms based on putative cell pathways and target identification. Unfortunately, there are no targeted therapies to date as in the case of conventional UC; however, we are optimistic that further collaborative efforts among UC studies may help direct treatment options for these aggressive histologic variants as well [49].
Conclusion
Precise identification and staging of variants including sarcomatoid, plasmacytoid, and micropapillary bladder cancer is cornerstone to making appropriate treatment decisions. Radical cystectomy is the mainstay of treatment with multimodal chemotherapy treatments also considered when feasible. Further research directed at risk stratification within each of the variant histologies is needed in order to identify appropriate treatments to ameliorate the often poor survival outcomes among these patients. As with the case of conventional UC, targeted therapies are needed, and further research among these variants as well as conventional UC may elucidate targeted agents for these variant histologies.
References
Wasco MJ, Daignault S, Zhang Y, et al. Urothelial carcinoma with divergent histologic differentiation (mixed histologic features) predicts the presence of locally advanced bladder cancer when detected at transurethral resection. Urology. 2007;70(1):69–74.
Kantor AF, Hartge P, Hoover RN, Fraumeni Jr JF. Epidemiological characteristics of squamous cell carcinoma and adenocarcinoma of the bladder. Cancer Res. 1988;48(13):3853–5.
Abd El-Latif A, Watts KE, Elson P, Fergany A, Hansel DE. The sensitivity of initial transurethral resection or biopsy of bladder tumor(s) for detecting bladder cancer variants on radical cystectomy. J Urol. 2013;189(4):1263–7.
Hansel DE, Amin MB, Comperat E, et al. A contemporary update on pathology standards for bladder cancer: transurethral resection and radical cystectomy specimens. Eur Urol. 2013;63(2):321–32.
Kamat AM, Gee JR, Dinney CP, et al. The case for early cystectomy in the treatment of nonmuscle invasive micropapillary bladder carcinoma. J Urol. 2006;175(3 Pt 1):881–5.
Ghoneim IA, Miocinovic R, Stephenson AJ, et al. Neoadjuvant systemic therapy or early cystectomy? Single-center analysis of outcomes after therapy for patients with clinically localized micropapillary urothelial carcinoma of the bladder. Urology. 2011;77(4):867–70.
Comperat E, Roupret M, Yaxley J, et al. Micropapillary urothelial carcinoma of the urinary bladder: a clinicopathological analysis of 72 cases. Pathology. 2010;42(7):650–4.
Vourganti S, Harbin A, Singer EA, Shuch B, Metwalli AR, Agarwal PK. Low grade micropapillary urothelial carcinoma, does it exist? – analysis of management and outcomes from the Surveillance, Epidemiology and End Results (SEER) database. J Cancer. 2013;4(4):336–42.
Amin A, Epstein JI. Noninvasive micropapillary urothelial carcinoma: a clinicopathologic study of 18 cases. Hum Pathol. 2012;43(12):2124–8.
Wright JL, Black PC, Brown GA, et al. Differences in survival among patients with sarcomatoid carcinoma, carcinosarcoma and urothelial carcinoma of the bladder. J Urol. 2007;178(6):2302–6; discussion 2307.
Shapur NK, Katz R, Pode D, et al. Is radical cystectomy mandatory in every patient with variant histology of bladder cancer. Rare Tumors. 2011;3(2):e22.
Jozwicki W, Domaniewski J, Skok Z, Wolski Z, Domanowska E, Jozwicka G. Usefulness of histologic homogeneity estimation of muscle-invasive urinary bladder cancer in an individual prognosis: a mapping study. Urology. 2005;66(5):1122–6.
Monn MF, Kaimakliotis HZ, Pedrosa JA, et al. Contemporary bladder cancer: variant histology may be a significant driver of disease. Urol Oncol. 2015;33(1):18 e15–20.
Turker P, Bostrom PJ, Wroclawski ML, et al. Upstaging of urothelial cancer at the time of radical cystectomy: factors associated with upstaging and its effect on outcome. BJU Int. 2012;110(6):804–11.
Kassouf W, Agarwal PK, Grossman HB, et al. Outcome of patients with bladder cancer with pN+ disease after preoperative chemotherapy and radical cystectomy. Urology. 2009;73(1):147–52.
Domanowska E, Jozwicki W, Domaniewski J, et al. Muscle-invasive urothelial cell carcinoma of the human bladder: multidirectional differentiation and ability to metastasize. Hum Pathol. 2007;38(5):741–6.
Rogers CG, Palapattu GS, Shariat SF, et al. Clinical outcomes following radical cystectomy for primary nontransitional cell carcinoma of the bladder compared to transitional cell carcinoma of the bladder. J Urol. 2006;175(6):2048–53; discussion 2053.
Scosyrev E, Ely BW, Messing EM, et al. Do mixed histological features affect survival benefit from neoadjuvant platinum-based combination chemotherapy in patients with locally advanced bladder cancer? A secondary analysis of Southwest Oncology Group-Directed Intergroup Study (S8710). BJU Int. 2011;108(5):693–9.
Weizer AZ, Wasco MJ, Wang R, Daignault S, Lee CT, Shah RB. Multiple adverse histological features increase the odds of under staging T1 bladder cancer. J Urol. 2009;182(1):59–65; discussion 65.
El-Sebaie M, Zaghloul MS, Howard G, Mokhtar A. Squamous cell carcinoma of the bilharzial and non-bilharzial urinary bladder: a review of etiological features, natural history, and management. Int J Clin Oncol. 2005;10(1):20–5.
Kamat AM, Dinney CP, Gee JR, et al. Micropapillary bladder cancer: a review of the University of Texas M. D. Anderson Cancer Center experience with 100 consecutive patients. Cancer. 2007;110(1):62–7.
Zhai QJ, Black J, Ayala AG, Ro JY. Histologic variants of infiltrating urothelial carcinoma. Arch Pathol Lab Med. 2007;131(8):1244–56.
Sung MT, Wang M, MacLennan GT, et al. Histogenesis of sarcomatoid urothelial carcinoma of the urinary bladder: evidence for a common clonal origin with divergent differentiation. J Pathol. 2007;211(4):420–30.
Lopez-Beltran A, Pacelli A, Rothenberg HJ, et al. Carcinosarcoma and sarcomatoid carcinoma of the bladder: clinicopathological study of 41 cases. J Urol. 1998;159(5):1497–503.
Wang J, Wang FW, Lagrange CA, Hemstreet Iii GP, Kessinger A. Clinical features of sarcomatoid carcinoma (carcinosarcoma) of the urinary bladder: analysis of 221 cases. Sarcoma. 2010;2010:454792, 7.
Black PC, Brown GA, Dinney CP. The impact of variant histology on the outcome of bladder cancer treated with curative intent. Urol Oncol. 2009;27(1):3–7.
Froehner M, Gaertner HJ, Manseck A, Wirth MP. Durable complete remission of metastatic sarcomatoid carcinoma of the bladder with cisplatin and gemcitabine in an 80-year-old man. Urology. 2001;58(5):799.
Keck B, Wach S, Stoehr R, et al. Plasmacytoid variant of bladder cancer defines patients with poor prognosis if treated with cystectomy and adjuvant cisplatin-based chemotherapy. BMC Cancer. 2013;13:71.
Keck B, Stoehr R, Wach S, et al. The plasmacytoid carcinoma of the bladder – rare variant of aggressive urothelial carcinoma. Int J Cancer. 2011;129(2):346–54.
Shiota M, Song Y, Yokomizo A, et al. Foxo3a suppression of urothelial cancer invasiveness through Twist1, Y-box-binding protein 1, and E-cadherin regulation. Clin Cancer Res. 2010;16(23):5654–63.
Topalak O, Saygili U, Soyturk M, et al. Serum, pleural effusion, and ascites CA-125 levels in ovarian cancer and nonovarian benign and malignant diseases: a comparative study. Gynecol Oncol. 2002;85(1):108–13.
Dayyani F, Czerniak BA, Sircar K, et al. Plasmacytoid urothelial carcinoma, a chemosensitive cancer with poor prognosis, and peritoneal carcinomatosis. J Urol. 2013;189(5):1656–61.
Hayashi T, Tanigawa G, Fujita K, et al. Two cases of plasmacytoid variant of urothelial carcinoma of urinary bladder: systemic chemotherapy might be of benefit. Int J Clin Oncol. 2011;16(6):759–62.
Holmang S, Thomsen J, Johansson SL. Micropapillary carcinoma of the renal pelvis and ureter. J Urol. 2006;175(2):463–6; discussion 466–7.
Johansson SL, Borghede G, Holmang S. Micropapillary bladder carcinoma: a clinicopathological study of 20 cases. J Urol. 1999;161(6):1798–802.
Alvarado-Cabrero I, Sierra-Santiesteban FI, Mantilla-Morales A, Hernandez-Hernandez DM. Micropapillary carcinoma of the urothelial tract. A clinicopathologic study of 38 cases. Ann Diagn Pathol. 2005;9(1):1–5.
Baschinsky DY, Chen JH, Vadmal MS, Lucas JG, Bahnson RR, Niemann TH. Carcinosarcoma of the urinary bladder – an aggressive tumor with diverse histogenesis. A clinicopathologic study of 4 cases and review of the literature. Arch Pathol Lab Med. 2000;124(8):1172–8.
Sangoi AR, Beck AH, Amin MB, et al. Interobserver reproducibility in the diagnosis of invasive micropapillary carcinoma of the urinary tract among urologic pathologists. Am J Surg Pathol. 2010;34(9):1367–76.
Samaratunga H, Khoo K. Micropapillary variant of urothelial carcinoma of the urinary bladder; a clinicopathological and immunohistochemical study. Histopathology. 2004;45(1):55–64.
Lopez-Beltran A, Cheng L. Histologic variants of urothelial carcinoma: differential diagnosis and clinical implications. Hum Pathol. 2006;37(11):1371–88.
Wang JK, Boorjian SA, Cheville JC, et al. Outcomes following radical cystectomy for micropapillary bladder cancer versus pure urothelial carcinoma: a matched cohort analysis. World J Urol. 2012;30(6):801–6.
Fairey AS, Daneshmand S, Wang L, et al. Impact of micropapillary urothelial carcinoma variant histology on survival after radical cystectomy. Urol Oncol. 2014;32(2):110–6.
Willis DL, Flaig TW, Hansel DE, et al. Micropapillary bladder cancer: current treatment patterns and review of the literature. Urol Oncol. 2014;32(6):826–32.
Meeks JJ, Taylor JM, Matsushita K, et al. Pathological response to neoadjuvant chemotherapy for muscle-invasive micropapillary bladder cancer. BJU Int. 2013;111(8):E325–30.
Willis DL, Fernandez MI, Dickstein RJ, et al. Clinical outcomes of cT1 micropapillary bladder cancer. J Urol. 2015;193(4):1129–34.
Spaliviero M, Dalbagni G, Bochner BH, et al. Clinical outcome of patients with T1 micropapillary urothelial carcinoma of the bladder. J Urol. 2014;192(3):702–7.
Porten SP, Willis D, Kamat AM. Variant histology: role in management and prognosis of nonmuscle invasive bladder cancer. Curr Opin Urol. 2014;24(5):517–23.
Choi W, Porten S, Kim S, et al. Identification of distinct basal and luminal subtypes of muscle-invasive bladder cancer with different sensitivities to frontline chemotherapy. Cancer Cell. 2014;25(2):152–65.
Choi W, Czerniak B, Ochoa A, et al. Intrinsic basal and luminal subtypes of muscle-invasive bladder cancer. Nat Rev Urol. 2014;11(7):400–10.
Eble JN, Sauter G, Epstein JI, Sesterhenn IA. Pathology and genetics of tumours of the urinary system and male genital organs. World Health Organization Classification of Tumours, IARC Press, Lyon, France. 2004. p. 1–354.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Williams, S.B., Kamat, A.M. (2016). Urothelial Carcinoma with Variant Histology: Sarcomatoid, Plasmacytoid, and Micropapillary. In: Pagliaro, L. (eds) Rare Genitourinary Tumors. Springer, Cham. https://doi.org/10.1007/978-3-319-30046-7_6
Download citation
DOI: https://doi.org/10.1007/978-3-319-30046-7_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-30044-3
Online ISBN: 978-3-319-30046-7
eBook Packages: MedicineMedicine (R0)