
Abstract
Interpersonal motor coordination is considered to be an integral part of maintaining successful social interactions. Research has shown that simply coordinating one’s movements with another actor can influence rapport as well as feelings of social connection and social competence. Past research has also found that deficits in social motor coordination are associated with psychological dysfunction such as schizophrenia and borderline personality disorders. However, the potential association between interpersonal motor coordination and autism spectrum disorder (ASD) has only received a very limited amount of attention. In the current experiment, children who had been previously diagnosed with ASD and typically developing (TD) children were asked to synchronize with or imitate the movements of an experimenter in two different interpersonal motor tasks: object tapping and hand-clapping. Both the experimenter’s and the participants’ movements were captured and compared to each other using relative phase analysis and cross-recurrence quantification analysis (CRQA). The results reveal differences not only in the patterning of the coordination that occurred for ASD and TD children, but also in the stability and deterministic structure of the coordination. Of particular interest was the finding that children with ASD exhibited less stable (robust), but more deterministic patterns of interpersonal social motor coordination compared to TD children.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others

Keywords
- Autism Spectrum Disorder
- Autism Spectrum Disorder
- Typically Develop
- Autism Spectrum Disorder Group
- Typically Develop Child
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Children with autism spectrum disorder (ASD) exhibit numerous impairments that can severely impede learning and overall social functioning at home and in school, as well as make successful treatment difficult. Even though the dynamics of interpersonal motor coordination is considered to be an integral part of maintaining successful social interactions [1, 2], this dimension of behavioral order remains overlooked within the field of ASD research. This is despite the fact that there is now a well-established body of research demonstrating how intentionally or unintentionally coordinating one’s movements with those of another individual can positively influence rapport, feelings of social connection, and feelings of social competence [2–5]. Previous research has also found that deficits in social motor coordination are associated with other social psychological disorders such as schizophrenia [6, 7] and borderline personality disorders [8]. It is therefore important to understand the degree to which social motor coordination (or the lack thereof) is related to social competency in children diagnosed with ASD.
With regard to the previous research examining social motor impairments in ASD, the general findings are often limited in scope and sometimes inconsistent and contradictory [9]. The limited scope and contradictory nature of this previous work is due, in part, to the fact that empirical, clinical, and observational research is often treated in isolation, without any attempt to formalize an integrative methodological approach for identifying and understanding the core ASD deficits in social motor coordination [9]. Thus, the social motor impairments that characterize children with ASD and the degree to which these impartments relate to ASD severity are largely unknown. Moreover, many researchers have simply focused their inquiries on whether children with ASD are or are not capable of carrying out certain social motor tasks, without examining how they perform these tasks over time—i.e., without examining the patterns or dynamics of the social motor behavior that occurs within a social context [9].
Of particular relevance for the current study, is that the few studies that have investigated the dynamics of social motor coordination in children with ASD have highlighted how these deficits might not be due to an absence of coordination, but rather to a difference in the patterning compared to typically developing (TD) children [1, 9, 10]. For example, Marsh and colleagues [1] investigated the interpersonal movement coordination that occurred between children and their parents sitting and rocking side-by-side in rocking chairs. The results revealed that both ASD and TD children could coordinate with the movements of their parents, but that the overall patterning (the relative phase relationship) that characterized the coordination for ASD and TD children was different, with TD children more spontaneously and reciprocally modifying their movements with respect to their parents than children with ASD. The goal of the current study was to further explore the dynamics of social motor coordination in children with ASD with the use of non-linear, as well as linear time-series methods.
Cross-Recurrence Quantification Analysis (CRQA) is a non-linear analysis method that quantifies the dynamic (time-evolving) similarity between two behavioral time- or event-series by identifying whether behavioral states/events in the two series reoccur over time. The benefits of this analysis method over other time-series methods (e.g., cross-correlation, cross-spectral analysis) is that it does not require a researcher to make any a priori assumptions about the structure or stationarity of the data analyzed. Moreover, this method can be employed to uncover recurrent structure between the behaviors of two individuals regardless of whether the behavior in question exists within a single state space or in a more abstract multi-dimensional (multivariate) state space. Defined at a more intuitive level, the method assesses whether the points (states) in a behavioral series visit the same states over time and then quantifies the dynamic patterns of these time-evolving recurrences using a range of statistics. Common statistics include: Percent Recurrence (%REC), which measures the percentage of recurrent states between the two time-series and is an index of the degree to which the two behavioral signals are confined to a similar region of state or phase space; Percent Determinism (%DET), which measures the percentage of recurrent states that form sequential lines of recurrent points (i.e., diagonal lines in a recurrence plot) and quantifies the degree to which the co-varying structure of two behavioral time-series is the result of deterministic vs. random processes; and MaxLine, which extracts the longest sequence of recurrent states (longest diagonal line in a recurrence plot), and provides a proportional measure of the stability of the coordination present between two behavioral time-series.
CRQA has previously been used to study the patterning and stability of coordination between people in social situations. For instance, Richardson and colleagues [11] demonstrated through the use of CRQA that the coordination that arises between the rhythmic limb movements of two people follows the same dynamics as a person coordinating her two arms intrapersonally. Furthermore, they were able to demonstrate that the increased variability in coordination observed in social situations was not due to an increase in movement noise (indexed with the use of %REC), but rather was due to the visual coupling of the interpersonal situation being significantly weaker than the biomechanical coupling that characterizes intrapersonal interlimb coordination (as indexed by MaxLine). In a more realistic, full-body conversational task, Shockley and colleagues [12] found that pairs of participants having a conversation in order to solve a puzzle showed higher amounts of postural coordination (greater %REC; greater recurrent postural activity) than when participants were conversing with a confederate. Additionally, they found that participants’ postural trajectories were more stable (as indexed by MaxLine) when talking with each other, compared to when they were conversing with a confederate.
Accordingly, the aim of the current study was to employ CRQA to investigate the potential differences in the stability and patterning of the interpersonal coordination that occurred for children diagnosed with ASD compared to TD children. To achieve this aim we investigated two simple coordination tasks (i.e., an object tapping and hand clapping tasks) performed between an experimenter and ASD or TD children. Once this aim is achieved, it would be feasible to use our new-found understanding to extract the pertinent CRQA measures derived from an interpersonal task during the diagnostic process and include these findings as part of the criteria when deciding whether to apply the ASD diagnosis. Furthermore, these measures could instigate new intervention models focused on interpersonal coordination for children and adults already diagnosed with ASD.
2 Method
Forty three children previously diagnosed with ASD (and with a confirmed diagnosis made by a research certified clinician administering the Autism Diagnostic Observation Schedule second edition (ADOS-2)) who were classified as high functioning, and 47 typically developing children participated in the study.Footnote 1 Participants were between the ages of 6 and 10 years (M = 7.92, SD = 1.45 years, see Table 12.1 for age and gender distribution by group).
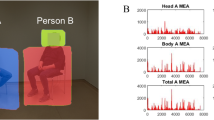
The study was conducted in a 10 by 12 foot laboratory room at Cincinnati Children’s Hospital Medical Center (University of Cincinnati, Cincinnati, OH). Children came into the laboratory room and were asked to sit at a 2 foot wide × 4 foot long × 2 foot high table next to the seated experimenter (see Fig. 12.1). Four Polhemus Latus receptors were attached to the underside of the table top, one in each corner, to create a 10 × 12 × 8 foot capture volume around the table. As soon as the child was seated, the four Polhemus Liberty Latus wireless markers/sensors were placed in wristbands and slipped over the child’s and experimenter’s wrists (one marker on each wrist of the child and experimenter). The motion of the Polhemus sensors was recorded at 94 Hz on a Dell PC computer using a custom software application written by the authors using the Polhemus Latus C/C ++ SDK Library.

Room set-up for the a tapping task and b, c interpersonal hand clapping game
The data presented here was part of a bigger project, in which participants performed a large range of motor, social and cognitive tasks. Here, we selected two social motor coordination tasks that were performed by all of the children. The first coordination task was a sequence of tapping movements, which involved children using a stick to tap/hit three drum-like cylinders from left to right (see Fig. 12.1a). Children repeated this left-to-right drumming sequence six separate times with the experimenter showing the sequence previous to every child in a continuous manner. Participants were randomly assigned to either an imitation or synchrony condition for this task, in the ASD group 20 children were in the imitation condition, while 21 were in the synchrony, as for the TD group, 26 synchronized while 21 imitated. In the imitation condition, the child was asked to repeat the tapping pattern demonstrated by the experimenter. In the synchrony condition, children were asked to repeat the tapping pattern in time with the experimenter after every sequence. The second task was an interpersonal hand clapping game (pat-a-cake), in which children completed a simple repetitive sequence of clapping their hands together and then with the experimenter (see Fig. 12.1b, c). The hand clapping game was completed twice, with each sequence involving around 15 consecutive intrapersonal and interpersonal clapping movements.
2.1 Data Analysis
The x-plane (left-right), y-plane (forward-back) and z-plane (up-down) positional coordinates of the sensors placed on the wrists of the experimenter and child were recorded for each task. To best determine the stability and pattering of the behavioral coordination that occurred between the child and experimenter, we first isolated the primary plane of motion for each task. Since the primary plane of motion for the tapping task was in the left-right (sagittal) plane, the x-plane movement time series was used to assess the behavioral coordination that occurred for this task (for a sample time series see Fig. 12.2a). For the interpersonal hand clapping game, the largest amplitude of movement was in the up-down (transverse), z-plane, with the intrapersonal clapping events occurring at a lower height than the interpersonal clap events (see Fig. 12.2b). Accordingly, this plane of motion was employed to assess the behavioral coordination that occurred for this task.Footnote 2

Sample movement time series (raw unfiltered data) from a child in the a object tapping task and the b interpersonal hand clapping game
For the tapping task, we then performed a coordination analysis as well as a cross-recurrence quantification analysis using the primary plane of motion time series of the experimenter’s right forearm (the experimenter always used his right hand/arm for all the tasks) and the primary plane of motion time series of the forearm used by the child for analysis. Note that for this task the child was free to use either left or right arm/hand. Although both arms/hands were employed by the experimenter and child for the hand clapping game, we only report the analysis of the right forearm movements of the experimenter and child because the coordination that occurred between the left forearm movements was completely redundant with the right.
Prior to analysis all of the pre- and post-non-task relevant movement transient periods were cropped from the different time series such as the period from the start of the recording to the start of the task and the periods in the synchrony condition where the experimenter repeated the sequence every time, otherwise all trials were included in the analysis. The time series were allowed to vary in length across participants. The resulting time series lengths in the tapping task were (ASD: Mean (M) number of data points = 3286.82, Standard Deviation (SD) = 761.30; TD: M = 3087.46, SD = 674.12) and in the hand clapping game (ASD: M = 4774.47, SD = 491.03; TD M = 4194.15, SD = 439.01). These final motion time series were then low-passed filtered using 10 Hz 4th order Butterworth filter to remove measurement noise.
To determine the patterning and stability of the social motor coordination that occurred between the children and the experimenter for each task and condition, two measures of interpersonal coordination were employed: distribution of relative phase (see [13] for a review of studies that have employed this measure) and CRQA.
2.1.1 Distribution of Relative Phase Angles (DRP)
This measure evaluated the concentration of relative phase angles between the movements of the child and experimenter (i.e., the relative space-time angular location of the movements of the child and experimenter) across nine 20° regions of relative phase (0–20°, 21–40°, 41–60°, 61–80°, 81–100°, 101–120°, 121–140°, 141–160°, 161–180°). To determine these distributions, we computed the continuous relative phase of the two time series between −180° and 180° using the Hilbert transform [14]. We then computed the percentage of occurrence of the absolute value of the relative phase angles across the nine 20° relative phase regions from 0° to 180°. Previous research has demonstrated that stable social motor coordination is characterized by a concentration of relative phase angles in the portions of the distribution near 0° and 180° (e.g., [9, 15, 16]), which corresponds to inphase and antiphase patterns of coordination, respectively.
DRP was analyzed using a 9 (phase region: 0°, 30°, 50°, 70°, 90°, 110°, 130°, 150°, 180°) × 2 (diagnosis: ASD, TD) × 2 (condition: imitation, synchrony) mixed ANOVA for the object tapping task with phase region as the repeated measures factor (a Greenhouse-Geisser correction was employed where necessary). For the interpersonal hand clapping game, DRP was analyzed using a 9 (phase region) × 2 (diagnosis) mixed ANOVA. Of particular interest was the difference between ASD and TD children in the magnitude of inphase coordination (percentage of time in 0° bin) for synchronous object-tapping and hand-clapping tasks and in the magnitude of antiphase coordination (percentage of time in the 180° bin) for the imitation object-tapping task. Therefore, when a phase region by diagnosis interaction was found to be significant, planned t-tests were employed to compare these relative phase regions as a function of diagnosis.
2.1.2 Cross Recurrence Quantification Analysis (CRQA)
This measure evaluated the time-evolving phase-space structure of coordination that arose between the experimenter and the child when performing the two coordinative tasks. When analyzing the object tapping task data, an embedding dimension of 7, lag of 100, and radius of 15 % was used. For the interpersonal hand clapping game, an embedding dimension of 5, lag of 45 and radius of 10 % was used.Footnote 3 These differences in parameter settings were due to the different pace and constraints of each experimental task. Since the goal of the study was to investigate the differences that might arise between children previously diagnosed with ASD and those who are typically developing, the parameters were kept constant for every child in each task. The CRQA measures %REC, %DET, and MaxLine were then analyzed using separate 2 (diagnosis: ASD, TD) × 2 (condition: imitation, synchrony) between subjects ANOVAs for the object tapping task. For the interpersonal hand clapping game, %REC, %DET and MaxLine were analyzed using separate independent samples t-tests.
3 Results
3.1 Object Tapping Task
For the object tapping task the DRP analysis revealed a main effect of phase region (F(8,672) = 62.62, p < 0.01, η 2 p = 0.43), a two-way interaction between phase region and diagnosis (F(8,672) = 8.07, p < 0.01, η 2 p = 0.09) a two-way interaction between phase region and condition (F(8,672) = 316.52, p < 0.01, η 2 p = 0.79) and, most importantly, a three-way interaction between phase region, diagnosis and condition (F(8,672) = 10.10, p < 0.01, η 2 p = 0.11; see Fig. 12.3). Planned t-tests revealed a lack of difference between the ASD and TD at the 180° phase region (t(39) = −0.68, p = 0.50) when the children were asked to imitate the experimenter. However, when asked to synchronize with the experimenter, the children in the TD group showed significantly larger occurrence of 0° phase relationship (M = 39.71, SD = 15.53) than those in the ASD group (M = 23.44, SD = 9.71; t(45) = −4.18, p < 0.01).

Mean DRP observed in the object tapping task by phase region, diagnosis and condition. The error bars represent the standard error of the mean
Collectively, these DRP results would seem to indicate that children diagnosed with ASD were just as capable of imitating the experimenter’s tapping movements as TD children. In contrast, however, the stability of the synchronous coordination for children with ASD was significantly weaker compared to TD children, which suggests that the synchronous motor coordination that occurred between the children with ASD and the experimenter was either less robust or more variable than the coordination that occurred between the experimenter and TD children.
The analyses of the CRQA measures revealed no significant main effects of diagnosis (all ps > 0.19). However, there was a significant main effect for condition in all measures (%REC: F(1, 84) = 90.03, p < 0.01, η 2 p = 0.52; MaxLine: F(1, 84) = 36.53, p < 0.01, η 2 p = 0.30; and %DET: F(1, 84) = 22.08, p < 0.01, η 2 p = 0.21), such that children who were in the imitation group showed higher %REC (M = 1.97, SD = 1.06), %DET (M = 98.85, SD = 1.17) and MaxLine (M = 112.68, SD = 97.71) than those in the synchrony group (%REC: M = 0.23, SD = 0.68; %DET: M = 92.20, SD = 8.82; MaxLine: M = 23.32, SD = 18.79). Finally, there was a significant interaction between diagnosis and condition for %REC (F(1, 84) = 8.36, p = 0.01, η 2 p = 0.09; for both %DET and MaxLine, ps > 0.20; see Fig. 12.4). Simple effects analyses for %REC showed that in the imitation group, TD children had significantly more recurrent activity (M = 2.34, SD = 1.10) than the children with ASD (M = 1.58, SD = 0.89, t(39) = −2.44, p = 0.02), while there was no significant difference in the synchrony group (t(45) = 1.42, p = 0.16). Accordingly, the results for CRQA with respect to diagnosis are somewhat opposite the results observed for DRP above, in that they appear to indicate that the similarity between the child and experimenter phase-space trajectories is similar for ASD and TD children during synchronous performance, but that this is not the case during imitative performance. That is, for the imitation condition there was less recurrent activity for ASD compared to TD children.

Mean a %REC, b %DET and c MaxLine by diagnosis and condition for the object tapping task. The error bars show the standard error of the mean
3.2 Interpersonal Hand Clapping Game
Consistent with the synchrony results for the object tapping task, the DRP analysis for the synchronous hand-clapping task revealed a significant main effect of phase region (F(8, 656) = 614.73, p < 0.01, η 2 p = 0.88) and a significant phase region by diagnosis interaction (F(1, 656) = 15.12, p < 0.01, η 2 p = 0.16; see Fig. 12.5). Again, the planned t-test revealed that children with ASD spent significantly less time in the 0° phase region (M = 43.37, SD = 15.28) than those in the TD group (M = 57.10, SD = 14.31; t(82) = −4.25, p < 0.01), indicating that the coordination for the ASD children was less stable or more variable compared to TD children.

Mean distribution of relative phase angles (DRP) by diagnosis. The error bars represent standard error of the mean
The analyses of the CRQA measures showed no significant differences in %REC between the ASD and TD children (t(84) = 0.18, p = 0.86). Surprisingly, however, there was a significant difference between the ASD and TD groups for MaxLine (t(84) = 1.95, p = 0.05), with children previously diagnosed with ASD having significantly longer MaxLine scores (M = 141.53, SD = 120.25) than the TD children (M = 97.47, SD = 86.30). Similarly, children previously diagnosed with ASD showed significantly higher %DETFootnote 4 (M = 98.01, SD = 1.06) than the TD children (M = 97.14, SD = 2.34; t(84) = 2.22, p = 0.03; see Fig. 12.6). Together, these MaxLine and %DET results appear to suggest that the coordination observed for the ASD children was more regular and exhibited a greater level of local stability than the coordination observed for the TD children.

Mean a %REC, b %DET and c MaxLine by diagnosis for the interpersonal hand clapping game. The error bars show the standard error of the mean
4 Discussion
The goal of the current study was to better understand the differences in social motor coordination between typically developing children and those that have been diagnosed with autism spectrum disorder through the use of a nonlinear analysis technique (i.e. cross-recurrence quantification analysis, CRQA) as well as a linear analysis technique (i.e. distribution of the relative phase, DRP). These differences were explored using a simple imitative and synchronous interpersonal object tapping task and synchronous hand-clapping task. For the object tapping task, children’s movements were in general more stable in the imitation condition than in the synchrony condition, as shown by the higher occurrence of antiphase relative phase angles (a relative phase of 180°) during imitation trials as opposed to the diminished occurrence of inphase relative phase angles in the synchrony trials. Additionally, the TD children were able to maintain the desired inphase relationship more often than those who had been previously diagnosed with autism in the synchrony condition. This finding was supported by the CRQA measures where MaxLine was significantly higher (i.e. showing a higher degree of stability) for the trials in the imitation condition than those in the synchrony condition. Also, the measure of %REC was able to capture the higher degree of coordination established between the children and the experimenter in the imitation trials compared to the synchrony trials. However, this measure was only able to differentiate the two diagnostic groups in the imitation trials, and not in the synchrony trials.
Regarding the seemingly contradicting results of the object tapping task in the context of diagnosis, where the DRP and CRQA measures differed, we would conclude that DRP and %REC in particular are isolating different aspects of the underlying coordination dynamics and, thus, that these measures provide a complementary index of the stability of coordination for the social object tapping task. Although conclusively defining what these different aspects are remains to be determined, one possibility is that DRP is providing a greater overall index of spatial-temporal coordination independent of movement amplitude or the degree of asymmetric movement kinematics, whereas %REC is providing a better measure of differences in the intrinsic dynamics (i.e., movement stiffness, variability, etc.) of the children’s or experimenter’s movements during social motor coordination [11, 17]. Thus, for the object tapping task, the current results may indicate that the local movement dynamics of children with ASD are more different than the experimenter’s compared to TD children, and that this is more apparent in the imitation task due to the lack of local coupling (which is present in the synchronous condition).
For the interpersonal hand clapping game, the distribution of relative phase showed a significant difference by diagnosis, showing that TD children were able to maintain the desired inphase relationship more often than those previously diagnosed with ASD. Again, however, the CRQA analysis provides a slightly different picture compared to the DRP results. More specifically, although there was no difference in %REC, children with ASD exhibited more deterministic (i.e., higher %DET) patterns of coordination compared to TD children, as well as a higher degree of local stability (i.e., greater MaxLine) than the TD children. As argued above, the DRP seems to capture an overall index of the spatio-temporal patterning of the coordination, but is less sensitive to the underlying dynamics of the coordination or the intrinsic dynamics of the movements themselves [11, 17]. Indeed, for the synchronous hand-clapping task the CRQA analysis appears to be indicating that the local stability and deterministic structure of the coordination for the ASD children is significantly greater than for TD children. Why then, is the overall coordination as measured by the DRP greater for TD children than for ASD children? Normally, when coordination is seen as less stable, it is assumed that this instability is created by increased random fluctuations, however, it seems that for the synchronous hand-clapping task employed here that the decrease in overall spatial-temporal coordination for ASD children compared to TD children is fueled by more deterministic movements of the child or experimenter when the coordination task involves a child with ASD. This is consistent with previous research examining the structure of movements in patients with Parkinson’s disease [18] and Schizophrenia [6] and implies that the movements of the ASD children are less flexible than the movements of TD children [19]. Finally, the current results also highlight the need for future research more specifically aimed at examining the influence of the experimenter’s movement modulation in cooperative tasks like the hand clapping game. Indeed, although we see differences and an effect of diagnosis in the task employed here, further work is required to tease apart how much of the difference is mediated by experimenter versus the child since the experimenter in this case was not blind to the child’s group membership (due to the easily observable differences between the children’s behaviors).
In conclusion, the current study provides new insights about the differences in social motor coordination in children with and without ASD and further exemplifies how the dynamics of social motor coordination can be used as an ASD related behavioral bio-marker in children, and eventually exploited as a diagnostic measure to improve this process. It is important to note that the differences observed between ASD and TD children were most pronounced during synchronized behavior, as opposed to imitative behavior. Accordingly, simple cooperative synchrony tasks seem to be better suited to uncovering ASD related social motor deficiencies [9]. The current results also demonstrate the importance of employing both linear (i.e., DRP) and nonlinear (i.e., CRQA) analysis techniques in order to fully understand the processes underlying social motor deficits in ASD (as well as in other disorders).
Notes
- 1.
Due to measurement and experimenter error, data for two ASD participants in the object tapping task and four TD participants in the interpersonal hand clapping game was missing.
- 2.
An analysis of secondary planes of motion produced results that were consistent with those reported here.
- 3.
The embedding dimension was chosen through the use of the false nearest neighbor (FNN) methodology while the lag was determined with the use of average mutual information (AMI).
- 4.
Since %DET showed a ceiling effect in all of these analyses, the number of points required to be considered a line in the recurrence plot was systematically raised from 3 up to 7 points in order to investigate more fine-grained differences that might arise between the two groups in this particular measure. The results of this additional analysis however, matched the main results and did not add any new information.
References
K.L. Marsh, R.W. Isenhower, M.J. Richardson, M. Helt, A.D. Verbalis, R.C. Schmidt, D. Fein, Autism and social disconnection in interpersonal rocking. Front. Integr. Neurosci. 7(4), 1–8 (2013)
K.L. Marsh, M.J. Richardson, R.C. Schmidt, Social connection through joint action and interpersonal coordination. Top. Cogn. Sci. 1(2), 320–339 (2009). doi:10.1111/j.1756-8765.2009.01022.x
F.J. Bernieri, Coordinated movement and rapport in teacher-student interactions. J. Nonverbal Behav. 12(2), 120–138 (1988)
J.E. Grahe, F.J. Bernieri, The importance of nonverbal cues in judging rapport. J. Nonverbal Behav. 23(4), 253–269 (1999)
L.K. Miles, L.K. Nind, C.N. Macrae, The rhythm of rapport: interpersonal synchrony and social perception. J. Exp. Soc. Psychol. 45(3), 585–589 (2009)
M. Varlet, L. Marin, S. Raffard, R.C. Schmidt, D. Capdevielle, P. Boulenger, J. Del-Monte, B.G. Bardy, Impairments of social motor coordination in Schizophrenia. PLoS One 7(1) (2012), doi:10.1371/journal.pone.0029772
F. Ramseyer, W. Tschachter, Nonverbal synchrony in psychotherapy: coordinated body movement reflects relationship quality and outcome. J. Consult. Clin. Psych. 79, 284–295 (2011)
M. Gratier, G. Apter-Danon, The musicality of belonging: repetition and variation in mother-infant vocal interaction, in communicative musicality: narratives of expressive gesture and being human, in Communicative Musicality: Exploring the Basis of Human Companionship, ed. by S. Malloch, C. Trevarthen (Oxford University Press, Oxford, 2008), pp. 301–327
P. Fitzpatrick, R. Diorio, M.J. Richardson, R.C. Schmidt, Dynamical methods for evaluating the time-dependent unfolding of social coordination in children with autism. Front. Integr. Neurosci. 7(21), 1–13 (2013)
C.M. Glazebrook, D. Elliot, J. Lyons, A kinematic analysis of how young adults with and without autism plan and control goal-directed movements. Mot. Control 10(3), 244–264 (2006)
M.J. Richardson, R.C. Schmidt, B. Kay, Distinguishing the noise and attractor strength of coordinated limb movements using recurrence analysis. Biol. Cybern. 96, 59–78 (2007)
K. Shockley, M. Santana, C.A. Fowler, Mutual interpersonal postural constraints are involved in cooperative conversation. J. Exp. Psychol. Hum. Percept. Perform. 29(2), 326–332 (2003)
R.C. Schmidt, M.J. Richardson, Dynamics of interpersonal coordination, in Coordination: Neural, Behavioral and Social Dynamics, ed. by A. Fuchs, V. Jirsa (Springer, Heidelberg, 2008), pp. 281–308
A. Pikovsky, M. Rosenblum, J. Kurths, Synchrony: A Universal Concept in Nonlinear Sciences (Cambridge University Press, Cambridge, 2001)
M.J. Richardson, K.L. Marsh, R.W. Isenhower, J.R. Goodman, R.C. Schmidt, Rocking together: dynamics of intentional and unintentional interpersonal coordination. Hum. Mov. Sci. 26(6), 867–891 (2007)
R.C. Schmidt, S. Morr, P.A. Fitzpatrick, M.J. Richardson, Measuring the dynamics of interactional synchrony. J. Nonverbal Behav. 36, 263–279 (2012)
M.J. Richardson, S. Lopresti-Goodman, M. Mancini, B. Kay, R.C. Schmidt, Comparing the attractor strength of intra- and interpersonal interlimb coordination using cross-recurrence analysis. Neurosci. Lett. 438, 340–345 (2008)
J.M. Schmit, M.A. Riley, A. Dalvi, A. Sahay, P.K. Shear, K.D. Shockley, R.Y. Pun, Deterministic center of pressure patterns characterize postural instability in Parkinson’s disease. Exp. Brain Res. 168(3), 357–367 (2006)
G.C. Van Orden, H. Kloos, S. Wallot, Living in the pink: intentionality, wellbeing, and complexity, in Handbook of the Philosophy of Science, Philosophy of Complex Systems, vol. 10, ed. by C. Hooker (Elsevier, Amsterdam, 2011), pp. 639–682
Acknowledgments
The authors would like to thank Dr. Holly Barnard, Dr. Amie Duncan, Dr. Joseph Amaral, and Carrie Thomas for their help in data collection. Research reported in this publication was supported by the National Institutes of Health under Award Number R21MH094659. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this paper
Cite this paper
Romero, V., Fitzpatrick, P., Schmidt, R.C., Richardson, M.J. (2016). Using Cross-Recurrence Quantification Analysis to Understand Social Motor Coordination in Children with Autism Spectrum Disorder . In: Webber, Jr., C., Ioana, C., Marwan, N. (eds) Recurrence Plots and Their Quantifications: Expanding Horizons. Springer Proceedings in Physics, vol 180. Springer, Cham. https://doi.org/10.1007/978-3-319-29922-8_12
Download citation
DOI: https://doi.org/10.1007/978-3-319-29922-8_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-29921-1
Online ISBN: 978-3-319-29922-8
eBook Packages: Physics and AstronomyPhysics and Astronomy (R0)