
Abstract
Our skin is exposed daily to a large number of chemicals in household products, cosmetics, in the environment and in the workplace. Many of these chemicals can cause irritant or allergic contact dermatitis. Allergic contact dermatitis is an inflammatory skin disease that is mediated by our immune system. In this chapter we summarize current methods for the diagnosis of contact dermatitis and treatment strategies. In addition we review our current understanding of the cellular and molecular pathomechanisms and its implications for the development of novel diagnostic and treatment strategies and of animal-free testing strategies for contact allergen identification.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Allergic contact dermatitis
- ACD
- Antigen presenting cell
- APC
- Hypersensitivity
- Damage-associated molecular pattern
- T cell
- Mononuclear cell
- Local Lymph Node Assay
- LLNA
- Contact dermatitis
- Heterologous innate immunity
-
Allergic contact dermatitis affects 5–10 % of the general population and prevalence is increasing
-
Contact dermatitis is the most important occupation-related skin disease
-
Causative treatment strategies, development of new drugs and of in vitro assays to replace animal testing for contact allergen identification are needed and require a detailed mechanistic understanding of the pathomechanisms
-
The innate immune response to contact allergens is mechanistically similar to anti-infectious immune responses
-
Biomarker panels are being identified for improved diagnostics and distinction of different types of eczema
Allergic Contact Dermatitis: Prevalence, Clinical Presentation and Etiology
Allergic contact dermatitis (ACD) is an eczematous skin reaction to substances (mostly small chemical compounds, so-called haptens) in non-toxic concentrations that requires an immunological cell-mediated sensitization and usually occurs after repeated exposure to the substance, while the same substance does not elicit reactions in non-sensitized individuals.
ACD is caused by activation of the immune system by chemical allergens due to their ability to cause skin inflammation and, consequently, a chemical-specific T cell response. ACD shows increasing prevalence. Roughly 20 % of the general population is sensitized to at least one contact allergen and about 5–10 % develop ACD once per year [1, 2].
The more than 4,000 known contact allergens are found for example in household products, cosmetics, plants, jewelry, clothes and in the workplace. Sensitization does not necessary result in the development of ACD but once the disease has developed, it can become chronic. A major problem is the formation of memory T cells which cause eczema upon re-exposure to the eliciting contact allergen.
Occupational contact dermatitis is the most common occupation-related skin disease [3]. Here, chronic ACD may result from chronic allergen exposure leading to significant damage to the skin. Chronic ACD is difficult to treat and requires complete avoidance of the contact allergen. This often demands that the patients change profession. The socio-economic costs of ICD and ACD are very high and the treatment options are still limited [3–5].
The yearly hitlist of the clinically most relevant contact allergens as presented by the German working group for contact dermatitis (DKG)/German Information Network of Departments of Dermatology (IVDK) consortium has nickel in the first place for many years already, followed by fragrance mix and balsam of Peru [6]. The contact allergen of the year 2013 was the preservative methylisothiazolinone (MI) and sensitization to MI remains a very serious problem [7, 8]. MI is used in cosmetics but also in household products such as paint. Due to the replacement of other preservatives the use of MI and methylchloroisothiazolinone (MCI)/MI (Kathon CG) has increased, and the concentrations used seem problematic. Even airborne exposure to MI can cause severe allergic skin reactions as well as asthma symptoms [9]. Action is now taken to reduce the concentrations of MI in consumer products and to find replacements.
The clinical presentations of ACD can be classified according to the disease kinetics and duration (acute versus chronic ACD), the route of allergen exposure (direct skin exposure, airborne exposure, systemic exposure), the localization (localized e.g., hand, lower leg, face, eyelid, genitoanal, generalized, flexural etc.), the exposure conditions (occupational, accidental, iatrogenic) and the type of contact allergen (e.g., weak, strong, obligatory contact sensitizer).
The acute ACD is characterized by an onset of clinical signs and symptoms within 3–12 h after contact with the allergen. The kinetic of the response depends on the degree of the preexisting sensitization – the stronger the degree of sensitization the faster the onset of symptoms. The initial reaction is characterized by dermal edema, vasodilatation and a beginning perivascular infiltrate of mononuclear cells. Within 6–24 h the infiltrate becomes more prominent and is accompanied by epidermal changes with spongiosis and increasing exocytosis of mononuclear cells into the epidermis. Depending on the type of contact allergen and degree of sensitization the reaction peaks at 24–48 h with a dense dermal mononuclear infiltrate, intra-epidermal blister formation, loss of the granular layer (stratum granulosum) and signs of parakeratosis. The resolution of the acute ACD reaction usually starts around 48–72 h and is characterized by reduction of epidermal spongiosis and blister formation, acanthosis of the epidermis and gradual reduction of the dermal and epidermal mononuclear infiltrate. Clinically, ACD is characterized by infiltrated erythematous pruritic patches and papules with or without vesicular reactions. The histological changes are reflected by the symptoms of acute ACD that initially present as pruritic erythema (stadium erythematosum), pruritic palpable infiltration, with or without formations of small and sometimes confluent larger blisters (stadium vesiculosum), subsequently crust formation (stadium crustosum) and a resolution with eczematous fine lamellar scaling (stadium squamosum). Chronic ACD is mostly characterized by a less prominent spongiosis and a more prominent acanthosis, hyper- and parakeratosis and a less prominent mononuclear infiltrate mostly in the upper dermis. Clinically, chronic lesions are typically characterized by pruritus, lichenification, erythema, scaling, fissures and excoriations.
Neither acute nor chronic ACD present with histological or clinical changes that definitely allow the differentiation of the type of insult that caused the dermatitis. The only clinical signs that are suggestive of ACD are disseminated small papular eczematous skin reactions that extend beyond the actual area of contact to the allergen. In contrast, irritant contact dermatitis (ICD) is usually sharply demarcated and restricted to the area of direct skin contact with the irritant.
Clinical manifestations of ACD can vary according to the anatomical location in which the contact allergen was encountered. Frequent locations are hands (in particular in occupational ACD), face and eyelids (often associated with use of cosmetics), lower legs (in particular in patients with topical treatment of leg ulcers), and perianal region (in particular in patients with topical treatment of pre-existing perianal dermatosis).
Clinical manifestations of ACD also vary based on the route of allergen exposure. The classical ACD usually begins in the area of direct skin contact. Since some of the contact allergens are volatile components, ACD may also primarily present in areas of airborne exposure such as the face, the neck and extremities. Examples of airborne contact allergens are composite plants allergens (Asteraceae), formaldehyde, expoxy resins, isothiazolones, fragrances, drugs and others [10–12].
Also systemic exposure to contact allergens either via enteral or via parenteral application can trigger ACD in sensitized individuals. Clinical examples of systemic ACD are patients sensitized to drugs (e.g., via epicutaneous exposure at the work place) that develop generalized dermatitis upon oral or parenteral application. This often presents with a characteristic clinical pattern as sharply defined symmetrical erythema of the gluteal/perianal area, and/or V-shaped erythema of the inguinal/perigenital area and in flexural or intertriginous folds. Due to the prominent involvement of the buttocks this presentation had previously been designated “Baboon syndrome”, a term that was more recently suggested to be replaced by the less derogative and more descriptive acronym SDRIFE, symmetric drug-related intertriginous and flexural exanthema [13]. Allergens reported to induce this drug-induced systemic ACD include betalactam antibiotics such as aminopenicillins, cephalosporins, but also a wide range of other drugs such as clindamycin, macrolides, mitomycin, cimetidine, naproxene, and pseudoephedrine [13]. Other examples of contact allergens that have been reported to induce ACD include oral intake of nickel, chromium and cobalt salts, inhalation of mercury vapours, andingestion of balsam of Peru. Clinically systemic ACD presents either as dermatitis flare-up in areas of previous contact with allergen, flare-up of previous positive patch test sites, or as dermatitis in previously unaffected skin [14].
Finally, ACD can also develop to substances that only in combination with exposure to ultraviolet radiation act as allergens/haptens. The mechanism of this photoallergic contact dermatitis involves photochemical reactions that lead to the generation of haptens or full allergens which in turn induce allergic sensitization and classical T cell-mediated hypersensitivity reactions upon subsequent exposure [15]. Examples of photoallergens include systemic drugs such as non-steroidal anti-inflammatory drugs (NSAID), diphenhydramine, phenothiazine and topically applied substances such as halogenated aromatic hydrocarbons (e.g., salicylanilides), hexachlorophene, and chemical components of sunscreens such as 2-hydroxy-4-methoxybenophenone, 4-isopropyl dibenzoyl methane, or para-amino benzoic acid. Photoallergic reactions differ from phototoxic reactions in which exposure to UV radiation leads to the generation of phototoxic substances that cause damage to epithelial, endothelial and immune cells in the vicinity without involving allergic sensitization and hapten/allergen-specific T cell responses. Classical examples of phototoxic substances include furocumarines (psoralens), amiodarone, sulfonamides and certain dyes such as acridine orange. Clinically, both photoallergic and phototoxic reactions are characterized by occurrence in skin areas that are exposed to UV radiation, and sparing of areas that are naturally less exposed such as the skin behind the ear lobes or under the chin. While phototoxic reactions are usually restricted to the area of exposure to the photosensitizer (e.g., bullous dermatitis pratensis induced by giant hogweed) photoallergic reactions may extend beyond the area of exposure.
Conflicting data exist concerning atopy as a potential predisposing factor for ACD [16–19]. The skin barrier defect and bacterial colonization may favor ACD due to enhanced penetration of chemical allergens and enhanced basal inflammation [19, 20]. Infection or tissue damage may facilitate sensitization by providing danger signals that activate the innate immune system (Fig. 23.1, 3) [21]. These danger signals are essential for ACD [22] and such heterologous innate immune stimulation may amplify the contact allergen-dependent, autologous danger signaling or even replace it (Fig. 23.2) [23].

Contact allergens and irritants cause tissue stress and damage. ROS are induced and stressed or damaged cells release and or/produce danger signals such as PRR-activating DAMPs. Additional danger signals are derived from the extracellular matrix. Consequently skin inflammation results and DCs are activated and migrate from the epidermis to the dermis and then to skin draining lymph nodes. Due to the chemical modification of proteins contact allergens form T cell epitopes that are presented on activated DCs in the lymph node and prime contact allergen-specific T cells. This concludes the sensitization phase of ACD. The recruitment of activated effector/memory T cells to the skin upon repeated contact with the contact allergen leads to eczema. Irritants cause eczema without induction of an allergen-specific T cell response

Heterologous innate immune stimulation. Contact allergens can directly or indirectly provide autologous innate immune stimulation for example by triggering TLRs leading to activation of NF-kB and production of inflammatory cytokines and DC activation and migration. Heterologus innate immune stimulation can be provided for example by infection (e.g., PAMPs), tissue damage (DAMPs), irritants and other contact allergens that trigger the same signaling pathways via the same or different TLRs. As a result autologous innate immune stimulation can be amplified or – when absent – be substituted by heterologous innate immune stimulation. Due to T cell epitope formation by the contact allergen a T cell response is induced by activated DC when the innate immune stimulation is sufficiently strong. Upon repeated allergen contact contact allergen-specific effector/memory T cells enter the skin and exert effector function such as cytokine production and cytotoxicity
Diagnosis of Allergic Contact Dermatitis
The diagnosis of ACD is ideally based on the patient’s history, the clinical presentation and a positive patch test reaction to the suspected contact allergen. In every day practice this ideal situation is rarely present. The clinical presentation, the affected areas and the distribution may be suggestive of ACD, while morphological skin changes and histology do not allow a definite differentiation between ACD and other forms of dermatitis, such as ICD, atopic dermatitis or seborrheic dermatitis. For the identification of relevant contact allergens a detailed patient history is of utmost importance. This must include detailed information on the work environment, recreational activities, medication, use of cosmetics, emollients, detergents and other substances that the patient has been exposed to prior to the onset of the dermatitis.
The mainstay for the diagnosis of ACD is the patch test in which under standardized conditions contact allergens are applied to the healthy skin of the patient with the goal to reproduce the allergic eczematous skin reaction. Prerequisite for patch testing with suspected contact allergens is that skin reactions during acute or chronic ACD have been sufficiently controlled or even better resolved by topical or systemic anti-inflammatory treatment. Patch testing during ongoing ACD produces increased numbers of false positive patch test reactions and thus should be avoided.
The standard procedure of the patch test involves application of the contact allergen in the corresponding vehicle (vaseline for lipophilic, aqueous solution for hydrophilic allergens) in a Finn chamber to the skin (usually skin of the back) of the patient for 24 h or 48 h. The first reading is taken at 48 h, a second reading is recommended at 72–96 h after initiation of the test. Standardized criteria for reading the patch test reactions have been developed by the DKG and allow a grading and interpretation of the reaction (Table 23.1). Like all test systems the patch test has also a number of pitfalls and limitations and may generate false positive or false negative results. False positive results may occur in patients in whom the ACD has not sufficiently been treated or in patients that display a very strong sensitization. In these situations multiple chemically non-related allergens can induce false positive reactions. This phenomenon is described as “angry back” or excited skin syndrome and most likely reflects the fact that the skin displays reduced thresholds to the irritative capacity of these unrelated allergens.
The majority of contact allergens has an intrinsic capacity to activate mechanisms of the innate immune response and in this sense can act as irritants. Since this effect is concentration-dependent, using the optimal test concentration of the contact allergen is crucial for the interpretation of the test results. To optimize the performance, test conditions for the most common contact allergens have been standardized. Since relative allergenic and irritative potential of contact allergens can vary a great deal, attempts have been made to classify allergens into those that have a higher irritative than allergenic capacity and those that have a high allergenic and little irritative potency. Calculation of the reaction index (RI) which analyzes the relationship between number of positive patch test reactions and number of questionable or irritant reactions was suggested by the IVDK a parameter to assess the quality of patch test preparations [24, 25]. Similarly, an additional parameter, the positivity ratio (PR) which is defined as the frequency of + reactions among the total number of positive patch test reactions (+ to +++), was developed to be used in combination with the RI to identify problematic allergens [26]. Even though subsequent evaluation of both parameters by a Danish group has challenged the general applicability of this concept [27] it clearly demonstrates that interpretation of the patch test reactions very much depends on the type of allergen tested.
Similarly, false negative reactions may be related to low allergen concentrations in the test preparation or reduced or altered skin permeability. In particular, weak contact allergens that may elicit ACD in sensitive skin areas such as the eyelids, may not be detected when tested on the back skin of the patient. Similarly, weak contact allergens may elicit ACD in areas with a preexisting damage of the barrier function, while they are not strong enough to elicit a reaction on the intact skin of the back. Since the epidermal barrier is crucially involved in determining the level of allergen penetration, modification of the patch test by tape stripping the upper layers of the epidermal stratum corneum prior to allergen application may be used to simulate particularly sensitive or damaged skin areas. Even though this approach has recently been standardized and shown to increase test sensitivity in particular to weak contact allergens [28, 29] interpretation needs to be done very carefully in particular in relation to irritative test reactions which occur more frequently under these conditions.
Both positive or negative test reactions may be re-evaluated by a repeated open application of the suspected substance [30, 31]. Often positive test reactions are observed that are of questionable relevance. They may simply indicate that the patient is sensitized but not necessary allergic to the substance. In this case the substance of interest can be applied twice daily to a 2 × 2 cm area of the cubital skin for consecutive 7 days after which ACD should develop provided that the contact sensitization is clinically relevant. The same approach can be taken when a strongly suspected substance gives a negative patch test reaction or is not available or suitable for occlusive patch testing.
Finally, when photoallergic reactions are suspected a modified patch (photopatch) test may be applied in which two identical panels of allergens are applied to the back skin for 24 h and subsequently one panel is irradiated with UVA (5–10 J/cm2), while the other panel is protected from UV radiation. The test readings are performed at 48, 72 and 96 h according to the same criteria as the standard patch test and allow addressing the role of UV light for the elicitation of the ACD [32].
Treatment of Allergic Contact Dermatitis
Since in the majority of the cases ACD presents as a localized skin reaction and the inflammatory skin infiltrate is accessible to topical treatment, the use of topical glucocorticosteriods applied to the affected skin areas is the mainstay of ACD treatment. In cases of extended skin involvement or generalized ACD short term systemic therapy with glucocorticosteriods may be considered. The topical treatment of ACD corresponds to treatment of other forms of dermatitis. The vehicles used for topical glucocorticosteriod treatment should be adapted to the clinical presentation and state of the eczematous skin reaction. Acute dermatitis requires treatment with hydrophilic creams and/or lotions that provide a cooling and anti-inflammatory effect and help to dry acute weeping or blistering skin lesions. In contrast, chronic dermatitis is usually characterized by dry and brittle skin with lichenification and hyperkeratosis and thus requires more lipophilic vehicles such as lipophilic creams or ointments. In cases of prominent hyperkeratosis in particular on palms and soles the keratolytic effects of salicylic acid or urea may be used to reduce the hyperkeratosis and thus allow better access of the topical anti-inflammatory agents. In case of dermatitis with bacterial superinfection, anti-infective agents such as octinidine or polyhexanide may be used. Supportive measures should include minimizing irritative insults to the skin such as chronic exposure to wet conditions at the work place or repeated hand washing. Since allergic sensitization and elicitation of ACD requires for a variety of allergens some sort of adjuvant irritative effect or skin damage as cofactor to fully develop, reduction of this kind of aggravating cofactors will help to improve the skin condition and to avoid relapses. The mainstay of the treatment of ACD is the anti-inflammatory therapy with topical glucocorticosteriods in the correct vehicle. Topical calcineurin inhibitors such as tacrolimus or pimecrolimus can also be effective, and due to an almost absent induction of skin atrophy may be considered in chronic patients that already have steroid-damaged skin. In patients in whom steroid therapy is not appropriate, UVB or PUVA phototherapy may be an effective alternative. In particular in patients with localized chronic hand dermatitis crème PUVA therapy has proven to be a valuable and well standardized therapeutic option.
However the treatment can only be successful if the offending allergen is avoided. So great care should be taken to identify the relevant allergen and large efforts must be taken to explain the necessity of allergen avoidance. In particular in work related contact allergies this may mean leaving the workplace for good and/or changing the profession. The best prophylaxis of ACD is the complete avoidance of the contact allergen, which in many cases is not possible. In addition, risk factors to develop ACD, such as chronic skin damage that leads to a reduced skin barrier function, should be avoided and/or treated. In the same line of thought, consequent basic skin care using rehydrating lipophilic creams or ointments should be recommended to prevent impairment of barrier function. In addition, the use of barrier creams can be recommended for some allergens and irritants that prevent or reduce penetration of the offending agent.
Finally, animal experiments suggest that in ACD specific tolerance can be induced. Attempts to induce contact allergen specific tolerance in humans have been reported, however only for certain plant allergens like poison ivy [33]. Overall the effects were rather transient and the clinical benefit was not convincing. Similarly oral tolerance induction to nickel has been reported that caused an amelioration of skin manifestation, a reduced skin test reactivity to nickel and a reduced T cell reactivity upon nickel restimulation [34]. Again effects were rather moderate and transient in nature. In summary, so far no effective and lasting allergen specific tolerance induction has been established in humans.
Risk Factors Predisposing to ACD
Many factors may contribute to the susceptibility to ACD. Up to now, genetic studies have not revealed an association of ACD with specific HLA alleles. However, several gene polymorphisms have been identified [35]. These are found in genes regulating skin barrier function, detoxification, innate inflammatory immune responses and T cell responses. Several polymorphisms in the stratum corneum protein filaggrin (FLG) have been found to impact its function and to impair the barrier function of the skin [36]. FLG mutations have been associated with increased susceptibility to atopy [37, 38] but also to ICD and ACD [39, 40]. FLG-deficient mice exhibit increased antigen penetration and exacerbated CHS responses triggered by the irritant croton oil or the contact allergen DNFB [41].
Chemistry and Contact Dermatitis
Contact allergens are low molecular weight chemicals that share one characteristic feature: they are protein-reactive. Due to their small size the chemicals per se cannot be recognized by the immune system and are therefore also designated haptens (half-antigens). Their protein binding is essential for their immunogenicity and antigenicity. Organic chemical allergens can covalently bind to proteins, and metal ions form complexes with proteins. Some contact allergens are not reactive haptens but are pre-haptens which require oxidation or pro-haptens which require metabolic conversion to full haptens. Such chemicals are highly problematic in terms of contact allergen identification in patch testing and in in vitro assays since an adduct and not the parent compound causes sensitization and ACD [42].
A detailed understanding of the relation between the physico-chemical properties, structure and reaction mechanisms and their biological activity is used to develop in silico prediction methods to identify potential contact sensitizers in so-called quantitative structure-activity relationship (QSAR) approaches. Grouping according to so-called mechanistic domains [43, 44] is being analysed with respect to allergenicity and allergenic potency. In a recent study allergenic potency as determined in the mouse local lymph node assay (LLNA) could be correlated with mechanistic domains. The results of that study showed that the more potent contact allergens triggered a broader range of signaling pathways than the less potent ones [45]. These data are encouraging further investigations using QSAR and mechanistic domains to promote our understanding of the relation of the chemistry of contact allergens and its impact on the immune system.
Functional Consequences of Protein Modification by Contact Allergens
The most fascinating question that remains to be solved is how the chemical reactivity of contact allergens is translated into biological responses that can lead to the development of ACD. The interaction of chemicals with biomolecules can alter their function. Since contact allergens are generally chemically reactive electrophiles or complex-forming metal ions, it is to be expected that this reactivity is responsible for their action as allergens. In fact, neutralizing the reactivity of the strong contact allergen 2,4-dinitrochlorobenzene (DNCB) by coupling it to lysine abrogates its ability to induce CHS (our unpublished data). Hypothetically, contact allergens may mimic or interfere with conventional post-translational protein modifications [46].
The chemical reactivity of contact allergens regulates immunity at two levels: the first level is the induction of signaling cascades due to chemical protein modification and the second, resulting level is the regulation of gene expression. Information regarding the identity of the functionally relevant chemically modified proteins is scarce. In one study it was demonstrated that treatment of the human monocytic leukemia cell line THP-1 with the contact allergen DNFB does not modify all cellular proteins but only some which are not necessarily the most abundant proteins [47]. Thus, there is selectivity in the targeting of proteins by contact allergens. New studies begin to analyse contact allergen-modified proteins in 3D skin models. In a recent study high resolution magic angle spinning (HR-MAS) nuclear magnetic resonance (NMR) spectroscopy was used to identify protein modifications by a 13C-labeled electrophile in reconstructed human epidermis (RHE) [48]. Compared to in vitro modification of human serum albumin (HSA) which took several days to be detectable, the in situ protein modification in RHE was detectable after less than 24 h. The predominant lysine modification of HSA, as observed in vitro, was not detected in RHE. This method will be useful to identify contact allergen-modified adducts formed in the skin. Eventually this technique may promote the identification as well as quantitative and qualitative analysis of the contact allergen-modified proteome.
Up to now, only very few proteins, whose modification by contact allergens induce a biological response, have been identified (Fig. 23.3). Human TLR4, the receptor for lipopolysaccharide (LPS, endotoxin) from the cell wall of Gram-negative bacteria, is complexed and dimerized by the metal ions Ni2+, Co2+ [49, 50]. Pd2+ also interacts with human TLR4 [51]. This results in signal transduction for production of inflammatory mediators in the absence of LPS. The cytosolic, cysteine-rich sensor protein for oxidative or electrophilic stress, Keap1, contains cysteine residues that can be modified by contact allergens. This triggers expression of anti-oxidant phase 2 response- and immune genes due to their activation by the Keap1-regulated transcription factor Nrf2. The promoters of these genes harbor an antioxidant response element (ARE). This pathway limits contact allergen-triggered inflammation. Mice lacking Nrf2 have a much lower sensitization threshold for contact allergens, most likely due to an increased level of pro-inflammatory oxidative stress [52, 53]. A third target for modification by electrophilic contact allergens is the ion channel transient receptor potential ankyrin 1 (TRPA1). TRPA1 also harbors cysteines that are attacked by contact allergens such as cinnamic aldehyde or DNCB [54, 55]. Extracellular Ca2+ can then enter the cell. TRPA1 is expressed on a subset of nociceptive nerve fibers, also in the skin, but also on keratinocytes and endothelial cells. The TRPA1 channel is involved in pain but also in itching in inflammatory immune responses [56]. For atopic dermatitis it has been shown that TSLP produced by Th2 cells acts on sensory neurons in the skin to cause itch in a TRPA1 dependent manner [57]. TRPA1-deficient mice show reduced edema, inflammation and itching in cinnamic aldehyde-induced edema in mouse ear skin or in CHS to oxazolone and urushiol [58]. Interestingly, one of the endogenous agonists of TRPA1, 4-hydroxy-2-nonenal (HNE), is produced as a consequence of ROS-mediated oxidation of membrane phospholipids [59]. ROS are important inflammatory mediators in CHS [60].

Direct activation of signaling cascades by contact allergens. The metal ions nickel and cobalt form complexes with conserved histidines in human TLR4 resulting in TLR4 dimerization and signaling via NF-kB and MAP kinases and production of inflammatory mediators. Organic chemical allergens such as TNCB or DNCB bind covalently to cysteine residues in the cytosolic protein Keap1. This leads to release of the transcription factor Nrf2, its nuclear translocation and transcriptional activation of the expression of genes containing antioxidant response elements (ARE). These contact allergens can also bind to cysteines in the calcium channel protein TRPA1. Calcium influx activates pathways involved in itch and inflammation
Innate Immune Responses in Allergic Contact Dermatitis
The induction of ACD requires the priming of contact allergen-specific T cells. This depends on two crucial events: activation of the innate immune system and formation of T cell epitopes (Fig. 23.1). It is a peculiarity of contact allergens that they have this dual function [46]. The activation of the innate immune system results in skin inflammation. The most important outcome of this innate inflammatory response in the sensitization phase is the activation and polarization of skin DCs allowing their migration to the draining lymph nodes and presentation of contact allergen to T cells in the context of MHC molecules. Naïve, contact allergen-specific T cells are then primed and polarized towards a Tc1/Th1, Tc17/Th17 phenotype. In the elicitation phase, the innate inflammatory response results in the secretion of cytokines and chemokines, up-regulation of adhesion molecules on endothelial cells and eventually the recruitment of effector or memory T cells into the skin where they exert their effector function to produce ACD.
Recent studies in the mouse CHS model have uncovered mechanistic details of the cellular and molecular innate immune response [22, 61, 62]. The emerging picture clearly indicates that the immune system reacts to contact allergens as if they were infectious agents. This is due to the fact that contact allergens activate the same anti-infectious immune response mechanisms as viruses and bacteria.
The innate cellular response to contact allergens is initiated in the epidermis by activation of keratinocytes and Langerhans cells. Here, the innate inflammatory response is essential to abrogate the naturally tolerogenic milieu in the skin as a major immunologic barrier. As a consequence the normally tolerogenic Langerhans cells are switched to an immunogenic phenotype allowing lymph node migration and T cell priming [63, 64]. Despite the fact that Langerhans cells are dispensable for CHS in some experimental models which usually use saturating contact allergen concentrations, they most likely play a role in ACD under physiological conditions, especially at low contact allergen concentrations and absence of spreading to the dermis [65–67]. Further analysis of the orchestration of the cellular innate immune response has identified mast cells as important initiators of skin inflammation [68]. Mast cell deficiency or mast cell depletion before sensitization significantly reduces CHS in mice. This is due to a role of histamine from mast cells in increasing the permeability of the blood vessels in the skin. The absence of mast cells decreases the infiltration of neutrophils and the emigration of DCs from the skin. Neutrophil depletion efficiently abrogates CHS as does the depletion of subsets of skin DCs [66, 67, 69–71]. Both the sensitization and elicitation phase of CHS depend on the presence of neutrophils [71]. The fact that depletion of one or the other cell type has a similar outcome underlines the essential collaboration of the different innate immune effector cells. The same principle is seen in the orchestration of the molecular mechanisms of contact allergen-induced innate immune responses [46].
Pathogens are recognized by the innate immune system via so-called pattern recognition receptors (PRRs) which are triggered by pathogen- or microbe-associated molecular patterns (PAMPs, MAMPs). Examples for families of PRRs are the Toll-like receptors (TLRs), transmembrane proteins in the plasma membrane or endosomal membranes, the cytosolic NOD-like receptors (NLRs), the RIG-I like receptors (RLRs) and C-type lectin receptors (CLRs) in the plasma membrane [72].
PAMPs/MAMPs can be bacterial cell wall components, flagellin, viral and bacterial nucleic acids, lipids and carbohydrates. These are perceived as danger signals by PRRs and induce innate anti-infectious immune responses. Contact allergens can also trigger PRRs by direct or indirect mechanisms [61]. Nickel- and cobalt ions bind to conserved histidine residues of human TLR4 inducing dimerization and signaling [49, 50]. The murine TLR4 lacks these histidines and therefore is not triggered by Ni or Co. This results in resistance of mice to CHS to these metal ions. However, replacement of the murine TLR4 by the human TLR4 in transgenic mice renders these mice susceptible to CHS [49]. Up to now this is the only known case where contact allergens are directly activating a PRR. For other contact allergens, organic molecules such as 2,4,6-trinitrochlorbenzene (TNCB) or 2,4-dinitrofluorobenzene (DNFB) or oxazolone an indirect activation of PRR has been demonstrated [60, 73, 74]. These contact allergens induce endogenous danger signals. A rapid induction of ROS and release of ATP from skin cells has been revealed [60, 74]. Moreover, the degradation of the extracellular matrix (ECM) component hyaluronic acid (HA) results in fragments that can activate TLR2 and TLR4 [60]. Constitutive overexpression or induction of expression of human hyaluronidase 1 in mouse skin under control of the K14 promoter resulted in lack of CHS when expression was induced before sensitization, most likely due to DC depletion from the skin. CHS was enhanced when overexpression was induced at the time of sensitization [75]. HA breakdown resulted in the emigration of DCs from the skin. The HA effects were dependent on TLR4. These data show a TLR4-dependent role of HA fragments for the mobilization of DC from the skin. The pro-inflammatory role of HA breakdown is evident in Shar-Pei dogs who accumulate HA over time due to an overexpression of hyaluronan synthetase (HAS) 2. Periodic breakdown of accumulated HA results in a periodic fever syndrome in these dogs [76]. These findings illustrate the important role of the ECM in innate immunity [77].
The endogenous danger signal high mobility group box 1 (HMGB1) is involved in the in vitro induction of IL-18 in the human keratinocyte cell line NCTC2544 [78]. HMGB1 was released upon treatment of the cells with the contact allergens para-phenylene diamine (pPD), DNFB or citral.
While ATP triggers the activation of the cytosolic NLPR3 inflammasome that induces the maturation of immature pro-IL-1β and pro-IL-18 via caspase-1, ROS contribute to skin inflammation for example by triggering oxidative HA breakdown and by promoting TLR signaling and inflammasome activation. Nickel also activates the NLRP3 inflammasome [79].
A recent study [80] demonstrated that mice lacking MyD88 or CARD9 are resistant to CHS to TNCB. Irritant CHS to SLS was normal. While MyD88 is an adaptor protein involved in TLR/IL-1R signaling, CARD9 is an adaptor that plays a role in the signaling of CLRs. The study clearly showed that the contact allergens TNCB/TNBS, DNFB and oxazolone can trigger ITAM-Syk-Card9/Malt10 signaling in DCs in vitro resulting in IL-1α and IL-1β production. Signaling was dependent on the ITAM containing adaptor protein DAP12. Syk phosphorylation and CARD9/Bcl-10 mediated NF-kB activation resulted in the production of immature pro-IL-1α and -IL-1β. ROS formation and ROS mediated NLRP3 inflammasome activation for the production of mature IL-α and IL-1β in DCs was Syk-dependent but independent of CARD-9/Bcl-10. The DC-mediated priming and differentiation of contact allergen-specific IFN-γ and IL-17-producing effector T cells was dependent on IL-1β and MyD88. It remains to be determined if and which receptor (e.g., a CLR), couples to this signaling pathway and how it is activated by contact allergens. Moreover, the molecular mechanisms of crosstalk of this signaling pathway with the TLR pathway remain to be determined.
Further important signaling pathways have been identified by genomic or proteomic profiling studies using human cell lines. Two prominent pathways are the aryl hydrocarbon receptor (AhR) and the Keap1/Nrf2 pathway [81]. The AhR is a transcription factor that regulates not only detoxification pathways but also immune processes such as Langerhans cell function and Th17 differentiation. Dietary and endogenous ligands have been identified that modulate immune function [82] and evidence for contact allergen-mediated activation of the AhR has been provided [83].
Disturbed epidermal homeostasis involving keratinocyte death promotes skin inflammation [84] Here, the NF-kB pathway plays an important regulatory role. Mice with an epidermis-specific loss of the NF-kB subunit RelA did not develop spontaneous inflammation. However, DNFB- and oxazolone-induced allergic CHS was aggravated while croton oil-induced irritant CHS developed as in wild type mice [85]. The loss of RelA leads to up-regulation of the small calcium-binding proteins S100A8/A9. These proteins are up-regulated in inflammatory and autoimmune diseases and can have pro-inflammatory, but also anti-inflammatory activity by acting as ligand for TLR4 [86–88]. Increased keratinocyte apoptosis and up-regulation of XIAP associated factor 1 (XIAF1) were observed for contact allergens and croton oil. XIAF1 blocks the anti-apoptotic function of X-linked inhibitors of apoptosis (XIAPs). It was speculated that the selective aggravation of contact allergy may be due to an effect of the contact allergen-specific T cell response on the proliferation of keratinocytes. The nuclear hormone receptor peroxisome proliferator activated receptor (PPAR)-α is involved in the regulation of keratinocyte proliferation and differentiation as well as inflammation. PPAR-α is expressed in keratinocytes but also in Langerhans cells, mast cells and T cells. Its activation can inhibit NF-kB activation [89]. Topical treatment of mice with PPAR-α ligands such as clofibrate counteracts keratinocyte hyperproliferation [90] and reduces TPA-induced irritant CHS and oxazolone-induced allergic CHS. This correlated with a reduction in the levels of TNF-α and IL-1-α [91]. PPAR-α-deficient mice had exacerbated CHS which was associated with impaired IL-2 production in lymph nodes and a decrease in regulatory T cell (Treg) numbers and function [92]. Interestingly, an endogenous PPAR-α ligand, palmitoyl ethanolamide (PEA), is up-regulated along with PPAR-α by contact allergens [93]. These findings underline the importance of dysregulated keratinocyte homeostasis for inflammatory skin diseases.
Many of the mechanisms described above for contact allergens can also be triggered by chemically reactive drugs or drug metabolites. N-acetyl-p-benzo-quinoneimine (NAPQI), the toxic metabolite of acetaminophen is involved in drug-induced liver injury. It can damage hepatocytes. These release self-DNA which acts as DAMP and activates TLR9 on sinusoidal endothelial cells. ROS and ATP then contribute to activation of the NLRP3 inflammasome [94, 95]. Moreover, NAPQI can also activate TRPA1 [96].
The polarization of the cytokine profile secreted by skin DCs is an essential step in the development of ACD. Polarization of T cells towards a Th1/Tc1 phenotype requires IFN-γ and IL-12 or IL-18, IL-21 and IL-27 whereas the polarization of Tc17/Th17 cells requires IL-6 and TGF-β or IL-6, IL1-β and IL-23 [97]. The innate immune response is certainly instrumental in this polarization process. However, there is also evidence for chemical-intrinsic properties that contribute to that [98, 99]. It was observed that the contact allergens DNFB and DNCB induced a type 1 cytokine profile (IFN-γhi, IL-4/-5/-10lo) in the skin draining lymph nodes following topical exposure of Balb/c mice. In contrast, the respiratory allergen trimellitic anhydride (TMA) as well as FITC and DNBSCl induced a type 2 profile (IL-4/-5/-10hi, IFN-γlo). Interestingly, these cytokine profiles correlated with the modification of proteins. In vitro studies using human U937 monocytes showed preferential modification of cellular proteins by DNFB and DNCB, but preferential modification of serum proteins by the other chemicals [100].
A modulation of the epigenetic regulation of gene expression has also been discussed in the context of T cell polarization [101]. A first study analyzed genome wide changes in the methylation of DNA from skin draining lymph nodes of Balb/c mice exposed to DNCB or TMA [102]. Characteristic changes were found for both chemicals with differently methylated regions in various pathways including cytokine and chemokine genes. Future studies using T cells or DCs are needed to identify potential methylation signatures that are specific for contact or respiratory allergens.
Mechanisms of Irritant Contact Dermatitis
Unlike ACD, ICD is caused by chemicals that are not covalently binding to proteins or form complexes with proteins like metal ions do. Chemicals such as detergents, acids, bases and solvents with a variety of physico-chemical properties cause a toxic-irritant skin eczema that may evoke pathologically relevant stress or damage to the skin barrier (Fig. 23.1) [103]. Innate inflammatory immune responses also play a role in ICD but adaptive immunity is not involved. The underlying cellular and molecular mechanisms are not well understood. From the CHS model it is known that ICD to the irritant croton oil is absent in mice lacking TLR4 and IL-12Rβ2 or TLR2 and TLR4 (our unpublished data) but is normal in mice lacking P2X7R [74]. SLS induced CHS is normal in mice lacking MyD88 or CARD9 [80]. Addition of croton oil to sub-sensitizing doses of TNCB or oxazolone is not able to compensate the lack of sufficient innate immune stimulation in the CHS model [104]. On the other hand, addition of SLS to the tolerogen/weak contact allergen restores IL-1β production and prevents 2,4-dinitrothiocyanobenzene (DNTB)-mediated tolerance induction to DNFB [105]. These data suggest that there are contact allergen-specific signaling pathways that cannot be triggered by some irritants. In addition, other pathways are triggered by irritants and there may also be irritant-specific pathways not triggered by contact allergens. Due to the essential irritant effect of contact allergens that is required to induce skin inflammation, it is not surprising that there is an overlap of cytokine and chemokine profiles induced by irritants and contact allergens [106, 107].
Differences between contact allergens and irritants are for example the selective up-regulation of CXCR4 on Langerhans cells by contact allergens. This leads to chemokine-selective migration of LCs to the dermis: LC migration in response to contact allergens is driven by CXCL12 while migration in response to irritants is driven by CCL2 and CCL5 derived from dermal fibroblasts [108, 109]. A recent study revealed a role for basophils in attracting eosinophils in a mouse model of croton oil-induced ICD [110]. Eosinophil-deficient mice had impaired, IL-5-transgenic mice exacerbated ICD. In an in vitro co-culture model basophils secreted IL-4 and TNF-α, and promoted CCL11 expression from fibroblasts. These data suggest a role for basophils in the maturation and attraction of eosinophils to the skin in ICD. Their contribution to production of pro-inflammatory ROS was discussed. Interestingly, basophils and eosinophils are found in other inflammatory human skin diseases including ACD [111–113].
These findings highlight common principles for the immune response to chemicals. Contact allergens, protein-reactive drugs or their reactive metabolites and irritants cause tissue stress and damage. This leads to oxidative stress and the formation of DAMPs, release of DAMPs from stressed and damaged cells and the activation of downstream signaling events that are in part mediated by PRRs. The chemical reactivity of contact allergens and protein-reactive drugs causes the chemical modification of proteins which can result in the direct activation of signaling cascades as is the case for human TLR4, Keap1 and TRPA1 and in in the formation of T cell epitopes. The former leads to innate immune responses resulting in xenoinflammation which is essential for the subsequent activation of the adaptive immune system and the generation of contact allergen- or drug-specific effector and memory T cells [22].
Heterologous Innate Immunity
Contact allergens and irritants are rarely encountered as pure, single substances. Consumer products such as cosmetics, household products or occupational chemicals such as paints or metal cutting fluids often contain combinations of irritants and contact allergens with other chemicals. This combination is of great relevance. The interaction of the different chemicals may result in enhanced skin penetration or augmentation of sensitization and challenge reactions. Facilitated sensitization may be the result [114–116]. Examples are the augmentation effects by combinations of irritants and contact allergens or several contact allergens [117, 118]. Mechanistically, this can be explained based on the specificity of the innate immune response. Due to the activation of identical signaling pathways by different TLRs or other PRRs, a given contact allergen can generate signals for example via TLR4 and these may be amplified by irritants or other contact allergens that also trigger TLR-dependent inflammation. The result is a T cell response and ACD to this contact allergen. If the autologous innate signals triggered by the contact allergen that elicits the T cell response are too weak, augmentation by heterologous innate immune stimulation by irritants or other contact allergens is possible (Fig. 23.2). Moreover, such heterologous innate stimuli may replace missing autologous stimulation. Heterologous innate immune stimulation can also be provided by infections. This may even break tolerance or abrogate genetically based resistance to contact allergy as shown in the CHS model. Here mimicking an infection renders CHS-resistant TLR4/IL-12Rβ2 deficient mice susceptible to CHS. Injection of contact allergen-modified DCs from these mice fail to induce sensitization in wildtype mice. Stimulation of their TLR9 with CpG-oligodeoxynucleotides (CpG-ODN) in vitro restores their sensitizing potential [73]. Likewise, CpG-ODN injection of the CHS-resistant mice at the time of sensitization with contact allergen also abrogates resistance (our unpublished data). Combining nickel which does not trigger mouse TLR4 with LPS allows to efficiently sensitize mice for CHS to nickel [119] and amplifies patch test reactivity [120]. These data highlight the importance of heterologous innate immune stimulation as a process that significantly impacts the outcome of immune responses to chemicals depending on their context [23].
Adaptive Immune Responses in ACD
ACD develops in two phases. The first, sensitization phase is initiated upon skin contact with a chemical allergen. The contact allergen penetrates into the skin and due to its reactivity binds to extracellular, plasma membrane-associated and intracellular proteins. T cells specific for organic chemical contact allergens such as TNCB recognize hapten-modified peptides on MHC molecules [121]. Metal ions such as nickel are recognized by T cells due to complex formation of the metal ion with histidine residues in the MHC molecule and the T cell receptor. For some T cell clones one coordination site is a histidine residue in the peptide bound to the MHC molecule, for others this not the case [122, 123]. The effector T cells in ACD are CD4+ and CD8+ T cells. In the mouse CHS model the effector T cells are usually cytotoxic CD8+ T cells that produce IFN-γ. Moreover, CD8+ IL-17 producing T cells play a role in ACD [113, 124, 125]. In the mouse CHS model a role for dendritic epidermal T cells (DETC) as producers of IL-17 has been described [126] and the ASK1/p38 MAP kinase pathway was shown to be involved in IL-17 production in the elicitation phase of CHS [127]. In human ACD there is some evidence for early infiltrating CD8+ T cells that may cause initial damage. This is similar to results from atopy patch tests [128]. CD4+ T cells are then also detected later. Other effector cells in ACD are infiltrating NK cells that amplify the response due to their IFN-γ production [129]. In the CHS model evidence for contact allergen-specific NK cell responses and solely NK cell-mediated CHS-like reactions in T-cell deficient mice has been provided [130, 131]. However, these reactions seem to be quite different from T cell-mediated CHS [132].
Down-regulation of the immune response in ACD is determined not only by effector T cell death but also by regulatory immune cells such as Treg. In the CHS model ICOS + CD4 + CD25 + Foxp3+ Treg have been identified and a critical role for Langerhans cells in Treg induction has been identified [63, 133]. Invariant NKT cells (iNKT cells) also have regulatory function in CHS [134]. More recently, PU1 + CD4+ Th9 cells have been isolated from ACD skin biopsies of nickel allergic patients [135]. They may have a regulatory role in ACD by acting on Th1 cells directly or via enhancement of IL-4 production by Th2 cells. Interestingly, IL-9 was increased after skin exposure to nickel, rubber and fragrance in a gene expression profiling study of skin biopsies from allergic patients [136].
Tolerance Induction to Contact Allergens
Induction of allergen-specific tolerance is a major goal of the immunotherapy of allergic diseases. Hyposensitization can re-establish allergen tolerance for some years in type I allergies for example to insect venoms, house dust mite and pollen allergens. Immunotherapy (IT) involves the application of increasing doses of the allergen via the subcutaneous (SCIT) or sublingual (SLIT) route. Allergen peptides or recombinant allergens are now also used [137]. The underlying mechanisms involve a shift in the balance between allergen-specific Th2 cells and Treg as well as other regulatory cells such as regulatory B cells, including the de novo induction of such regulatory cells [138]. For ACD there are up to now no established protocols to induce contact allergen-specific tolerance and studies in the CHS model show successful tolerance induction only before sensitization. The clinical problem is therefore not solved, yet [139]. In the CHS model, low zone tolerance (LZT) has been studied for many years. LZT is induced before sensitization and results from the repeated application of contact allergen at doses 100- to 1000-fold below the dose required for sensitization. Recent work has revealed that tolerogenic CD11c + DCs induce contact allergen-specific CD8+ Treg [140]. IL-10 producing CD4 + Foxp3+ Treg were essential for LZT induction and rendered CD11c + DC tolerogenic by direct cell-cell contact via gap junctions. In addition, in the skin draining lymph node, DCs produce TNF-α, which induces the death of effector T cells [141].
The tolerogenicity of contact allergens can be dose-related as in the case of LZT or intrinsic as in the case of DNTB which is a very weak contact allergen and used as a tolerogen. The common principle is most likely the lack of induction of a productive innate immune response. This fails to overcome the homeostatic immunoregulatory default which maintains tolerance and induces active contact allergen-specific tolerance involving DCs and regulatory T cells. The latter occurs due to the fact that T cell epitopes can still be formed by low dose contact allergen or weak contact allergens/tolerogens such as DNTB. The contact allergen is then presented on immature/tolerogenic DCs which results in the induction of CD4+- or CD8+ Treg and the induction of effector T cell anergy and death [63, 140, 141]. The central importance of the innate immune response in shifting the balance between tolerance and immunity was demonstrated by the fact that the irritant SLS was able to prevent tolerance induction by DNTB [105]. The combination of SLS, a heterologous innate immune stimulus [23], with DNTB induced IL-1β. DNTB alone failed to do so.
These findings clearly show that the magnitude of the innate inflammatory immune response is a critical determinant of tolerance and immunity and, most likely, of allergenic potency [142]. It remains to be tested whether tolerogenic adjuvants may be successful as negative heterologous innate stimuli in the re-establishment of tolerance to contact allergens [23]. A major issue is the tolerization of effector and memory T cells. A combination of anti-inflammatory therapies and strategies targeting effector/memory T cells and inducing contact allergen-specific regulatory T cells should be promising.
Biomarker Identification, Gene Signatures
The identification of changes in gene and protein expression induced by contact allergens and irritants will provide important information regarding the mechanisms of action of these chemicals. Pathway analysis can then be used to validate the pathologically relevant pathways and to identify drug targets for new, causative therapies. In addition, characteristic gene signatures can be identified that allow identification of contact allergens and their discrimination from irritants. The classification of chemicals based on physico-chemical and reaction-mechanistic characteristics will reveal whether the gene and protein expression profiles segregate with these characteristics. Dose-response studies will also be important in this context in order to understand the regulation of the balance between immunity and tolerance by contact allergens.
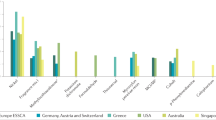
A recent study has provided such initial results from the genomic profiling of patch test biopsies for nickel, fragrance and rubber [136]. One hundred forty-nine genes were commonly regulated by all contact allergens compared to petrolatum as control. Differences between the allergens were observed for their efficiency in the induction of innate immunity and Th1/Th2/Th17/Th22 responses. Another recent genomic profiling study focused on the intra-individual comparison of skin lesion for psoriasis and non-atopic or atopic eczema in patients with both diseases, but also provided data on nickel-induced contact dermatitis [143]. Induced ACD could be differentiated from naturally occuring eczema by the selective down-regulation of late epidermal differentiation markers such as late cornified epithelial (LCE)1 and LCE2 family members, selective up-regulation of adhesion molecules such as ICAM-1 and of extracellular matrix associated HAS3 and epithelial-stromal interaction 1 (EPSTI1) the expression of which is modulated by inflammatory cytokines. Moreover, inflammasome components and neutrophil attracting chemokines were up-regulated in ACD. These studies mark the beginning of future genomic and proteomic studies that will hopefully identify chemical class-specific biomarker signatures for the identification of drug targets, improvement of diagnostics and development of in vitro assays for the identification of contact allergens.
A genome-wide association study (GWAS) with volunteers exposed to the irritants SLS and nonanoic acid revealed differential expression of 883 genes for the two irritants. Only 23 genes were commonly regulated by both chemicals [144].
These data highlight the importance to consider chemical-specific mechanisms. Especially in the case of irritants, it should be rewarding to classify them according to their physico-chemical properties and to analyse their mechanism of action by global technologies as there is little mechanistic understanding regarding the signaling pathways triggered by different irritants. Such studies will not only provide potential therapeutic targets, they will also help to understand the clinically relevant interaction of irritants with contact allergens which may lead to an augmentation of sensitization and of the clinical response, for example due to heterologous innate immune stimulation [23, 117].
In Vitro Assays for Contact Allergen Identification
A great challenge is the replacement of the LLNA (OECD guideline 429) by in vitro assays that identify contact allergens. The LLNA measures the proliferation of mouse lymph node cells following repeated topical application of a test substance or the solvent to the ear skin. Stimulation indices are calculated and effective chemical concentrations needed to give an SI = 3 (EC3 values) are used to classify chemicals including the determination of relative allergenic potency.
The current roadmap for the development of such assays is the so-called adverse outcome pathway (AOP) for skin sensitization [145]. It describes the key steps in the sensitization process of ACD that should be addressed by in vitro assays. Given the complexity of sensitization, it is clear that a combination of different assays in an integrated testing strategy (ITS) is the most likely strategy for the identification of sensitizing chemicals. Different assays have been developed and are tested for their sensitivity, specificity and accuracy [146]. A recent study demonstrated the advantages of the combination of selected in vitro assays covering different mechanistic aspects of the sensitization process of ACD in an ITS [147].
Eventually, the identification of contact sensitizers must also include assessment of their allergenic potency which is currently not possible in in vitro assays and remains a major advantage of the LLNA. Potency assessment is relevant to determine concentrations of contact allergens such as fragrances that can be used safely in consumer products or in the workplace. Recently, 131 substances have been categorized solely based on relative human skin sensitizing potency data. Such datasets should be more critical for judging the performance of non-animal methods that aim at measuring allergenic potency than a comparison with LLNA EC3 values [148]. Eventually, safety levels must be determined for contact sensitizers used in consumer products or in the workplace and the impact on clinical outcome has to be monitored. A comprehensive review of testing strategies and preventive measures and their impact on clinical outcome was published by Thyssen et al. [149–151].
Future Clinical and Research Challenges
Our mechanistic understanding now allows us to develop strategies that decrease or prevent sensitization. Already at the level of the chemistry, steps for primary prevention can be undertaken. For example, the introduction of a methyl group into the allergenic hair dye pPD reduces its skin sensitizing potency [152]. Chemical alteration of epoxy resin monomers can also reduce their skin sensitizing potency [153]. Such efforts reduce the risk of ACD. Moreover, interference with innate immune responses may prevent sensitization or even elicitation as shown in the CHS model [60, 61, 74, 80] and aid in the induction of tolerance. Targeted therapies to blunt the effector/memory T cell response and to induce regulatory T cells are needed. Global technologies will help to identify biomarker profiles for contact allergens and irritants that should improve diagnostics and promote the identification of relevant signaling pathways and novel drug targets as well as the development of mechanistically-based assays for the in vitro identification of contact allergens.
Abbreviations
- ACD:
-
Allergic contact dermatitis
- APC:
-
Antigen presenting cell
- CHS:
-
Contact hypersensitivity
- DAMP:
-
Damage-associated molecular pattern
- DNBS:
-
2,4-dinitrobenzene sulfonic acid
- DNCB:
-
2,4-dinitrochlorobenzene
- DNFB:
-
2,4-dinitrofluorobenzene
- DNTB:
-
2,4-dinitrothiocyanobenzene
- FLG:
-
Filaggrin
- HA:
-
Hyaluronic acid
- hTCPA:
-
Human T cell priming assay
- ICD:
-
Irritant contact dermatitis
- LLNA:
-
Local Lymph Node Assay
- LZT:
-
Low zone tolerance
- MAMP:
-
Microbe-associated molecular pattern
- MHC:
-
Major histocompatibility complex
- PAMP:
-
Pathogen-associated molecular pattern
- PBMC:
-
Peripheral blood mononuclear cell
- PRR:
-
Pattern recognition receptor
- TCR:
-
T cell receptor
- TNBS:
-
2,4,6-trinitrobenzene sulfonic acid
- TNCB:
-
2,4,6-trinitrochlorobenzene
- TLR:
-
Toll-like receptor
- Treg:
-
Regulatory T cell
References
Peiser M, Tralau T, Heidler J, Api AM, Arts JH, Basketter DA, English J, Diepgen TL, Fuhlbrigge RC, Gaspari AA, Johansen JD, Karlberg AT, Kimber I, Lepoittevin JP, Liebsch M, Maibach HI, Martin SF, Merk HF, Platzek T, Rustemeyer T, Schnuch A, Vandebriel RJ, White IR, Luch A. Allergic contact dermatitis: epidemiology, molecular mechanisms, in vitro methods and regulatory aspects. Current knowledge assembled at an international workshop at BfR, Germany. Cell Mol Life Sci. 2012;69(5):763–81. doi:10.1007/s00018-011-0846-8.
Thyssen JP, Linneberg A, Menne T, Johansen JD. The epidemiology of contact allergy in the general population–prevalence and main findings. Contact Dermatitis. 2007;57(5):287–99. COD1220 [pii]. doi:10.1111/j.1600-0536.2007.01220.x.
Diepgen TL. Occupational skin diseases. J Dtsch Dermatol Ges (Journal of the German Society of Dermatology). 2012;10(5):297–313. doi:10.1111/j.1610-0387.2012.07890.x. quiz 314–295.
Sartorelli P, Kezic S, Larese Filon F, John SM. Prevention of occupational dermatitis. Int J Immunopathol Pharmacol. 2011;24(1 Suppl):89S–93.
Holness DL. Recent advances in occupational dermatitis. Curr Opin Allergy Clin Immunol. 2013;13(2):145–50. doi:10.1097/ACI.0b013e32835e12cf.
Mahler V, Geier J, Schnuch A. Current trends in patch testing – new data from the German Contact Dermatitis Research Group (DKG) and the Information Network of Departments of Dermatology (IVDK). J Dtsch Dermatol Ges (Journal of the German Society of Dermatology). 2014;12(7):583–92. doi:10.1111/ddg.12371.
McFadden JP, Mann J, White JM, Banerjee P, White IR. Outbreak of methylisothiazolinone allergy targeting those aged >/=40 years. Contact Dermatitis. 2013;69(1):53–5. doi:10.1111/cod.12093.
Lundov MD, Opstrup MS, Johansen JD. Methylisothiazolinone contact allergy–growing epidemic. Contact Dermatitis. 2013;69(5):271–5. doi:10.1111/cod.12149.
Lundov MD, Zachariae C, Menne T, Johansen JD. Airborne exposure to preservative methylisothiazolinone causes severe allergic reactions. BMJ. 2012;345:e8221. doi:10.1136/bmj.e8221.
Santos R, Goossens A. An update on airborne contact dermatitis: 2001–2006. Contact Dermatitis. 2007;57(6):353–60. doi:10.1111/j.1600-0536.2007.01233.x.
Swinnen I, Goossens A. An update on airborne contact dermatitis: 2007–2011. Contact Dermatitis. 2013;68(4):232–8. doi:10.1111/cod.12022.
Lundov MD, Friis UF, Menne T, Johansen JD. Methylisothiazolinone in paint forces a patient out of her apartment. Contact Dermatitis. 2013;69(4):252–3. doi:10.1111/cod.12136.
Hausermann P, Harr T, Bircher AJ. Baboon syndrome resulting from systemic drugs: is there strife between SDRIFE and allergic contact dermatitis syndrome? Contact Dermatitis. 2004;51(5-6):297–310. doi:10.1111/j.0105-1873.2004.00445.x.
Veien NK. Systemic contact dermatitis. Int J Dermatol. 2011;50(12):1445–56. doi:10.1111/j.1365-4632.2011.05104.x.
Kerr A, Ferguson J. Photoallergic contact dermatitis. Photodermatol Photoimmunol Photomed. 2010;26(2):56–65. doi:10.1111/j.1600-0781.2010.00494.x.
Novak N, Baurecht H, Schafer T, Rodriguez E, Wagenpfeil S, Klopp N, Heinrich J, Behrendt H, Ring J, Wichmann E, Illig T, Weidinger S. Loss-of-function mutations in the filaggrin gene and allergic contact sensitization to nickel. J Invest Dermatol. 2008;128(6):1430–5. 5701190[pii]. doi:10.1038/sj.jid.5701190.
Spiewak R. Contact dermatitis in atopic individuals. Curr Opin Allergy Clin Immunol. 2012;12(5):491–7. doi:10.1097/ACI.0b013e328357b05a.
Gittler JK, Krueger JG, Guttman-Yassky E. Atopic dermatitis results in intrinsic barrier and immune abnormalities: implications for contact dermatitis. J Allergy Clin Immunol. 2013;131(2):300–13. doi:10.1016/j.jaci.2012.06.048.
Thyssen JP, McFadden JP, Kimber I. The multiple factors affecting the association between atopic dermatitis and contact sensitization. Allergy. 2014;69(1):28–36. doi:10.1111/all.12358.
De Benedetto A, Kubo A, Beck LA. Skin barrier disruption: a requirement for allergen sensitization? J Invest Dermatol. 2012;132(3 Pt 2):949–63. doi:10.1038/jid.2011.435.
Matzinger P. The danger model: a renewed sense of self. Science. 2002;296(5566):301–5. doi:10.1126/science.1071059296/5566/301[pii].
Martin SF. Allergic contact dermatitis: xenoinflammation of the skin. Curr Opin Immunol. 2012;24(6):720–9. doi:10.1016/j.coi.2012.08.003.
Martin SF. Adaptation in the innate immune system and heterologous innate immunity. Cell Mol Life Sci. 2014;71(21):4115–30. doi:10.1007/s00018-014-1676-2.
Brasch J, Henseler T. The reaction index: a parameter to assess the quality of patch test preparations. Contact Dermatitis. 1992;27(3):203–4.
Brasch J, Geier J, Henseler T. Evaluation of patch test results by use of the reaction index. An analysis of data recorded by the Information Network of Departments of Dermatology (IVDK). Contact Dermatitis. 1995;33(6):375–80.
Geier J, Uter W, Lessmann H, Schnuch A. The positivity ratio–another parameter to assess the diagnostic quality of a patch test preparation. Contact Dermatitis. 2003;48(5):280–2.
Andersen KE, Andersen F. The reaction index and positivity ratio revisited. Contact Dermatitis. 2008;58(1):28–31. doi:10.1111/j.1600-0536.2007.01252.x.
Dickel H, Kreft B, Kuss O, Worm M, Soost S, Brasch J, Pfutzner W, Grabbe J, Angelova-Fischer I, Elsner P, Fluhr J, Altmeyer P, Geier J. Increased sensitivity of patch testing by standardized tape stripping beforehand: a multicentre diagnostic accuracy study. Contact Dermatitis. 2010;62(5):294–302. doi:10.1111/j.1600-0536.2010.01710.x.
Dickel H, Gambichler T, Kamphowe J, Altmeyer P, Skrygan M. Standardized tape stripping prior to patch testing induces upregulation of Hsp90, Hsp70, IL-33, TNF-alpha and IL-8/CXCL8 mRNA: new insights into the involvement of ‘alarmins’. Contact Dermatitis. 2010;63(4):215–22. doi:10.1111/j.1600-0536.2010.01769.x.
Johansen JD, Bruze M, Andersen KE, Frosch PJ, Dreier B, White IR, Rastogi S, Lepoittevin JP, Menne T. The repeated open application test: suggestions for a scale of evaluation. Contact Dermatitis. 1998;39(2):95–6.
Nakada T, Hostynek JJ, Maibach HI. Use tests: ROAT (repeated open application test)/PUT (provocative use test): an overview. Contact Dermatitis. 2000;43(1):1–3.
Goncalo M, Ferguson J, Bonevalle A, Bruynzeel DP, Gimenez-Arnau A, Goossens A, Kerr A, Lecha M, Neumann N, Niklasson B, Pigatto P, Rhodes LE, Rustemeyer T, Sarkany R, Thomas P, Wilkinson M. Photopatch testing: recommendations for a European photopatch test baseline series. Contact Dermatitis. 2013;68(4):239–43. doi:10.1111/cod.12037.
Watson ES. Toxicodendron hyposensitization programs. Clin Dermatol. 1986;4(2):160–70.
Bonamonte D, Cristaudo A, Nasorri F, Carbone T, De Pita O, Angelini G, Cavani A. Efficacy of oral hyposensitization in allergic contact dermatitis caused by nickel. Contact Dermatitis. 2011;65(5):293–301. doi:10.1111/j.1600-0536.2011.01940.x.
Schnuch A, Westphal G, Mossner R, Uter W, Reich K. Genetic factors in contact allergy–review and future goals. Contact Dermatitis. 2011;64(1):2–23. doi:10.1111/j.1600-0536.2010.01800.x.
Irvine AD, McLean WH, Leung DY. Filaggrin mutations associated with skin and allergic diseases. N Engl J Med. 2011;365(14):1315–27. doi:10.1056/NEJMra1011040.
Palmer CN, Irvine AD, Terron-Kwiatkowski A, Zhao Y, Liao H, Lee SP, Goudie DR, Sandilands A, Campbell LE, Smith FJ, O'Regan GM, Watson RM, Cecil JE, Bale SJ, Compton JG, DiGiovanna JJ, Fleckman P, Lewis-Jones S, Arseculeratne G, Sergeant A, Munro CS, El Houate B, McElreavey K, Halkjaer LB, Bisgaard H, Mukhopadhyay S, McLean WH. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nat Genet. 2006;38(4):441–6. doi:10.1038/ng1767.
McLean WH, Irvine AD. Heritable filaggrin disorders: the paradigm of atopic dermatitis. J Invest Dermatol. 2012;132(E1):E20–1. doi:10.1038/skinbio.2012.6.
Thyssen JP. The association between filaggrin mutations, hand eczema and contact dermatitis: a clear picture is emerging. Br J Dermatol. 2012;167(6):1197–8. doi:10.1111/bjd.12075.
Visser MJ, Landeck L, Campbell LE, McLean WH, Weidinger S, Calkoen F, John SM, Kezic S. Impact of atopic dermatitis and loss-of-function mutations in the filaggrin gene on the development of occupational irritant contact dermatitis. Br J Dermatol. 2013;168(2):326–32. doi:10.1111/bjd.12083.
Kawasaki H, Nagao K, Kubo A, Hata T, Shimizu A, Mizuno H, Yamada T, Amagai M. Altered stratum corneum barrier and enhanced percutaneous immune responses in filaggrin-null mice. J Allergy Clin Immunol. 2012;129(6):1538–46.e1536. doi:10.1016/j.jaci.2012.01.068.
Karlberg AT, Borje A, Duus Johansen J, Liden C, Rastogi S, Roberts D, Uter W, White IR. Activation of non-sensitizing or low-sensitizing fragrance substances into potent sensitizers – prehaptens and prohaptens. Contact Dermatitis. 2013;69(6):323–34. doi:10.1111/cod.12127.
Aptula AO, Patlewicz G, Roberts DW. Skin sensitization: reaction mechanistic applicability domains for structure-activity relationships. Chem Res Toxicol. 2005;18(9):1420–6. doi:10.1021/tx050075m.
Roberts DW, Aptula AO, Patlewicz G. Electrophilic chemistry related to skin sensitization. Reaction mechanistic applicability domain classification for a published data set of 106 chemicals tested in the mouse local lymph node assay. Chem Res Toxicol. 2007;20(1):44–60. doi:10.1021/tx060121y.
Albrekt AS, Johansson H, Borje A, Borrebaeck C, Lindstedt M. Skin sensitizers differentially regulate signaling pathways in MUTZ-3 cells in relation to their individual potency. BMC Pharmacol Toxicol. 2014;15:5. doi:10.1186/2050-6511-15-5.
Martin SF. Contact dermatitis: from pathomechanisms to immunotoxicology. Exp Dermatol. 2012;21(5):382–9. doi:10.1111/j.1600-0625.2012.01471.x.
Megherbi R, Kiorpelidou E, Foster B, Rowe C, Naisbitt DJ, Goldring CE, Park BK. Role of protein haptenation in triggering maturation events in the dendritic cell surrogate cell line THP-1. Toxicol Appl Pharmacol. 2009;238(2):120–32.
Elbayed K, Berl V, Debeuckelaere C, Moussallieh FM, Piotto M, Namer IJ, Lepoittevin JP. HR-MAS NMR spectroscopy of reconstructed human epidermis: potential for the in situ investigation of the chemical interactions between skin allergens and nucleophilic amino acids. Chem Res Toxicol. 2013;26(1):136–45. doi:10.1021/tx300428u.
Schmidt M, Raghavan B, Muller V, Vogl T, Fejer G, Tchaptchet S, Keck S, Kalis C, Nielsen PJ, Galanos C, Roth J, Skerra A, Martin SF, Freudenberg MA, Goebeler M. Crucial role for human Toll-like receptor 4 in the development of contact allergy to nickel. Nat Immunol. 2010;11(9):814–9. ni.1919 [pii]. doi:10.1038/ni.1919.
Raghavan B, Martin SF, Esser PR, Goebeler M, Schmidt M. Metal allergens nickel and cobalt facilitate TLR4 homodimerization independently of MD2. EMBO Rep. 2012;13(12):1109–15. doi:10.1038/embor.2012.155.
Rachmawati D, Bontkes HJ, Verstege MI, Muris J, von Blomberg BM, Scheper RJ, van Hoogstraten IM. Transition metal sensing by Toll-like receptor-4: next to nickel, cobalt and palladium are potent human dendritic cell stimulators. Contact Dermatitis. 2013;68(6):331–8. doi:10.1111/cod.12042.
El Ali Z, Gerbeix C, Hemon P, Esser PR, Martin SF, Pallardy M, Kerdine-Romer S. Allergic skin inflammation induced by chemical sensitizers is controlled by the transcription factor Nrf2. Toxicol Sci. 2013;134(1):39–48. doi:10.1093/toxsci/kft084.
van der Veen JW, Gremmer ER, Vermeulen JP, van Loveren H, Ezendam J. Induction of skin sensitization is augmented in Nrf2-deficient mice. Arch Toxicol. 2013;87(4):763–6. doi:10.1007/s00204-012-0976-2.
Silva CR, Oliveira SM, Rossato MF, Dalmolin GD, Guerra GP, da Silveira Prudente A, Cabrini DA, Otuki MF, Andre E, Ferreira J. The involvement of TRPA1 channel activation in the inflammatory response evoked by topical application of cinnamaldehyde to mice. Life Sci. 2011;88(25–26):1077–87. doi:10.1016/j.lfs.2011.03.017.
Saarnilehto M, Chapman H, Savinko T, Lindstedt K, Lauerma AI, Koivisto A. Contact sensitizer 2,4-dinitrochlorobenzene is a highly potent human TRPA1 agonist. Allergy. 2014;69(10):1424–7. doi:10.1111/all.12488.
Bautista DM, Pellegrino M, Tsunozaki M. TRPA1: a gatekeeper for inflammation. Annu Rev Physiol. 2013;75:181–200. doi:10.1146/annurev-physiol-030212-183811.
Wilson SR, Gerhold KA, Bifolck-Fisher A, Liu Q, Patel KN, Dong X, Bautista DM. TRPA1 is required for histamine-independent, Mas-related G protein-coupled receptor-mediated itch. Nat Neurosci. 2011;14(5):595–602. doi:10.1038/nn.2789.
Liu B, Escalera J, Balakrishna S, Fan L, Caceres AI, Robinson E, Sui A, McKay MC, McAlexander MA, Herrick CA, Jordt SE. TRPA1 controls inflammation and pruritogen responses in allergic contact dermatitis. FASEB J (Official Publication of the Federation of American Societies for Experimental Biology). 2013;27(9):3549–63. doi:10.1096/fj.13-229948.
Trevisani M, Siemens J, Materazzi S, Bautista DM, Nassini R, Campi B, Imamachi N, Andre E, Patacchini R, Cottrell GS, Gatti R, Basbaum AI, Bunnett NW, Julius D, Geppetti P. 4-Hydroxynonenal, an endogenous aldehyde, causes pain and neurogenic inflammation through activation of the irritant receptor TRPA1. Proc Natl Acad Sci U S A. 2007;104(33):13519–24. doi:10.1073/pnas.0705923104.
Esser PR, Wolfle U, Durr C, von Loewenich FD, Schempp CM, Freudenberg MA, Jakob T, Martin SF. Contact sensitizers induce skin inflammation via ROS production and hyaluronic acid degradation. PLoS One. 2012;7(7):e41340. doi:10.1371/journal.pone.0041340.
Martin SF, Esser PR, Weber FC, Jakob T, Freudenberg MA, Schmidt M, Goebeler M. Mechanisms of chemical-induced innate immunity in allergic contact dermatitis. Allergy. 2011;66:1152–63. doi:10.1111/j.1398-9995.2011.02652.x.
Kaplan DH, Igyarto BZ, Gaspari AA. Early immune events in the induction of allergic contact dermatitis. Nat Rev Immunol. 2012;12(2):114–24. nri3150 [pii]. doi:10.1038/nri3150.
Gomez de Aguero M, Vocanson M, Hacini-Rachinel F, Taillardet M, Sparwasser T, Kissenpfennig A, Malissen B, Kaiserlian D, Dubois B. Langerhans cells protect from allergic contact dermatitis in mice by tolerizing CD8(+) T cells and activating Foxp3(+) regulatory T cells. J Clin Invest. 2012;122(5):1700–11. 59725 [pii]. doi:10.1172/JCI59725.
Seneschal J, Clark RA, Gehad A, Baecher-Allan CM, Kupper TS. Human epidermal langerhans cells maintain immune homeostasis in skin by activating skin resident regulatory T cells. Immunity. 2012;36(5):873–84. S1074-7613(12)00176-8 [pii]. doi:10.1016/j.immuni.2012.03.018.
Kaplan DH, Kissenpfennig A, Clausen BE. Insights into Langerhans cell function from Langerhans cell ablation models. Eur J Immunol. 2008;38(9):2369–76. doi:10.1002/eji.200838397.
Clausen BE, Kel JM. Langerhans cells: critical regulators of skin immunity? Immunol Cell Biol. 2010;88(4):351–60. doi:10.1038/icb.2010.40.
Noordegraaf M, Flacher V, Stoitzner P, Clausen BE. Functional redundancy of Langerhans cells and Langerin + dermal dendritic cells in contact hypersensitivity. J Invest Dermatol. 2010;130(12):2752–9. doi:10.1038/jid.2010.223.
Dudeck A, Dudeck J, Scholten J, Petzold A, Surianarayanan S, Kohler A, Peschke K, Vohringer D, Waskow C, Krieg T, Muller W, Waisman A, Hartmann K, Gunzer M, Roers A. Mast cells are key promoters of contact allergy that mediate the adjuvant effects of haptens. Immunity. 2011;34(6):973–84. S1074-7613(11)00229-9 [pii]. doi:10.1016/j.immuni.2011.03.028.
Engeman T, Gorbachev AV, Kish DD, Fairchild RL. The intensity of neutrophil infiltration controls the number of antigen-primed CD8 T cells recruited into cutaneous antigen challenge sites. J Leukoc Biol. 2004;76(5):941–9. doi:10.1189/jlb.0304193jlb.0304193[pii].
Christensen AD, Skov S, Haase C. The role of neutrophils and G-CSF in DNFB-induced contact hypersensitivity in mice. Immun Inflamm Dis. 2014;2(1):21–34. doi:10.1002/iid3.16.
Weber FC, Nemeth T, Csepregi JZ, Dudeck A, Roers A, Ozsvari B, Oswald E, Puskas LG, Jakob T, Mocsai A, Martin SF. Neutrophils are required for both the sensitization and elicitation phase of contact hypersensitivity. J Exp Med. 2014;212:15–22. doi:10.1084/jem.20130062.
Kawai T, Akira S. The role of pattern-recognition receptors in innate immunity: update on Toll-like receptors. Nat Immunol. 2010;11(5):373–84. ni.1863 [pii]. doi:10.1038/ni.1863.
Martin SF, Dudda JC, Bachtanian E, Lembo A, Liller S, Durr C, Heimesaat MM, Bereswill S, Fejer G, Vassileva R, Jakob T, Freudenberg N, Termeer CC, Johner C, Galanos C, Freudenberg MA. Toll-like receptor and IL-12 signaling control susceptibility to contact hypersensitivity. J Exp Med. 2008;205(9):2151–62. jem.20070509 [pii]. doi:10.1084/jem.20070509.
Weber FC, Esser PR, Muller T, Ganesan J, Pellegatti P, Simon MM, Zeiser R, Idzko M, Jakob T, Martin SF. Lack of the purinergic receptor P2X(7) results in resistance to contact hypersensitivity. J Exp Med. 2010;207(12):2609–19. jem.20092489 [pii]. doi:10.1084/jem.20092489.
Muto J, Morioka Y, Yamasaki K, Kim M, Garcia A, Carlin AF, Varki A, Gallo RL. Hyaluronan digestion controls DC migration from the skin. J Clin Invest. 2014;124(3):1309–19. doi:10.1172/JCI67947.
Docampo MJ, Zanna G, Fondevila D, Cabrera J, Lopez-Iglesias C, Carvalho A, Cerrato S, Ferrer L, Bassols A. Increased HAS2-driven hyaluronic acid synthesis in shar-pei dogs with hereditary cutaneous hyaluronosis (mucinosis). Vet Dermatol. 2011;22(6):535–45. doi:10.1111/j.1365-3164.2011.00986.x.
Sorokin L. The impact of the extracellular matrix on inflammation. Nat Rev Immunol. 2010;10(10):712–23. nri2852 [pii]. doi:10.1038/nri2852.
Galbiati V, Papale A, Galli CL, Marinovich M, Corsini E. Role of ROS and HMGB1 in contact allergen-induced IL-18 production in human keratinocytes. J Invest Dermatol. 2014;134:2719–27. doi:10.1038/jid.2014.203.
Li X, Zhong F. Nickel induces interleukin-1beta secretion via the NLRP3-ASC-caspase-1 pathway. Inflammation. 2014;37(2):457–66. doi:10.1007/s10753-013-9759-z.
Yasukawa S, Miyazaki Y, Yoshii C, Nakaya M, Ozaki N, Toda S, Kuroda E, Ishibashi K, Yasuda T, Natsuaki Y, Mi-ichi F, Iizasa E, Nakahara T, Yamazaki M, Kabashima K, Iwakura Y, Takai T, Saito T, Kurosaki T, Malissen B, Ohno N, Furue M, Yoshida H, Hara H. An ITAM-Syk-CARD9 signalling axis triggers contact hypersensitivity by stimulating IL-1 production in dendritic cells. Nat Commun. 2014;5:3755. doi:10.1038/ncomms4755.
Johansson H, Lindstedt M, Albrekt AS, Borrebaeck CA. A genomic biomarker signature can predict skin sensitizers using a cell-based in vitro alternative to animal tests. BMC Genomics. 2011;12:399. doi:10.1186/1471-2164-12-399.
Stockinger B, Di Meglio P, Gialitakis M, Duarte JH. The aryl hydrocarbon receptor: multitasking in the immune system. Annu Rev Immunol. 2014;32:403–32. doi:10.1146/annurev-immunol-032713-120245.
Kalmes M, Blomeke B. Impact of eugenol and isoeugenol on AhR translocation, target gene expression, and proliferation in human HaCaT keratinocytes. J Toxicol Environ Health A. 2012;75(8–10):478–91. doi:10.1080/15287394.2012.674916.
Pasparakis M, Haase I, Nestle FO. Mechanisms regulating skin immunity and inflammation. Nat Rev Immunol. 2014;14(5):289–301. doi:10.1038/nri3646.
Kumari S, Herzberg B, Pofahl R, Krieg T, Haase I. Epidermal RelA specifically restricts contact allergen-induced inflammation and apoptosis in skin. J Invest Dermatol. 2014;134:2541–50. doi:10.1038/jid.2014.193.
Vogl T, Tenbrock K, Ludwig S, Leukert N, Ehrhardt C, van Zoelen MA, Nacken W, Foell D, van der Poll T, Sorg C, Roth J. Mrp8 and Mrp14 are endogenous activators of Toll-like receptor 4, promoting lethal, endotoxin-induced shock. Nat Med. 2007;13(9):1042–9. doi:10.1038/nm1638.
Chan JK, Roth J, Oppenheim JJ, Tracey KJ, Vogl T, Feldmann M, Horwood N, Nanchahal J. Alarmins: awaiting a clinical response. J Clin Invest. 2012;122(8):2711–9. doi:10.1172/JCI62423.
Petersen B, Wolf M, Austermann J, van Lent P, Foell D, Ahlmann M, Kupas V, Loser K, Sorg C, Roth J, Vogl T. The alarmin Mrp8/14 as regulator of the adaptive immune response during allergic contact dermatitis. EMBO J. 2013;32(1):100–11. doi:10.1038/emboj.2012.309.
Dubrac S, Schmuth M. PPAR-alpha in cutaneous inflammation. Dermatoendocrinol. 2011;3(1):23–6. doi:10.4161/derm.3.1.14615.
Komuves LG, Hanley K, Man MQ, Elias PM, Williams ML, Feingold KR. Keratinocyte differentiation in hyperproliferative epidermis: topical application of PPARalpha activators restores tissue homeostasis. J Invest Dermatol. 2000;115(3):361–7. doi:10.1046/j.1523-1747.2000.00076.x.
Sheu MY, Fowler AJ, Kao J, Schmuth M, Schoonjans K, Auwerx J, Fluhr JW, Man MQ, Elias PM, Feingold KR. Topical peroxisome proliferator activated receptor-alpha activators reduce inflammation in irritant and allergic contact dermatitis models. J Invest Dermatol. 2002;118(1):94–101. doi:10.1046/j.0022-202x.2001.01626.x.
Dubrac S, Elentner A, Schoonjans K, Auwerx J, Schmuth M. Lack of IL-2 in PPAR-alpha-deficient mice triggers allergic contact dermatitis by affecting regulatory T cells. Eur J Immunol. 2011;41(7):1980–91. doi:10.1002/eji.201041357.
Petrosino S, Cristino L, Karsak M, Gaffal E, Ueda N, Tuting T, Bisogno T, De Filippis D, D'Amico A, Saturnino C, Orlando P, Zimmer A, Iuvone T, Di Marzo V. Protective role of palmitoylethanolamide in contact allergic dermatitis. Allergy. 2010;65(6):698–711. doi:10.1111/j.1398-9995.2009.02254.x.
Imaeda AB, Watanabe A, Sohail MA, Mahmood S, Mohamadnejad M, Sutterwala FS, Flavell RA, Mehal WZ. Acetaminophen-induced hepatotoxicity in mice is dependent on Tlr9 and the Nalp3 inflammasome. J Clin Invest. 2009;119(2):305–14. 35958 [pii]. doi:10.1172/JCI35958.
Hoque R, Sohail MA, Salhanick S, Malik AF, Ghani A, Robson SC, Mehal WZ. P2X7 receptor-mediated purinergic signaling promotes liver injury in acetaminophen hepatotoxicity in mice. Am J Physiol Gastrointest Liver Physiol. 2012;302(10):G1171–9. ajpgi.00352.2011 [pii]10.1152/ajpgi.00352.2011.
Nassini R, Materazzi S, Andre E, Sartiani L, Aldini G, Trevisani M, Carnini C, Massi D, Pedretti P, Carini M, Cerbai E, Preti D, Villetti G, Civelli M, Trevisan G, Azzari C, Stokesberry S, Sadofsky L, McGarvey L, Patacchini R, Geppetti P. Acetaminophen, via its reactive metabolite N-acetyl-p-benzo-quinoneimine and transient receptor potential ankyrin-1 stimulation, causes neurogenic inflammation in the airways and other tissues in rodents. FASEB J (Official Publication of the Federation of American Societies for Experimental Biology). 2010;24(12):4904–16. doi:10.1096/fj.10-162438.
Akdis M, Palomares O, van de Veen W, van Splunter M and Akdis CA. TH17 and TH22 cells: a confusion of antimicrobial response with tissue inflammation versus protection. J Allergy Clin Immunol. 2012;129(6):1438–49; quiz1450–1431. doi:10.1016/j.jaci.2012.05.003.
Dearman RJ, Warbrick EV, Skinner R, Kimber I. Cytokine fingerprinting of chemical allergens: species comparisons and statistical analyses. Food Chem Toxicol (An International Journal Published for the British Industrial Biological Research Association). 2002;40(12):1881–92.
Dearman RJ, Betts CJ, Caddick HT, Kimber I. Cytokine profiling of chemical allergens in mice: impact of mitogen on selectivity of response. J Appl Toxicol. 2009;29(3):233–41. doi:10.1002/jat.1401.
Hopkins JE, Naisbitt DJ, Kitteringham NR, Dearman RJ, Kimber I, Park BK. Selective haptenation of cellular or extracellular protein by chemical allergens: association with cytokine polarization. Chem Res Toxicol. 2005;18(2):375–81.
Moggs JG, Terranova R, Kammuller ME, Chibout SD, Chapman V, Dearman RJ, Kimber I. Regulation of allergic responses to chemicals and drugs: possible roles of epigenetic mechanisms. Toxicol Sci. 2012;130(1):60–9. doi:10.1093/toxsci/kfs207.
Chapman VL, Zollinger T, Terranova R, Moggs J, Kimber I, Dearman RJ. Chemical allergen induced perturbations of the mouse lymph node DNA methylome. Toxicol Sci. 2014;139(2):350–61. doi:10.1093/toxsci/kfu047.
Proksch E, Brasch J. Abnormal epidermal barrier in the pathogenesis of contact dermatitis. Clin Dermatol. 2012;30(3):335–44. doi:10.1016/j.clindermatol.2011.08.019.
Grabbe S, Steinert M, Mahnke K, Schwartz A, Luger TA, Schwarz T. Dissection of antigenic and irritative effects of epicutaneously applied haptens in mice. Evidence that not the antigenic component but nonspecific proinflammatory effects of haptens determine the concentration-dependent elicitation of allergic contact dermatitis. J Clin Invest. 1996;98(5):1158–64. doi:10.1172/JCI118899.
Watanabe H, Gehrke S, Contassot E, Roques S, Tschopp J, Friedmann PS, French LE, Gaide O. Danger signaling through the inflammasome acts as a master switch between tolerance and sensitization. J Immunol. 2008;180(9):5826–32. doi:180/9/5826[pii].
de Jongh CM, Lutter R, Verberk MM, Kezic S. Differential cytokine expression in skin after single and repeated irritation by sodium lauryl sulphate. Exp Dermatol. 2007;16(12):1032–40. doi:10.1111/j.1600-0625.2007.00628.x.
Lee HY, Stieger M, Yawalkar N, Kakeda M. Cytokines and chemokines in irritant contact dermatitis. Mediators Inflamm. 2013;2013:916497. doi:10.1155/2013/916497.
Ouwehand K, Santegoets SJ, Bruynzeel DP, Scheper RJ, de Gruijl TD, Gibbs S. CXCL12 is essential for migration of activated Langerhans cells from epidermis to dermis. Eur J Immunol. 2008;38(11):3050–9. doi:10.1002/eji.200838384.
Ouwehand K, Scheper RJ, de Gruijl TD, Gibbs S. Epidermis-to-dermis migration of immature Langerhans cells upon topical irritant exposure is dependent on CCL2 and CCL5. Eur J Immunol. 2010;40(7):2026–34. doi:10.1002/eji.200940150.
Nakashima C, Otsuka A, Kitoh A, Honda T, Egawa G, Nakajima S, Nakamizo S, Arita M, Kubo M, Miyachi Y, Kabashima K. Basophils regulate the recruitment of eosinophils in a murine model of irritant contact dermatitis. J Allergy Clin Immunol. 2014;134:100–7. doi:10.1016/j.jaci.2014.02.026.
Dvorak HF, Mihm Jr MC. Basophilic leukocytes in allergic contact dermatitis. J Exp Med. 1972;135(2):235–54.
Ito Y, Satoh T, Takayama K, Miyagishi C, Walls AF, Yokozeki H. Basophil recruitment and activation in inflammatory skin diseases. Allergy. 2011;66(8):1107–13. doi:10.1111/j.1398-9995.2011.02570.x.
Simon D, Aeberhard C, Erdemoglu Y, Simon HU. Th17 cells and tissue remodeling in atopic and contact dermatitis. Allergy. 2014;69(1):125–31. doi:10.1111/all.12351.
Uter W, Yazar K, Kratz EM, Mildau G, Liden C. Coupled exposure to ingredients of cosmetic products: I. Fragrances. Contact Dermatitis. 2013;69(6):335–41. doi:10.1111/cod.12125.
Uter W, Yazar K, Kratz EM, Mildau G, Liden C. Coupled exposure to ingredients of cosmetic products: II. Preservatives. Contact Dermatitis. 2014;70(4):219–26. doi:10.1111/cod.12165.
Uter W, Goncalo M, Yazar K, Kratz EM, Mildau G, Liden C. Coupled exposure to ingredients of cosmetic products: III. Ultraviolet filters. Contact Dermatitis. 2014;71:162–9. doi:10.1111/cod.12245.
Pedersen LK, Johansen JD, Held E, Agner T. Augmentation of skin response by exposure to a combination of allergens and irritants – a review. Contact Dermatitis. 2004;50(5):265–73. doi:10.1111/j.0105-1873.2004.00342.x.
Bonefeld CM, Nielsen MM, Rubin IM, Vennegaard MT, Dabelsteen S, Gimenez-Arnau E, Lepoittevin JP, Geisler C, Johansen JD. Enhanced sensitization and elicitation responses caused by mixtures of common fragrance allergens. Contact Dermatitis. 2011;65(6):336–42. doi:10.1111/j.1600-0536.2011.01945.x.
Kinbara M, Sato N, Kuroishi T, Takano-Yamamoto T, Sugawara S, Endo Y. Allergy-inducing nickel concentration is lowered by lipopolysaccharide at both the sensitization and elicitation steps in a murine model. Br J Dermatol. 2011;164(2):356–62. BJD10016 [pii]. doi:10.1111/j.1365-2133.2010.10016.x.
Agner T, Johansen JD, Overgaard L, Volund A, Basketter D, Menne T. Combined effects of irritants and allergens. Synergistic effects of nickel and sodium lauryl sulfate in nickel- sensitized individuals. Contact Dermatitis. 2002;47(1):21–6.
Martin SF, Esser PR, Schmucker S, Dietz L, Naisbitt DJ, Park BK, Vocanson M, Nicolas JF, Keller M, Pichler WJ, Peiser M, Luch A, Wanner R, Maggi E, Cavani A, Rustemeyer T, Richter A, Thierse HJ, Sallusto F. T-cell recognition of chemicals, protein allergens and drugs: towards the development of in vitro assays. Cell Mol Life Sci. 2010;67(24):4171–84. doi:10.1007/s00018-010-0495-3.
Lu L, Vollmer J, Moulon C, Weltzien HU, Marrack P, Kappler J. Components of the ligand for a Ni++ reactive human T cell clone. J Exp Med. 2003;197(5):567–74.
Gamerdinger K, Moulon C, Karp DR, Van Bergen J, Koning F, Wild D, Pflugfelder U, Weltzien HU. A new type of metal recognition by human T cells: contact residues for peptide-independent bridging of T cell receptor and major histocompatibility complex by nickel. J Exp Med. 2003;197(10):1345–53. doi:10.1084/jem.20030121jem.20030121[pii].
Peiser M. Role of Th17 cells in skin inflammation of allergic contact dermatitis. Clin Dev Immunol. 2013;2013:261037. doi:10.1155/2013/261037.
Cavani A, Pennino D, Eyerich K. Th17 and Th22 in skin allergy. Chem Immunol Allergy. 2012;96:39–44. doi:10.1159/000331870.
Nielsen MM, Lovato P, MacLeod AS, Witherden DA, Skov L, Dyring-Andersen B, Dabelsteen S, Woetmann A, Odum N, Havran WL, Geisler C, Bonefeld CM. IL-1beta-dependent activation of dendritic epidermal T cells in contact hypersensitivity. J Immunol. 2014;192(7):2975–83. doi:10.4049/jimmunol.1301689.
Mizukami J, Sato T, Camps M, Ji H, Rueckle T, Swinnen D, Tsuboi R, Takeda K, Ichijo H. ASK1 promotes the contact hypersensitivity response through IL-17 production. Scientific reports. 2014;4:4714. doi:10.1038/srep04714.
Hennino A, Jean-Decoster C, Giordano-Labadie F, Debeer S, Vanbervliet B, Rozieres A, Schmitt AM, Nicolas JF. CD8+ T cells are recruited early to allergen exposure sites in atopy patch test reactions in human atopic dermatitis. J Allergy Clin Immunol. 2011;127(4):1064–7. S0091-6749(10)01837-3 [pii]. doi:10.1016/j.jaci.2010.11.022.
Carbone T, Nasorri F, Pennino D, Eyerich K, Foerster S, Cifaldi L, Traidl-Hoffman C, Behrendt H, Cavani A. CD56highCD16-CD62L- NK cells accumulate in allergic contact dermatitis and contribute to the expression of allergic responses. J Immunol. 2010;184(2):1102–10. doi:10.4049/jimmunol.0902518.
O'Leary JG, Goodarzi M, Drayton DL, von Andrian UH. T cell- and B cell-independent adaptive immunity mediated by natural killer cells. Nat Immunol. 2006;7(5):507–16. ni1332 [pii]. doi:10.1038/ni1332.
Paust S, Gill HS, Wang BZ, Flynn MP, Moseman EA, Senman B, Szczepanik M, Telenti A, Askenase PW, Compans RW, von Andrian UH. Critical role for the chemokine receptor CXCR6 in NK cell-mediated antigen-specific memory of haptens and viruses. Nat Immunol. 2010;11(12):1127–35. doi:10.1038/ni.1953.
Rouzaire P, Luci C, Blasco E, Bienvenu J, Walzer T, Nicolas JF, Hennino A. Natural killer cells and T cells induce different types of skin reactions during recall responses to haptens. Eur J Immunol. 2011;42:80–8. doi:10.1002/eji.201141820.
Vocanson M, Rozieres A, Hennino A, Poyet G, Gaillard V, Renaudineau S, Achachi A, Benetiere J, Kaiserlian D, Dubois B, Nicolas JF. Inducible costimulator (ICOS) is a marker for highly suppressive antigen-specific T cells sharing features of TH17/TH1 and regulatory T cells. J Allergy Clin Immunol. 2010;126(2):280–9. 289.e281–287. S0091-6749(10)00827-4 [pii]. doi:10.1016/j.jaci.2010.05.022.
Goubier A, Vocanson M, Macari C, Poyet G, Herbelin A, Nicolas JF, Dubois B, Kaiserlian D. Invariant NKT cells suppress CD8(+) T-cell-mediated allergic contact dermatitis independently of regulatory CD4(+) T cells. J Invest Dermatol. 2013;133(4):980–7. doi:10.1038/jid.2012.404.
Liu J, Harberts E, Tammaro A, Girardi N, Filler RB, Fishelevich R, Temann A, Licona-Limon P, Girardi M, Flavell RA, Gaspari AA. IL-9 regulates allergen-specific Th1 responses in allergic contact dermatitis. J Invest Dermatol. 2014;134(7):1903–11. doi:10.1038/jid.2014.61.
Dhingra N, Shemer A, Correa da Rosa J, Rozenblit M, Fuentes-Duculan J, Gittler JK, Finney R, Czarnowicki T, Zheng X, Xu H, Estrada YD, Cardinale I, Suarez-Farinas M, Krueger JG, Guttman-Yassky E. Molecular profiling of contact dermatitis skin identifies allergen-dependent differences in immune response. J Allergy Clin Immunol. 2014;134(2):362–72. doi:10.1016/j.jaci.2014.03.009.
Marth K, Focke-Tejkl M, Lupinek C, Valenta R, Niederberger V. Allergen Peptides, Recombinant Allergens and Hypoallergens for Allergen-Specific Immunotherapy. Curr Treat Options Allergy. 2014;1:91–106. doi:10.1007/s40521-013-0006-5.
Cavkaytar O, Akdis CA, Akdis M. Modulation of immune responses by immunotherapy in allergic diseases. Curr Opin Pharmacol. 2014;17C:30–7. doi:10.1016/j.coph.2014.07.003.
Spiewak R. Immunotherapy of allergic contact dermatitis. Immunotherapy. 2011;3(8):979–96. doi:10.2217/imt.11.89.
Luckey U, Schmidt T, Pfender N, Romer M, Lorenz N, Martin SF, Bopp T, Schmitt E, Nikolaev A, Yogev N, Waisman A, Jakob T, Steinbrink K. Interplay between CD4 + CD25+ regulatory T cells, tolerogenic CD11c + dendritic cells and CD8+ suppressor T cells is critical for tolerance to contact allergens. J Allergy Clin Immunol. 2012;130:781–91.e711.
Luckey U, Maurer M, Schmidt T, Lorenz N, Seebach B, Metz M, Steinbrink K. T cell killing by tolerogenic dendritic cells protects mice from allergy. J Clin Invest. 2011;121(10):3860–71. 45963 [pii]. doi:10.1172/JCI45963.
Esser PR, Kimber I, Martin SF. Correlation of contact sensitizer potency with T cell frequency and TCR repertoire diversity. Exs. 2014;104:101–14. doi:10.1007/978-3-0348-0726-5_8.
Quaranta M, Knapp B, Garzorz N, Mattii M, Pullabhatla V, Pennino D, Andres C, Traidl-Hoffmann C, Cavani A, Theis FJ, Ring J, Schmidt-Weber CB, Eyerich S and Eyerich K. Intraindividual genome expression analysis reveals a specific molecular signature of psoriasis and eczema. Sci Transl Med. 2014;6(244):244ra290. doi:10.1126/scitranslmed.3008946.
Clemmensen A, Andersen KE, Clemmensen O, Tan Q, Petersen TK, Kruse TA, Thomassen M. Genome-wide expression analysis of human in vivo irritated epidermis: differential profiles induced by sodium lauryl sulfate and nonanoic acid. J Invest Dermatol. 2010;130(9):2201–10. doi:10.1038/jid.2010.102.
Maxwell G, MacKay C, Cubberley R, Davies M, Gellatly N, Glavin S, Gouin T, Jacquoilleot S, Moore C, Pendlington R, Saib O, Sheffield D, Stark R, Summerfield V. Applying the skin sensitisation adverse outcome pathway (AOP) to quantitative risk assessment. Toxicol In Vitro. 2014;28(1):8–12. doi:10.1016/j.tiv.2013.10.013.
Bauch C, Kolle SN, Ramirez T, Eltze T, Fabian E, Mehling A, Teubner W, van Ravenzwaay B, Landsiedel R. Putting the parts together: combining in vitro methods to test for skin sensitizing potentials. Regul Toxicol Pharmacol. 2012;63(3):489–504. doi:10.1016/j.yrtph.2012.05.013.
van der Veen JW, Rorije E, Emter R, Natsch A, van Loveren H, Ezendam J. Evaluating the performance of integrated approaches for hazard identification of skin sensitizing chemicals. Regul Toxicol Pharmacol. 2014;69(3):371–9. doi:10.1016/j.yrtph.2014.04.018.
Basketter DA, Alepee N, Ashikaga T, Barroso J, Gilmour N, Goebel C, Hibatallah J, Hoffmann S, Kern P, Martinozzi-Teissier S, Maxwell G, Reisinger K, Sakaguchi H, Schepky A, Tailhardat M, Templier M. Categorization of chemicals according to their relative human skin sensitizing potency. Dermatitis. 2014;25(1):11–21. doi:10.1097/DER.0000000000000003.
Thyssen JP, Gimenez-Arnau E, Lepoittevin JP, Menne T, Boman A, Schnuch A. The critical review of methodologies and approaches to assess the inherent skin sensitization potential (skin allergies) of chemicals. Part III. Contact Dermatitis. 2012;66 Suppl 1:53–70. doi:10.1111/j.1600-0536.2011.02004_4.x.
Thyssen JP, Gimenez-Arnau E, Lepoittevin JP, Menne T, Boman A, Schnuch A. The critical review of methodologies and approaches to assess the inherent skin sensitization potential (skin allergies) of chemicals. Part II. Contact Dermatitis. 2012;66 Suppl 1:25–52. doi:10.1111/j.1600-0536.2011.02004_3.x.
Thyssen JP, Gimenez-Arnau E, Lepoittevin JP, Menne T, Boman A, Schnuch A. The critical review of methodologies and approaches to assess the inherent skin sensitization potential (skin allergies) of chemicals. Part I. Contact Dermatitis. 2012;66 Suppl 1:11–24. doi:10.1111/j.1600-0536.2011.02004_2.x.
Goebel C, Troutman J, Hennen J, Rothe H, Schlatter H, Gerberick GF, Blomeke B. Introduction of a methoxymethyl side chain into p-phenylenediamine attenuates its sensitizing potency and reduces the risk of allergy induction. Toxicol Appl Pharmacol. 2014;274(3):480–7. doi:10.1016/j.taap.2013.11.016.
O'Boyle NM, Niklasson IB, Tehrani-Bagha AR, Delaine T, Holmberg K, Luthman K, Karlberg AT. Epoxy resin monomers with reduced skin sensitizing potency. Chem Res Toxicol. 2014;27(6):1002–10. doi:10.1021/tx5000624.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Questions
Questions
-
1.
What is the outcome of the sensitization to contact allergens?
-
A.
The primary activation of contact allergen-specific T cells
-
B.
The recruitment of T cells from the blood into the skin
-
C.
The induction of skin inflammation by T cells
-
D.
The reactivation of memory T cells
-
A.
-
2.
What is a hallmark of contact allergens?
-
A.
Contact allergens are proteins
-
B.
Contact allergens have enzymatic activity
-
C.
Contact allergens bind to proteins covalently or by complex formation
-
D.
Contact allergens bind to NF-κB
-
A.
-
3.
Which standard test is used for the diagnosis of ACD?
-
A.
The Prick test is the current standard test
-
B.
The Local Lymph Node Assay is the current standard test
-
C.
The Patch test is the current standard test
-
A.
-
4.
How do the metal ions nickel, cobalt and palladium activate the human innate immune system?
-
A.
These metal ions induce penetration of bacterial TLR ligands into the skin
-
B.
These metal ions bind to and dimerize human TLR4
-
C.
These metal ions induce extracellular matrix degradation
-
D.
These metal ions destroy the skin barrier
-
A.
-
5.
ACD is a T cell-mediated skin disease. Which T cell subsets are the main effector cells of ACD?
-
A.
CD4+ Th2 cells
-
B.
Invariant NKT cells
-
C.
CD4+CD25+ regulatory T cells
-
D.
CD4+ Th1 and Th17 cells, CD8+ Tc1 and Tc17 cells
-
A.
Answers
-
1.
A
-
2.
C
-
3.
C
-
4.
B
-
5.
D
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Martin, S.F., Jakob, T. (2017). Contact Dermatitis. In: Gaspari, A., Tyring, S., Kaplan, D. (eds) Clinical and Basic Immunodermatology. Springer, Cham. https://doi.org/10.1007/978-3-319-29785-9_23
Download citation
DOI: https://doi.org/10.1007/978-3-319-29785-9_23
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-29783-5
Online ISBN: 978-3-319-29785-9
eBook Packages: MedicineMedicine (R0)