
Abstract
In the clinical practice, increased intracranial pressure can drive the patient towards a severe and life-threatening condition. According to a number of clinical observations, the three leading clinical symptoms (headache, vomiting, papilledema) are NOT early symptoms of emergency, since according to the observations, these symptoms can only be detected in 50 % of patients with a cerebral tumor that needs to be operated on. The ophthalmologists are mostly asked to examine the fundus; however, alarming pupillary signs and eye movement disorders can indicate or even precede an increase in intracranial pressure that could evoke the development of a papilledema. Ocular symptoms leading to papilledema are rather poor, as there are no alarming symptoms apart from obscuration (transient darkening of the sight in both eyes for short periods of time). Edema of the optic nerve head developed due to different etiologies show the same clinical signs both in intracranial hypertension and in other systemic diseases (such as inflammation, circulatory disorder). Therefore, in such cases, the significance of differential diagnosis is especially high.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
In the clinical practice, increased intracranial pressure can drive the patient towards a severe and life-threatening condition. According to a number of clinical observations, the three leading clinical symptoms (headache, vomiting, papilledema) are NOT early symptoms of emergency, since according to the observations, these symptoms can only be detected in 50 % of patients with a cerebral tumor that needs to be operated on. The ophthalmologists are mostly asked to examine the fundus; however, alarming pupillary signs and eye movement disorders can indicate or even precede an increase in intracranial pressure that could evoke the development of a papilledema. Ocular symptoms leading to papilledema are rather poor, as there are no alarming symptoms apart from obscuration (transient darkening of the sight in both eyes for short periods of time). Edema of the optic nerve head developed due to different etiologies show the same clinical signs both in intracranial hypertension and in other systemic diseases (such as inflammation, circulatory disorder). Therefore, in such cases, the significance of differential diagnosis is especially high.
The Pathomechanism and Most Frequent Causes of Intracranial Hypertension
Papilledema mostly develops as a consequence of increased intracranial pressure. Causes of intracranial hypertension are different; however, their pathomechanism can be interrelated, such as:
-
intracranial mass
-
disturbances in CSF production, circulation and/or absorption
-
cerebral edema (of metabolic, traumatic, inflammatory as well as circulatory disorder-related origin)
-
spatial disproportion between the skull volume and intracranial content (developmental abnormality)
-
intracranial circulatory disturbance (disturbed cerebral venous flow: e.g., sinus thrombosis)
Overcome by the space-occupying process, the brain can only be dislocated within the bony skull in directions that are allowed by:
-
the falx,
-
the tentorium,
-
and the skull open from below (foramen magnum).
Acute Neurological Consequences of Increased Intracranial Pressure (Intracranial Hypertension, IH)
The slowly enlarging space occupation is initially not accompanied by an increased pressure, due to the effect of compensatory processes. Thus the occupation of space happens at the expense of cerebral and cerebrospinal fluid (CSF) volume. However, reaching the limits of compensatory processes, the intracranial pressure begins to increase rapidly. The relationship between the expansion of the space-occupying process and intracranial pressure is non-linear, and in the end even a small amount of tissue enlargement will result in a rapid and high degree of increase in intracranial pressure. (This is supported by the fact that the drainage of even a small amount of CSF is sufficient to restore the pressure.) Brainstem dysfunction evoked by processes associated with rapidly increasing intracranial pressure, inintracranial hypertension (IH) lead to respiratory disorder, which triggers a further increase in pressure as a vicious circle. This is due to the phenomenon that respiratory disturbance is accompanied by an increased CO2 concentration in the blood, leading to subsequent vasodilation and hyperemia, which result in an increase in cerebral, i.e., total volume inside the enclosed intracranial space. Increased intracranial pressure leads to a progressive deterioration of circulation owing to an immediate decrease in arterial perfusion pressure. This is due the fact that cerebral autoregulation does not work below 50 mmHg (also known as critical cerebral perfusion pressure) and therefore, the cerebral circulation passively follows the cerebral pressure, which leads to a subsequent deterioration of perfusion. If intracranial pressure reaches the mean arterial pressure, the perfusion will be zero, i.e., the cerebral circulation stops. Increased intracranial pressure leads to an increased venous pressure and an increased venous resistance. This plays an important role in the development of cerebral edema.
Suddenly Developing Increased Intracranial Pressure due to Local Circulatory Disturbance
Pathological processes leading to double vision and/or the development of a papilledema are not exclusively caused by space occupation but can also be induced by intracranial circulatory disturbance. For instance, the arteriolization of venous blood (carotid-cavernous fistula, CCF) or a progressive venous congestion (e.g., cerebral sinus thrombosis), which lead to local volume translocation and thus to a subsequent alteration in one of the three components that determine the intracranial pressure. Venous drainage of the optic nerve is in a rather close functional interconnection with venous sinuses of the skull base that play the most important role in the venous drainage of the brain (Fig. 50.1). Therefore, a circulatory disturbance, stasis or thrombosis of these venous sinuses leads to a disturbed venous drainage of the eye in a retrograde manner. Such conditions include the pre-thrombosis of the optic disc accompanied by papilledema and/or eye movement disorder. Figure 50.2 presents the close physiological and therefore, pathophysiological relationship between venous sinuses and the circulation of CSF. Due to this close interconnection, disturbances in the circulation of CSF and in the venous drainage within the central nervous system (CNS) can lead to ocular symptoms. The peculiar blood supply of the brainstem as well as the special cerebral venous network play essential roles in the development of eye movement disorders caused by brainstem dysfunctions due to increased intracranial pressure. (Circulatory disorders of the retina and the visual pathway are discussed in more detailsin Chap. 43.).

Venous drainage of the optic nerve is in a rather close functional interconnection with the venous sinuses of the skull base that play the most important role in the venous drainage of the brain. Kayenbuhl et al. (1968)

Due to the close physiological and therefore, pathophysiological relationship between venous sinuses and the circulation of CSF, disturbances either in the circulation of CSF or in the venous drainage can lead to ocular symptoms. Weed (1923)
Types of Herniation as a Consequence of Intracranial Hypertension
Central (Axial) Herniation
This is most frequently caused by a space-occupying process located in the medial fossa or close to the midline, associated with increased production of edema or a general cerebral edema. Together with a direct downward displacement of the brainstem, increased supratentorial pressure shifts to the posterior fossa and the cerebellar tonsils can be pushed into the foramen magnum. The major causes include non-communicating hydrocephalus, meningitis, diffuse cerebral edema and midline tumors (predominantly that are located in the region of the diencephalon) (Fig. 50.3).

Depiction of the different types of cerebral herniations. Pasztor (1983)
Lateral (Hemispheric) Herniations
Hemispheric i.e., lateral space-occupying processes dislocate the brain medially. In the beginning, the pressure affects merely the diencephalon, similarly to that seen in axial herniation. Further displacements can result in two different forms of herniation:
-
uncal herniation (Fig. 50.3) The further increase in intracranial pressure results in the herniation of the medial part of one of the temporal lobes (uncus and hippocampal gyrus) in the tentorial incisura. This may lead to the development of one of the characteristic ocular symptoms due to the compression of the oculomotor nerve running there. Anisocoria and ophthalmoparesis due to eye movement disorder.
-
cingular herniation: (Fig. 50.3) In case of a lateral increase in intracranial pressure, the paramedian structures can herniate beneath the falx (subfalcine herniation).
The most frequent causes of lateral herniation include intracranial, e.g., subdural and epidural hemorrhages, tumors and sudden intratumoral bleedings.
Infratentorial Space-Occupying Lesion
In case of an infratentorial herniation, the space-occupying process within the posterior fossa leads to a impaction of the anterior-superior part of the cerebellum in the tentorial incisura from below (where the tentorium merges with the falx – straight sinus), whereas in case of a foraminal herination, the process in the posterior fossa herniates into the foramen magnum as a consequence of mass effect.
Foraminal Herniation (Herniation into the Foramen Magnum)
Cerebellar tonsils reach the plane of the foramen magnum in most of healthy individuals. Space-occupying processes growing in the posterior fossa result in the displacement of the tonsils into the foramen magnum, which leads to the compression of the lower brainstem region (Fig. 50.3). The major causes include processes in the posterior fossa such as tumors, hemorrhages, space-occupying lesions of the cerebellar lobes and that expanding towards the central structure, as well as status epilepticus – progressive cerebral edema. Ocular symptoms are not that much informative due to the rapid deterioration of autonomic functions. Only the presence or absence of oculocephalic reflex checked during the careful examination of neck stiffness can provide some additional information (Fig. 50.4).

CT image of a lateral herniation caused by subdural hemorrhage
Symptoms and Signs of Intracranial Hypertension – Papilledema (Synonyms: Swollen Disc or Chocked Disc)
Though the mechanism of the development of papilledema is not known, we may come closer to understanding intracranial hypertension if we make an attempt to think about the factors determining intraocular pressure as an analogy. Intraocular pressure is determined by the relationship of the actual characteristics of the aqueous humor in terms of quantity, production, drainage and absorption; furthermore, the stability or imbalance in the physiological equilibrium developed between the intraocular space-occupying lesion and the arterial–venous circulation of the eye plays a role as well. Within the completely closed intracranial space, an increase in pressure can develop in different pace, of different origin and with different etiopathomechanism.
The Most Frequent Causes of Papilledema
The most frequent causes of papilledema (synonyms include swollen disc or papilledema) are summarized in the table below. Edema of the optic nerve head most frequently develops as a result of intracranial or intraorbital spaceoccupying processes, local vascular processes, and, rarely, inflammatory processes (Table 50.1).
The Clinical Features of Papilledema
Visual Acuity (Vision) and a Decrease in Critical Fusion Frequency (CFF) Value
At the initial, acute stage, increased pressure expanding towards the subarachnoid space does not result in a loss of visual functions, as the numerous small arteries supplying the optic nerve head (e.g., pial end arteries, terminal branches of short ciliary arteries) provide compensatory blood supply despite the increasing pressure and consequent disturbance in venous drainage. With time, however, the permanent increase results in a situation analogous to a pre-thrombotic retinal circulatory condition due to the disturbance of venous drainage, naturally with different etiologies. When a secondary blood supply disorder is permanently present, the decrease in CFF in both eyes will develop as first sign, and the transient episodes of blurred vision subsequently lead to a permanent decrease in visual acuity (Fig. 50.5).

Blind spot enlargement due to papilledema on Bjerrum’s screen and computer perimetry
Visual Field Defects: ‘Blind Spot Enlargement syndrome’
The evaluation of fundoscopic appearance is rather difficult in case of an early papilledema. In case the cooperation of the patient enables, the detection of abnormal size of the blind spot via visual field examination provide the most objective measure of early edema of the optic disc as well as the consequent functional impairment. The enlargement of the diameter of the optic nerve head is caused by the hyperemia of the optic disc, and the subsequent edema developed due to a circulatory disturbance. Due to the subsequent circulatory consequences (obliterated vascular funnel, and later the protrusion of the optic disc also known as prominent optic disc, and finally the presence of peripapillary abnormalities) the diameter of the optic disc and correspondingly that of the blind spot become enlarged. Enlargement of the blind spot can be well tested in a plane surface, i.e., via the examination of the central part of the field of vision by the use of a Bjerrum’s screen and/or computer perimetry (Fig. 50.6).

Visual field defect developed as a consequence of persistent papilledema presents in a right-dominant bilateral concentric constriction of the field of vision, computer perimetry, program G2
The deterioration of the visual field defect is a sensitive marker of untreated or late-diagnosed cases. Permanent intracranial hypertension results in an irreversible loss of nerve fibers manifesting in form of a temporal and subsequently concentric constriction of the visual field. Finally even a ‘tunnel vision’ can develop accompanied by optic disc pallor.
Characteristic Fundoscopic – Ophthalmoscopic Appearance (Frisén’s Scale)
The enlargement of the diameter of the optic disc is caused by the edema of the optic nerve head, which is indicated, in addition to the subjective assessment, by the enlargement of the blind spot as measured by visual field test. Hyperemia of the optic disc is an early sign indicating capillary dilation and a disturbance in circulation. Progressive edema due to a disturbance in venous drainage pushes the papillary nerve fibers apart, which in the beginning gives the optic disc a ‘fibrous’ appearance, and subsequently elevating above the level of the lamina cribrosa the optic disc becomes ‘filled’. Due to the increasing edema, the optic disc progressively protrudes into the vitreous body. The prominence can be assessed by the use of an ophthalmoscope via the measurement of the difference between the diopter value the peripapillary (base) and highest intrapapillary blood vessel (peak) – a difference of 1 mm corresponds to a prominence of three diopters (Fig. 50.7).

Normal state of subarachnoid space surrounding the intraorbital segment of the optic nerve, and tissue abnormalities caused by increased intracranial pressure, which secondarily lead to disturbed cerebral venous drainage (redrawn). Rosen et al. (1998)
Signs of venous circulatory disorder will appear as a consequence of rapidly increasing intracranial pressure due to shifting of increased intracranial pressure to the subarachnoid space surrounding the intraorbital segment of the optic nerve. This results in a subsequent deceleration of the reflux of venous blood from the retina, leading to a stasis in intraocular retinal veins.
This can be observed through the tortuosity of veins surrounding the choked disc, which subsequently become accompanied by signs of perivenous hemorrhages and metabolic disturbance. Disturbance of venous drainage can be so severe as the process deteriorates that the margins of the optic disc can be covered by the bleeds leaking from the damaged veins.
In the event of a central retinal vein (trunk) thrombosis, hemorrhages expand towards the peripheral segments of the venous branch as well, which is an essential sign from differential diagnostic point of view. As a consequence of long-lasting untreated intracranial hypertension, exudates and soft degenerative foci appear on fundoscopy, which are already associated with nerve fiber damage. On fundoscopy, the disturbance in retinal blood supply is indicated by the presence of perimacular folds (also known as ‘Spritz figur’ in the German terminology). In chronic papilledema, the margins of the optic nerve head become almost sharp, surrounded by organized edema.
At the same time, the optic disc becomes pale, i.e., porcelain-white, and the visual functions severely deteriorate, which is followed by a concentric constriction of the field of vision (Table 50.2).
Stages of Papilledema (Frisén’s Scale)
In the next two figures, fundoscopic images of early papilledema highly characteristic of Frisén stage one can be seen with blurred nasal optic disc margin and intact temporal optic disc margin (Fig. 50.8).

Frisen stage two papilledema. Concentric blurred margins and the diameter of the optic nerve head is increased
Whereas in the fundoscopic image highly characteristic of Frisén stage three, the concentrically blurred and elevated (prominent) optic disc is accompanied by obscured blood vessels coursing in and out of the optic disc, and the peripapillary halo becomes irregular with finger-like extensions (Fig. 50.9).

Frisén stage three papilledema. Concentric obscuration of a proportion of blood vessels radiating from the optic nerve head and of all borders of the optic disc can be observed, the margins of the optic disc become concentrically elevated, the diameter of the optic nerve head is increased
Differential Diagnosis of Papilledema
In the early and acute phase of papilledema developed as a consequence of intracranial hypertension, the visual functions remain intact for a long period. However, antechiasmal optic neuropathies caused by circulatory disorder such as anterior ischemic optic neuropathy (AION) as well retinal trunk thromboses do not only present with a similar initial fundoscopic appearance but also with a remarkable deterioration of vision at the onset. (This is discussed in more details in Chap. 43.).
In inflammatory processes (such as multiple sclerosis) – except for papillitis – the deterioration of visual functions is not accompanied by any sort of fundoscopic abnormality. In addition to a comprehensive ophthalmological and neurological medical history, the sound and long-term examination documentation represents a true support for the examiner.
Among diseases resulting in intracranial hypertension, benign intracranial hypertension (BIH) also known as pseudotumor cerebri has a special position. Its diagnostic criteria include narrow cerebral ventricles in the absence of intracranial spaceoccupying lesion on CT or MRI scan, in addition to a bilateral papilledema and the general symptoms and signs of increased intracranial pressure (abducens palsy, headache) (Table 50.3).
Besides, the CSF pressure is mostly increased. Cerebral venous circulatory disorders (sinus thrombosis or stasis) as well as primary and secondary pathologies of CSF dynamics comprise the main syndromes in this group.
Symptoms and Signs of Intracranial Hypertension – eye Movement Disorders
The aligned gaze of eyes looking straight ahead can be assessed in the outpatient clinic as well as in unconscious patients (this is called primary position) The precise documentation of pupil size, their difference in size as well as the pupillary responses are, however, essential during the bedside examination of an inpatient. This is because an initial anisocoria or the clinical signs of a unior bilateral afferent or efferent pupillomotor pathway lesion can be the most important warning signs of initial or even progressive cases of intracranial hypertension associated with different degrees of impaired consciousness. Eye movement disorders and/or pupillary symptoms and signs may have an alarming role especially if they precede the development of a papilledema. Therefore, in the everyday clinical practice the examination of the eye movement system is a task for the ophthalmologist, in addition to fundoscopy. Signs of eye movement system dysfunctions are classified hereby based on the typical associating type of herniation, which may be of help in the localization diagnosis. The particular types of eye movement disorders are discussed in details in Chaps. 54 and 55, respectively.
Central–axial herniation is most frequently caused by a space-occupying process located in the medial fossa or close to the midline associated with increased production of edema or a general cerebral edema. This is associated with a direct downward displacement of the brainstem.
Major causes:
-
non-communicating hydrocephalus
-
meningitis
-
diffuse general edema
-
midline tumors (especially in the region of the diencephalon)
Symptoms and Signs
The efferent parasympathetic (pretectal region of the mesencephalon) fibers and the trineuronal sympathetic pathways can damage separately or jointly (sympathetic–central fibers originating from the diencephalon descend through the midbrain, the pons and the dorsolateral part of the medulla towards the lateral funiculus of the cervical spinal cord, where they synapse; the preganglionic nerve fiber originating from here and traveling along the superior thoracic motor nerve root synapses in the superior cervical ganglion, from where the fibers run with the carotid plexus and eventually reach the pupillary sphincter muscle located in the iris in the eyeball.
Eye Movement Disorders Caused by Central Herniation
In central herniation, the brainstem suffers direct or indirect compression, and, therefore, brainstem dysfunctions predominate. Diencephalic syndrome
-
Pupils (sympathetic effect): constricted, responsive
-
In case of a diencephalic compression, a moderate response to light and slightly constricted pupils can be seen. The pathological background is in part the absence of pupil-dilating effect of sympathetic fibers, with intact a pupil-constricting parasympathetic functions
-
Increased oculocephalic reflex: the doll’s eye phenomenon: the head is tilted backward and to the side. If the brainstem is intact, the eyeballs move towards the contralateral direction, whereas if the brainstem is damaged, the eyeballs move towards the direction of the tilting, passively following its direction
-
Eye movement disorder: upward gaze palsy – downward gaze of the eyes
-
Injury to nuclei controlling vertical eye movements and their internuclear fibers: functional interconnections between the diencephalon and midbrain are also affected. Bell’s phenomenon: on forced closing of the eyelids, the bulbs roll upward and to the lateral side corresponding to a normal innervation
-
Injury to the upward gaze center: Bell’s sign is intact or is absent only in cases when the afferent fibers or the nucleus itself or its surrounding is damaged
Midbrain Damage
Pupillary symptoms and signs:
-
midbrain tectum: bilaterally dilated, unresponsive pupils with hippus
-
lesions of upper brainstem tectal and midbrain nuclei and fibers (with predominant involvement of parasympathetic fibers but affecting the sympathetic fibers as well) lead to the development of fixed, dilated, unresponsive pupils
-
in case of an isolated compressive injury to the midbrain, pupils remain midsize, but are unresponsive on both sides, which is probably due to the damage of both sympathetic and parasympathetic fibers
-
cranial nerve (uncal herniation): unilaterally dilated, unresponsive
-
oculocephalic reflex: decreased
Signs of Medullary – Pontine Lesions
-
pupill: pinpoint
-
in case of a pontine compressive lesion, pinpoint – myotic – pupils develop because the parasympathetic pathway already exited from the brainstem and only the sympathetic fibers travel along this region, which due to the extended injury of the sympathetic fibers results in the predominance of the parasympathetic effect.
Injury to the Lower Pons-Medulla Oblongata
-
coma, irregular respiration, and severe autonomic symptoms and signs are accompanied by:
-
eye movement disorder – the characteristic ‘ocular bobbing’: a rapid downward movement of the eye followed by a return to the midline
-
oculocephalic reflex: lost
-
pupillary sign: unilateral central Horner’s syndrome, i.e., unilaterally constricted pinpoint pupil can be observed in case of a lateral pontomedullary brainstem compression (as well as in case of a cardiovascular origin as a part of Wallenberg’s syndrome)
Different Forms of eye Movement Disorders due to Lateral Hemispheric–Uncal Herniation
They are mostly observed in association with hemispheric space-occupying processes.
Most frequent causes
-
intracranial hemorrhage
-
subdural, epidural hemorrhage
-
tumor, intratumoral hemorrhage
Ocular symptoms:
-
Oculomotor palsy: The oculomotor nerve exiting from the brainstem gets under compression due to the mass effect of the herniating brain part. Lateral herniation is most frequently associated with oculomotor nerve compression, by means of the herniation of the uncus of the hippocampal gyrus beneath the edge of the tentorium. This is the characteristic uncal – downward transtentorial herniation. Its signs include miosis, which is followed by a slightly responsive pupil, and in the end of the process, a pupil unresponsive to contralateral lighting, this is anisocoria. Pupillomotor fibers traveling superficially within the cranial nerve are highly exposed to suffer injury due to compression; therefore, the first sign of a direct impact on the oculomotor nerve is the decrease in pupillary response (Fig. 50.10 – depiction).
Fig. 50.10 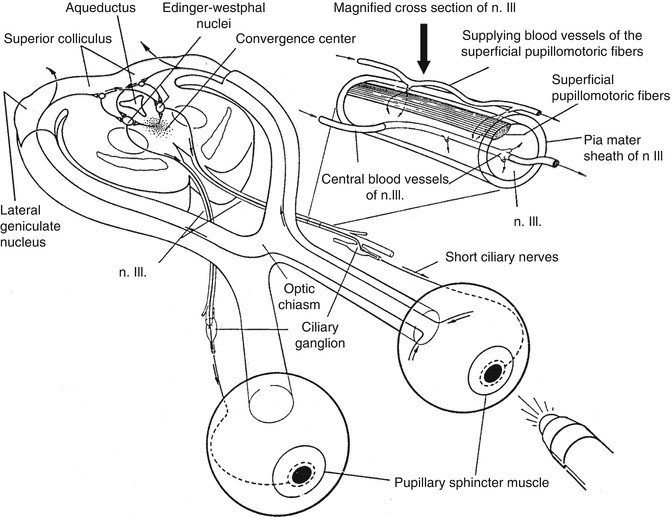
The afferent and efferent routes of the parasympathetic pupillomotor pathway. In the upper-right quadrant of the Figure: magnification of a section the oculomotor nerve emphasizing the external therefore, more vulnerable pupillomotor fibers (Redrawn after Peter 1989)
-
abducens nerve palsy: long-lasting intracranial hypertension can cause uni- or bilateral compression of the abducens nerve – the etiopathomechanism is not entirely clear, but they most frequently occur in slowly enlarging skull base tumors
-
nystagmus and cerebellar symptoms and signs can be observed as a consequence of brachium pontis compression

Initial neurological symptoms: nausea, headache, vomiting, and then apathy. Subsequently, long tract symptoms, pyramidal signs and paresis occur. The later signs include decerebrate (extensor) posturing and cerebellar fits due to brainstem herniation (these are already signs of central herniation).
Foraminal Herniation (Herniation into the Foramen Magnum)
Cerebellar tonsils reach the plane of the foramen magnum in most of the healthy individuals. Space-occupying processes growing in the posterior fossa result in the displacement of the tonsils into the foramen magnum, which leads to the compression of the lower brainstem region.
Major causes:
-
tumors, hemorrhages located in the posterior fossa
-
space-occupying lesions of the cerebellar lobes and that expanding towards the central structure
-
status epilepticus – progressive cerebral edema.
Ocular symptoms are not that much informative due to the rapid deterioration of autonomic functions. Only the presence or absence of oculocephalic reflex checked during the careful examination of neck stiffness can provide some additional information.
As a continuation of supratentorial herniation, the tonsils of the cerebellum herniate into the foramen magnum. The upper part of the brainstem suffers damage, and subsequently, the compression of the medulla oblongata leads to the following signs: the irregular respiration becomes shallow, the pulse is irregular and filiform. The infratentorial process can evoke sudden respiratory paralysis. In the beginning, the consciousness is preserved. However, later, the diffuse occipital headache may be accompanied by neck stiffness and an abnormal posture of the head.
General Therapeutic Guidelines in Intracranial Hypertension
The potential therapeutic tools include the monitoring of intracranial pressure (it has prognostic significance), ventilation, oxygen supplementation, decreasing hypercapnia, the application of osmotics, diuretic treatments, the use of hyperosmotic Mannitol solution.(it increases the osmolality of the blood while decreasing the edema and the viscosity of the blood), the administration of corticosteroids (they decrease vasogenic edema and the production of CSF), neurosurgical interventions, decompression surgeries, the application of ventricular or lumbar drain). The most frequent causes of intracranial hypertension and their therapeutic options are summarized in Table 50.4.
The Most Frequent Causes of Intracranial Hypertension and Their Therapeutic Options
Edema of the optic nerve head and pupillomotor signs can indicate (or even predict) the early intracranial hypertension, i.e., they may have an alarming role. Timely examinations and the differential diagnostic approaches do not only lead us to adequate medical therapy and a neurosurgical intervention if necessary, but may also prevent the development of potentially life-threatening conditions. Furthermore, we can save our patients from the development of an irreversible loss of vision or bilateral blindness caused by a late diagnosis.
References
Frisén L. Swelling of the optic nerve head: a staging scheme. J Neurol Neurosurg Psychiatry. 1982;45:13–8.
Kayenbuhl H, Yasargil M. Cerebral angiography Ed. 2. 1968. In: Miller N, Neman N, editors. Walsh & Hoyt’s: clinical neuro-ophthalmology, 1956. 2005.
Pasztor E. Operalhato idegsebeszeti betegsegek. 60. Medicina; 1983.
Peter D. Topical diagnosis in neurology. Thieme; 1989.
Rosen ES, et al. Neuroophthalmology. London: Mosby Ltd; 1998.
Weed LH. The absorption of cerebrospinal fluid into the venous system. Am J Anat. 1923; 31: 191–221. Miller N, Neman N. Walsh & Hoyt’s: clinical neuro-ophthalmology, 1950. 2005.
Further Readings
Albright A, et al. Occult hydrocephalus in children with cerebral palsy. Neurosurgery. 2005;56(1):93–7.
Brandt T. Vertigo: its multisensory syndromes. London: Springer; 1991. p. 233–77.
Brandt T, et al. Neurological disorders (course and treatment). San Diego: Acad Press; 1996. p. 571–2.
Crassare I, et al. Cerebral venous thrombosis. J Neuroophthalmol. 2004;24(2):156–63.
Ewerback H. Gyermekkori elkülönítő diagnosztika[Pediatric differential diagnostics]. Budapest: Medicina; 1989. p. 181–4 (In Hungarian).
Glaser JS. Neuroophthalmology. Philadelphia: Lippincott; 1990. p. 115–23.
Korányi K. A pangásos papilla jellemzői és differenciáldiagnosztikája [Characteristics and differential diagnoses in congested papilla]. In: Somlai J, editor. Neuroophthalmologia. Budapest: Literatura Medica; 1996. p. 129–34 (In Hungarian).
Maródi L, et al. Gyermekgyógyászat [Pediatrics]. Budapest: Medicina; 1998. p. 666–9 (In Hungarian).
Miller N, Neman N. Walsh & Hoyt’s: clinical neuro-ophthalmology. 1950. p. 2005.
Miller NR, Newman NJ. Papillaoedema. In: Walsh & Hoyts clinical neuro-ophthalmology. VIth ed. Philadelphia: Lippincott; 2005. p. 237–92.
Minns RA, et al. Cerebrospinal fluid pressure in pyogenic meningitis. Arch Dis Child. 1989;64:814–20.
Pásztor E. Operálható idegsebészeti betegségek [Operable neurosurgical diseases], 60. Medicina; 1985 (In Hungarian).
Rabinstein AA. Treatment cerebral edema. Neurology. 2006;12(2):59–73.
Somlai J, Kollár Gy, Szeifert Gy. Gyermekkori papillaoedema differenciál diagnosztikája [Differential diagnostics in pediatric papilloedema]. Gyermekorvos Továbbképző Szemle. 2006; IV (In Hungarian).
Somlai J et al. A koponyaűri nyomásfokozódás figyelmeztető tünetei: jellegzetes szemmozgászavarok és pupillomotoros funkciózavarok [Warning signs in increasing intracranial pressure: characteristic disorders of eye movements and pupillomotor dysfunctions]. Balatonaliga: Magyar Szemorvos Társaság; 2003 (In Hungarian).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Somlai, J. (2016). Ocular Symptoms and Signs of Intracranial Hypertension. In: Somlai, J., Kovács, T. (eds) Neuro-Ophthalmology. Springer, Cham. https://doi.org/10.1007/978-3-319-28956-4_50
Download citation
DOI: https://doi.org/10.1007/978-3-319-28956-4_50
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-28954-0
Online ISBN: 978-3-319-28956-4
eBook Packages: MedicineMedicine (R0)