
Abstract
Transverse vaginal septa are a rare type of mullerian anomaly that results from failed fusion or canalization of the vaginal plate and the caudal end of the mullerian ducts. Septa are most commonly imperforate and manifest as primary amenorrhea, abdominal pain, and hematocolpos in adolescence. Perforate septa have a more variable presentation, usually associated with the foreshortened vagina and can present in adolescence or young adulthood. Proper diagnosis is made with clinical exam and imaging, usually Magnetic Resonance Imaging (MRI). Surgical management is highly dependent on the thickness and location of the septum and includes vaginal and abdominoperineal procedures. The patients’ age, developmental level, and ability to perform postoperative dilation should be considered when exploring surgical options, since prolonged dilation is often indicated in the postoperative period. Long-term complications include vaginal stenosis and re-obstruction, which may require repeat surgery. The risk of endometriosis increases with imperforate septa that are located higher in the vagina. There is limited data available on reproductive outcomes, but vaginal births have been reported.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Mullerian anomaly
- Transverse
- Vaginal septum
- Distal vaginal agenesis
- Imperforate
- Hematocolpos
- Hematometra
- Obstruction
- Vaginal stenosis
- Dilation
Introduction and Incidence
Transverse vaginal septa are a rare type of mullerian anomaly that results from failed fusion or canalization of the vaginal plate and the caudal end of the mullerian ducts, leading to a complete or partial blockage of the vaginal canal. The exact incidence is not known and estimates ranging between 1:21,000 [1] and 1:84,000 [2] are based on limited data. Transverse vaginal septa are unlikely to be associated with other mullerian anomalies; however, there are case reports of transverse septa with a septate uterus [3], unicornuate uterus, and hymenal abnormalities [4–6]. Concurrent renal anomalies, as seen with other mullerian anomalies, occasionally occur with transverse vaginal septa [7].
There is no accepted classification system for congenital vaginal anomalies among the American and European gynecologic societies. The American Society for Reproductive Medicine (ASRM) classification for mullerian anomalies only includes vaginal agenesis and hypoplasia (Type 1A), however does allow for the description of associated vaginal anomalies [8]. The European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE) include transverse vaginal septa, but only as a subclass (V3) in their classification system for mullerian anomalies [9]. There have been several proposed classification systems for vaginal anomalies, including the VCUAM classification and an embryological-clinical based system [10–12]. See Chap. 1 for more details.
Transverse vaginal septa have a variety of characteristics including position in the vagina, thickness, and presence of perforations. Position is generally described as low, mid, or high (Figs. 4.1 and 4.2), though there is no accepted system for classifying the location and a variety of measurements are used in the literature. In a recent observational study, the largest to date, septal location was described as the distance measured in clinic or during an exam under anesthesia between the vaginal introitus and the distal end of the septum [13]. Septa were classified as low if less than 3 cm, mid position if between 3 and 6 cm, and high if greater than 6 cm from the introitus. In this study, the most common location was low (72 %), followed by mid position (22 %), and high (6 %) [13]. In a review of the literature from 1966 to 1997, location of the septum was reported in 67 patients and described as low (distal 1–3 cm) in 20 %, mid (4–5 cm) in 33 %, and high (>6 cm) in 47 % of patients [14].

Location of transverse vaginal septum

Diagram showing location of High (1), Mid (2), and Low (1) transverse vaginal Septum in pelvis
The thickness of septum is the most important characteristic in terms of surgical planning. Septa are considered thin if less than 1 cm and thick if greater than 1 cm [15] (Figs. 4.3 and 4.4). Fortunately, most septa are less than 1 cm in thickness [8, 16]; however, in about 15 % of cases a several centimeter thick septum is present and can be considered partial vaginal agenesis or atresia [17]. In general, thicker septa occur higher in the vagina [18]. Most (61–65 %) transverse septa are imperforate [13, 14]. When a perforation is present, it is usually small and centrally located, but eccentric, bilateral, and multiple perforations have also been described [14] (Fig. 4.5).

Thick transverse vaginal septum (distal vaginal agenesis)

Diagram showing location of thick transverse vaginal septum in pelvis

Transverse vaginal septum with microperforation
Etiology
Embryologic development of the vagina begins around 9 weeks gestation, when the distal mullerian ducts fuse to form the uterovaginal canal. The mullerian ducts contribute to the upper portion of the vagina, whereas the lower portion arises from the urogenital sinus. At 12 weeks the sinovaginal bulbs develop as two solid evaginations from the mullerian tubercle on the urogenital sinus. The sinovaginal bulbs grow into the uterovaginal canal and develop a solid vaginal plate of stratified squamous epithelium [8]. The solid vaginal plate proliferates toward the cephalad direction, replacing the original mullerian epithelium with squamous epithelium [2]. It then cannulates which is complete by 5 months gestation. The hymen, which typically perforates at birth, originates from the caudal end of the sinovaginal bulbs [8].
The embryologic etiology of transverse vaginal septa is controversial and cannot be solely explained by failed fusion of the urogenital sinus and mullerian ducts; this would lead to formation of transverse septa in the lower one-third of the vagina only, while in fact, septa can be located at many different levels in the vagina (Figs. 4.1 and 4.2). It is hypothesized that the squamous epithelium that invaginates from the vaginal plate can leave behind vestigial shreds during canalization causing septa to form at different locations in the vagina [14, 19].
Isolated vaginal anomalies likely have a polygenic or multifactorial inheritance pattern. McKusick-Kaufman Syndrome (MKS) is an autosomal recessive condition caused by mutations in the MKKS gene. In females with MKS, transverse vaginal septa as well as vaginal agenesis or imperforate hymen are found in association with polydactyly and congenital cardiac defects [20, 21].
Differential Diagnosis
When a patient presents with an obstructive vaginal anomaly, clinicians should consider imperforate hymen, transverse vaginal septum, cervical agenesis, and vaginal atresia in the differential diagnosis . An imperforate hymen, the most common obstructive anomaly, can easily be diagnosed with visualization. Though the presence of a patent hymen can usually be confirmed at an early age on genital examination, an imperforate hymen is often not recognized until after menarche. Typically, a membranous bulge is seen at the introitus and the hymen presents as a solid plate. The mass increases with a valsalva maneuver and can be confirmed on rectal examination with a low lying bulge, extending almost to the rectal orifice [8, 16, 17]. See Chap. 3 for more details.
Cervical agenesis, congenital absence of the cervix and/or upper vagina, is a rare anomaly that is important to diagnosis correctly. Absence of a cervix on MRI is the feature that distinguishes this anomaly from other obstructive anomalies [8]. Details on the presentation and management are discussed in Chap. 5. Vaginal atresia, or agenesis of the lower vagina, occurs when the lower vagina fails to develop from the urogenital sinus and is instead replaced by fibrous tissue. This leads to an obstructed upper vagina and clinically presents like an imperforate transverse septum. Examination of the external genitalia reveals a normal hymen, vaginal dimple and on rectal exam a high bulge is palpated from a blood filled upper vagina [8, 16]. Adolescents with complete vaginal agenesis (MRKH) who have uterine remnants with functioning endometrium can also present with obstructive symptoms [16]. This should be considered in patients with a vaginal dimple who do not have a palpable bulge on rectal exam. Most of these anomalies can be diagnosed correctly with a proper physical exam, including a rectal exam, and appropriate imaging.
Patients with a perforated transverse vaginal septum have a more variable presentation which does not include amenorrhea. The differential diagnosis includes all conditions and anomalies that preclude visualization of the cervix, inability to place tampons, dyspareunia, or inability to have intercourse.
Diagnosis
Presentation
A transverse vaginal septum can be diagnosed during infancy, childhood, adolescence, or adulthood. The symptoms vary and are dependent on whether the septum is imperforate or perforate. A complete vaginal transverse septum leads to obstruction of the outflow tract, which presents as mucocolpos during infancy or hematocolpos shortly after menarche. Incomplete vaginal septa are usually diagnosed at a later age with a more variable presentation.
-
Complete (imperforate) transverse vaginal septum: The most common presentation, usually occurring 2–3 years after thelarche, is primary amenorrhea with worsening cyclic pelvic pain. Hematocolpos and sometimes hematometra develops from accumulated menstrual blood which in extreme cases may present as an abdominopelvic mass. Patients complain of moderate to severe pain located in the abdomen, pelvis, or back. Pain can be significant enough to cause nausea and vomiting as well as school absences and frequent visits to the pediatrician or emergency department [17]. Adolescents with a high septum tend to present earlier because the upper vagina and uterus distend quickly with blood, causing severe pain [16]. In a series of 46 patients with transverse vaginal septa, 61 % were imperforate, diagnosed at a mean age of 14.3 years with primary amenorrhea and pain due to obstructed menstruation. One patient presented with cyclical hematuria due to a vagino-vesical fistula [13]. Though rare, obstructions can develop in the neonatal period as a result of increased vaginal and cervical secretions from exposure to maternal estrogen. In infants, a large hydrometrocolpos can cause symptoms related to compression of the ureters, rectum, and vena cava, which can be life threatening from resulting cardiorespiratory failure [22, 23].
-
Incomplete (perforate) transverse vaginal septum: Patients with a perforate septum usually have a normal menarche and are more likely to present in late adolescence or young adulthood with complaints of difficulty inserting tampons, dyspareunia, dysmenorrhea, or infertility. Pyocolpos from an ascending infection, abnormal discharge, or abnormal bleeding can also occur in the setting of a partial obstruction, but is more uncommon [13, 14, 24]. The reported mean age of diagnosis is 24 years [13].
Physical Examination
-
Complete (imperforate) transverse vaginal septum: Visualization of the external genitalia should reveal a normal open hymenal ring, which helps to distinguish a transverse septum from an imperforate hymen. In the young adolescent, a small and lubricated Q-tip can sometimes be used to assess the distance from the hymen to the obstruction. The physician should avoid touching the hymen, which is especially sensitive and causes pain in many young patients [17]. For those that can tolerate a speculum or digital exam, the vagina appears short and is often described as a “blind pouch.” If the septum is thin, a bulge might be palpated or seen in the vagina from the distended upper vagina. A rectal exam, which is often better tolerated than a vaginal exam, can help delineate the lower edge of the septum by measuring the distance from the rectal opening to the bottom of the vaginal bulge (Fig. 4.6). If the obstruction is high or longstanding, an abdominal mass due to a distended vagina and uterus can be palpated [16, 24, 25].
Fig. 4.6 
Diagram of transverse vaginal septum with distended upper vagina that may be palpated on rectal exam
-
Incomplete (imperforate) transverse vaginal septum: Since these patients usually present at a later age, a pelvic exam with a speculum is generally tolerated. The external genitalia and hymen are normal and upon insertion of the speculum a short vagina is noted and no cervix is seen; the length of the lower vagina is dependent on the location of the septum. The septal perforation opening can usually be identified by inspection or gentle probing with a Q-tip. If no opening is seen, the patient should be reexamined during her menses, as blood can aid in identifying a microperforation (Figs. 4.7 and 4.8).
Fig. 4.7 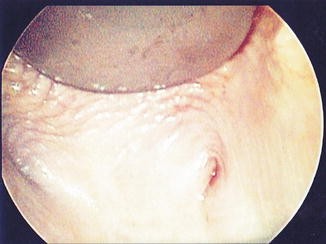
Transverse vaginal septum microperforation (image provided by Samantha M. Pfeifer M.D.)
Fig. 4.8 
View of cervix via hysteroscope passed through microperforation in transverse vaginal septum (image provided by Samantha M. Pfeifer M.D.)



Laboratory Studies
Laboratory studies do not aid in the diagnosis of a transverse vaginal septum. If tumor markers are drawn as part of the evaluation of the abdominopelvic mass, then CA 125 and/or CA 19-9 may be elevated [26].
Imaging
A pelvic ultrasound is typically the first line imaging modality for gynecological structures but is limited in evaluating complex anatomy. Three-dimensional (3D) ultrasound has been found useful in diagnosing uterine malformations; however, studies on the efficacy of 3D ultrasound in diagnosing vaginal anomalies are limited [27]. MRI is highly specific and sensitive for identifying mullerian tract anomalies, while also providing information on associated genitourinary abnormalities. Since an adequate MRI requires the patient to lie still for a period of time, general anesthesia or sedation may be necessary in young girls or anxious adolescents. Though MRI is more expensive than Computed Tomography (CT) scan, it provides high resolution and detailed images of the anatomy without exposure to radiation [28].
In general T2 weighted sequences are most helpful in evaluating internal pelvic structures. The zonal anatomy of the uterus, cervix, and vagina are delineated with varying signal intensities; the vagina has bright mucosa with a darker submucosa. T1 weighted sequences do not depict zonal anatomy but are helpful in delineating obstructed blood flow, which appears as a bright signal [29].
The literature supports the use of MRI as the gold standard for evaluation of upper mullerian tract anomalies; however, MRI evaluation of the vagina is more challenging [30]. In a retrospective review of 44 patients with a variety of congenital anomalies of the genitourinary tract, 30 of which had abnormal vaginal anatomy including vaginal agenesis, there was a 6.8 % discordance between clinical and imaging findings on the first review. This study emphasizes the importance of a multidisciplinary discussion about the clinical and MRI findings to aid in final and correct diagnosis of vaginal anomalies. The caudal end of the urethra, located at the same level of the hymen, can be used as an anatomical marker for the introitus when measuring vaginal length on MRI (Fig. 4.9). With transverse vaginal septum, there should be clear identification of the cervical canal to differentiate from cervical agenesis (Fig. 4.10).

(a, b) MRI sagittal T2 weighted images of transverse vaginal septum demonstrating clear cervix and distended upper vagina superior to symphysis. (c) MRI image of imperforate hymen (image provided by Samantha M. Pfeifer M.D.)

MRI, T2 weighted image, view of cervix. (a) clear cervical canal (b) distended uterus, cervix, and vagina, making identification of cervix more difficult (image provided by Samantha M. Pfeifer M.D.)
Another technique for marking the introitus on MRI is placement of external oil beads at the level of the hymen prior to imaging [31]. Surgilube, which acts as a contrast agent, can be placed in the vagina to help delineate complex vaginal anomalies, or when the vaginal walls are collapsed, as is the case with a perforate transverse vaginal septum [32]. While some report the use of tampons as helpful in highlighting the vagina, others report that tampons obscure vaginal wall anatomy in MRI [31, 33].
-
Complete (imperforate) transverse vaginal septum: The initial diagnosis of obstruction is often made with ultrasound by identifying a cystic mass in the vagina and/or a uterus distended with blood products. This provides the diagnosis, but does not give enough detail of the anatomy, location, and thickness of the septum. Because surgical technique changes based on the location and thickness of the septum, attempts should be made to fully characterize the septum preoperatively by MRI.
-
Incomplete (perforate) transverse vaginal septum. Imaging for the thickness of the perforate transverse septum is more challenging, as the anatomy is harder to characterize with collapsed vaginal walls. In these cases, MRI can be considered using the above-described techniques.
Treatment
The goals of treatment are to relieve the obstruction if present and restore anatomy so that the vagina can function for menstrual outflow and coitus. Anomalies that are obstructive require immediate attention to resolve symptoms, whereas surgical resection of a perforate septum is elective. Hormonal suppression of menses with delay in surgery can be considered while the appropriate testing is performed. The patients’ age, developmental level, and ability to perform postoperative dilation factors into the decision making and in certain cases, longer delays to surgery may be necessary.
The location and especially the thickness of septum are important characteristics in terms of surgical planning. In general, low and thin septa are less complicated, easier to resect, and require less postoperative care.
The outer surface of a transverse septum resembles normal vaginal mucosa and histologically is stratified squamous epithelium. The histopathology of the obstructed side of the septum varies, but in general the upper vagina is lined with glandular columnar epithelium and typically appears more erythematous. After resection of the septum, the upper vagina will undergo a metaplastic process and transform into squamous epithelium [23, 24].
Primary Resection and Anastomosis
Treatment of a thin septum is typically straightforward and requires resection of the septum followed by end-to-end anastomosis of the upper and lower vaginal mucosa. After placement of a catheter to keep the bladder drained, the initial incision should be made in the center of the septum, with an assistant using abdominal pressure to create or increase a bulge. If a bulge is not easily appreciated, then transabdominal ultrasound can be used to help establish a connection to the upper vagina. A spinal needle, under ultrasound guidance can be used to find the obstructed space, a wire is then placed in the obstructed area and sequential dilation of the septum over the wire can subsequently be performed. The incision is then stretched and obstructed blood evacuated. The inner vaginal walls and cervix should be palpated before resecting the residual septum. Resection of the septum in its entirety decreases the risk of stenosis and re-obstruction [34]. If the septum is high in the vagina, a Foley catheter can be placed through the initial incision and behind the septum. The catheter balloon is then filled with saline and pulled against the septum, which allows for easier resection of the septum [35].
The upper and lower vagina should be re-approximated with a delayed absorbable suture (such as 3-0 polysorb) in an interrupted fashion to minimize postoperative constriction [34]. Anastomosis tends to be easier when the upper vagina is distended with menstrual blood, by expanding the upper vaginal walls and providing more tissue for surgery [15].
Resection of thick septa is associated with increased risk of injury to nearby structures including bowel, bladder, and cervix. Surgical correction of a thick septum is more complicated and often requires undermining and mobilization of the upper vagina to aid in re-anastomosis without tension on the suture line (pull through procedure). The initial incision into a thick septum can be challenging; however, there are several techniques that can aid in establishing the connection between the upper and lower vagina. Interventional radiology can be consulted to place a catheter through the septum into the distended upper vagina under ultrasound guidance. The septum is then carefully resected around the catheter, paying special attention to orientation and nearby structures [34]. Another option is utilizing a transabdominal or laparoscopic approach to resect a high septum, an approach that works better when the upper vagina has been dilated with blood products. The push through technique is another option for thick transverse septa. After creating a bladder flap, the upper vagina is opened (with care taken not to enter through the potentially dilated and thinned cervix) and the obstructed blood is removed. A blunt object, such as a sterile marble, is placed in the upper vagina. Tension from the sterile object allows for better visualization and easier resection of the septum vaginally [35]. Alternatively, a sound can be passed through the fundus and into the upper vagina in an effort to help identify the vaginal septum from below [25].
A Z-plasty incision may help prevent circumferential scarring by changing the axis of the suture line so that scar contracts in a longitudinal fashion rather than a transverse fashion. The first step in performing a Z-plasty is making two oblique and crossed incisions over the lower edge of the vaginal septum. Using oblique incisions minimizes risk of injury to the bladder and rectum. The vaginal tissue is then undermined, creating four triangular shaped mucosal flaps of vagina, which can be tagged with suture to help with orientation and traction. The connective tissue in the septum should then be sharply dissected off the vaginal wall and removed. The inner vaginal lining of the septum is then incised with two crossed incisions, rotated 45° from the outer incisions. The flaps are undermined until mobilized enough for anastomosis. The apex of each flap is joined to the basal intersection of the two opposite flaps to form a continuous Z-plasty. This technique (Garica Z-plasty \with Grunberger modification) was successfully performed on a series of 13 patients with both obstructed and nonobstructed transverse vaginal septa. In this series, the thickness of septa ranged from 2 to 3.5 cm and patients were followed for a mean of 6.3 years postoperatively. Vaginal lengths ranged from 9 to 12 cm and there were no patients with signs of vaginal contracture. Eight of the patients were known to eventually have a vaginal delivery [7].
Resection of a thick septum has the potential to leave a gap between the distal and proximal vagina. If native vaginal tissue cannot be mobilized enough to cover the resected area, other tissue is needed to create a patent vaginal canal. Options for closing this gap include use of bowel, skin, or buccal mucosal grafts. The disadvantages of skin grafting include risk of postoperative vaginal stenosis and scarring at the graft site [13]. Bowel interposition, a much larger operation, is associated with less stenosis and usually does not require postoperative dilation; however, patients do report copious vaginal discharge [24]. Vaginoplasty with buccal mucosa offers many advantages over skin grafting and bowel interposition; it eliminates the need for abdominal surgery, provides moist pliable mucosa without hair, and has a hidden donor site [36, 37]. Postoperative mouth pain is usually short and well tolerated. Vaginal tissue engineering is a promising option for vaginal reconstruction and has been used successfully in small numbers of patients with MRKH [38]. Postoperative hospital admission should be considered if a graft is used, requiring immobilization and Foley catheter use.
The risk of postoperative scarring and stenosis of the surgical area is higher with the thick septa and may require repeat surgery [13]. Postoperative dilation is recommended for most septal resections, however given the rarity of these anomalies, there is minimal outcome data and little information about the best method for postoperative dilation. In the original description by Rock in Telinde’s Gynecology, a hollow vaginal mold was used that allowed outflow of menstrual blood. Typically silicone dilators or vaginal molds made of soft foam and covered with a latex condom are used. If the dilator is small enough to fit above the levator ani muscles, it will usually stay in the vagina without any additional support [23]. Custom made molds (10.5 cm in length with a diameter of 2.6 cm) with harness-like belts to keep the dilator in place have been described [39]. Alternatively, the use of tight spandex shorts can be helpful in keeping firm dilators in the vagina for prolonged periods of time. Postoperatively, after resolution of hematometra, the patient should wear a vaginal stent or dilator continuously for around 2 months to prevent stenosis or re-obstruction. Patients should be advised that they may need to remove the dilator for bowel movements or urination. If the surgical site is healing well and there are no complications, dilator use can be decreased to nighttime only for several more months and then intermittent until sexual activity is started [34]. Frequent vaginal examination will help to individualize dilator use.
Short-term and long-term complications of vaginal septum resection include bladder, bowel, and cervical injuries during surgery, infection, and vaginal stenosis or re-obstruction. A bladder catheter should be placed during surgery and cystouretheroscopy considered to rule out injury to the bladder. Frequent rectal exams during the surgery can be used to maintain orientation and prevent rectal injury. Efforts should be made to identify the dilated ectocervix on preoperative MRI. A dilated cervix can resemble vaginal wall, therefore caution should be used when resecting a septum located near the cervix. If it is unclear where vagina ends and cervix begins, a biopsy of the tissue can be taken for frozen section.
In William’s study of 46 patients with transverse vaginal septa, 15 patients (33 %) had a high septum that was managed with an abdominoperineal approach. Short-term complications after surgery occurred in 27 % of those patients and included vessel injury, wound infection, pyometra, and pneumonia. Five patients (33 %) had recurrent obstructions that were treated with hysterectomy in two patients and repeat vaginal surgery in three patients. One patient had vaginal stenosis that was treated with dilation. Of the 27 patients (59 %) who underwent a vaginal approach, there were no short-term complications and two cases of vaginal stenosis (7 %) that were treated with dilation. Fourteen percent of patients in this study had already undergone one surgical procedure and were having a second surgery for re-obstruction [13].
Drainage and Suppression of Menstruation
The patient’s psychological maturity and age should be considered when exploring surgical options for a transverse vaginal septum. If there are concerns that the patient cannot comply with postoperative dilation, then a delayed repair can be considered. Hormonal suppression of menses with or without drainage of the hematocolpos allows for delayed surgery and improved compliance with postoperative dilation in select patients. Decompression of hematocolpos has been described but carries a potential risk of ascending infection [16]. Hurst and Rock have reported ultrasound guided aspiration as a method to relieve acute pain associated with hematocolpos. The three patients in this report received broad spectrum prophylactic antibiotics with one postoperative infection [40]. In a review of patients at Royal Hospital for Women, three patients with lower vaginal agenesis had an attempted vaginal drainage of hematocolpos prior to referral, all of which became infected [41]. Laparoscopic drainage of hematocolpos has also been described as an approach in managing acute symptoms, which theoretically carries a lower risk of infection, because the upper vaginal cavity remains relatively sterile [42]. Hematocolpos acts as a natural tissue expander; therefore, once decompressed, the septum may become thicker and more difficult to treat.
Delayed Anastomosis
If diagnosed early and a symptomatic obstruction has not yet developed, menstrual suppression with continuous oral contraceptive pills, depot medroxyprogesterone acetate, or GnRH agonists followed by delayed anastomosis can be considered [34]. Delay allows for a period of preoperative dilation of the lower vagina in patients with a thick septum, which will increase the amount of native vaginal tissue available for re-anastomosis and may alleviate the need for grafts [40, 43].
Expectant management should be considered in the asymptomatic young girl who is diagnosed with a transverse septum before menarche. Delaying surgery until after puberty allows gradual development of hematocolpos, which can flatten the septum. Surgery is then less complicated with a thin septum and estrogenized epithelium. This approach was described in a case report and after 9 months of expectant management, a thick transverse septum decreased from 26 mm in thickness to 8 mm [44].
Infants with mucocolpos due to a transverse vaginal septum can usually be managed expectantly unless the obstruction is causing compression of nearby structures. In the rare circumstance, when the fluid collection is large enough to compress the ureters, rectum, or vena cava, the septum is life threatening and requires urgent surgical management [45]. Infants undergoing early surgery may require repeat surgery and should be followed closely through puberty [23].
Impact on Fertility and Reproduction
Patients with obstructing transverse septa can develop endometriosis from retrograde menstruation. In a study by Rock et al., seven patients with a transverse septum undergoing surgical correction had a concurrent laparotomy, diagnosing endometriosis in 86 % of those cases. The risk of endometriosis increases with imperforate septa that are located higher in the vagina [46]. Williams et al. report a 42 % incidence of endometriosis among low septa, 50 % among mid septa, and 100 % among high septa. The risk of tubal dysfunction increases if the obstruction results in hematosalpinx. Sexual activity and subsequent fertility can also be affected by psychosocial stressors associated with diagnosis and treatment, vaginal stenosis, dyspareunia, and re-obstruction.
Limited reproductive outcome data is available. Williams et al. reported data on seven patients who attempted pregnancy in their series of 46; they all achieved pregnancy with three vaginal deliveries, three cesarean deliveries, and one early termination. This limited reproductive outcome data may be the result of a young patient population and/or response bias in returning mailed questionnaires [13]. Rock et al. report increased rates of infertility and endometriosis among obstructive transverse septa compared to imperforate hymens. Among 19 patients who attempted pregnancy after surgical correction of a transverse septum, 9 conceived (47 %) and 7 had live births (36 %) [46].
There are reports of asymptomatic perforated transverse septa discovered in pregnancy. Proposed management for these cases includes resection of the septum before labor, prophylactic cesarean delivery, and expectant management allowing for spontaneous delivery with option to incise the septum as needed during the second stage of labor. Many argue that prophylactic cesarean delivery is indicated when a transverse septum is diagnosed in pregnancy to avoid vaginal laceration, scarring, and labor obstruction [47]. Others have challenged the need for prophylactic cesarean delivery by reporting two patients who had successful vaginal deliveries after incision of the septa in active labor. Though challenging during labor, because cervical dilatation cannot easily be assessed and internal monitors cannot be used, expectant management may be an option for patients with thin, perforate septa [48].
References
Lodi A. Contribuo clinic statistic sulle malformazione all vagina osservate nella. Clinca Obstetricia e Gynecoligia di Mmilano dal 1906–1950. Ann Ostet Ginecol. 1951;73:1246–51.
Wenof M, Reynaih JV, Novendstern J, Castadot MJ. Transverse vaginal Septum. Obstet Gynecol. 1979;54:60–4.
Jain N, Gupta A, Kumar R, Minj A. Complete imperforate transverse vaginal septum with septate uterus: a rare anomaly. J Hum Reprod Sci. 2013;6(1):74–6.
Dilbaz B, Altinbas SK, Altinbas NK, Sengul O, Dilbaz S. Concomitant imperforate hymen and transverse vaginal septum complicated with pyocolpos and abdominovaginal fistula. Case Rep Obstet Gynecol. 2014;2014:1–4.
Deligeoroglou E, Deliveliotou A, Makrakis E, Creatsas G. Concurrent imperforate hymen, transverse vaginal septum, and unicornuate uterus: a case report. J Pediatr Surg. 2007;42(8):1446–8.
Ahmed S, Morris LL, Atkinson E. Distal mucocolpos and proximal hematocolpos secondary to concurrent imperforate hymen and transverse vaginal septum. J Pediatr Surg. 1999;34(10):1555–6.
Wierrani F, Bodner K, Spangler B, Grunberger W. “Z”-plasty of the transverse vaginal septum using Garcia’s procedure and the Grunberger modification. Fertil Steril. 2003;79(3):608–12.
Laufer MR. Structural abnormalities of the female reproductive tract. In: Emans SJ, Laufer MR, editors. Emans, Laufer, Goldstein’s pediatric and adolescent gynecology. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2012. p. 188–236.
Grimbizis GF, Gordts S, Di Seizio SA, Brucker S, De Angelis C, Gergolet M, et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum Reprod. 2013;28(8):2032–44.
Grimbizis GF, Campo R. Congenital malformations of the female genital tract: the need for a new classification system. Fertil Steril. 2010;94(2):401–7.
Acien P, Acien MI. The history of female genital tract malformation classifications and proposal of an updated system. Hum Reprod Update. 2011;17(5):693–705.
Oppelt P, Renner SP, Brucker S, Strissel PL, Strick R, Oppelt PG, et al. The VCUAM (Vagina Cervix Uterus Adnex-associated Malformation) classification: a new classification for genital malformations. Fertil Steril. 2005;85(5):1493–7.
Williams CE, Nakhal RS, Hall-Craggs MA, Wood D, Cutner A, Pattison SH, Creighton SM. Transverse vaginal septae: management and long term outcomes. BJOG. 2014;121:1653–9.
Levy G, Warren M, Maidman J. Transverse vaginal septum: case report and review of the literature. Int Urogynecol J Pelvic Floor Dysfunct. 1997;8:173–6.
Banerjee R, Laufer MR. Reproductive disorders associated with pelvic pain. Semin Pediatr Surg. 1998;7(1):52–61.
Breech LL, Laufer MR. Mullerian anomalies. Obstet Gynecol Clin North Am. 2009;36:47–68.
Dietrich JE, Miller DM, Quint EH. Obstructive reproductive tract anomalies. J Pediatr Adolesc Gynecol. 2014;27:396–402.
Rock JA. Anomalous development of the vagina. Semin Rerpod Endocrinol. 1986;4:13–31.
Suidan FG, Azoury FS. The transverse vaginal septum: a clinicopathologic evaluation. Obstet Gynecol. 1979;54(3):278–83.
Simpson JL. Genetics of the female reproductive ducts. Am J Med Genet. 1999;89:224–39.
Slavotinek AM. Mckusick-Kaufman syndrome. Gene Review. http://www.ncbi.nlm.nih.gov/books/NBK1502/. Accessed 29 June 2010.
Ameh EA, Mshelbwala PM, Ameh N. Congenital vaginal obstruction in neonates and infants: recognition and management. J Pediatr Adolesc Gynecol. 2011;24:74–8.
Rock JA, Brrech LL. Surgery for anomalies of the mullerian ducts. In: Rock JA, Jones HW, editors. Telinde’s operative gynecology. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2009. p. 539–84.
Attaran M, Falcone T, Gidwani G. Obstructive mullerian anomalies. In: Gidwani G, Falcone T, editors. Congenital malformations of the female genital tract. Philadelphia: Lippincott Williams & Wilkins; 1999. p. 145–68.
Rock JA, Azziz R. Genital anomalies in Childhood. Clin Obstet Gynecol. 1987;30(3):682–96.
Kaya C, Cengiz H, Ekin M, Yasar L. Transverse vaginal septum: a benign reason for elevated serum CA19-9 and CA 125 levels. Arch Gynecol Obstet. 2012;286:821–3.
Bermejo C, Martinez-Ten P, Recio M, Ruiz-Lopez L, Diaz D, Illescas T. Three-dimensional ultrasound and magnetic resonance imaging assessment of cervix and vagina in women with uterine malformations. Ultrasound Obstet Gynecol. 2014;43:336–45.
Krafft C, Hartin CW, Ozgediz DE. Magnetic resonance as an aid in the diagnosis of a transverse vaginal septum. J Pediatr Surg. 2012;47:422–5.
Church DG, Vancil JM, Vasanawala S. Magnetic resonance imaging for uterine and vaginal anomalies. Curr Opin Obstet Gynecol. 2009;21:379–89.
Olpin JD, Heilbrun M. Imaging of mullerian duct anomalies. Clin Obstet Gynecol. 2009;52(1):40–56.
Humphries PD, Simpson JC, Creighton SM, Hall-Craggs MA. MRI assessment of congenital vaginal anomalies. Clin Radiol. 2008;63:442–8.
Brown MA, Mattrey RF, Stamato S, Sirlin CB. MRI of the female pelvis using vaginal gel. AJR Am J Roentgenol. 2005;185:1221–7.
Lang IM, Babyn P, Oliver GD. MR imaging of paediatric uterovaginal anomalies. Pediatr Radiol. 1999;29:163–70.
Quint EH, McCarthy JD, Smith YR. Vaginal surgery for congenital anomalies. Clin Obstet Gynecol. 2010;53(1):115–24.
Van Bijsterveldt C, Willemsen W. Treatment of patients with congenital transversal vaginal septum or partial aplasia of the vagina. The vaginal pull-through versus the push-through technique. J Pediatr Adolesc Gynecol. 2009;22:157–61.
Bush NC, Prieto JC, Baker LA. Vaginoplasty in children using autologous buccal mucosa. J Urol. 2008;179(4):94.
Yesim Ozgenel G, Ozcan M. Neo vaginal construction with buccal mucosal grafts. Plast Reconstr Surg. 2003;111:2250–4.
Raya-Rivera AM, Esquiliano D, Fierro-Pastrana R, Lopez Bayghen E, Valencia P, Ordorica-Flores R, et al. Tissue-engineered autologous vaginal organs in patients: a pilot cohort study. Lancet. 2014;384:329–36.
Lacy J, Correll GR, Walmer DK, Price TM. Simple vaginal mold for use in the postoperative care of patients with transverse vaginal septum. Fertil Steril. 2007;87(5):1225–6.
Hurst BS, Rock JA. Preoperative dilation to facilitate repair of the high transverse vaginal septum. Fertil Steril. 1992;57(6):1351–3.
Mizia K, Bennett MJ, Dudley J, Morrisey J. Mullerian dysgenesis: a review of recent outcomes at Royal Hospital for Women. Aust N Z J Obstet Gynaecol. 2006;46:29–31.
Dennie J, Pillay S, Watson D, Grover S. Laparoscopic drainage of hematocolpos: a new treatment option for the acute management of a transverse septum. Fertil Steril. 2010;94(5):1853–7.
Miller RJ, Breech LL. Surgical correction of vaginal anomalies. Clin Obstet Gynecol. 2008;52(2):223–36.
Beyth Y, Klein Z, Weinstein S, Tepper R. Thick transverse vaginal septum: expectant management followed by surgery. J Pediatr Adolesc Gynecol. 2004;17:373–81.
Burgis J. Obstructive mullerian anomalies: case report, diagnosis, and management. Am J Obstet Gynecol. 2001;185(2):338–44.
Rock JA, Zacur HA, Dlugi AM, Jones HW, TeLinde RW. Pregnancy success following surgical correction of imperforate hymen and complete transverse vaginal septum. Obstet Gynecol. 1982;59(4):448–51.
Malhotra V, Bhuria V, Nanda S, Chauhan MB, Dahiya P. Transverse vaginal septum in labor. J Gynecol Surg. 2013;29(4):207–9.
Blanton EN, Rouse DJ. Trial of labor in women with transverse vaginal septa. Obstet Gynecol. 2003;101(5):1110–2.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is distributed under the terms of the Creative Commons Attribution Noncommercial License, which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Alaniz, V.I., Quint, E.H. (2016). Transverse Vaginal Septum. In: Pfeifer, S. (eds) Congenital Müllerian Anomalies. Springer, Cham. https://doi.org/10.1007/978-3-319-27231-3_4
Download citation
DOI: https://doi.org/10.1007/978-3-319-27231-3_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-27229-0
Online ISBN: 978-3-319-27231-3
eBook Packages: MedicineMedicine (R0)