
Abstract
Localization studies have an important role in the assessment of patients with hyperparathyroidism. After a biochemical diagnosis of hyperparathyroidism is made, the utilization of real-time ultrasonography for precision treatment planning has become increasingly common amongst parathyroid surgeons. Characterization of pathologic parathyroid glands within the context of the surrounding anatomy is essential to plan a surgical approach, and to counsel the patient on treatment options. Preoperative ultrasound may direct the clinician towards or away from immediate surgical intervention. For example, in early or asymptomatic cases of hyperparathyroidism, a non-localizing sestamibi scan may be followed by ultrasound that does not reveal parathyroid pathology. The clinician may recommend additional localization and diagnostic studies, and postpone surgery. In another scenario, concomitant thyroid pathology may be identified on preoperative ultrasound and receive the appropriate evaluation before surgery is planned. The principles of ultrasound apply to the intraoperative setting as well—ultrasound immediately prior to skin incision can enhance surgical strategy. In this chapter we discuss the application of ultrasound technology in the preoperative and intraoperative management of parathyroid disease.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Keywords
- Ultrasound
- Ultrasound Doppler
- Parathyroid surgery
- Hyperparathyroidism
- Head and neck imaging
- Parathyroid adenoma
- Parathyroid hyperplasia
Introduction
An introduction to the fundamentals of ultrasound is provided elsewhere in this book (Chap. 13). Here we review some of the basic principles of ultrasound that make this imaging modality a very useful instrument in the management of parathyroid disease. A more in-depth description of ultrasound fundamentals can be found within several dedicated textbooks of ultrasonography [1, 2]. Sound waves require a medium through which to propagate. Various mediums demonstrate differing impedance properties and speed at which they propagate sound based upon their density and composition. The difference in impedance of adjacent mediums results in the reflection of sound waves, a principle that allows for high-resolution imaging of anatomical structures in the neck with various natural densities. The computing power of an ultrasound machine infers the distance away from the ultrasound transducer that an object is located based upon the time elapsed from emission of a sound wave from the transducer until the reflected wave returns to the transducer. Along with the propagation and reflection of ultrasound waves, a third important property of sound travel is the degree of attenuation of the wave, which increases the farther from the transducer the wave propagates. The higher the frequency utilized in ultrasound, the earlier the attenuation and shorter distance of propagation through tissues; yet the resolution of imaging will be greater. The optimal frequency of ultrasound in parathyroid imaging, considering the need for high resolution and adequate depth of imaging, ranges from 7.5 to 13 MHz.
Ultrasound technology also takes advantage of the Doppler effect in evaluating vascular flow. The Doppler principle states that an object moving towards (or away) from the direction of a sound wave source will reflect the sound wave at a greater (or lower) frequency than the original emitted wave. This property is exploited by the ultrasound machine computations to determine both directionality and velocity of blood flow. A Doppler map is created by modern ultrasound systems that is superimposed on the B-mode (gray scale) ultrasound image to depict variations in blood flow within anatomic structures of interest, including pathologic parathyroid glands.
Indications for Parathyroid Ultrasound
Preoperative parathyroid ultrasound is one of the most frequently utilized imaging modalities in the evaluation of hyperparathyroidism, often providing stand-alone localization of abnormal parathyroid glands or complementary information to radionuclide scanning. The same preoperative utility of ultrasound can be applied to patients in the intraoperative setting when sonographic equipment is available. Whether the patient is under local or general anesthesia in preparation for surgery, he or she is in the appropriate operating head and neck position. The surgeon or other sonographer can then perform a thorough neck ultrasound examination to reconfirm the predicted location of the parathyroid lesion and plan an appropriate incision and approach. After excision of the parathyroid candidate, the surgeon can also ultrasound the specimen ex vivo to confirm that it resembles the candidate targeted preoperatively.
The indications for utilizing ultrasound in parathyroid disease are important to understand. All patients suspected of having primary hyperparathyroidism based upon history, exam, and laboratory workup, who are considered surgical candidates, are also candidates for both radionuclide scanning and neck ultrasound. Since approximately 85 % of patients with primary hyperparathyroidism will have a solitary parathyroid adenoma, localizing a target can be critical to surgical planning [3] (Fig. 23.1). In addition to evaluating the neck for one or more enlarged parathyroid glands, any potential thyroid pathology should also be evaluated by ultrasound prior to counseling the patient on the extent of surgery. Preoperative ultrasonographic evaluation of the thyroid gland directs further diagnostic testing that may then dictate a procedure that can be performed at the same time as parathyroid surgery [4]. Surgery of the central neck compartment is ideally performed at one session, as each subsequent surgery becomes more technically difficult and can raise the risk of operative morbidity [5, 6].

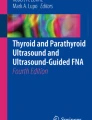
Left inferior parathyroid adenoma abutting left common carotid artery and dorsal to left thyroid lobe. Transverse view. CCA common carotid artery, IJV internal jugular vein, SH/ST sternohyoid and sternothyroid muscles, PTA parathyroid adenoma, SCM sternocleidomastoid
In patients suspected of having secondary or tertiary hyperparathyroidism, multigland hyperplasia is more commonly encountered than a solitary adenoma. Four-gland hyperplasia can usually be appreciated on ultrasound. In parathyroid hyperplasia , the four glands may not be uniformly enlarged, as one or more glands may demonstrate greater hyperplastic changes than the others [7–9] (Fig. 23.2). Ultrasound assessment may aid in planning the order of exploration, from the most prominently enlarged gland downwards, while following intraoperative PTH levels. Again thorough assessment of the thyroid gland will be important for planning the appropriate operation [10].

Parathyroid hyperplasia showing a larger superior parathyroid and smaller inferior parathyroid gland. Both glands are hyperplastic but are asymmetrically enlarged. Sagittal view. SPT superior parathyroid, IPT inferior parathyroid, SH/ST sternohyoid and sternothyroid muscles
Neither radionuclide scanning nor parathyroid ultrasound exhibit absolute sensitivity nor specificity for parathyroid adenomas. A strongly localizing result from one image test may be sufficient to direct surgery, but it does not preclude an indication for radionuclide scanning or other imaging modalities [11, 12]. Identification of a cervical parathyroid adenoma candidate on ultrasound does not rule out the possibility of a second, ectopic adenoma in a location inaccessible to ultrasound (e.g., mediastinum, retropharynx). Whereas an ultrasound may reveal a hypoechoic lesion in an anatomically appropriate location for a parathyroid gland, a small lymph node may be difficult to distinguish from parathyroid tissue sonographically (Fig. 23.3). Sestamibi radionuclide scanning may help scrutinize a parathyroid candidate further with a functional evaluation. Conversely, a “positive” sestamibi radionuclide scan that suggests a sidedness to a parathyroid candidate is ideally supported by an ultrasound that demonstrates an enlarged hypoechoic lesion with the same laterality, as radionuclide scan interpretation is subject to distraction by background noise inherent to the properties of this imaging technique.

Left level 6 lymph node . Transverse (left) and sagittal (right) views. LN lymph node
Preoperative or intraoperative ultrasound of the neck allows the surgeon to identify aberrant anatomy prior to the operation. For example a non-recurrent right laryngeal nerve is readily suspected if the right subclavian and carotid arteries do not proximally arise from an innominate artery, which should be identifiable on ultrasound in most patients [13]. While it is not necessary in all parathyroid cases to identify the recurrent (or non-recurrent) laryngeal nerve, its anatomical course should be understood and anticipated as well as possible in any central neck compartment surgery (Fig. 23.4 and Video 23.1).

Right common carotid and subclavian artery confluence. CCA common carotid artery, SCA subclavian artery, INA innominate artery
Ultrasonographic Appearance of Parathyroid Tissue
Normal parathyroid glands are typically less than 40 mg in mass, and measure approximately 6 mm in cranio-caudad length, and 3–4 mm in width [3, 14]. They are typically too small and too similar to surrounding structures to be appreciated by ultrasound imaging. In the majority of cases, ultrasound imaging of pathologically enlarged parathyroid glands demonstrates a homogeneous ovoid, hypoechoic lesion that may have a distinct, more echogenic rim [15–17]. Less commonly, enlarged parathyroid glands may be multilobulated in shape; they may also appear anechoic, or even show echogenicity similar to thyroid tissue. The appearance may be difficult to distinguish from a lymph node, which also may be ovoid with a hypoechoic appearance. In enlarged lymph nodes, a fatty central hilum may be visible as a more echogenic region, and Doppler signaling for vascular flow should demonstrate central flow through the hilar vascular pedicle. In contrast, a parathyroid adenoma has a primarily polar vascular pedicle—rather than central within the ovoid mass; the pedicle typically terminates at the superior pole (Fig. 23.5 and Videos 23.2, 23.3, and 23.4). This may be best appreciated in sagittal orientation on ultrasound. A vascular “arc” has also been described coursing over the surface of parathyroid tissue [18]. Hypervascularity of the parathyroid capsule, or hypervascularity of the adjacent thyroid gland, has also been reported on ultrasound Doppler flow studies [19]. The contrasting vascular characteristics of lymph nodes and parathyroid adenomas are difficult to discern in small lymph nodes, in which ultrasonographic resolution is insufficient to visualize the central hilum clearly.

Left inferior parathyroid adenoma showing superior polar vascularity (arrow). Sagittal view. PTA parathyroid adenoma
A parathyroid candidate on ultrasound may also be difficult to distinguish from a thyroid nodule if an intracapsular parathyroid gland is suspected (Fig. 23.6). While echogenicity of the lesion may be somewhat helpful, many thyroid nodules are hypoechoic, round, or ovoid in appearance. Ordinarily a subcentimeter thyroid nodule without suspicious characteristics (e.g., microcalcification, irregular borders) may not warrant a fine-needle aspiration (FNA) biopsy . However if such a nodule is a candidate for parathyroid tissue, an ultrasound-guided FNA biopsy with saline washings for parathyroid hormone (PTH) levels is a useful next diagnostic step, provided that accurate aspiration of the lesion is achieved [20, 21].

Right intracapsular parathyroid adenoma. Transverse (left) and sagittal (right) views. PTA parathyroid adenoma, CCA common carotid artery, IJV internal jugular vein
Patients diagnosed with primary hyperparathyroidism will be found to have a solitary adenoma in 85 % of cases; multigland disease, either diffuse hyperplasia or less commonly double adenomas in 15 % of cases; and in less than 1 % of cases, parathyroid carcinoma [3]. The key distinguishing factor between the rare parathyroid carcinoma and an adenoma on ultrasound is the invasion, by carcinoma, into adjacent structures that may be visualized on ultrasound, with an irregular lesion border. Physical exam findings of a palpable mass, and laboratory findings of a serum calcium greater than 14 mg/dL, a PTH greater than three times normal, and a markedly elevated serum alkaline phosphatase should also increase suspicion for parathyroid malignancy, although these each has low specificity [22, 23]. In multiple endocrine neoplasia types I and IIa, as well as secondary and tertiary hyperparathyroidism, multigland hyperplasia is typically appreciated on ultrasound, whereas sporadic cases of multiglandular disease may not present with enlarged parathyroid glands to a size visible on ultrasound.
Embryology and Location of the Parathyroid Glands
A brief review of the embryologic development of the parathyroid glands is useful to aid in understanding their most common anatomical locations and methodically survey potential ectopic sites for ultrasonographic identification. The superior and inferior parathyroid glands develop from the dorsal wings of the embryonic fourth and third pharyngeal pouches, respectively. Differentiation into parathyroid parenchyma occurs during the fifth to sixth week of gestation, followed by detachment from the pharynx at week 7 after which both pairs of glands begin a caudal migration. The superior parathyroid glands attach to the thyroid and migrate caudally for a much shorter distance than the inferior parathyroid glands. The superior parathyroid glands typically deposit along the posterior aspect of the mid to superior thyroid lobe. Whereas the inferior parathyroid glands develop from the dorsal wing of the third pharyngeal pouch, the thymus develops from the ventral wing of this same pouch. As the thymus migrates caudally into the superior mediastinum, the attached inferior parathyroid glands follow; however they usually detach from the thymus and deposit proximally, just inferior and posterior to the inferior thyroid pole.
The superior parathyroid gland is located posterior, or dorsal, to the recurrent laryngeal nerve (RLN) , whereas the inferior parathyroid rests anterior, or ventral, to the nerve. Since the RLN is not visualized on parathyroid ultrasound, the posterior, or deep, border of the carotid artery or the inferior thyroid artery serves as sonographic surrogate landmark for the plane of the RLN (Figs. 23.7 and 23.8). For example a parathyroid candidate lying anterior, or superficial, to this plane would likely be an inferior parathyroid.

A descended left superior parathyroid adenoma, abutting esophagus deep to posterior plane of the common carotid artery. Intraoperatively, the recurrent laryngeal nerve was identified ventral to the adenoma, as expected in relation to a superior parathyroid gland. Transverse view. PTA parathyroid adenoma, CCA common carotid artery, EGS esophagus

Left superior parathyroid adenoma. Transverse (left) and sagittal (right) views. PTA parathyroid adenoma, CCA common carotid artery, SCM sternocleidomastoid, SH/ST sternohyoid and sternothyroid muscles
During a parathyroid ultrasound survey , it is helpful to anticipate typical and ectopic locations of parathyroid glands based on their embryological development. The superior parathyroid glands may be identified as high as the hyoid bone or level of the carotid bifurcation. In addition to the central compartment proper, ultrasound should examine the carotid sheath, retropharyngeal, retroesophageal, retrotracheal, and parapharyngeal spaces to the extent possible for potential ectopic glands [24]. The superior parathyroid gland may also descend into the posterior mediastinum, a space bounded superiorly by the upper border of pericardium, and inferiorly by the diaphragm, beyond visibility by transcutaneous ultrasound . The inferior parathyroid gland may continue to descend into the superior, or even anterior (anteroinferior) mediastinum as it follows the descent of the thymus. The inferior parathyroid gland may be found as far cephalic as the hyoid bone as well if it failed to descend with the thymus. A parathyroid candidate at this cephalic limit would be considered inferior or superior based on its relationship to the RLN.
Techniques in Parathyroid Ultrasound
Ultrasound evaluation of parathyroid disease should first begin with a thorough survey of the central neck compartment , from hyoid bone cephalically to the thoracic inlet as far caudally as can be accessed by the ultrasound transducer [18]. A suggested approach begins by identification of the innominate artery as it courses from the superior mediastinum towards the right central neck compartment, branching into the right common carotid and subclavian artery. The space from right carotid sheath to larynx and trachea is carefully examined in a caudal to cephalad direction with the transducer in a transverse orientation. Examination continues to the superior limit of the thyroid lobe, and can extend to the hyoid. Any parathyroid candidates are then investigated with the transducer in a sagittal plane, which aids in visualizing the vascular pedicle that frequently can be seen at the superior pole of the enlarged gland. Examining the right central neck compartment beginning at the right innominate artery also provides rapid confirmation of the normal great vessel anatomy, and therefore RLN anatomy. The awake patient can be asked to turn his or her head towards and away from the examiner to further enhance visualization of otherwise overlapping structures; in the sedated patient, the examiner may need to carefully rotate the patient’s head to accomplish the same result. An awake patient can also be asked to swallow, which can aid in distinguishing the esophagus from other nodular structures. The anesthetized patient may have an endotracheal tube and/or an esophageal probe in place that can distort anatomy or create ultrasound artifacts, such as acoustic shadowing, and should be noted.
The left central neck compartment is subsequently evaluated from the thoracic inlet to superior limit of the thyroid lobe, again from carotid sheath laterally to the trachea and larynx medially. Both transverse and sagittal transducer orientations are employed. Next the thyroid gland itself is evaluated, beginning with the right thyroid lobe from caudal to cephalad, transversely, and then in sagittal view. This step is repeated on the left, followed by examining the isthmus. As discussed earlier, it is worthwhile to perform thyroid ultrasound in all hyperparathyroidism patients, both in search of ectopic intrathyroidal parathyroid glands and to assess possible thyroid pathology that may warrant further diagnostic and therapeutic measures. Ultrasound-guided FNA biopsy of suspicious intrathyroidal lesions with saline needle washing for PTH assay can then be employed [21]. Often the middle thyroid vein is seen draining from the mid to lower thyroid lobe, and is a useful surgical landmark that may help orient the surgeon if a parathyroid candidate is visualized nearby (Fig. 23.9).

Left inferior parathyroid adenoma. The left middle thyroid vein (arrow) is seen exiting the left mid-thyroid lobe, draining into the internal jugular vein. Transverse view. PTA parathyroid adenoma, CCA common carotid artery, SCM sternocleidomastoid, SH/ST sternohyoid and sternothyroid muscles, IJV internal jugular vein
Ultrasonographic visualization beyond the thoracic inlet into the superior mediastinum is often limited by patient habitus, and sometimes can be facilitated by sagittal positioning of the transducer, leading with one corner of the transducer. Deep planes, including potential ectopic sites such as prevertebral, and retropharyngeal, retroesophageal, and retrotracheal spaces, may require adjustments of the ultrasound settings to a lower frequency, which allows for better penetration of sound energy due to longer wavelength. The ultrasound field gain (either overall gain or time-gain compensation in the far field) is increased for deeper examination as well. In addition to an anteroposterior direction of transducer placement, a lateral approach is employed to examine these “retro-aerodigestive” spaces with less impedance from the carotid artery and laryngotracheal framework. After parathyroid candidates have been identified, Doppler flow can be utilized to assess for typical vascular patterns, such as a polar vascular pedicle, a vascular arch, or increased adjacent thyroidal vascularity.
The surgeon or sonographer should avoid quick conclusions about the location of the pathologic parathyroid gland based upon prior knowledge of radionuclide findings, as this bias can lead to a less thorough examination of the entire space at risk for harboring parathyroid disease. Even in cases of multigland hyperplasia, one parathyroid gland may be larger than the other three, and lead to the assumption that the patient has a solitary adenoma (Fig. 23.10). Rather the surgeon or radiologist can use the full potential of ultrasound to map out the entire at-risk neck spaces.

Parathyroid hyperplasia , superior greater than inferior. Sagittal view. SPT superior parathyroid, IPT inferior parathyroid
Current Investigations into Parathyroid Ultrasound
As discussed earlier, preoperative radionuclide scanning and neck ultrasound provide complementary information that is pivotal for surgical planning in primary hyperparathyroidism. For both preoperative and intraoperative ultrasound, the experience and motivation of the sonographer are vital attributes in determining the quality and validity of an exam [25–28]. For the patient with primary hyperparathyroidism who is suspected of having a solitary adenoma on ultrasound, the sonographer can help direct the tailoring of a small, targeted incision by specifying the most likely central neck quadrant and triangulating location with respect to regional anatomy for a minimally invasive surgical approach [29] (Figs. 23.11 and 23.12 and Video 23.5). The surgeon must plan an incision that can be extended if necessary, such that both surgical exposure and final cosmesis are optimized. While other imaging modalities can also potentially localize an adenoma to the correct quadrant (e.g., MRI, CT, 4D CT, sestamibi), none has the low cost, speed, and/or non-radiation-based advantages of ultrasound.

Right inferior parathyroid adenoma, transverse (left) and sagittal (right) views. PTA parathyroid adenoma, CCA common carotid artery, SH/ST sternohyoid and sternothyroid muscles, IJV internal jugular vein

Large right inferior parathyroid adenoma . Transverse view (12A); sagittal view (12B); Doppler shows hypervascular pattern of the adenoma, adjacent to the high flow of the common carotid artery (12C—arrow marks PTA, star marks CCA). PTA parathyroid adenoma, CCA common carotid artery, SH/ST sternohyoid and sternothyroid muscles, IJV internal jugular vein, SCM sternocleidomastoid. *On sagittal view, left side of image is cephalad, right side is caudal
Some surgeons have endorsed the use of adjunctive intraoperative localizing procedures such as ultrasound-guided, intralesional methylene blue dye injection, particularly in reoperative necks in which the normal tissue planes can be significantly altered [30, 31]. This technique of tattooing the suspected parathyroid adenoma is logical; however it must be implemented with precision. As a dry, bloodless field is essential in parathyroid surgery, any staining of methylene blue into tissues surrounding the candidate adenoma can blur tissue interfaces. As an endocrine gland that is primarily secreting hormone into systemic circulation, successful injection of the parathyroid may be followed by egress of blue dye through the gland’s venous outflow into surrounding tissues, again obscuring planes of dissection.
The application of ultrasound in parathyroid hyperplasia has also been investigated as a potential quantitative instrument for preoperatively calculating the extent of gland excision necessary in the preoperative setting. While this concept requires further investigation in larger patient cohorts, a recent study of ten patients with multiple endocrine neoplasia type I showed a positive correlation between total calculated parathyroid volume on preoperative ultrasound and preoperative serum intact parathyroid hormone (iPTH) level (R = 0.96, P < 0.001) [32]. The investigators derived a formula directly relating sonographic parathyroid volume and iPTH (volume in mm3 = 15 × iPTH (pg/mL) − 1000). They postulated a scenario in which such a correlation could be useful. If a patient with parathyroid hyperplasia is also found to have a thyroid lesion (i.e., nodule versus intrathyroidal parathyroid), a simple calculation of parathyroid volume by preoperative ultrasound, compared to the volume predicted by the above formula, might suggest the probability that the intrathyroidal lesion represented functional parathyroid tissue. Future studies with larger patient cohorts may better validate this proposed correlation. Ultimately an intraoperative determination by the surgeon for adequacy of four-gland exploration is necessary, but innovative approaches to preoperative planning are helpful for the surgeon to anticipate the course of surgery, and provide patient counseling. Likewise in cases of parathyroid hyperplasia associated with secondary and tertiary hyperparathyroidism, while preoperative ultrasound does not replace a thorough four-gland exploration, evaluation of the thyroid gland for concomitant pathology (or ectopic parathyroid tissue) is key to operative planning prior to making an incision [10].
There remains a need for high-resolution imaging modalities to visualize the retropharynx, retroesophagus, and mediastinum—potential sites for ectopic parathyroid tissue that are not easily visualized with percutaneous transcervical ultrasound. MRI or CT imaging may complement sestamibi in identifying such ectopic parathyroids. Preoperative endoscopic ultrasound has also been described to interrogate these anatomical locations, and can also be combined with a fine-needle aspirate measuring PTH levels [33, 34]. To our knowledge only case reports have described the usage of endobronchial ultrasound (EBUS) to identify and plan excision of mediastinal and retroesophageal parathyroid adenomas. However EBUS-assisted FNA has been widely utilized to diagnose mediastinal masses prior to surgical intervention [35]. In patients with persistent hyperparathyroidism after a thorough prior neck exploration (e.g., with parathyroid adenoma excision), detection of a suspected ectopic hyperfunctional parathyroid may be facilitated by endoscopic ultrasound.
Summary
Localization studies have been described as preoperative tools for the surgeon to use only after a biochemical diagnosis of hyperparathyroidism has been made and surgery recommended. Increasingly, however, parathyroid surgeons are knowledgeable of and adept at utilizing the advantages of real-time ultrasonography for precise assessment of pathologic parathyroid glands in the context of the associated surgical anatomy. In equivocal, asymptomatic, or early cases of hyperparathyroidism, a preoperative ultrasound that fails to reveal a candidate for a pathologic parathyroid gland, especially in the setting of a nonlocalizing sestamibi parathyroid scan, might appropriately lead the clinician to postpone surgery or consider ancillary studies for localization. On the other hand, a finding of thyroid pathology in addition to localization of parathyroid candidate(s) with ultrasound may lead to expansion of the surgical plan. Once the decision has been made to operate, the use of ultrasound in the operating room immediately prior to incision can significantly enhance surgical strategy. After an incision has been made, ultrasound can still be performed through adjacent skin using a sterile or sterilely draped transducer, and intracavitary ultrasound, although difficult within the minimal access incision, can be used to confirm a target. Back table ultrasound of excised specimens can further help to confirm retrieval of intended targets.
Society Guidelines:
N/A
Best Practices:
N/A
Expert Opinion
Ultrasound can be relied upon at multiple phases in the care of the patient with hyperparathyroidism, enabling characterization of and vision through, not just around, anatomical structures.
References
Orloff LA, editor. Head and neck ultrasonography. San Diego: Plural Publishing, Inc.; 2008. Clinical Review; Level 2; Grade A–B.
Sofferman RA. Ultrasound of the thyroid and parathyroid glands. In: Sofferman RA, Ahuja AT, editor. Springer Science + Business Media; 2012, Clinical Review; Level 2; Grade A–B.
Flint PW, editor. Cummings otolaryngology-head and neck surgery. 2015, Clinical Review; Level 2; Grade A–B.
Milas M, Mensah A, Alghoul M, Berber E, Stephen A, Siperstein A, et al. The impact of office neck ultrasonography on reducing unnecessary thyroid surgery in patients undergoing parathyroidectomy. Thyroid. 2005;15(9):1055–9. Clinical Review; Level 2; Grade A–B.
Pelizzo MR, Variolo M, Bernardi C, Izuzquiza M, Piotto A, Grassetto G, et al. Complications in thyroid resurgery: a single institutional experience on 233 patients from a whole series of 4,752 homogeneously treated patients. Endocrine. 2014;47(1):100–6. Population/Observational Study; Level 3; Grade A–B.
Kim MK, Mandel SH, Baloch Z, Livolsi VA, Langer JE, Didonato L, et al. Morbidity following central compartment reoperation for recurrent or persistent thyroid cancer. Arch Otolaryngol. 2004;130(10):1214–6. Population/Observational Study; Level 3; Grade A–B.
Berger AC, Libutti SK, Bartlett DL, Skarulis MG, Marx SJ, Spiegel AM, et al. Heterogeneous gland size in sporadic multiple gland parathyroid hyperplasia. J Am Coll Surg. 1999;188(4):382–9. Clinical Investigation; Level 2; Grade C.
Doherty GM. Multiple endocrine neoplasia type 1. J Surg Oncol. 2005;89(3):143–50. Clinical Review; Level 2; Grade A–B.
Nilubol N, Weinstein L, Simonds WF, Jensen RT, Phan GQ, Hughes MS, et al. Preoperative localizing studies for initial parathyroidectomy in MEN1 syndrome: is there any benefit? World J Surg. 2012;36(6):1368–74. Clinical Review; Level 2; Grade A–B.
Alkhalili E, Tasci Y, Aksoy E, Aliyev S, Soundararajan S, Taskin E, et al. The utility of neck ultrasound and sestamibi scans in patients with secondary and tertiary hyperparathyroidism. World J Surg. 2015;39(3):701–5. Clinical Investigation; Level 2; Grade C.
Steward DL, Danielson GP, Afman CE, Welge JA. Parathyroid adenoma localization: surgeon-performed ultrasound versus sestamibi. Laryngoscope. 2006;116(8):1380–4. Clinical Investigation; Level 2; Grade C.
Yeh MW, Barraclough BM, Sidhu SB, Sywak MS, Barraclough BH, Delbridge LW. Two hundred consecutive parathyroid ultrasound studies by a single clinician: the impact of experience. Endocr Pract. 2006;12(3):257–63. Clinical Review; Level 2; Grade A–B.
Iacobone M, Citton M, Pagura G, Viel G, Nitti D. Increased and safer detection of nonrecurrent inferior laryngeal nerve after preoperative ultrasonography. Laryngoscope. 2015, Clinical Investigation; Level 2; Grade C.
Policeni BA, Smoker WR, Reede DL. Anatomy and embryology of the thyroid and parathyroid glands. Semin Ultrasound CT MR. 2012;33(2):104–14. Clinical Review; Level 2; Grade A–B.
Cheung K, Wang TS, Farrokhyar F, Roman SA, Sosa JA. A meta-analysis of preoperative localization techniques for patients with primary hyperparathyroidism. Ann Surg Oncol. 2012;19(2):577–83. Clinical Review; Level 2; Grade A–B.
Johnson NA, Tublin ME, Ogilvie JB. Parathyroid imaging: technique and role in the preoperative evaluation of primary hyperparathyroidism. AJR Am J Roentgenol. 2007;188(6):1706–15. Clinical Review; Level 2; Grade A–B.
Smith RB, Evasovich M, Girod DA, Jorgensen JB, Lydiatt WM, Pagedar NA, et al. Ultrasound for localization in primary hyperparathyroidism. Otolaryngology. 2013;149(3):366–71. Clinical Investigation; Level 2; Grade C.
Sung JY. Parathyroid ultrasonography: the evolving role of the radiologist. Ultrasonography. 2015, Clinical Review; Level 2; Grade A–B.
Lane MJ, Desser TS, Weigel RJ, Jeffrey Jr RB. Use of color and power Doppler sonography to identify feeding arteries associated with parathyroid adenomas. AJR Am J Roentgenol. 1998;171(3):819–23. Clinical Investigation; Level 2; Grade B–C.
Kwak JY, Kim EK, Moon HJ, Kim MJ, Ahn SS, Son EJ, et al. Parathyroid incidentalomas detected on routine ultrasound-directed fine-needle aspiration biopsy in patients referred for thyroid nodules and the role of parathyroid hormone analysis in the samples. Thyroid. 2009;19(7):743–8. Clinical Review; Level 2; Grade A–B.
Owens CL, Rekhtman N, Sokoll L, Ali SZ. Parathyroid hormone assay in fine-needle aspirate is useful in differentiating inadvertently sampled parathyroid tissue from thyroid lesions. Diagn Cytopathol. 2008;36(4):227–31. Clinical Investigation; Level 2; Grade A–B.
Clayman GL, Gonzalez HE, El-Naggar A, Vassilopoulou-Sellin R. Parathyroid carcinoma: evaluation and interdisciplinary management. Cancer. 2004;100(5):900–5. Clinical Review; Level 2; Grade A–B.
Fyfe ST, Hoover LA, Zuckerbraun L, Goodman MD. Parathyroid carcinoma: clinical presentation and treatment. Am J Otolaryngol. 1990;11(4):268–73. Clinical Review; Level 2; Grade A–B.
American Institute of Ultrasound in Medicine, American College of Radiology, Society for Pediatric Research, Society of Radiologists in Ultrasound. AIUM practice guideline for the performance of a thyroid and parathyroid ultrasound examination. J Ultrasound Med. 2013;32(7):1319–29. Clinical Review; Level 2; Grade A–B.
Gurney TA, Orloff LA. Otolaryngologist-head and neck surgeon-performed ultrasonography for parathyroid adenoma localization. Laryngoscope. 2008;118(2):243–6. Clinical Investigation; Level 2; Grade C.
Hessman O, Stalberg P, Sundin A, Garske U, Rudberg C, Eriksson LG, et al. High success rate of parathyroid reoperation may be achieved with improved localization diagnosis. World J Surg. 2008;32(5):774–81. discussion 82-3, Clinical Investigation; Level 2; Grade A–B.
Solorzano CC, Carneiro-Pla DM, Irvin 3rd GL. Surgeon-performed ultrasonography as the initial and only localizing study in sporadic primary hyperparathyroidism. J Am Coll Surg. 2006;202(1):18–24. Clinical Investigation; Level 2; Grade A–B.
Van Husen R, Kim LT. Accuracy of surgeon-performed ultrasound in parathyroid localization. World J Surg. 2004;28(11):1122–6. Clinical Investigation; Level 2; Grade A–B.
Miller B. SPUS Facilitates MIP. World J Surg. 2008;32(5):772–3. Clinical Review; Level 2; Grade A–B.
Candell L, Campbell MJ, Shen WT, Gosnell JE, Clark OH, Duh QY. Ultrasound-guided methylene blue dye injection for parathyroid localization in the reoperative neck. World J Surg. 2014;38(1):88–91. Clinical Investigation; Level 2; Grade B–C.
Ryan WR, Orloff LA. Intraoperative tumor localizaiton with surgeon-performed ultrasound-guided needle dye injection. Laryngoscope. 2011;121(8):1651–5. Clinical Investigation; Level 2; Grade B–C.
Tamiya H, Miyakawa M, Takeshita A, Miura D, Takeuchi Y. Ultrasonographic evaluation of parathyroid hyperplasia in multiple endocrine neoplasia type 1: positive correlation between parathyroid volume and circulating parathyroid hormone concentration. J Bone Miner Metabolism. 2014, Population/Observational Study; Level 3; Grade A–B.
Buderi SI, Saleh HZ, Theologou T, Shackcloth M. Endobronchial ultrasound-guided biopsy to diagnose large posterior mediastinal parathyroid adenoma prior to video-assisted thoracoscopic resection. BMJ Case Rep. 2014;2014, Clinical Investigation; Level 2; Grade B–C.
Vu DH, Erickson RA. Endoscopic ultrasound-guided fine-needle aspiration with aspirate assay to diagnose suspected mediastinal parathyroid adenomas. Endocr Pract. 2010;16(3):437–40. Clinical Review; Level 3; Grade A–B.
Yasufuku K, Nakajima T, Fujiwara T, Yoshino I, Keshavjee S. Utility of endobronchial ultrasound-guided transbronchial needle aspiration in the diagnosis of mediastinal masses of unknown etiology. Ann Thorac Surg. 2011;91(3):831–6. Clinical Review; Level 3; Grade A–B.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Simple sweep in transverse plane following right common carotid artery inferiorly to where it meets right subclavian artery at bifurcation from innominate artery (WMV 4914 kb)
Sagittal-view power Doppler demonstrating increased and polar vascularity of parathyroid adenoma (middle arrow) in relation to thyroid (superior to adenoma, left arrow) and lymph node (inferior to adenoma, right arrow), in a patient with coexisting Hashimoto’s thyroiditis and central compartment lymphadenopathy (WMV 2575 kb)
Transverse view in same patient as Video 23.2, showing increased and polar vascularity of parathyroid adenoma compared to hypovascularity of lymph node (parathyroid = upper arrow, lymph node = lower arrow) (WMV 4240 kb)
Sagittal-view power Doppler demonstrating polar vascularity of small right inferior parathyroid adenoma (WMV 1146 kb)
Ultrasound sweep from inferior to superior and back in transverse plane to visualize a parathyroid adenoma in the context of regional anatomy (large left inferior parathyroid adenoma deep/posterior to a relatively small left thyroid lobe) (WMV 8625 kb)
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Li, R.J., Orloff, L.A. (2017). Intraoperative Parathyroid Ultrasound. In: Stack, Jr., B., Bodenner, D. (eds) Medical and Surgical Treatment of Parathyroid Diseases. Springer, Cham. https://doi.org/10.1007/978-3-319-26794-4_23
Download citation
DOI: https://doi.org/10.1007/978-3-319-26794-4_23
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-26792-0
Online ISBN: 978-3-319-26794-4
eBook Packages: MedicineMedicine (R0)