
Abstract
The repair of abdominal aortic aneurysms (AAA) in order to prevent aneurysm rupture and patient death represents one of the central tenets of vascular and endovascular surgery. The ability to predict AAA rupture is therefore of paramount importance. While maximum aortic diameter is an empirically proven metric in the prediction of AAA rupture, it is far from ideal.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Introduction
The repair of abdominal aortic aneurysms (AAA) in order to prevent aneurysm rupture and patient death represents one of the central tenets of vascular and endovascular surgery. The ability to predict AAA rupture is therefore of paramount importance. While maximum aortic diameter is an empirically proven metric in the prediction of AAA rupture, it is far from ideal.
Biomechanical analysis has been demonstrated to improve the understanding and prediction of AAA rupture. In particular, wall stress has been shown to predict more accurately the rupture and growth of AAA than maximum diameter. Finite element analysis represents the most commonly employed biomechanical technique to analyze AAA rupture risk, although other methods, including computational fluid dynamics and fluid–structure interaction analysis, have emerged as an important and nuanced means of predicting AAA behavior.
The review of the literature herein highlights the limitations of maximum aneurysm diameter as a predictor of AAA rupture; the use of biomechanical analyses, such as wall stress, to predict AAA rupture; and the evidence in support of wall stress in elucidating the natural history of AAA. While maximum aneurysm diameter remains one of the most important tools available to vascular surgeons in the evaluation and management of AAA, aneurysm diameter is not rigorously predictive of aneurysm rupture, and wall stress represents an important complement and adjuvant in understanding and predicting the behavior of abdominal aortic aneurysms.
Maximum Diameter Is a Less than Ideal Predictor of AAA Rupture
Several studies have demonstrated that a not insignificant number of AAAs rupture at a size less than the maximum diameter of 5.5 cm at which repair is typically recommended. One large, single-center study reported that 16 of 161 (9.9 %) ruptured AAAs that presented over a 10-year period were 5 cm or smaller in maximum diameter [1]. This finding led the authors to suggest that in appropriately selected patients, a lower size threshold might be used to recommend repair. The UK Small Aneurysm Trial followed a cohort of over 2000 patients prospectively over time. In that trial, 24 patients with AAAs between 4 and 5 cm ruptured. Patients with AAAs between 4 and 5.5 cm had a crude rupture rate of 2.7 per 100 person-years [2]. It is important to note that in both of the above studies, ultrasound was the primary imaging modality for determining maximum aortic diameter, and ultrasound has been shown to underestimate AAA size compared to computed tomography-based measurements by between 1 and 5 mm depending on the method utilized [3]. Nonetheless, it appears that a number of AAAs rupture prior to reaching the maximum diameter threshold at which repair is recommended. One might ask whether some larger aneurysms are stable over long-term follow-up, which might further impugn the predictive value of aneurysm diameter, but the same UK Small Aneurysm Trial found that very few patients with aneurysms greater than 6 cm survived more than 3 years without rupture. That small aneurysms sometimes rupture highlights the fact that current criteria for aneurysm repair that rely exclusively on maximum diameter are far from ideal in predicting AAA behavior.
Computational Biomechanics in the Prediction of AAA Rupture
Biomechanical analysis utilizing wall stress represents an additional manner of predicting AAA rupture. The Law of Laplace states that wall tension is proportional to pressure times radius for thin-walled spheres or cylinders. Wall stress is wall tension divided by wall thickness. This axiom forms much of the basis for the use of maximum diameter to predict AAA rupture, which, as described above, is the default – but less than ideal – method of predicting AAA rupture. The axiom that an AAA ruptures when the stress on the aortic wall exceeds its strength may offer a more sophisticated and reliable means of predicting the natural history of AAAs. Biomechanical analyses that yield calculations of wall stress and wall strength, as a result, may improve the ability to prognosticate the behavior of aortic aneurysms.
Role of Wall Strength
There are several means of assessing the wall strength of aneurysms of the abdominal aorta. One method is noninvasive and predicated on imaging modalities, such as ultrasound, computed tomography, and magnetic resonance, with cardiac cycle tracking to evaluate the compliance of the aortic wall. Wilson and colleagues employed ultrasound with electrocardiogram gating to measure the aortic wall stiffness at the point of maximum aneurysm diameter in 210 patients over a median follow-up of 19 months [4]. It was found that decreased stiffness, or increased distensibility, conferred a significant increase in rupture risk. Patients with decreased stiffness had almost as great an increased risk of rupture as patients with a 10 % increase in maximum aortic diameter (28 % versus 36 %). While illustrative of the biomechanics of the aortic wall, ultrasound with cardiac cycle tracking has several limitations, including a significant learning curve to master the technique, and moderate interobserver and intraobserver variation [5]. Electrocardiogram-gated computed tomography has been used to quantify circumferential and longitudinal cyclical strain in the aorta; however, this technique remains more of a research-oriented than a practical clinical application at this time [6].
Another manner of calculating AAA wall strength is through the ex vivo analysis of the aortic wall tissue excised from an aneurysm during surgical repair. In this manner, Di Martino and colleagues compared the wall strength of the ruptured and non-ruptured AAA [7]. Aortic wall thickness was measured using a laser micrometer, and wall strength was determined in a uniaxial tensile testing system. The thickness of the ruptured AAA was significantly greater than the non-ruptured AAA; of note, the former were not any greater in maximum diameter than the latter. Moreover, consistent with the findings of the previous study from Wilson and colleagues, decreased stiffness was associated with decreased wall strength. Therefore, both ex vivo and in vivo studies are able to assess the biomechanical properties of the aortic wall and thus aid in the description of AAA behavior. Unfortunately, the most reliable way to determine aortic wall strength is by stretching the surgically excised aortic wall tissue until it ruptures or breaks, which may explain why studies of aortic wall strength have lagged behind those of aortic wall stress.
Finally, Vorp and Vande Geest and colleagues at the University of Pittsburgh, developed circa 2006, a statistical model capable of predicting regional aortic wall strength based on the inputs: age, gender, family history of AAA, smoking status, AAA diameter, normalized regional aortic diameter, and regional intraluminal thrombus (ILT) thickness. The statistical model was validated against ex vivo specimens [8]. This has been implemented in a “rupture potential index,” or RPI, elucidated by the same group and described below.
Role of Wall Stress
Calculation of AAA wall stress with finite element analysis (FEA) remains the most widely employed method of investigating in vivo aortic biomechanics. Wall stress determinations with FEA represent a noninvasive, computational method of investigating the biomechanics of aortic aneurysms. Although the specific details of the FEA technique may vary across studies, in general, there are several fundamental steps to the process. First, finite element analysis requires the creation of a precise and robust three-dimensional (3D) reconstruction of the abdominal aorta. This 3D reconstruction is most commonly abstracted from computed tomography imaging [9]. In the case of computed tomography-based methodology, the construction of a 3D model suitable for wall stress analysis requires multi-slice spiral computed tomography scanning with collimation and rotation time that is sufficiently narrow and fast, respectively. The 3D model can be reconstructed and segmented by automatic or manual means. A semiautomatic segmentation method with automated reconstruction based on different material density followed by manual review to confirm that the automatic construction is correct is commonly used. Indeed, this technique is favored by the authors of this chapter and other investigators with extensive experience with FEA and the study of aneurysm wall stress [9, 10].
Early studies of FEA of AAA wall stress only included the wall of the abdominal aorta, while the remainder of the abdominal aorta in the 3D reconstruction was assumed to be the flow lumen. However, as CTA imaging has increased in resolution and availability, and image analysis techniques have become more sophisticated; mural thrombus and atherosclerotic calcifications have been included in models as well. Several studies have demonstrated that the inclusion of mural thrombus and calcifications has important ramifications for AAA wall stress calculations [11, 12]. An additional advancement in FEA technique has been the ability to measure the thickness of the aortic wall. Whereas prior 3D AAA reconstructions were assumed to have uniform wall thickness and improvements in computed tomography imaging provided the spatial resolution necessary to enable patient and region-specific aortic wall thickness measurements; these locally resolved aortic wall thickness measurements have been shown to improve the ability of wall stress to predict AAA behavior [10, 11].
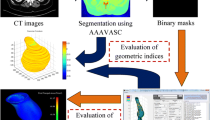
From the 3D reconstruction of the CTA, a mesh is generated, which is composed of thousands of individual nodes and elements representing the abdominal aorta, including the aortic wall, mural thrombus, and calcifications. Computerized algorithms “smooth” the mesh in order to yield a precise 3D model that is suitable for FEA. Boundary conditions and material properties of the model are specified. Boundary conditions include the blood pressure applied to the inside of the modeled aorta, while material properties refer to the mechanical characteristics of the components of the model. The aortic wall, mural thrombus, and calcification are generally given unique material properties, and may behave in an isotropic or anisotropic manner. Elastic or hyperelastic material properties are typically specified. While assigning anisotropic and hyperelastic properties to the various materials may be more accurate or realistic, these specifications will risk rendering the FEA model computationally unwieldy and time-consuming. In the clinical milieu, time-consuming imaging, image analysis and segmentation, and computational modeling are currently not tenable. Finally, the computational algorithms solve the linked partial differential equations to determine the predicted locally resolved wall stresses. These can easily be depicted visually, as in Fig. 5.1.

(a) Calculated wall thickness map overlaid onto aortic geometry. (b) Stress contour map derived from uniform wall thickness aortic geometry. (c) Stress contour map derived from variable wall thickness aortic geometry. Note the colocalization of areas with low wall thickness and high peak wall stress, especially in the aneurysm neck (From Shang et al. [10])
Wall Stress as a Predictor of AAA Rupture and Dilatation
In 2002, Fillinger and colleagues at Dartmouth Hitchcock Medical Center employed FEA to assess the association between wall stress and AAA behavior. Patients who underwent elective repair of asymptomatic AAAs, urgent repair of symptomatic AAAs, and emergent repair of ruptured AAAs were included in the study. The peak wall stress of the symptomatic and ruptured AAAs undergoing nonelective repair was significantly greater than that of the asymptomatic AAAs undergoing elective repair [9]. Moreover, even when accounting for differences in maximum aneurysm diameter, the symptomatic and ruptured AAAs still had a significantly greater peak wall stress than the asymptomatic AAAs. Indeed, the smallest ruptured AAA at 4.8 cm had a peak wall stress equivalent to that of an asymptomatic 6.3 cm abdominal aortic aneurysm. The authors also reported that the location of peak wall stress was not at the point of maximum diameter, but in the posterolateral aspect of the AAA. This location of peak wall stress coincided with the area of rupture in the six patients for whom the location of rupture was known. This seminal study from Fillinger and colleagues highlighted that a noninvasive computational biomechanical analysis of 3D AAA geometry might be superior to maximum diameter alone in predicting an aneurysm rupture risk.
Expanding on their work, Fillinger and colleagues analyzed the ability of maximum diameter versus peak wall stress to predict rupture risk over time in a cohort of patients with AAAs under prospective longitudinal observation [13]. One hundred and three patients with AAAs were assessed in an elective setting: 42 underwent observation without intervention within 1 year of their assessment, 39 underwent elective repair within 1 year, and 22 underwent emergent repair for rupture (n = 8) or symptoms (n = 14). Both index maximum diameter and peak wall stress differed between the groups; however, the latter appeared to better differentiate the AAAs that required emergent repair by receiver operating characteristic curve analysis. Multivariate analysis confirmed that peak wall stress, and not maximum aneurysm diameter, was an independent predictor of rupture risk over time. In addition to these results, the authors reported that almost one-quarter of the patients with ruptured and symptomatic AAAs who underwent emergent repair had maximum aneurysm diameters of 5 cm or less. Approximately three-quarters of the patients who underwent observation without intervention had peak wall stresses lower than the lowest recorded peak wall stress for AAAs that required emergent repair. The findings of this later study by Fillinger and colleagues confirmed those of the previous investigation, suggesting that differences in wall stress could be identified early in the evaluation and treatment of patients with AAA, and thus that FEA might be useful in clinical decision-making.
Additional evidence in support of the role of wall stress in predicting AAA natural history comes from Li and colleagues [14]. Utilizing the rate of AAA expansion as a metric of the risk of aneurysm rupture, these authors sought to analyze the association between wall stress and aneurysm growth. Patients with AAA were included in a longitudinal study with serial computed tomography imaging. Patients with AAA that expanded rapidly (≥4 mm/year) had higher baseline wall stress than slowly expanding AAA (≤4 mm/year). There was no difference in baseline maximum aortic diameter between the two groups. This investigation suggested that AAA with higher wall stress have a greater rate of expansion and consequently a greater risk of rupture. The authors concluded that while the decision to repair AAA remains multifaceted, wall stress could play a role in the management of AAA with diameters in the range of 4–5.5 cm.
As indicated in the prior section, investigators at the University of Pittsburgh have also examined the computationally predicted aortic wall stress in AAAs. However, they have concentrated their efforts on a locally and regionally resolved RPI, instead of peak wall stress alone. They defined the RPI as the ratio between local wall stress and local wall strength, and found that RPI was higher – though the difference was not statistically different – in ruptured than intact AAA [15]. Interestingly, the wall strength was significantly lower in the ruptured group than the intact group, casting some doubt on the clinical utility of wall stress calculations in isolation. Other groups have implemented analyses bases on the RPI formulation: among these is the Munchën group who did find statistically significant increased RPI in symptomatic and ruptured AAA [16].
Our laboratory at the University of Pennsylvania has recently demonstrated the ability to detect the regional aortic wall thickness of the abdominal aorta, including in areas with mural thrombus present [17]. Furthermore, Shang and colleagues in the same lab have shown that the inclusion of locally resolved aortic wall thickness significantly impacts FEA estimates of peak wall stress and that variable wall thickness computational models are more correlated with expansion of AAAs (a putative marker of rupture risk) than are models assuming a uniform aortic wall thickness [10].
Role of Wall Stress in Other Pathologies
Thoracic Aortic Rupture Risk Prediction
While indications for repair of infrarenal AAA are well established, and patients with 6 cm AAA have a high 3-year mortality, similar straightforward and rational indications for the treatment of thoracic aortic pathologies are not uniformly accepted. Historically, an elective repair of descending thoracic aortic aneurysms (DTAA) and thoracoabdominal aortic aneurysms was not universally recommended until maximal diameter exceeded 6.5 cm [18]. But elective repair of even 6.5 cm DTAA is much less compelling than the repair of 5 cm AAA’s: only 30 % of 6.5 cm DTAA are expected to be ruptured in 5 years [19]. Surgeons cannot simply ignore relatively small thoracic aneurysms either: the annual risk of rupture, dissection, or death at a diameter of 6.0 cm is 16 % [12]. Therefore, computational stress modeling or other biomechanical indices might play in guiding therapeutic decisions in patients with thoracic aortic aneurysms.
Our laboratory has investigated this possibility and demonstrated that computational peak wall stress was strongly correlated with aneurysm expansion rate, a proxy for rupture risk (Fig. 5.2) [20]. In addition, Shang and colleagues showed that more sophisticated FEA models (Fig. 5.3), incorporating variable aortic wall thickness, intraluminal thrombus, and aortic calcification, predicted very different peak wall stresses, highlighting the importance of choosing an appropriately refined and validated computational model for aneurysm rupture risk prediction [21].

Correlations between thoracic aortic expansion rate and initial diameter (left) and between thoracic aortic expansion rate and peak wall stress (right), demonstrating that peak wall stress is a better predictor of aneurysm expansion rate (From Shang et al. [13])

Von Mises wall stress distribution in the descending thoracic aorta of a patient with an aneurysm. (a) with locally resolved wall thickness. (b) with uniform wall thickness (From Shang et al. [14])
Summary
While computational wall stress modeling of AAAs can better predict rupture than diameter-based risk assessment alone, FEA, RPI, and similar computationally based models have not been implemented clinically to any significant degree. Nevertheless, the clinical insights derived from biomechanical analyses currently can influence our understanding of AAA rupture risk, and future work formally incorporating computational stress modeling into clinical decision-making should be emphasized. Meanwhile, our management of other pathologies, including thoracic aortic aneurysms, should be influenced by predictive biomechanical analyses.
References
Nicholls SC, Gardner JB, Meissner MH, Johansen HK. Rupture in small abdominal aortic aneurysms. J Vasc Surg. 1998;28:884–8.
Brown LC, Powell JT. Risk factors for aneurysm rupture in patients kept under ultrasound surveillance. UK Small Aneurysm Trial Participants. Ann Surg. 1999;230:289–96.
Chiu KW, Ling L, Tripathi V, Ahmed M, Shrivastava V. Ultrasound measurement for abdominal aortic aneurysm screening: a direct comparison of the three leading methods. Eur J Vasc Endovasc Surg. 2014;47:367–73.
Wilson KA, Lee AJ, Lee AJ, Hoskins PR, Fowkes FG, Ruckley CV, Bradbury AW. The relationship between aortic wall distensibility and rupture of infrarenal abdominal aortic aneurysm. J Vasc Surg. 2003;37:112–7.
Wilson KA, Hoskins PR, Lee AJ, Fowkes FG, Ruckley CV, Bradbury AW. Ultrasonic measurement of abdominal aortic aneurysm wall compliance: a reproducibility study. J Vasc Surg. 2000;31:507–13.
Morrison TM, Choi G, Zarins CK, Taylor CA. Circumferential and longitudinal cyclic strain of the human thoracic aorta: age-related changes. J Vasc Surg. 2009;49:1029–36.
Di Martino ES1, Bohra A, Vande Geest JP, Gupta N, Makaroun MS, Vorp DA. Biomechanical properties of ruptured versus electively repaired abdominal aortic aneurysm wall tissue. J Vasc Surg. 2006;43:570–6.
Vande Geest JP, Wang DH, Wisniewski SR, Makaroun MS, Vorp DA. Towards a noninvasive method for determination of patient-specific wall strength distribution in abdominal aortic aneurysms. Ann Biomed Eng. 2006;34(7):1098–106.
Fillinger MF, Raghavan ML, Marra SP, Cronenwett JL, Kennedy FE. In vivo analysis of mechanical wall stress and abdominal aortic aneurysm rupture risk. J Vasc Surg. 2002;36:589–97.
Shang EK, Nathan DP, Woo EY, Fairman RM, Wang GJ, Gorman RC, Gorman 3rd JH, Jackson BM. Local wall thickness in finite element models improves prediction of abdominal aortic aneurysm growth. J Vasc Surg. 2015;61:217–23.
Wang DH, Makaroun MS, Webster MW, Vorp DA. Effect of intraluminal thrombus on wall stress in patient-specific models of abdominal aortic aneurysm. J Vasc Surg. 2002;36:598–604.
Li ZY, U-King-Im J, Tang TY, Soh E, See TC, Gillard JH. Impact of calcification and intraluminal thrombus on the computed wall stresses of abdominal aortic aneurysm. J Vasc Surg. 2008;47:928–35.
Fillinger MF, Marra SP, Raghavan ML, Kennedy FE. Prediction of rupture risk in abdominal aortic aneurysm during observation: wall stress versus diameter. J Vasc Surg. 2003;37:724–32.
Li ZY, Sadat U, U-King-Im J, Tang TY, Bowden DJ, Hayes PD, Gillard JH. Association between aneurysm shoulder stress and abdominal aortic aneurysm expansion: a longitudinal follow-up study. Circulation. 2010;122:1815–22.
Vande Geest JP, Di Martino ES, Bohra A, Makaroun MS, Vorp DA. A biomechanics-based rupture potential index for abdominal aortic aneurysm risk assessment: demonstrative application. Ann N Y Acad Sci. 2006;1085:11–21.
Maier A, Gee MW, Reeps C, Pongratz J, Eckstein HH, Wall WA. A comparison of diameter, wall stress, and rupture potential index for abdominal aortic aneurysm rupture risk prediction. Ann Biomed Eng. 2010;38:3124–34.
Shang EK, Lai E, Pouch AM, Hinmon R, Gorman RC, Gorman 3rd JH, Sehgal CM, Ferrari G, Bavaria JE, Jackson BM. Validation of semiautomated and locally resolved aortic wall thickness measurements from computed tomography. J Vasc Surg. 2015;61:1034–40.
Coady MA, Ikonomidis JS, Cheung AT, Matsumoto AH, Dake MD, Chaikof EL, Cambria RP, Mora-Mangano CT, Sundt TM, Sellke FW. Surgical management of descending thoracic aortic disease: open and endovascular approaches: a scientific statement from the American Heart Association. Circulation. 2010;121:2780–804.
Davies RR, Goldstein LJ, Coady MA, Tittle SL, Rizzo JA, Kopf GS, Elefteriades JA. Yearly rupture or dissection rates for thoracic aortic aneurysms: simple prediction based on size. Ann Thorac Surg. 2002;73:17–28.
Shang EK, Nathan DP, Sprinkle SR, Vigmostad SC, Fairman RM, Bavaria JE, Gorman RC, Gorman 3rd JH, Chandran KB, Jackson BM. Peak wall stress predicts expansion rate in descending thoracic aortic aneurysms. Ann Thorac Surg. 2013;95:593–8.
Shang EK, Nathan DP, Sprinkle SR, Fairman RM, Bavaria JE, Gorman RC, Gorman 3rd JH, Jackson BM. Impact of wall thickness and saccular geometry on the computational wall stress of descending thoracic aortic aneurysms. Circulation. 2013;128:S157–62.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Nathan, D.P., Jackson, B.M. (2017). Wall Stress. In: Starnes, B., Mehta, M., Veith, F. (eds) Ruptured Abdominal Aortic Aneurysm. Springer, Cham. https://doi.org/10.1007/978-3-319-23844-9_5
Download citation
DOI: https://doi.org/10.1007/978-3-319-23844-9_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-23843-2
Online ISBN: 978-3-319-23844-9
eBook Packages: MedicineMedicine (R0)