
Abstract
Localized pancreatic cancer remains a therapeutic challenge despite advances in multiple treatment techniques. In patients with borderline resectable and unresectable (locally advanced) pancreatic cancer, stereotactic body radiation therapy (SBRT) has emerged as a promising treatment option. Potential benefits include shorter treatment duration and increased patient convenience, encouraging surgical outcomes, lower acute toxicity, and reduced delay of chemotherapy. In the last decade, multiple retrospective reports have been published on this technique. More recently, prospective assessment of SBRT in pancreatic cancer has demonstrated increased resectability of previously unresectable lesions, as well as lower rates of margin-positive resections. As a higher dose of radiation is utilized, however, this technique requires careful patient selection and treatment planning to ensure safety. In this chapter, the published literature using SBRT in pancreatic cancer, along with treatment recommendations and contraindications, is presented. Long-term data regarding SBRT is forthcoming and may result in the adoption of this technique not only as an adequate option, but also as the future standard-of-care.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Pancreas cancer
- Pancreatic cancer
- Carcinoma
- Stereotactic
- SBRT
- SABR
- Locally advanced
- Unresectable
- Borderline
- Borderline resectable
- Radiation
- Radiotherapy
- Localized
- Non-metastatic
Introduction
Despite improvements in imaging, treatment, and symptom management, the prognosis of a patient with newly diagnosed pancreatic cancer remains exceedingly poor. In 2015, it is estimated that 40,560 of the 48,960 patients diagnosed with pancreatic cancer will die as a consequence of the disease [1]. This translates to an 83 % mortality rate. Pancreatic cancer is the fourth most common cause of cancer-related death among both men and women in the United States [1]. At this time, no prospectively validated screening tool is available, though the incidence of this disease continues to rise.
The majority of patients who present with localized—borderline resectable (BRPC) and locally advanced (LAPC) tumors—disease are unable to undergo a curative resection due to extensive tumor involvement of adjacent vasculature. In these patients, the options for potentially curative therapy include concurrent chemoradiation (CRT), aggressive multi-agent chemotherapy, or chemotherapy followed by CRT [2]. While standard fraction radiation has been considered the standard-of-care in both BRPC and LAPC patients for decades, more recent data has questioned the impact of conventional three-dimensional conformal radiation therapy (3D-CRT) on overall survival, and a significant debate in the field of gastrointestinal oncology has resulted [3–5].
Advanced imaging and radiation techniques allow for an increase in the precision of radiation delivery. The field of radiation oncology has witnessed a paradigm shift in the delivery of radiotherapy from small daily fractions of radiation (1.8–2.5 Gy/day) to large daily doses given over fewer consecutive days or alternating days (5–40 Gy/day) [6]. This radiotherapy technique, entitled stereotactic body radiotherapy (SBRT) or stereotactic ablative radiotherapy (SABR) , is now gaining traction in pancreatic cancer as an option for patients with borderline resectable and locally advanced disease. By delivering a higher daily dose per fraction of radiation over a shorter total number of days, this treatment appears to result in an increased biologically effective dose (BED) as compared to standard radiation [7]. In doing so, a higher level of tumor sterilization and improved clinical and pathologic outcomes may be achieved. This can be seen in Fig. 8.1, which provides anecdotal radiographic evidence of the marked response observed after a patient received FOLFIRINOX (5-fluorouracil, irinotecan, leucovorin, and oxaliplatin) chemotherapy and SBRT.

Computed tomography scan of a locally advanced tumor (a) prior to chemotherapy and (b) following chemotherapy and SBRT to 33 Gy in 5 fractions. Patient then underwent a successful margin- and node-negative resection in which only scattered microscopic foci of adenocarcinoma (a near-pathologic complete response) was found
In this chapter, we will explore the published data, including that of retrospective and prospective studies in the field of SBRT for pancreatic cancer. The opportunities and challenges in the utilization of this technique, including appropriate patient selection and treatment methodology, will be discussed.
Resectability in Borderline Resectable and Locally Advanced Pancreatic Cancer
In pancreatic cancer , surgical resectability is considered paramount in achieving a cure. To determine whether a tumor is resectable, careful consideration of arterial and venous involvement—the superior mesenteric artery (SMA), celiac axis, common hepatic artery (CHA), superior mesenteric vein (SMV), and portal vein (PV) specifically—is taken into account. While the nomenclature defining surgical resectability has remained fairly constant for years, the definition of borderline resectable disease was recently formalized by a consensus group from the Americas Hepato-Pancreatico-Biliary Association (AHPBA), Society of Surgical Oncology (SSO), and Society for Surgery of the Alimentary Tract (SSAT) [8]. These criteria are often referred to as the Consensus or Callery guidelines and have been reproduced in Table 8.1. The criteria adopted by the National Comprehensive Cancer Network (NCCN) are listed in Table 8.2 [2]. A more refined definition of borderline resectable tumors, classically a difficult subgroup to define, is noted in Table 8.3 [9]. The definition listed in Table 8.3 provides specific criteria used in the Intergroup trial (A021101) testing neoadjuvant FOLFIRINOX followed by 50.4 Gy of external beam radiation and capecitabine in patients with borderline resectable pancreatic cancer [9]. Due to the heterogeneous definitions of resectability, careful consideration of these criteria and the involved vasculature is necessary to compare clinical outcomes among populations involving patients with borderline resectable and locally advanced pancreatic cancer. Standardization of resectability in pancreatic cancer is essential.
In general, patients with LAPC are considered unsuitable candidates for upfront surgery, in part due to the morbidity and mortality risk associated with vasculature resection [10]. Additionally, the decision to resect a tumor with a high likelihood of a positive margin at the site of vascular involvement is suboptimal as the survival of patients with a microscopically (R1) or grossly (R2) positive margin has been shown to be significantly inferior to patients resected to a negative (R0) margin [10, 11]. The standard-of-care in these patients is most often upfront chemotherapy alone or CRT. The goal of this therapy is to optimally downsize (or, if possible, sterilize) the tumor to allow for surgical resection and increase the likelihood of improved pathologic outcomes (i.e., margin- and node-negative resection, pathologic complete response). In fact, a recent study has suggested promising outcomes in 40 patients with BRPC or LAPC who underwent neoadjuvant FOLFIRINOX (5-fluorouracil, irinotecan, leucovorin, and oxaliplatin) therapy. Of these 40 patients, 30 (75 %) received radiation therapy: 24 received 50.4 Gy CRT and 5-fluorouracil (5-FU), 10 of which also received a 7–12 Gy intraoperative radiation therapy (IORT) boost, and 6 received proton beam therapy with charged particles. On final pathology, the patients who received neoadjuvant therapy had a significant decrease in lymph node positivity (35 % vs. 79 %) and perineural invasion (72 % vs. 95 %) in comparison with 87 patients who underwent upfront surgery. Furthermore, the neoadjuvant patients achieved margin-negative and node-negative resection rates of 92 % and 65 %, respectively.
Unpublished data exploring neoadjuvant SBRT in borderline and locally advanced patients at Johns Hopkins University. Among 80 resected patients with BRPC or LAPC, 33 received neoadjuvant chemotherapy alone and 47 received induction chemotherapy followed by SBRT. FOLFIRINOX-based chemotherapy was administered to 63 and 45 % of the SBRT group and chemotherapy group, respectively. The majority (57 %) of SBRT patients were deemed unresectable while only 24 % in the chemotherapy alone group had LAPC (p = 0.009). Pancreaticoduodenectomy was performed in 68 % of patients who underwent SBRT vs. 85 % of patients who received chemotherapy (p = NS). In the SBRT group, the R0 resection rate was 85 % in BRPC and 89 % in LAPC vs. 48 % in BRPC and 63 % in LAPC patients in the chemotherapy group (p = NS). Node-negative resections were achieved in 72 % of patients who received SBRT (60 % in BRPC, 81 % in LAPC) vs. 42 % of patients who received chemotherapy alone (40 % in BRPC, 50 % in LAPC) (p = NS). The pathologic complete response rate was 13 % in the SBRT group (10 % in BRPC, 15 % in LAPC) vs. 3 % in the chemo group (0 % in BRPC, 13 % in LAPC) (p = NS). The near-pathologic complete response rate, defined as microscopic foci of single cells or groups of single cells of adenocarcinoma, was 28 % in the SBRT group (25 % in BRPC, 30 % in LAPC) vs. 12 % in the chemotherapy group (12 % in BRPC, 13 % in LAPC) (p = NS). Figures 8.2 and 8.3 demonstrate the extensive treatment effect seen macroscopically (Fig. 8.2) and microscopically (Fig. 8.3) in patients who underwent neoadjuvant SBRT. Further follow-up data is underway to determine the impact of these pathologic outcomes on survival.

Resected bivalve specimen has been sliced along the pancreatic duct. The pancreas (the left side) looks hyperemic. The tumor is located in the center. The upstream pancreas is to the right (towards the spleen). The dilated pancreatic duct and the stroma appear to be edematous. Courtesy of Ralph H. Hruban

Microscopic evidence of (a) extensive treatment effect observed following pancreas SBRT to a tumor that was measured to be 3.8 cm in size, and (b) the presence of hemosiderin-laden macrophages (brown cells), inflammatory cells that are suggestive of a reactive process following therapy
Standard Treatment for Borderline Resectable and Locally Advanced Pancreatic Cancer
The morbidity and potential mortality associated with surgical resection of BRPC and LAPC implies that CRT or chemotherapy alone is the only viable option for cure in these patients [12]. Despite the completion of multiple studies on this topic, no consensus regarding the optimal course of management exists. The most recent NCCN clinical practice guidelines recommend enrollment onto a clinical trial as the first-line option [2]. In patients with good performance status, multi-agent chemotherapy followed by CRT is considered appropriate.
Data supporting the above approach are derived from decades of clinical trials dating back to the 1980s [4, 5, 13–17]. Table 8.4 presents a selection of the clinical trials which have investigated the role of standard fractionated radiation in LAPC. As is evidenced by the table, the survival of patients has not progressed dramatically despite the numerous advances in chemotherapy agents and radiation technology in the last three decades.
The most significant debate in the appropriate management of patients with BRPC and LAPC centers on the role of radiation in this disease. Some studies have demonstrated a survival decrement with the application of radiation therapy in this patient population. However, these studies suffer from major drawbacks, including poor radiation quality assurance, excess radiation dose, unclear dose constraints for adjacent critical structures, and the use of “split-course” radiation in which a 2-week treatment break is part of the planned course of treatment. Other studies have shown a potential benefit for radiotherapy [4]. However, a major criticism of all these data is the utilization of outdated or ineffective chemotherapy.
A more modern approach to the treatment of this disease has been to use combination chemotherapy with either FOLFIRINOX or gemcitabine with nab-paclitaxel [18–20]. These two combination chemotherapeutic regimens have demonstrated a survival benefit in comparison to gemcitabine alone, albeit in the metastatic setting. In BRPC and LAPC, the current NCCN guidelines recommend either single-agent gemcitabine or combination chemotherapy, with CRT preferred following a course of initial chemotherapy. SBRT is listed as an option, though its use is encouraged as part of enrollment on a clinical trial [2].
Stereotactic Body Radiation Therapy
Traditional radiotherapy has been delivered in small daily fractions to take advantage of the ability of normal human tissue to repair radiation more quickly than tumor tissue. This “therapeutic window” is particularly critical in anatomical locations prone to severe, irreparable radiation damage [7]. One of the dangers of using high-dose-per-fraction radiation is the risk of overwhelming the therapeutic window and damaging sensitive adjacent normal tissues without precise targeting of the tumor [21, 22]. However, the development of advanced radiotherapy techniques in the last two decades has dramatically changed the landscape of radiation oncology [6].
SBRT is defined as the use of intensity modulation, image guidance, tumor motion control, and stereotactic targeting to deliver a high dose of radiation to the tumor in five or less fractions [6]. Each of the aforementioned techniques and technological developments contributed to the ability to use this type of treatment. Image guidance ensures that the tumor and/or fiducial or stent is visualized at the time of each treatment, allowing for reduced treatment margins (thereby reducing normal tissue exposure). Whereas treatment margins had historically been measured in centimeters, the use of this technology has reduced these margins to only a few millimeters (mm) [6].
SBRT was first used to treat intracranial neoplasms [23]. Later, this was expanded to extracranial sites, particularly with early stage lung cancer, demonstrating outstanding local control, virtually absent acute (<3 months) toxicity, and minimal chronic (>3 months) toxicity [24]. By nature of its “parallel” normal tissue unit arrangement, lung tissue benefits from being able to receive an ablative dose to one region without compromising the overall function of the organ. In contrast, the perceived risk of using SBRT in locations abutting normal tissues with a “serial” arrangement of normal tissues, including the small bowel and stomach as seen with the pancreas, is more concerning. Consequently, SBRT to areas within the abdomen and pelvis have been adopted with much more caution [6]. Without a firm understanding of the dose constraints of these sensitive organs at risk (OARs), practitioners have been hesitant to use ablative doses of radiation in this region. As data has emerged from groups that have utilized this approach, a stronger understanding of the dose tolerance of the small bowel and stomach has led to the widespread adoption of SBRT in the infradiaphragmatic space [25]. An analysis of patterns of care of radiation delivery from 39 centers in the United States indicates that the use of SBRT for pancreatic cancer is increasing, but still represents a relatively small absolute value [25].
In the following sections, the clinical results, toxicities, and techniques for the safe and effective utilization of pancreas SBRT are described.
Clinical Trials Utilizing SBRT for Borderline Resectable and Locally Advanced Pancreatic Cancer
In the last decade, retrospective reports and prospective clinical trials have supported the use of pancreas SBRT as a potent method for providing excellent tumor control, increasing resectability rates, and improving surgical outcomes in patients with BRPC and LAPC (Table 8.5) [26–40]. However, heterogeneity in selection criteria, patient immobilization technique, radiation dose, radiation planning techniques, and radiation delivery devices limit direct comparisons between these studies.
The first published data using SBRT in pancreatic cancer was from researchers at Stanford University [26]. Koong and colleagues described their experience treating 15 patients with LAPC using a CyberKnife (Accuray Inc, Sunnyvale, CA, USA) linear accelerator. Two patients had previously received conventionally fractionated radiation to a dose of 50 Gy. This phase I dose escalation study planned to increase radiation dose from 15 to 25 Gy in a single fraction if patients met predefined toxicity criteria at 12 weeks. Three patients were treated at 15 Gy in one fraction, five patients at 20 Gy in one fraction, and seven patients at 25 Gy in one fraction. Even at the highest dose level, no grade 3 or greater acute toxicity was observed. With a median follow-up of 5 months, no local failures were observed, though this may be a consequence of the short median follow-up interval. The median survival noted in the study was 11 months and, in that time, only acute grade 2 or less toxicity was observed.
Shortly thereafter, researchers from Aarhus University in Denmark published their experience with linear accelerator (Linac)-based SBRT [27]. Their phase I trial used three fractions of 15 Gy each in 22 patients with LAPC. The results of this trial were significantly inferior to the local control rate and overall survival seen in the aforementioned Stanford study. Local control was only achieved in 57 % of patients, and median overall survival was 5.4 months (vs. 11 months in the Stanford study). Finally, when assessing patient tolerability of this regimen, a much higher toxicity rate was seen, with 79 % of patients experiencing a grade 2 or greater toxicity.
Considering the starkly different results for both trials using the same disease and treatment, a comparison of the treatment technique in both sets of clinical trials must be performed. In the 2004 Stanford study, the breath-hold technique was used to account for tumor motion during respiration. Each dose of radiation was delivered during deep inspiration only, allowing for small tumor margins of 2.5 mm [26]. However, in the 2005 Aarhus analysis, abdominal compression was utilized, and the tumor margins were much larger: 10 mm in the cranio-caudal dimension and 5 mm in the transverse dimension [27]. Additionally, whereas implanted fiducials within the tumor were used to target the lesion during treatment in the Stanford trial, this was not performed in the Aarhus trial [26, 27]. Based on interpretation of these two sets of data, the recommendation for the implementation of SBRT in pancreatic cancer has been to use both tumor motion management strategies as well as image guidance to optimally target the lesion and limit margins to <5 mm. This has limited untoward treatment-related toxicity and improved oncologic outcomes.
The largest prospective experience in pancreas SBRT has recently been published [40]. This multi-institutional phase II trial included patients treated at three major academic centers and accrued 49 LAPC patients. All patients were allowed up to 3 doses of gemcitabine (to allow time for SBRT simulation and planning), followed by a five-fraction SBRT regimen to a total cumulative dose of 33 Gy (6.6 Gy per fraction) delivered over a maximum of 2 weeks. While direct comparison to prior trials can be challenging, the median overall survival of 13.9 months seen in this trial is superior to other published studies. Despite including only patients with LAPC, 18 % of patients survived 2 years or longer from the date of diagnosis. The local control rate was equally impressive; the 1-year freedom from local progression was 78 %.
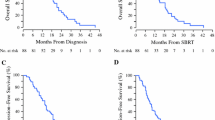
A large retrospective series of patients treated with pancreas SBRT has been published by investigators from Johns Hopkins University [39]. Eighty-eight patients with both BRPC and LAPC were treated with five-fraction SBRT treated to a total dose of 33 Gy. Of these 88 patients, 14 had BRPC and 74 had LAPC, and 32 (80 %) of the 74 patients with LAPC were treated on the aforementioned multi-institutional clinical trial. All patients had an ECOG performance status of 0 or 1. Prior to radiation, the vast majority of patients were treated with gemcitabine-based or FOLFIRINOX chemotherapy. Survival from diagnosis for the entire cohort was 18.4 months, specifically 18.4 months for patients with LAPC and 14.4 months for patients with BRPC. As with the multi-institutional trial, SBRT appeared to significantly improve local control, with median local progression-free survival found to be 13.9 months. However, the overall progression-free survival in this study was 9.8 months, demonstrating that distant failure continues to be a major detriment in this patient population.
A decade worth of published data demonstrates that SBRT in BRPC and LAPC is effective in providing local tumor control, and in some cases, significant patient longevity. However, the matter of patient safety remains critical in deciding whether or not this treatment is appropriate to supplant the role of standard dose and fractionation radiation.
Stereotactic Body Radiation Therapy and Treatment-Related Toxicity
To determine the safety profile of SBRT in pancreatic cancer, the most severe toxicities from the published studies should be analyzed.
Standard radiotherapy for pancreatic cancer, in which up to 6 weeks of daily fractionated radiation are delivered, is accompanied by fairly significant toxicity, most commonly gastrointestinal and hematologic, throughout the duration of treatment [4]. Indeed, early radiotherapy trials that demonstrated inferior outcomes with the application of adjuvant radiation included a mandatory 2-week treatment break due to known treatment toxicity [41]. Due to the exquisite radiosensitivity of the gastrointestinal tract, the proximity of the stomach, small bowel, and large bowel presents a significant challenge for delivering radiation in the acute setting. However, fractionated treatment maintains the integrity of the gastrointestinal tract by limiting the dose to critical structures below an established threshold. Chronic devastating toxicity, including gastrointestinal obstruction, ulcer, and perforation, may generally be avoided with fractionation.
While SBRT may allow for limited acute toxicity due to the completion of radiation within 3–5 treatments, the initial concerns from the greater radiation oncology community have been the risk of potentially lethal late toxicities resulting from a higher BED to sensitive gastrointestinal structures [21, 22]. However, the published data demonstrate that, by and large, SBRT can be completed with minimal acute and late toxicity when performed with appropriate patient selection, tumor motion control, image guidance, and well-defined dose constraints [26–40]. As previously discussed, abdominal SBRT is imprecise and potentially destructive without tumor motion management and image guidance [26, 27].
To understand the risk of toxicity from this type of treatment, a comparison may be made between two different SBRT regimens from separate institutions. Investigators from Harvard University have published their results using a three-fraction SBRT regimen treating up to a total dose of 36 Gy (BED10 Gy = 79 Gy, BED3 Gy = 180 Gy) [33]. While a significant number of patients had acute grade 1 (56 % fatigue, 18 % nausea) and grade 2 (23 % nausea) toxicity, no acute grade 3 or greater toxicity was seen. Further, the rate of late grade 3 or greater toxicity was also low, noted in only 6 % of patients (two patients with gastrointestinal hemorrhage requiring endoscopic intervention and transfusion, one patient with gastric outlet obstruction). Motion management was achieved using implanted fiducials within the tumor thereby allowing for tumor tracking using the CyberKnife Synchrony system (Accuray Inc., Sunnyvale, CA).
Investigators from Johns Hopkins University have utilized a five-fraction SBRT regimen treated up to a total dose of 33 Gy (BED10 Gy = 54 Gy, BED3 Gy = 103 Gy) [39]. Acute toxicity was found to be fairly minimal, with the two most common grade 2 toxicities reported as lymphopenia (14.7 % of patients) and fatigue (8.0 %). Acute grade 3 or greater gastrointestinal toxicities occurred in 3.4 % of patients. Late grade 3 or greater toxicity occurred in five patients (5.7 %): three duodenal ulcers (grade 3), one enteric fistula (grade 4), and one gastrointestinal hemorrhage (grade 5). The late grade 5 toxicity occurred in a patient with tumor invasion into the duodenal wall. Following tumor regression after treatment with SBRT, an ulcer resulted and, after a biliary stent exchange, he possibly had a perforation that resulted in a fatal gastrointestinal hemorrhage less than a day later. Because these events were a possible late toxicity due to the SBRT, the investigators adjusted their patient enrollment criteria to ensure that any patient with direct tumor invasion into the lumen of the stomach or duodenum on endoscopic ultrasound is ineligible for SBRT. Treatment planning on this protocol included a pretreatment endoscopic ultrasound with the implantation of gold fiducials to identify the lesion, a breath-hold technique to prevent tumor motion, and daily cone-beam computed tomography to accurately track the lesion during treatment.
Despite using a higher BED of radiation, the above data support the safety of SBRT in BRPC and LAPC when using appropriate tumor localization, motion management, and daily imaging. It is anticipated that long-term data and a comparison between standard radiation and dose-escalated SBRT will be forthcoming from the Alliance for Clinical Trials in Oncology three-arm clinical trial that is currently being developed to investigate the role of neoadjuvant chemotherapy vs. chemoradiation vs. chemotherapy and SBRT.
Impact of Stereotactic Body Radiation Therapy on Quality of Life and Pain
Even in pancreatic cancer patients who respond well to the most aggressive therapies, life expectancy is limited and maximizing quality of life and ameliorating pain is imperative. In addition to physician assessment of patient toxicity, several validated metrics have been used to assess patient-reported outcomes such as quality of life and symptom burden. Most frequently employed are the European Organization for Research and Treatment in Cancer quality of life core cancer questionnaire (EORTC QLQ-C30) and pancreatic cancer-specific module (EORTC QLQ-PAN26) [42, 43]. Although quality of life data are scarce, there have been a few published reports that explore these outcomes.
A number of studies have used these questionnaires in the setting of standard CRT in BRPC and LAPC [44, 45]. Serrano and colleagues reported a decline in global quality of life after neoadjuvant standard CRT and one cycle of chemotherapy in BRPC and resectable patients, whereas additional studies demonstrated unchanged or improved global quality of life at 3–4 month post-CRT follow-up when compared to baseline [45, 46]. Improvement in pain and jaundice after completion of CRT was reported; however, patients also experienced deterioration in physical and social functioning, an increase in diarrhea, nausea, and vomiting, and a variable impact on appetite change.
The previously mentioned prospective SBRT study indicated unchanged global quality of life scores from baseline to 4 weeks after SBRT and 4 months after SBRT [40]. Furthermore, patients demonstrated a significant improvement in pancreatic pain, body image, and jaundice scores on the QLQ-PAN26 from pre-SBRT values to 4 weeks post-SBRT. From 4 weeks pre-SBRT to 4 months post-SBRT, an improvement in body image approached statistical significance (Rao et al., publication forthcoming). Further prospective evaluation of quality of life data is necessary to assess optimal therapies in localized pancreatic cancer.
Stereotactic Body Radiation Therapy in Patients with Recurrent Pancreatic Cancer
Given the locally aggressive nature of pancreatic cancer , local recurrences may occur even after resection and adjuvant concurrent CRT. Surgical resection in the setting of recurrent disease is often difficult and, even when accomplished, rarely results in disease clearance [47]. In patients previously treated with standard radiation who later suffer local tumor progression, SBRT has been investigated as a viable option to provide local control or to palliate epigastric pain. Limited data exists regarding this patient population, but at least three studies have utilized SBRT in this clinical scenario, and are listed in Table 8.6 [35, 48, 49].
Tozzi and colleagues combined their analysis of patients treated with SBRT in LAPC and the setting of recurrent pancreatic disease [35]. Their analysis did not separate these two entities, but they specifically noted that the local control outcome in patients treated in the recurrent setting and LAPC were equivalent when using a dose of 45 Gy in six fractions (76 % at 2 years).
Lominska et al. and Wild et al. have published their individual institutional results in patients treated with SBRT for recurrent disease following standard CRT [48, 49]. Lominska and colleagues reported their results on the treatment of 28 patients treated with SBRT in the recurrent setting after receiving a median dose of 50.4 Gy of prior external beam radiation [48]. Various treatment fractionation schemes were utilized, most commonly 24 or 21 Gy in three fractions. Median follow-up was expectedly short in this analysis (5.9 months), with 1-year survival noted to be 18 %. Local control, however, was achieved in 86 % of patients. Wild and colleagues utilized Linac- and CyberKnife-based radiation delivery of SBRT (to a median dose of 25.0 Gy in five fractions) to 18 patients who experienced local progression after adjuvant CRT (15 patients) or definitive CRT (3 patients) to a prior median dose of 50.4 Gy at Stanford or Johns Hopkins University [49]. Median overall survival in this patient population was found to be 8.8 months following SBRT. Furthermore, 57 % of patients with abdominal or back pain prior to SBRT were able to achieve palliation following treatment delivery. The time frame of local recurrence at 9 months was found to be an important delineation in this study. Patients who suffered local recurrence within 9 months following initial surgery or definitive CRT lived only 3.4 months following SBRT, whereas those whose local failure occurred after 9 months lived 11.3 months following SBRT (p = 0.019). Freedom from local progression was 78 % at 6 months and 62 % at 12 months after completing SBRT, likely reflecting the lower BED of this fractionation. The treatment was safe in both of these studies, with late grade ≥3 toxicity in two patients and one patient, respectively.
In this population with limited treatment options, SBRT represents a reasonable option for safe and effective local tumor control. Although prospective data in this patient population is likely to be limited, enrollment on clinical trials or tumor registries should be encouraged to gather further information and gain long-term efficacy and toxicity data.
Techniques for Implementation of Stereotactic Body Radiation Therapy in Pancreatic Cancer
SBRT trials in pancreatic cancer may vary in the dose utilized, but consistently use multiple measures to ensure patient safety and reproducibility. At all phases of the treatment, from simulation to radiation delivery, accuracy and precision are paramount. The following section represents the authors’ consensus on patients treated definitively with pancreas SBRT [34]. Appropriate patient selection is the first step in delivering safe treatment with SBRT. Patients should be in a position to benefit from this more aggressive local treatment, i.e., ideally a performance status of two or better (ECOG ≤2). Specifically, a life expectancy of more than 6 months should be considered minimum, as was noted on the prospective, multi-institutional trial [40]. Tumor size is an additional key criterion, though this varies between studies—most of which involve a tumor under 100 cc, though the largest PTV was noted to be greater than 500 cc [26, 33, 37, 40].
A pre-radiation upper endoscopy procedure should be performed to accurately stage the tumor, to assess tumor extent into the duodenum and/or stomach, and to place gold markers (fiducials) into the lesion for precise tumor localization. We believe there is an increased risk of complications when the tumor directly extends into the stomach or bowel. Consequently, the investigators recommend that SBRT be limited to patients without this adverse finding. Regarding the placement of fiducial markers into the pancreas, one study has explored whether coiled fiducials were superior to traditional, linear fiducials in reducing fiducial migration [50]. The authors found that traditional fiducials had improved visualization compared to coiled fiducials, with no difference in fiducial migration or complications of placement. Traditional, linear fiducials remain the preferred choice for pancreas SBRT at this time.
Patients receiving SBRT for pancreatic cancer should be simulated using a CT scan (3 mm slices) with intravenous and oral contrast (240 cc) to highlight the tumor and standardize gastric filling (give 240 cc of water) during treatment. Many centers utilize positron emission tomography/computed tomography (PET/CT) scans to help identify the lesions as well as monitor for treatment response [51, 52].
As with any site in Radiation Oncology , appropriate immobilization at the time of simulation is paramount in importance. Given the proximity of the pancreas to the diaphragm, tumor motion is common and expected. As previously mentioned, multiple investigators have published their findings on tumor motion and appropriate margins for the use of SBRT in localized pancreatic cancer [53–58]. Table 8.7 lists the movement of pancreas tumors in different planes during the respiratory cycle. This data supports that pancreatic motion is a concern during radiation treatment and should be considered when planning these patients.
Tumor motion is often the greatest in the superior-inferior plane or the anterior-posterior plane, demonstrating the need for careful assessment of this factor at the time of treatment planning. To help stabilize the tumor, some centers utilize abdominal compression in which a device is applied to the abdomen to provide direct anterior pressure, thereby limiting breathing induced abdominal motion. Heinzerling’s data supports that this is an adequate method to help reduce tumor motion, thereby increasing reproducibility [55]. Other centers prefer a “breath-hold” technique using active breathing control in which the patient is instructed to pause their respiration at either full inspiration or expiration during which the treatment is delivered [39]. Again, no consensus exists as to whether treatment at full inspiration or expiration is optimal, though a small study (18 patients) from Taniguchi recommends treating patients at full expiration to minimize duodenal toxicity [59]. No data exists to specify which immobilization method is optimal and largely becomes a choice of the treating physician and institution. Lastly, in regard to tumor motion, daily imaging during treatment is a requirement. This can be accomplished using a cone-beam CT scan at the time of treatment, orthogonal kilovoltage (kV) imaging, and/or real-time tumor tracking.
The appropriate dose of radiation in pancreas SBRT is also the subject of significant debate. As noted in Table 8.5, the dose and fractionation has varied from 25 Gy in one fraction to 5 Gy in five fractions. Brunner et al. has completed a review of published data on patients treated with pancreatic SBRT from 2000 to 2013 [60]. By assessing the BED10 Gy and BED3 Gy, as well as the BED in 2 Gy fractions (EQD2), the authors of this review attempted to estimate the therapeutic window for tumor response and normal tissue complications from different radiation dose regimens. Their results demonstrated that a weak correlation was found between EQD2-α/β10 and BED-α/β10 (tumor control), but a much stronger correlation was found for EQD2-α/β3 and BED-α/β3 (normal tissue toxicity). A 5 and 10 % rate of late grade ≥2 toxicity was seen at EQD2-α/β3 doses of 66 and 100 Gy, respectively. This data is important for helping to determine the optimal dose to avoid long-term complications in these patients, but needs to be further refined. Regardless of the dose that is chosen for treatment, the physician should utilize published dose constraints from institutions utilizing a similar dosing regimen. For reference, dose constraints to surrounding OARs from the recently published multi-institutional trial using 33 Gy in five fractions are presented in Table 8.8 [40]. An SBRT treatment plan can be found in Fig. 8.4.

Example of a pancreas SBRT treatment plan. Patient was treated to 33 Gy in 5 fractions (6.6 Gy per fraction). Note that each color represents the isodose distribution of prescription dose. Beyond the isocenter, rapid dose falloff is achieved in order to minimize exposure to surrounding organs at risk such as the stomach and small bowel
Finally, it is important to support patients during and after SBRT. Due to the proximity of the lesions to sensitive gastrointestinal mucosa, prophylactic use of anti-nausea medication is important. The authors of this chapter recommend using ondansetron, with a minimum dose of 8 mg at least 1 h prior to therapy. Likewise, gastrointestinal reflux can be frustrating for patients after treatment, and the use of proton pump inhibitors or H2-antagonists may also help ameliorate this side effect. These medications may also be prescribed as a prophylactic measure to decrease the risk of developing stomach and/or bowel ulceration. The authors recommend taking a proton pump inhibitor daily during, and ideally 6 months following, the administration of SBRT. Furthermore, pancreatic enzymes are recommended to aid in digestion and absorption of nutrients and reduce the frequency and/or severity of digestive symptoms such as gas, bloating, and loose, oily stools.
Conclusion
The optimal treatment for patients with BRPC and LAPC remains an area of active investigation [61, 62]. Traditional chemotherapy and CRT remains only partially effective in treating this disease and is, at best, a temporizing measure for disease progression. Without the ability to significantly downstage these patients and render their disease resectable, the ability to cure these patients is unlikely. SBRT has demonstrated significantly improved rates of local tumor control, tumor down-staging, treatment response, and resectability rates. While more prospective, randomized data is necessary to officially compare SBRT with standard CRT, the current results with SBRT appear favorable and should be pursued in future clinical trials. Additionally, by reducing the amount of time these patients spend undergoing radiation, the delay in time to the delivery of full-dose chemotherapy is reduced, and the opportunity for both local and distant control is improved. Though the published results of this treatment are still early, they provide a measure of guarded optimism to radiation oncologists treating an otherwise uniformly lethal disease.
References
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29.
Tempero MA, Malafa MP, Behrman SW, Benson III AB, Casper ES, Chiorean EG, et al. Pancreatic adenocarcinoma, version 2.2014: featured updates to the NCCN guidelines. J Natl Compr Canc Netw. 2014;12(8):1083–93.
Hammel P, Huguet F, Van Laethem J-L, Goldstein D, Glimelius B, Artru P, et al. Comparison of chemoradiotherapy (CRT) and chemotherapy (CT) in patients with a locally advanced pancreatic cancer (LAPC) controlled after 4 months of gemcitabine with or without erlotinib: final results of the international phase III LAP 07 study. ASCO Meeting Abstr. 2013;31(18 Suppl):LBA4003.
Loehrer Sr PJ, Feng Y, Cardenes H, Wagner L, Brell JM, Cella D, et al. Gemcitabine alone versus gemcitabine plus radiotherapy in patients with locally advanced pancreatic cancer: an Eastern Cooperative Oncology Group trial. J Clin Oncol. 2011;29(31):4105–12.
Chauffert B, Mornex F, Bonnetain F, Rougier P, Mariette C, Bouche O, et al. Phase III trial comparing intensive induction chemoradiotherapy (60 Gy, infusional 5-FU and intermittent cisplatin) followed by maintenance gemcitabine with gemcitabine alone for locally advanced unresectable pancreatic cancer. Definitive results of the 2000-01 FFCD/SFRO study. Ann Oncol. 2008;19(9):1592–9.
Timmerman RD, Herman J, Cho LC. Emergence of stereotactic body radiation therapy and its impact on current and future clinical practice. J Clin Oncol. 2014;32(26):2847–54.
Hall EJ, Giaccia AJ. Radiobiology for the radiologist. 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2006. p. ix, 546.
Callery MP, Chang KJ, Fishman EK, Talamonti MS, William Traverso L, Linehan DC. Pretreatment assessment of resectable and borderline resectable pancreatic cancer: expert consensus statement. Ann Surg Oncol. 2009;16(7):1727–33.
Katz MH, Marsh R, Herman JM, Shi Q, Collison E, Venook AP, et al. Borderline resectable pancreatic cancer: need for standardization and methods for optimal clinical trial design. Ann Surg Oncol. 2013;20(8):2787–95.
Winter JM, Cameron JL, Campbell KA, Arnold MA, Chang DC, Coleman J, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: a single-institution experience. J Gastrointest Surg. 2006;10(9):1199–210; discussion 210–1.
Fatima J, Schnelldorfer T, Barton J, Wood CM, Wiste HJ, Smyrk TC, et al. Pancreatoduodenectomy for ductal adenocarcinoma: implications of positive margin on survival. Arch Surg. 2010;145(2):167–72.
Katz MH, Pisters PW, Evans DB, Sun CC, Lee JE, Fleming JB, et al. Borderline resectable pancreatic cancer: the importance of this emerging stage of disease. J Am Coll Surg. 2008;206(5):833–46; discussion 46–8.
Moertel CG, Frytak S, Hahn RG, O’Connell MJ, Reitemeier RJ, Rubin J, et al. Therapy of locally unresectable pancreatic carcinoma: a randomized comparison of high dose (6000 rads) radiation alone, moderate dose radiation (4000 rads + 5-fluorouracil), and high dose radiation + 5-fluorouracil: the Gastrointestinal Tumor Study Group. Cancer. 1981; 48(8):1705–10.
Treatment of locally unresectable carcinoma of the pancreas: comparison of combined-modality therapy (chemotherapy plus radiotherapy) to chemotherapy alone. Gastrointestinal Tumor Study Group. J Natl Cancer Inst. 1988;80(10):751–5.
Klaassen DJ, MacIntyre JM, Catton GE, Engstrom PF, Moertel CG. Treatment of locally unresectable cancer of the stomach and pancreas: a randomized comparison of 5-fluorouracil alone with radiation plus concurrent and maintenance 5-fluorouracil—an Eastern Cooperative Oncology Group study. J Clin Oncol. 1985;3(3):373–8.
Huguet F, Andre T, Hammel P, Artru P, Balosso J, Selle F, et al. Impact of chemoradiotherapy after disease control with chemotherapy in locally advanced pancreatic adenocarcinoma in GERCOR phase II and III studies. J Clin Oncol. 2007;25(3):326–31.
Krishnan S, Rana V, Janjan NA, Varadhachary GR, Abbruzzese JL, Das P, et al. Induction chemotherapy selects patients with locally advanced, unresectable pancreatic cancer for optimal benefit from consolidative chemoradiation therapy. Cancer. 2007;110(1):47–55.
Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364(19):1817–25.
Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369(18):1691–703.
Marsh RW, Talamonti MS, Katz MH, Herman JM. Pancreatic cancer and FOLFIRINOX: a new era and new questions. Cancer Med. 2015;4(6):853–63.
Fletcher GH. Hypofractionation: lessons from complications. Radiother Oncol. 1991;20(1):10–5.
Rosenthal DI, Glatstein E. We’ve got a treatment, but what’s the disease? Or a brief history of hypofractionation and its relationship to stereotactic radiosurgery. Oncologist. 1996;1(1 & 2):1–7.
Leksell L. Stereotactic radiosurgery. J Neurol Neurosurg Psychiatry. 1983;46(9):797–803.
Timmerman R, Papiez L, McGarry R, Likes L, DesRosiers C, Frost S, et al. Extracranial stereotactic radioablation: results of a phase I study in medically inoperable stage I non-small cell lung cancer. Chest. 2003;124(5):1946–55.
Davis JN, Medbery III C, Sharma S, Danish A, Mahadevan A. The RSSearch Registry: patterns of care and outcomes research on patients treated with stereotactic radiosurgery and stereotactic body radiotherapy. Radiat Oncol. 2013;8:275.
Koong AC, Le QT, Ho A, Fong B, Fisher G, Cho C, et al. Phase I study of stereotactic radiosurgery in patients with locally advanced pancreatic cancer. Int J Radiat Oncol Biol Phys. 2004;58(4):1017–21.
Hoyer M, Roed H, Sengelov L, Traberg A, Ohlhuis L, Pedersen J, et al. Phase-II study on stereotactic radiotherapy of locally advanced pancreatic carcinoma. Radiother Oncol. 2005;76(1):48–53.
Koong AC, Christofferson E, Le QT, Goodman KA, Ho A, Kuo T, et al. Phase II study to assess the efficacy of conventionally fractionated radiotherapy followed by a stereotactic radiosurgery boost in patients with locally advanced pancreatic cancer. Int J Radiat Oncol Biol Phys. 2005;63(2):320–3.
Chang DT, Schellenberg D, Shen J, Kim J, Goodman KA, Fisher GA, et al. Stereotactic radiotherapy for unresectable adenocarcinoma of the pancreas. Cancer. 2009;115(3):665–72.
Polistina F, Costantin G, Casamassima F, Francescon P, Guglielmi R, Panizzoni G, et al. Unresectable locally advanced pancreatic cancer: a multimodal treatment using neoadjuvant chemoradiotherapy (gemcitabine plus stereotactic radiosurgery) and subsequent surgical exploration. Ann Surg Oncol. 2010;17(8):2092–101.
Schellenberg D, Kim J, Christman-Skieller C, Chun CL, Columbo LA, Ford JM, et al. Single-fraction stereotactic body radiation therapy and sequential gemcitabine for the treatment of locally advanced pancreatic cancer. Int J Radiat Oncol Biol Phys. 2011;81(1):181–8.
Mahadevan A, Jain S, Goldstein M, Miksad R, Pleskow D, Sawhney M, et al. Stereotactic body radiotherapy and gemcitabine for locally advanced pancreatic cancer. Int J Radiat Oncol Biol Phys. 2010;78(3):735–42.
Mahadevan A, Miksad R, Goldstein M, Sullivan R, Bullock A, Buchbinder E, et al. Induction gemcitabine and stereotactic body radiotherapy for locally advanced nonmetastatic pancreas cancer. Int J Radiat Oncol Biol Phys. 2011;81(4):e615–22.
Chuong MD, Springett GM, Freilich JM, Park CK, Weber JM, Mellon EA, et al. Stereotactic body radiation therapy for locally advanced and borderline resectable pancreatic cancer is effective and well tolerated. Int J Radiat Oncol Biol Phys. 2013;86(3):516–22.
Tozzi A, Comito T, Alongi F, Navarria P, Iftode C, Mancosu P, et al. SBRT in unresectable advanced pancreatic cancer: preliminary results of a mono-institutional experience. Radiat Oncol. 2013;8:148.
Kim CH, Ling DC, Wegner RE, Flickinger JC, Heron DE, Zeh H, et al. Stereotactic body radiotherapy in the treatment of pancreatic adenocarcinoma in elderly patients. Radiat Oncol. 2013;8:240.
Rajagopalan MS, Heron DE, Wegner RE, Zeh HJ, Bahary N, Krasinskas AM, et al. Pathologic response with neoadjuvant chemotherapy and stereotactic body radiotherapy for borderline resectable and locally-advanced pancreatic cancer. Radiat Oncol. 2013;8:254.
Gurka MK, Kim C, He AR, Charabaty A, Haddad N, Turocy J, et al. Stereotactic body radiation therapy (SBRT) combined with chemotherapy for unresected pancreatic adenocarcinoma. Am J Clin Oncol. 2014 Aug 28. [Epub ahead of print] PMID: 25171298.
Moningi S, Dholakia AS, Raman SP, Blackford A, Cameron JL, Le DT, et al. The role of stereotactic body radiation therapy for pancreatic cancer: a single-institution experience. Ann Surg Oncol. 2015;22(7):2352–8.
Herman JM, Chang DT, Goodman KA, Dholakia AS, Raman SP, Hacker-Prietz A, et al. Phase 2 multi-institutional trial evaluating gemcitabine and stereotactic body radiotherapy for patients with locally advanced unresectable pancreatic adenocarcinoma. Cancer. 2015;121(7):1128–37.
Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. 2004;350(12):1200–10.
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365–76.
Groenvold M, Klee MC, Sprangers MA, Aaronson NK. Validation of the EORTC QLQ-C30 quality of life questionnaire through combined qualitative and quantitative assessment of patient-observer agreement. J Clin Epidemiol. 1997;50(4):441–50.
Serrano PE, Herman JM, Griffith KA, Zalupski MM, Kim EJ, Bekaii-Saab TS, et al. Quality of life in a prospective, multicenter phase 2 trial of neoadjuvant full-dose gemcitabine, oxaliplatin, and radiation in patients with resectable or borderline resectable pancreatic adenocarcinoma. Int J Radiat Oncol Biol Phys. 2014;90(2):270–7.
Short M, Goldstein D, Halkett G, Reece W, Borg M, Zissiadis Y, et al. Impact of gemcitabine chemotherapy and 3-dimensional conformal radiation therapy/5-fluorouracil on quality of life of patients managed for pancreatic cancer. Int J Radiat Oncol Biol Phys. 2013;85(1):157–62.
Heras P, Kritikos K, Hatzopoulos A, Kritikos N, Karagiannis S, Mitsibounas D. Effect of combined treatment methods on quality of life in patients with pancreatic cancer. Am J Ther. 2009;16(4):316–8.
Kleeff J, Reiser C, Hinz U, Bachmann J, Debus J, Jaeger D, et al. Surgery for recurrent pancreatic ductal adenocarcinoma. Ann Surg. 2007;245(4):566–72.
Lominska CE, Unger K, Nasr NM, Haddad N, Gagnon G. Stereotactic body radiation therapy for reirradiation of localized adenocarcinoma of the pancreas. Radiat Oncol. 2012;7:74.
Wild AT, Hiniker SM, Chang DT, Tran PT, Khashab MA, Limaye MR, et al. Re-irradiation with stereotactic body radiation therapy as a novel treatment option for isolated local recurrence of pancreatic cancer after multimodality therapy: experience from two institutions. J Gastrointest Oncol. 2013;4(4):343–51.
Khashab MA, Kim KJ, Tryggestad EJ, Wild AT, Roland T, Singh VK, et al. Comparative analysis of traditional and coiled fiducials implanted during EUS for pancreatic cancer patients receiving stereotactic body radiation therapy. Gastrointest Endosc. 2012;76(5):962–71.
Schellenberg D, Quon A, Minn AY, Graves EE, Kunz P, Ford JM, et al. 18Fluorodeoxyglucose PET is prognostic of progression-free and overall survival in locally advanced pancreas cancer treated with stereotactic radiotherapy. Int J Radiat Oncol Biol Phys. 2010;77(5):1420–5.
Dholakia AS, Chaudhry M, Leal JP, Chang DT, Raman SP, Hacker-Prietz A, et al. Baseline metabolic tumor volume and total lesion glycolysis are associated with survival outcomes in patients with locally advanced pancreatic cancer receiving stereotactic body radiation therapy. Int J Radiat Oncol Biol Phys. 2014;89(3):539–46.
Minn AY, Schellenberg D, Maxim P, Suh Y, McKenna S, Cox B, et al. Pancreatic tumor motion on a single planning 4D-CT does not correlate with intrafraction tumor motion during treatment. Am J Clin Oncol. 2009;32(4):364–8.
Song YC, You JQ, Yuan ZY, Wang W, Li XY, Wang P. A preliminary probe into the movement of pancreatic lesions and factors that influence it. Br J Radiol. 2010;83(990):505–8.
Heinzerling JH, Bland R, Mansour JC, Schwarz RE, Ramirez E, Ding C, et al. Dosimetric and motion analysis of margin-intensive therapy by stereotactic ablative radiotherapy for resectable pancreatic cancer. Radiat Oncol. 2011;6:146.
Knybel L, Cvek J, Otahal B, Jonszta T, Molenda L, Czerny D, et al. The analysis of respiration-induced pancreatic tumor motion based on reference measurement. Radiat Oncol. 2014;9:192.
Yang W, Fraass BA, Reznik R, Nissen N, Lo S, Jamil LH, et al. Adequacy of inhale/exhale breathhold CT based ITV margins and image-guided registration for free-breathing pancreas and liver SBRT. Radiat Oncol. 2014;9:11.
Goldstein SD, Ford EC, Duhon M, McNutt T, Wong J, Herman JM. Use of respiratory-correlated four-dimensional computed tomography to determine acceptable treatment margins for locally advanced pancreatic adenocarcinoma. Int J Radiat Oncol Biol Phys. 2010;76(2):597–602.
Taniguchi CM, Murphy JD, Eclov N, Atwood TF, Kielar KN, Christman-Skieller C, et al. Dosimetric analysis of organs at risk during expiratory gating in stereotactic body radiation therapy for pancreatic cancer. Int J Radiat Oncol Biol Phys. 2013;85(4):1090–5.
Brunner TB, Nestle U, Grosu AL, Partridge M. SBRT in pancreatic cancer: what is the therapeutic window? Radiother Oncol. 2015;114:109–16.
Wolfgang CL, Herman JM, Laheru DA, Klein AP, Erdek MA, Fishman EK, et al. Recent progress in pancreatic cancer. CA Cancer J Clin. 2013;63(5):318–48.
Moningi S, Marciscano AE, Rosati LM, Ng SK, Teboh Forbang R, Jackson J, et al. Stereotactic body radiation therapy in pancreatic cancer: the new frontier. Expert Rev Anticancer Ther. 2014;14(12):1461–75.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Kumar, R., Rosati, L.M., Herman, J.M. (2016). Stereotactic Body Radiation Therapy as an Emerging Option for Localized Pancreatic Cancer. In: Katz, M., Ahmad, S. (eds) Multimodality Management of Borderline Resectable Pancreatic Cancer. Springer, Cham. https://doi.org/10.1007/978-3-319-22780-1_8
Download citation
DOI: https://doi.org/10.1007/978-3-319-22780-1_8
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-22779-5
Online ISBN: 978-3-319-22780-1
eBook Packages: MedicineMedicine (R0)