
Abstract
Interventional ultrasound is increasing in popularity over the past decade as ultrasound technology has significantly improved. Many articles have come out about the use of ultrasound in diagnosis and therapeutic drainage of fluid collections throughout the body. In this chapter, we describe the various locations for collection of fluid, along with an approach to drainage, and avoiding potential pitfalls and preventing complications. We highlight patient preparation and technical considerations for each type of collection.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
There are many different types of collections of fluid (e.g., those in a cavity, those after surgery, those that are congenital); the approach to diagnosis or therapy may be different based on the type and location. Being able to categorize fluid collections by type and location in the body is the first step. These fluid collections can occur at any part of the body and knowing your anatomy is a key way to avoid any complications.
The next step is preparation which leads to a series of questions: Do I have all the equipment, does this need to be sterile, does the primary team managing the patient want the fluid sent for special things including cultures, is this a recurrence, do we need to perform a sclerosis, is this in conjunction with a biopsy, is ultrasound the correct image guidance modality for this instance. Knowing the history and doing a thorough physical checkup is still important prior to picking up the ultrasound. A patient with allergies, having severe anxiety to the procedure, or just after a meal, could seriously hinder the ability to perform an ultrasound. As interventional ultrasound is an adjunct to clinical care—the provider caring for the patient and the person performing the ultrasound-guided procedure may be different—leading to a fragmentation in care that could lead to communication issues.
Finally, technical considerations, such as having more than one ultrasound probe, are essential. The diagnostic and therapeutic probes used for ultrasound do not have to be the same. For example, identifying the collection may be better with a curved probe, but following the needle into the cavity may be better with a linear probe. Furthermore, having a range of drainage catheters, guidewires, and dilators is crucial to the success of a drainage procedure. Moreover, the path to the collection does not have to be directly percutaneous and may need to traverse an organ. For example, accessing the gallbladder through the liver parenchyma or a pelvic collection through a transrectal approach often is superior to other options. Finally, having the ability to inject the collection with contrast and monitoring this using fluoroscopy should not be underestimated.
In this chapter, we focus on general principles as briefly outlined above, then focus on a transrectal approach to drainage, after which we discuss special circumstances where there is literature to support a specific strategy. For example with ascites, make sure to have albumin available or know if the patient has significant liver disease; or with a pleural effusion, use of tissue plasminogen activator (TPA) to prevent a recurrence versus needing to send samples to rule out malignancy.
General Principles
Fluid collections can be differentiated into various types based on history and anatomic location. Categorizing them based on history and location helps with management by using a diagnostic or therapeutic algorithm. The following is an example of various ways a collection can be categorized:
-
1.
Collections in general: unknown, malignant, infectious, lymphatic
-
2.
Abscesses: postoperative, chest, mediastinal, abdominal, pelvic
-
3.
Gastrointestinal (GI): pancreatic, splenic, foregut/duplication, chronic cholecystitis, hydatid cyst
-
4.
Urologic: hydronephrosis, suprapubic catheter placement
Prior to drainage of a collection, the indications must be reviewed, coagulopathy must be excluded or treated, and the appropriate imaging modality must be chosen [1]. The diagnostic approach to fluid collections starts with a good history and location of the lesion. If the patient has a history of malignancy or risk factors that increase the risk for a malignancy, the identification of a collection, such as a pleural effusion, can be a marker of the malignancy. Furthermore, qualities of a collection, such as the percentage of solid material, can differentiate a cystic collection. Knowing the likelihood of a malignancy is important in the approach to drainage of a collection as the tract used to sample the fluid can be a potential pathway for the spread of the disease.
Similarly, the sampling of the collection can be diagnostic, therapeutic, or both. Therefore, having a general framework to approach the fluid is useful to prevent additional procedures or anesthetics. As there is always a risk in the aspiration of a collection, combining procedures into one setting can mitigate further risks. For example, injection of a sclerosant into the cavity during drainage of a lymphatic collection prevents recurrence of the collection and, concomitantly, an additional procedure.
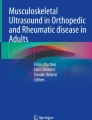
Drainage of a fluid collection should only be performed when there is [2]: a suspicion of infection, a need for fluid characterization, or symptoms that warrant drainage. “The basic indication for needle aspiration is to confirm the radiological diagnosis of an abscess because the radiological signs may not distinguish amongst various types of fluid collection including abscess, hematoma, urinoma, biloma, lymphocele, seroma, and loculated ascites . The main indications for catheter drainage include treatment or palliation of sepsis associated with an infected fluid collection, and alleviation of the symptoms that may be caused by fluid collections by virtue of their size, like pancreatic pseudocele or lymphocele” [1]. Figure 21.1 demonstrates needle entry into a fluid collection of unknown etiology for diagnostic purposes.

Figure represents needle entry into a collection of unknown etiology using a curved probe for guidance
Informed consent following a thorough discussion with the patient is mandatory for any invasive procedure. Rarely are the procedures emergent and the expectations of the patients and primary-care providers need to be assessed prior to performing the procedure. Identification of the indications, approach to drainage, choosing the appropriate imaging modality, specific diagnostic tests on the drainage, and therapeutic options should all be discussed at this time.
In diagnostic or therapeutic drainage, the steps are fairly simple though difficult to execute without sufficient practice. The collection is identified using an ultrasound probe (as mentioned earlier, the probe used to initially find the collection and that used for targeting drainage may be different). Using ultrasound guidance, the collection is approached using an 18- or 22-gauge entry needle based on the depth and size of the fluid. Advancing the needle in line with the ultrasound transducer provides excellent visualization of the entire needle and the target collection simultaneously. This improves safety and maneuverability in advancing the needle. If purulent fluid is aspirated, it is sent for culture; of note, immunocompromised patients may have bacteria or fungal collections without evidence of an immune response. Keep in mind that a Gram stain may fail to grow any organisms if the patient has already received antimicrobial therapy. Furthermore, use of a needle without the syringe attached can be a useful technique to facilitate guiding the needle into the cavity without the added weight of the syringe. The syringe can be attached once entry into the cavity can be confirmed by imaging. Based on the thickness of the fluid, the needle may need to be “upsized” prior to drainage of the contents.
To “upsize” the needle, a guidewire can be inserted with serial dilation over the guidewire using a Seldinger technique. A 0.010- or 0.018-in. wire can be placed through the 22-gauge needle whereas a 0.035 guidewire can be inserted through an 18-gauge entry needle. When using larger dilators, we routinely exchange a thinner guidewire to a larger diameter and stiffer wire to provide a stiff backbone for the dilator to travel over preventing dislodgment and errant passage of the dilator. Furthermore, the needle and guidewire exchange is easier to accomplish with the cavity filled with fluid as there is more resistance on the wall to prevent dislodgement as well as prevent inadvertent entry through the opposite wall. If the fluid within a cavity has already been evacuated for diagnosis, irrigation with saline can be used to refill the area and help with the needle and guidewire exchange. Once a drainage cathether has been inserted into the cavity, we routinely use ultrasound to confirm adequate drainage of the cavity and assess for additional located collections that were not initially noted or were inadequately drained. Although, the largest possible drainage catheter is generally used, there is no difference in recurrence, drainage time, and complications [3]. Figure 21.2 demonstrates evacuation of a loculated abscess by breaking up septations using the needle and placement of a pigtail for irrigation and drainage.

a Figure represents needle entry into a loculated abscess cavity with multiple septations. b Figure represents needle connecting multiple loculated collections by breaking up the septations under visualization. c Figure represents abscess cavity being drained by the pigtail catheter that is now in place. The abscess is irrigated with saline and collapsed down at the end of the procedure
The management of a drain when placed should be standard for each institution. Drains can be placed to bulb or gravity drainage based on the expected quality and quantity of output. They should be ideally flushed with saline daily and removed in about 1–3 days when the output is less than 10 ml/day or 5 ml/day in infants [2]. While a drain is in place, antibiotics should be considered if there is a risk of translocation based on host factors, if there is adjacent foreign material such as an implant, or if the output is presumptively infectious.
Ultrasound has become the imaging modality of choice for many interventions with the advent of high-resolution, wide-angle probes. Ultrasound also offers the unique advantages of portability, immediate availability, and flexibility, owing in part to the wide range of transducers now available. Ultrasound probes have been specifically designed to guide the biopsy of small lesions, allow precise control of biopsy instruments, and provide direct, real-time visualization of successful target lesion biopsies. Moreover, ultrasound avoids ionizing radiation—an important concern especially when imaging the organs of the pelvis, namely the gonads [4].
Transrectal Drainage
A transrectal approach can be used for drainage of an abscess or fluid collection in the pelvis. As the bowel can obscure the collection and prevent a transabdominal approach to the collection, a transrectal access can be more direct. Also, this approach may be less painful than transgluteal as it does not traverse any muscles. A transgluteal approach requires the catheter to be placed close to the sacrum/coccyx to avoid injury to the sciatic nerve and gluteal vessels; this approach can cause pelvic and leg pain if it passes through the piriformis muscle or near the sacral plexus [4]. Securing the catheter using the transrectal approach may be more difficult though, therefore, a pigtail is recommended. Figure 21.3 demonstrates the use of real-time ultrasound to access a pelvic abscess using the transrectal approach.

Figure represents needle entry into a pelvic abscess using a transrectal approach. The needle enters the cavity under direct visualization. The probe (curved) was placed in a longitudinal orientation on the abdominal wall visualizing the bladder and rectum while accessing the abscess cavity
One study recommends having all patients who are having transrectal or transvaginal drainage of an abscess be started on antibiotics at least 2 h in advance to achieve adequate systemic levels [5]. A bowel preparation is considered unnecessary for transrectal drainage; however a gentle enema—if not contraindicated—using saline or Fleet’s may help clear out remnant stool, making the procedure easier and cleaner to perform.
For teenagers, a transrectal probe with guide can be used since their anal sphincter complex can accommodate the probe without damage. However, in both older and younger children, a curved transducer in a sagittal orientation placed just above the pubic bone can provide excellent transabdominal guidance for transrectal abscess drainage. In this method the bladder acts as an acoustic window so that catheterizing the bladder to fill with saline augments visualization [5]. Leaving a pigtail catheter in the abscess is preferred to solely draining an abscess when transrectal approach is used. Furthermore, daily irrigation should be performed approximately every 8 h with 5–10 mL of sterile saline to flush both the abscess cavity and the associated tubing [4].
Transrectal techniques are also used in assessment of male infertility, hemospermia, and azospermia. Seminal vesicle, ejaculatory duct, and midline cysts can be aspirated under transrectal ultrasound guidance and analyzed for semen and sperm motility. Aspiration of ejaculatory duct cysts may improve obstructive azospermia and improve paternity rates [4].
Furthermore, the transrectal technique is a safe, adequate, and effective treatment for prostate abscess [6].
The rest of the chapter focuses on diagnostic and therapeutic approaches that should be considered for various anatomic locations.
Head and Neck
Drainage of a fluid collection in the head and neck region can be required for an infection with subsequent abscess formation, hemorrhage into an existing cyst, or a postoperative complication [7]. As the oral cavity is closely intertwined with head and neck anatomy, several sources of bacterial translocation can occur. As these anaerobic organisms spread, they can lead to a retropharyngeal abscess or those that track anteriorly into the mediastinum. Early drainage can identify these organisms and allow for aggressive treatment, preventing later complications [8].
Peritonsillar cellulitis and abscess can present similarly with edema, trismus, and erythema [9]. Usage of ultrasound improves the diagnostic accuracy and ability to drain the collection. As the carotid artery can be near the posterior extent of the abscess, an ultrasound can be used to guide the needle while limiting the potential injury to adjacent structures. In one study, ultrasound was used to diagnose and drain the collection in the emergency room, facilitating an earlier discharge home without complications [10].
Cysts in the head and neck region can be fairly common, arising from the thyroid origin as a thyroglossal duct cyst—a dermoid cyst confined to the superficial tissues or laterally as branchial cleft cysts. These cysts ultimately may require surgical excision; however, infection or hemorrhage can occur at initial presentation or postoperatively requiring ultrasound-guided drainage for management. The most important concepts to consider in the head and neck region include: (1) the use of anatomic landmarks and identification of important vascular and air-filled structures that course over a small area and (2) weighing the risks of drainage for diagnostic purposes versus an earlier more aggressive surgical approach for therapy. Alternatively, use of sclerotherapy after drainage of cysts in the thyroid, parathyroid, and salivary glands has been shown to be successful to prevent recurrence [11]. Figure 21.4 demonstrates entry into a thyroid cyst for diagnostic sampling.

Figure represents needle entry into a cyst in the thyroid. Note the adjacent vascular structures and how well they can be visualized and avoided using ultrasound
Chest
Pleural effusions or fluid collections in the chest can occur for a variety of reasons—infectious, malignant, lymphatic, or idiopathic. Classically, drainage of the fluid has been used for diagnosis—classifying effusions as transudative versus exudative. The Light criteria can be used to define the type of effusion [12]: pH < 7.2, lactate dehydrogenase > 1000 U, glucose < 40 mg/dL, or < 25 % blood glucose, Gram stain, or culture positive and with loculations or septations proven with imaging indicating an exudative or complex collection. In future studies, an exudative effusion was most definitively confirmed with a low pH [13−15]. Figure 21.5 demonstrates the use of ultrasound to drain a pleural fluid collection.

Figure represents needle entry into the pleural cavity using a linear probe. Note the image quality below each rib causing a shadow to appear. The needle usually “disappears” in this shadow and reappears on the other side. The lung is collapsed and therefore seen better than usual when fully filled with air
Parapneumonic effusions occur during or after a bout of bacterial pneumonia, with translocation of the bacteria into the pleural space from the interstitial. The fluid starts as clear with some mild particulate matter, thickening over time, until it reaches a fibrotic nature, compromising the lung volume by trapping the lung in various areas (Fig. 21.6a and b). Drainage of the fluid alone has been used for treatment, but has a high recurrence rate. Surgical approaches with or without using minimally invasive techniques have been advocated to decorticate the fibrotic bands and release trapped lung; however, this carries morbidity of the surgery and an increase in cost. Alternatively, drainage with insertion of a lytic agent has been proposed to decrease the recurrence rate without the morbidity or cost associated with surgery [16]. Placement of the drainage catheter can be performed using an ultrasound to target the area of fluid more precisely.

a and b The pictures show possible sonographic findings in the setting of an advanced parapneumonic pleural effusion or empyema . Treatment options include ultrasound-guided placement of pigtail chest tube with TPA(tissue plasminogen activator) applications or VATS (video-assisted thoracoscopic surgery) with decortication
On patients on a ventilator, drainage of simple or complex pleural effusions in mechanically ventilated patients appears to improve oxygenation and is safe [17]. A pleural effusion was detected in critically ill patients in 60 % of patients in one intensive care unit (ICU) with over 40 % present on admission [18]. These effusions can be the result of heart failure, atelectasis, malignancy, pneumonia, hypoalbuminemia, and even positive-pressure ventilation [18, 19]. In any patient where drainage of an effusion is considered, there is a risk of an iatrogenic pneumothorax with intervention. Therefore, the use of an ultrasound should be considered mandatory for the drainage of pleural effusions in this population of patients that has minimal reserve at baseline.
Malignant pleural effusions affect more than 175,000 people each year in the USA, with lung cancer contributing to 30 % of the cases [20]. Thoracentesis or drainage of the pleural fluid can be used for diagnostic and therapeutic purposes when a malignant effusion is suspected. Unfortunately, nearly a third of these procedures may be associated with a complication when performed without an ultrasound, with a third of these complications being a pneumothorax [21]. In contrast, an ultrasound-guided thoracentesis, especially when performed by an experienced operator, can have a less than 3 % rate of any of the following complications: pain, pneumothorax, bleeding or hematoma, shortness of breath, or re-expansion pulmonary edema [22].
Accumulation of fluid in the pericardial sac can cause cardiac compression and tamponade from elevated pressure. Classically, Beck’s triad of low blood pressure, distended neck veins (jugular venous distension), and muffled heart sounds represents cardiac tamponade. In reality however, the right ventricle and atrium have thinner walls and decreased pressures, therefore they collapse first and findings of low systemic blood pressure or cardiac output can be a late presentation. Furthermore, the rate and volume of fluid accumulation vary and determine the timing of hemodynamic compromise.
Ultrasound can be used to diagnose and drain a pericardial effusion in a timely manner with decreased risk. The following is an approach to diagnosis of tamponade adapted from Chandraratna et al. [23]: (1) Rarely is isolated right atrial collapse seen without right ventricular diastolic collapse (RVDC), (2) RVDC, best observed in the most compressible part—the right ventricle outflow tract—is a sensitive sign of cardiac tamponade because the right ventricular (RV) pressure is lowest in early diastole, (3) RVDC, occurs initially in early diastole and in more advanced tamponade, is seen throughout diastole, and (4) A dilated non-pulsatile inferior vena cava, nonspecific for tamponade, indicates marked elevation of right atrial (RA) pressure.
To drain the fluid, a subxiphoid or apical approach can be used. For the subxiphoid approach, the ultrasound probe is placed at the cardiac apex to obtain an apical four-chamber view; while for the apical approach, the transducer is placed at the left sternal border for monitoring. For a subxiphoid approach, a long needle is inserted under the xiphoid process and directed toward the left shoulder at a 15–30° angle to the skin between the xiphoid and left costal margin [23]. For the apical approach, an 18-gauge needle with a syringe, under constant negative pressure and attached to a 3-way stopcock, is passed through the rib space until fluid is aspirated [23]. Complications for either include “arrhythmias, coronary or left internal mammary artery puncture, hemothorax, pneumothorax, and hepatic injury” [23].
Ultrasound-guided interventions in the chest are limited by the bony ribs, spine and sternum exteriorly and the air-filled trachea, esophagus, and lungs interiorly but adequate windows can be gotten with sufficient practice and the use of acoustic windows from the neck, through the liver, or into the mediastinum and pleura between the ribs. These can be used to guide diagnostic and therapeutic procedures in the setting of bedside procedures or those requiring real-time visualization. In many instances, cross-sectional imaging may provide adequate diagnostic detail, curtailing the need for ultrasound and these should be considered based on the patient and procedure risk profiles.
Abdomen and Pelvis
Abdominal and pelvic abscesses may occur from solid organs such as spleen, kidney, or pancreas, or an enteric source such as those from post-surgery, appendicitis, diverticulitis, or Crohn’s disease24. Percutaneous drainage could potentially eliminate the need for surgical drainage altogether–whether the abscess is simple or complex and multiloculated. Approach to drainage can be through the abdominal wall, transgastric, transrectal, transvaginal, transperineal, or transgluteal [24]. Occasionally, a catheter cannot be placed and only a drainage with sampling of the fluid is performed, especially if the abscess is not large or loculated [25].
In children, the most common cause of abdominal abscess is appendicitis [2]. Other common etiologies for intra-abdominal collections in children include “cerebrospinal fluid pseudocysts, post-traumatic collections, pancreatic fluid collections, acalculous cholecystitis , and abscesses due to Crohn’s disease or necrotizing enterocolitis ” [2] . Furthermore, in children, the use of ultrasound is ubiquitous due to the increased radiation risk with computed tomography (CT) scans and the difficulty with prolonged sedation required for magnetic resonance imaging (MRI) for diagnosis and therapy of an abdominal source. Therefore, the algorithm for children with a fluid collection in the abdomen includes the early use of ultrasound-guided drainage for diagnosis or for therapy.
An enteric source of an abscess in the abdomen can be addressed via percutaneous intervention guided by ultrasound as a temporizing measure [1] addressing the acute bacterial infection; however, the underlying source must eventually be addressed as a general principle. For example, a perforated appendicitis, diverticulitis, or an ileopsoas abscess secondary to Crohn’s can be addressed with drainage of the abscess but eventually may require an appendectomy, colon resection, or ileocolic excision, respectively. Postoperative abscess secondary to an enteric source is another common indication for percutaneous drainage. Depending on the location, however, a CT-guided approach may be needed or preferred [26].
Occasionally, a patient presents with idiopathic ascites and part of the workup involves drainage of the fluid for diagnosis or for therapy. It is important to communicate extensively with the primary team to identify the specific indications, risks of bleeding secondary to liver disease, portal hypertension and venous congestion, and next steps with worsening patient status. When a large volume is identified on ultrasound, the drainage should be done in steps with protein-rich replacement to prevent severe hypotension. Patient access for transfusion and fluid resuscitation should be identified prior to starting a paracentesis. Finally, drainage of the ascites might occasionally identify chylous output (potentially indicating a malignancy from lymphatic congestion, an underlying lymphatic abnormality, or an undiagnosed malrotated state of the bowel requiring emergent operative detorsion).
An enteric source must be quickly identified and addressed for most abdominal and pelvic collections. Occasionally, an abdominal or pelvic collection can be secondary to a solid organ such as liver, pancreas, spleen, ovary, or kidney.
A liver abscess can be single or multiple, occurring more commonly in the right lobe or bilaterally, respectively. Various diseases that may lead to pyogenic liver abscesses include prior abdominal surgery, trauma, neoplastic disease, biliary tract disease, or bacteremia in immune-compromised patients [1]. A single abscess can be drained using ultrasound guidance but multiple usually require CT guidance with several catheters inserted. Furthermore, it is imperative that pyogenic abscesses are differentiated from amebic as these are treated with antimicrobials. Other conditions such as tumors, secondary abscesses, and hydatic cysts may present similarly and need to be differentiated as the management options differ drastically.
Pancreatic pseudocysts can develop 1–4 weeks from a bout of pancreatitis. These collections of fluid can be sterile or infected. Immature collections are usually observed unless an infection is suspected on imaging and a sample needs to be obtained. These cysts, once mature, are usually treated surgically or endoscopically, although a percutaneous approach can be used when patient condition prohibits a more definitive intervention. An ultrasound-guided intervention is rarely done due to the location of these cysts and bowel gas obscuring an adequate window for drainage.
Splenic cysts can be congenital, posttraumatic, or idiopathic. Rarely, these cysts can be complex and represent an abscess, presenting with a classic triad of left upper quadrant pain, fever, and leukocytosis [1]. Percutaneous drainage can be used for diagnosis and therapy of the cyst, with surgical excision used for recurrence. Multilocular abscesses and rupture with bleeding are considered relative contraindications with medical therapy reserved for fungal abscess [1].
Ultrasound is the workhorse and preferred imaging modality for the female pelvis: widely available, noninvasive, cheap, does not use ionizing radiations, and is able to provide definitive diagnostic information in heterogeneous clinical situations [27]. An abdominal approach is usually used initially to study the female anatomy; however, a transvaginal approach can be used to provide additional details and for therapeutic interventions. A filled bladder can act as an acoustic window augmenting the transabdominal view but can impede a transvaginal approach due to pressure anteriorly.
Simple cysts are the most common asymptomatic pelvic mass in a female patient. These can be observed and followed using ultrasound with larger lesions (greater than 5–6 cm) having a higher risk of being malignant [27] or requiring intervention to prevent torsion [28]. Hemorrhagic and ruptured cysts can be managed similarly with observation. Any cyst with solid components should have a workup for malignancy—ascites alone is not an accurate predictor of malignancy. Mature cystic teratomas are the most common ovarian tumors in children and adolescents and represent half of all tumors [28]; whereas in adults, epithelial tumors represent 70 % of all ovarian malignancies [27].
Pelvic inflammatory disease is a common cause of acute pelvic pain. A transvaginal approach can be used to diagnose and drain a tubo-ovarian abscess. Sampling of fluid to target antimicrobial therapy can also be a useful adjunct. Furthermore, use of ultrasound can be helpful to exclude alternate pathology causing pelvic pain such as ectopic pregnancy, appendicitis, or endometriosis.
In the setting of percutaneous nephrostomy, ultrasound is valuable for accessing the renal pelvis for interventional procedures and for drainage. Indications include “urinary diversion for urinary tract obstruction, nephrolithiasis, urinary tract infections, urinary fistulas, providing access for subsequent ureteral interventions, such as stent placement, nephroscopy, and ureteroscopy” [29]. These procedures can be performed on native and transplanted kidneys. The most important contraindication is severe coagulopathy. Figure 21.7 demonstrates drainage of a congenital hydronephrosis using ultrasound guidance.

Figure represents needle entry into an enlarged collecting system in the left kidney. Following entry into the collecting system, the needle is replaced by a guidewire, dilator, and drain to evacuate the congenital hydronephrosis
The most common indication is for urinary obstruction from congenital anomalies, from urinary calculi or from a malignancy. Hydronephrosis can also form without an obstruction, such as in pregnancy, over hydration, and diabetes insipidus [29]. Important pre-procedure concepts to consider include abnormal orientation or location of the kidney, presence of a duplicated collecting system, cysts, diverticula and tumors that increase the complexity and difficulty of a procedure, need for lithotripsy prior to or in conjunction with the procedure, and residual contrast that may obscure or eliminate the need for retrograde injection [29].
Infection can occur in the setting of urinary reflux, an obstruction from calculi, or susceptible transplanted kidneys. A renal abscess can rupture externally, presenting as a perinephric abscess, or it can rupture into the collecting system or vascular structures [1]. Percutaneous drainage of a renal or perinephric abscess may be enough, although additional drainage of the collecting system may be necessary if the abscess is associated with urinary obstruction.
Ultrasound can also be used for placement of suprapubic catheters for urinary retention after urethral trauma and in patients needing long-term catheterization for bladder dysfunction in neurological conditions, for example, multiple sclerosis, spinal cord injury [30]. Using an ultrasound, the bladder can be accessed and serially dilated to allow placement of a Foley or alternate catheter. The catheter can be secured to the skin and left in place for a prolonged time period. Once a tract has formed, routine removal and catheterization can be accomplished.
Soft Tissue and Extremities
Similar to head and neck, the soft tissue of the trunk and extremities may exhibit an indication of ultrasound-guided drainage for diagnosis and therapy of an infection, hemorrhage, or a postoperative complication. Use of ultrasound for percutaneous aspiration of breast abscess can be simple, performed as an outpatient, with a low recurrence rate, and improved cosmetic outcomes [31]. Other cysts, abscesses, and superficial collections can similarly be drained percutaneously with ultrasound, limiting morbidity and cosmetic disfigurement.
In extremities, joint aspiration can be augmented with the use of ultrasound with improved diagnostic and therapeutic capability. Systematically screening for soft-tissue infections, including abscesses and bursal fluid collections, before joint aspiration is imperative. Ultrasound use prior to aspiration can lessen the risk of delayed or missed diagnoses and can decrease the risk of joint aspiration by preventing seeding of superficial infection into a sterile joint [32]. Finally, using ultrasound guidance to access the fluid collection can prevent injury to normal or aberrant neurovascular structures. Figure 21.8 demonstrates drainage of a cyst on the anterior knee.

Figure represents needle entry into a cyst anterior to the knee. Similarly, joint effusions can also be drained using ultrasound guidance to minimize complications
Summary
Diagnostic and therapeutic drainage of fluid collections throughout the body using ultrasound guidance should be standard of care. The availability, flexibility, and real-time guidance provided by ultrasound can decrease complications, improve cosmesis, and increase the success of a procedure. Clarifying the indications and understanding the anatomic landmines are essential in completing the procedure with minimal complication. Technical skills are simple in concept but complex in practice and require meticulous care and dedicated training. Finally, thorough preparation including equipment readiness, understanding the disease process and patient’s history, and communication with primary care providers will provide ultimate satisfaction with this approach.
References
Men S, Akhan O, Köroğlu M. Percutaneous drainage of abdominal abcess. Eur J Radiol. 2002;43:204–18.
Hogan MJ, Hoffer FA. Biopsy and drainage techniques in children. Tech Vasc Interv Radiol. 2010;13:206–13.
Röthlin MA, Schöb O, Klotz H, Candinas D, Largiadèr F. Percutaneous drainage of abdominal abscesses: are large-bore catheters necessary? Eur J Surg Acta Chir. 1998;164:419–24.
Ganguli S, Brennan D. Transanorectal interventions. Semin Ultrasound CT MR. 2008;29:483–91.
Sudakoff GS, Lundeen SJ, Otterson MF. Transrectal and transvaginal sonographic intervention of infected pelvic fluid collections: a complete approach. Ultrasound Q. 2005;21:175–85.
Arrabal-Polo MA, Jimenez-Pacheco A, Arrabal-Martin M. Percutaneous drainage of prostatic abscess: case report and literature review. Urol Int. 2012;88:118–20.
Smith RB. Ultrasound-guided procedures for the office. Otolaryngol Clin North Am. 2010;43:1241–54.
Chang K-P, Chen Y-L, Hao S-P, Chen S-M. Ultrasound-guided closed drainage for abscesses of the head and neck. Otolaryngol Head Neck Surg. 2005;132:119–24.
Ramirez-Schrempp D, Dorfman DH, Baker WE, Liteplo AS. Ultrasound soft-tissue applications in the pediatric emergency department: to drain or not to drain? Pediatr Emerg Care. 2009;25:44–8.
Lyon M, Blaivas M. Intraoral ultrasound in the diagnosis and treatment of suspected peritonsillar abscess in the emergency department. Acad Emerg Med. 2005;12:85–8.
Lohela P. Ultrasound-guided drainages and sclerotherapy. Eur Radiol. 2002;12:288–95.
Light RW. Parapneumonic effusions and empyema. Clin Chest Med. 1985;6:55–62.
Padman R, King KA, Iqbal S, Wolfson PJ. Parapneumonic effusion and empyema in children: retrospective review of the duPont experience. Clin Pediatr (Phila). 2007;46:518–22.
Picard E, et al. Predictive factors of morbidity in childhood parapneumonic effusion-associated pneumonia: a retrospective study. Pediatr Infect Dis J. 2010;29:840–3.
Wong KS, Lin TY, Huang YC, Chang LY, Lai SH. Scoring system for empyema thoracis and help in management. Indian J Pediatr. 2005;72:1025–8.
St Peter SD, et al. Thoracoscopic decortication vs tube thoracostomy with fibrinolysis for empyema in children: a prospective, randomized trial. J Pediatr Surg. 2009;44:106–111; discussion 111.
Goligher EC, et al. Utility and safety of draining pleural effusions in mechanically ventilated patients: a systematic review and meta-analysis. Crit Care Lond Engl. 2011;15:R46.
Mattison LE, Coppage L, Alderman DF, Herlong JO, Sahn SA. Pleural effusions in the medical ICU: prevalence, causes, and clinical implications. Chest. 1997;111:1018–23.
Soni N, Williams P. Positive pressure ventilation: what is the real cost? Br J Anaesth. 2008;101:446–57.
Bennett R, Maskell N. Management of malignant pleural effusions. Curr Opin Pulm Med. 2005;11:296–300.
Kastelik JA. Management of malignant pleural effusion. Lung. 2013;191:165–75.
Jones PW, et al. Ultrasound-guided thoracentesis: is it a safer method? Chest. 2003;123:418–23.
Chandraratna PA, Mohar DS, Sidarous PF. Role of echocardiography in the treatment of cardiac tamponade. Echocardiography. 2014;31:899–910.
Fulcher AS, Turner MA. Percutaneous drainage of enteric-related abscesses. Gastroenterologist. 1996;4:276–85.
Lorentzen T, Nolsøe C, Skjoldbye B. Ultrasound-guided drainage of deep pelvic abscesses: experience with 33 cases. Ultrasound Med Biol. 2011;37:723–8.
Gazelle GS, Mueller PR. Abdominal abscess. Imaging and intervention. Radiol Clin North Am. 1994;32:913–32.
Derchi LE, Serafini G, Gandolfo N, Gandolfo NG, Martinoli C. Ultrasound in gynecology. Eur Radiol. 2001;11:2137–55.
Hayes-Jordan A. Surgical management of the incidentally identified ovarian mass. Semin Pediatr Surg. 2005;14:106–10.
Saad WEA, Moorthy M, Ginat D. Percutaneous nephrostomy: native and transplanted kidneys. Tech Vasc Interv Radiol. 2009;12:172–92.
Jacob P, Rai BP, Todd AW. Suprapubic catheter insertion using an ultrasound-guided technique and literature review. BJU Int. 2012;110:779–84.
Karstrup S, et al. Acute puerperal breast abscesses: US-guided drainage. Radiology. 1993;188:807–9.
Hadduck TA, et al. Value of ultrasound before joint aspiration. AJR Am J Roentgenol. 2013;201:W453–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Gadepalli, S. (2016). Diagnostic and Therapeutic Drainage. In: Scholz, S., Jarboe, M. (eds) Diagnostic and Interventional Ultrasound in Pediatrics and Pediatric Surgery. Springer, Cham. https://doi.org/10.1007/978-3-319-21699-7_21
Download citation
DOI: https://doi.org/10.1007/978-3-319-21699-7_21
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-21698-0
Online ISBN: 978-3-319-21699-7
eBook Packages: MedicineMedicine (R0)