
Abstract
The history of prostate-specific antigen (PSA) is full of significant discoveries that have revolutionized the diagnosis and management of prostate cancer. In this chapter we summarize the history of the discovery of PSA and how it became such an integral part of prostate cancer management. Basic biology and physiology of PSA will also be discussed to provide insight about its current and future applications.
The use of PSA to screen for prostate cancer remains a controversial topic of debate and in this chapter we present some of the salient points in the arguments for and against the use of PSA screening. This chapter provides a focused literature review of the benefits and risks of PSA screening and a basis for its current recommendations for prostate cancer early detection.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Prostate-specific antigen
- Prostatic neoplasms
- Mass screening
- History
- Diagnosis
- Randomized controlled trials as topic
- Adverse effects
The discovery and integration of prostate-specific antigen (PSA) has substantially changed the diagnosis, treatment, and management of prostate cancer. Only a few discoveries in the medical field over the last half century can rival the profound impact of PSA. While the current opinions of the appropriate use of PSA as a screening tool can be debated, its impact and the way it has directed the course of prostate cancer research can not.
For many younger clinicians it may be hard to imagine managing a prostate cancer patient without the use of PSA. Prior to the identification of PSA, there were many attempts to identify tumor markers for prostate cancer by several research groups around the world.
The Pursuit and Discovery of PSA
Many trace the initial pursuit for a prostate cancer marker to Gutman and Gutman in 1938 when they found elevated serum phosphatase levels in metastatic prostate cancer patients [1]. Later in 1941, Huggins and Hodges demonstrated this finding was likely related to the presence of bony metastasis in such patients [2]. While the use of serum phosphatase in prostate cancer was eventually found to be limited as a clinically useful tumor marker due to its poor sensitivity and specificity, it did pave the way for many groups to began focused research in the field.
Over the next decade, prostatic acid phosphatase (PAP ) was identified as a potential tumor marker. Several different assays to measure PAP were developed to aid in the clinical management of prostate cancer patients. Early assays measured total enzyme activity of PAP, mainly calorimetric, which involved the use of reagents that change color in the presence of a specific substrate [3]. Later, newer techniques using radioimmunoassays were able to moderately improve the specificity of testing for PAP [4]. Ultimately, while PAP was found to be a more specific marker, it lacked the sensitivity for prostate cancer needed to be clinically useful, as it was noted to be elevated in several benign prostatic diseases and even after digital rectal exam (DRE) [5]. It was also found only to be elevated in 20–30 % of patients with clinically localized prostate cancer.
The work with PAP and other markers brought to light the need for a more sensitive and reliable tumor marker. There was also a shift in focus to find a marker that was present or elevated in those patients with clinically localized disease, as these patients could possibly benefit from a serum assay test that could be useful to monitor or even initiate treatment .
Many groups claimed to have conducted the research that led to the discovery of PSA. One of the earliest reports on the identification of prostate-specific antigens was by Rubin Flocks in 1960 [6]. In 1966, a Japanese forensic scientist, Mitsuwo Hara, partially characterized and reported on a protein many consider similar to PSA. He labeled the protein “gamma-seminoprotein” and proposed its use as forensic evidence in rape cases because of its presence in seminal fluid [7]. Later Li and Beling further purified this protein and reported it to have a molecular weight of 31 kilodaltons (kDa) [8]. Similar reports and characterization were done by Sensabaugh and his group confirming this protein to have specificity for human semen [9]. Years later, through the work of Wang and Papsidero the purification of this protein demonstrated that it was identical to that of PSA found in human serum [10, 11]. More definitively, in 1970 and 1972 Albin published his reports of a purified antigen isolated from prostate tissue [12, 13].
In 1979, T. Ming Chu and his research group purified and characterized PSA and demonstrated its presence in both benign and malignant prostate tissue [11, 14]. These studies confirmed that PSA was highly specific for prostate tissue and was produced by prostatic epithelial cells. This group was also credited with the first development of an immunoassay that could be used for human serum testing although it was much less sensitive than those used today detecting PSA at a minimal concentration of 500 ng/ml compared to modern assay’s detecting PSA at <0.01 ng/ml [11]. In 1987, early work in the clinical applications of PSA by Chu’s group and Thomas Stamey demonstrated a use for PSA in monitoring the course of patients known to have prostate cancer [15].
More precise testing using protein sequencing has determined that many of the groups from the 1960s and 1970s were most likely describing prostate-specific antigen or one of its natural analogues [16].
Shortly after its discovery much of the interest on PSA focused on determination of its physiologic role. In 1984 Chu et al. reported that PSA was a protease and later through studies by Lilja its role in the proteolytic cleavage of seminal vesicle proteins was published [17, 18]. They described the role of PSA as cleaving the gel-forming proteins from the seminal vesicles (semenogelins I, II and fibronectin) which initiates liquefaction of the ejaculate, thereby increasing the motility of sperm and aiding in fertilization. These studies and others also identified several other prostatic proteins similar to PSA, notably human kallikrein 2 (hK2). Similar to PSA, it is expressed by prostatic tissue and has a similar role in cleaving of seminal vesicle proteins , although it is much more potent enzymatically [19].
Later in the 1980s PSA was confirmed to belong to the human kallikrein family of serine proteases, and it was given formal nomenclature and labeled human kallikrein 3 (hK3) [20]. There are currently 15 other members of this family that have been described in the literature and many of them are believed to play some role in many human cancers [21]. The relationship between PSA and hK2 is worth noting. These two share many common features but also some key differences. PSA and hK2 share 80 % amino acid sequence homology but hK2 is present in 1–2 % of the amount of PSA found in typical prostate tissue [22]. In vitro studies have demonstrated that hK2 has the ability to autoactivate, while PSA does not have this characteristic and for this reason some have proposed a role for hK2 in regulating the activity of PSA [23].
Further studies into the physiologic role of PSA also uncovered two forms of PSA most commonly found in patients serum. One form was smaller than the other (36 kDa compared to 90–100 kDa) and it was found later by Lilja and Stenman that the smaller form was that of free PSA and the larger was complexed PSA (also known as bound PSA) [24]. Studies showed that PSA was most commonly complexed with alpha-1-antichymotrypsin, a protease inhibitor [25]. Only 10–30 % of PSA was present in an uncomplexed form. Free PSA represented the inactive form and was typically higher in patients with begin prostatic conditions. Other studies demonstrated that the level of free PSA was lower in prostate cancer patients and this subsequently led to the development of immunoassays to test specifically for it [26]. The ratio of free PSA to total PSA has proven useful in its clinical application and ability to increase the positive predictive value for positive prostate biopsies [27].
The Golden Years of PSA Testing
The Federal Drug Administration (FDA ) approved the first commercial immunoassay for PSA testing in 1987. Around this time Stamey et al. and Oesterling reported the half-life of PSA to be 2.2 ± 0.8 and 3.2 ± 0.1 days respectively [15, 28]. Subsequently several assays were developed for PSA testing including Tandem-R PSA®, Pros-check PSA®, Tandem-E PSA®, IRMA-count PSA®, and Abbott IMX PSA®. Myrtle et al. was one of the first to attempt to give the reference range for a “normal” PSA value with the use of the Tandem R PSA® assay [29]. He studied the reported PSA values in a population of 472 men without a history of prostate cancer, most of which were below the age of 60 years. Other larger studies attempted to find the ideal value for initiating prostate biopsy looking at more clinically relevant patient populations (i.e., over 50 years of age) and varied in their suggested cutoff values between 2.8 and 4.0 ng/ml using a standard deviation of ±2 [30, 31]. Ultimately it was the screening test reported from a cohort of 6630 men aged 50–74 years of age using a cutoff value of 4.0 ng/ml that led to the FDA’s approval of screening with PSA [32–35]. Consequently the value of 4.0 ng/ml became most commonly used for initiating prostate biopsy, although at the time several groups felt this value to be too aggressive and proposed a cutoff value of 10 ng/ml. Notably in 2004 the National Comprehensive Cancer Network recommended a lower cutoff of 2.5 ng/ml citing the number of cancers missed with higher cutoffs and the benefits in patient outcomes reported at that time.
Early use of these commercial assays used in the clinical setting led to inconsistent results and created the need for standardization of PSA testing. Graves et al. called for an international standardization of PSA assays in 1990, which led to the principles used in PSA testing today [36]. The issue he described centered around the fact that each assay detected different molar ratios of the various forms of PSA found in the serum (free vs. bound to proteins) and therefore different results were obtained with different assays from the same serum [37]. As many of the initial PSA screening trials were done using the Tandem R PSA® assay from Hybritech, newer assays that came on the market were initially “standardized” to the values of this assay. With time it became apparent that there was increasing variability between these assays and their reported PSA values. Naturally this raised many concerns, especially when following patients’ PSA values could dictate the decision to perform a prostate biopsy. In an effort to mitigate these effects, a group of researchers and experts convened at Stanford University in 1994 and proposed a method of standardization that later was adopted by the World Health Organization (WHO) who issued the First International Reference Preparation (IRP) for PSA in 1999. Unknowingly the standardization from the WHO produced PSA values that were approximately 22 % lower than that of the traditional results from the Tandem R PSA assay®. These discrepancies had the potential to cause serious confusion among physicians and potentially resulted in some patients not being offered biopsy, especially when following patients by such metrics as PSA velocity.
In 1990, the idea for the incorporation of PSA as part of the initial work up for diagnosing prostate cancer was introduced by Cooner [38]. He described using PSA testing as part of a “three-legged stool” which included DRE and transrectal ultrasound guided prostate biopsies. This algorithm was believed to be superior for prostate cancer screening since DRE alone found that 70–80 % of patient had locally advanced or metastatic disease at diagnosis [39]. Subsequent to his initial study, Cooner and several other groups attempted to improve the specificity of PSA testing for prostate cancer by reporting on age-specific PSA values [40–42]. These studies were done in part due to the fact that patients with benign prostatic hyperplasia (BPH) had increased PSA levels making one “normal” value for all men unreliable. The introduction of PSA density (prostate volume/PSA) and PSA velocity (changes over time) was an attempt to compensate for these limitations [43].
In 1991, Catalona et al. used a PSA cutoff of 4.0 ng/mL in the initial screening of prostate cancer patients and suggested the use of PSA as a screening test for prostate cancer [32, 40]. Over the next couple of years several medical groups including the American Urological Association (AUA ) and American Cancer Association (ACA ) endorsed annual PSA screening for men over 50 years of age.
During this time PSA screening was hailed as dramatically improving the detection of curable prostate cancer. Gann et al. found in men diagnosed with prostate cancer an elevated PSA preceded an abnormal DRE by an average of 6.2 years [42]. Incorporation of PSA screening into clinical practice resulted in an increase of prostate cancer detection from 1987 to 1992 of 85 %. By 1997, 75 % of prostate cancers were diagnosed by elevated or abnormal PSAs in the United States of America (USA) [44, 45]. Stage migration of prostate cancer also dramatically shifted during this time with Catalona et al. publishing a report in 1993 that 70–80 % of men were being diagnosed with organ confined disease compared to historical cohorts of 20–30 % [33]. The Center for Prostate Disease Research (CPDR) reported that the percentage of patients presenting with metastatic disease decreased from 19.8 % in 1989 to 3.3 % by 1998 [46].
The Trials and Tribulations of PSA Screening
After PSA screening came into practice in the USA in the late 1980s and especially in the early 1990s, the incidence of prostate cancer diagnosis rapidly increased, with mortality rates subsequently declining [47]. Etzioni and colleagues used modeling data from Surveillance, Epidemiology, and End Results (SEER) Medicare and screening standards used in the Prostate, Lung, Colorectal and Ovarian screening trial (PLCO ) to show that PSA screening alone could not account for the decrease in prostate cancer mortality seen during the 1990s [48]. Their work and others highlighted the fact that while PSA screening certainly played a role in the mortality decrease for prostate cancer patients, especially in the USA, the increase in new and more aggressive treatments also contributed to this decline. Tapering enthusiasm for PSA screening, Albertsen and colleagues published data that showed that many patients in the pre-PSA screening era, when followed without treatment, were destined to die of causes other than prostate cancer [49].
Opposition to PSA’s use and specifically PSA screening became more common by the late 1990s and early 2000s. Concern grew that the results of the emerging retrospective studies showing improved diagnosis and survival of prostate cancer patients using PSA screening were confounded by lead time and length time biases. Around this time several large randomized studies testing the hypothesis that PSA screening could decrease prostate cancer-specific mortality were initiated.
The two largest and most discussed studies regarding PSA screening are the Prostate, Lung, Colorectal and Ovarian screening trial (PLCO) in the USA and the European Randomized Study of Screening for Prostate Cancer (ERSPC) [50, 51]. Several other large studies also contributed to the evaluation of the benefits and risks of PSA screening including Prostate Cancer Intervention Versus Observation Trial (PIVOT), Prostate Cancer Prevention Trial (PCPT), and Reduction by Dutasteride of Clinical Progression Events in Expectant Management (REDEEM) trial [52–54]. It is essential that all physicians who treat or manage prostate cancer patients read and understand the results of these trials.
The primary objectives of both ERSPC and PLCO were nearly identical. The main endpoint in both studies was prostate cancer mortality. One of the main differences between the two studies was the population in Europe, at least during the early years of the study, had less exposure to PSA testing and thus offered a less “contaminated” control group. Unfortunately, men enrolling in the US study had significant exposure to PSA testing compromising the PLCO control group. In this regard many consider the PLCO trial to be one of comparing systematic PSA screening to “opportunistic” screening as evidenced by the fact that the absolute difference in those who underwent PSA screening at anytime during the study between the screening and control group was only 33 %.
There was also some other differences between the trials that deserve mention. In PLCO the contamination rate was reported to be 54.8 % with patients obtaining a PSA outside the trials design [55]. The best reported rate of contamination in ERSPC published was 30.7 %, although this data is hard to come by in Europe [56]. It should be mentioned that for the power calculations used in the design of the ERSPC trial a contamination rate of 20 % was employed. There was also a large difference between the two trials with regard to performing indicated prostate biopsies. In PLCO the rate of biopsy was 41 % in patients indicated for biopsy during the first year of the study and rose to 64 % with the third year of screening. In ERSPC the rate was 85.8 % for patients indicated within its trial design [57]. This difference likely contributes to the lower rate of cancer detection seen in the PLCO screening arm and may have impacted comparison between the two arms in regard to prostate cancer mortality.
The randomization of patients in both trials also had some notable differences, along with the indications for biopsy. Patients aged 50–74 years were randomized to the two arms but later a “core age group” was defined in reporting much of the data from ERSPC, which had patients aged 55–69. Men in the screening arm were screened at 4-year interval, except in Sweden in which they were screened at 2-year intervals. Indications for biopsy varied among the constitute centers for the ERSPC trial. Initially some centers required a PSA over 4.0 ng/dl and an abnormal DRE as an indication for biopsy. After 1997, all centers, minus Finland, recommended biopsy for a PSA over 3.0 ng/dl. In Finland DRE was required to be positive for PSA in the 3–3.9 ng/dl range and later this changed to having a free/total ratio of PSA of equal to or less than 0.16. In Italy patients with a PSA of 2.5–3.9 ng/dl had DRE and transrectal ultrasound (TRUS) performed. When performing biopsies a lateral sextant method was applied in all centers but the execution of these was left to individual study groups within ERSPC. Medical contraindications were the only exception listed for not performing an indicated biopsy. After a diagnosis of prostate cancer, treatment decisions were left to the discretion of local providers.
PLCO initially randomized patients aged 60–74 years old, later they included patients aged 55–60 and also used prior PSA testing with 3 years of entry to the trial to reduce contamination between the two arms. In PLCO screening with DRE and PSA was offered yearly for the first 4 years and then with PSA alone for another 2 years. Recommended indications for prostate biopsy were “community standard” where initially a PSA value above 4.0 ng/dl and/or abnormal DRE. In later years a significant percentage of patients underwent biopsy for a PSA 2.5–4.0 ng/dl. The biopsy extent and the number of cores were left to the individual providers in the community.
In 2009 both trials published their initial results. ERSPC reported it findings after its data monitoring committee found a significant difference in prostate cancer mortality in favor of the screening arm at the time of its third predetermined interim analysis. The publishing of the results for the PLCO trial was done after the safety monitoring committee found a continuing lack of significant difference in the death rates between the two study groups and felt that this presented concerns in regard to public health. The PLCO trial was updated in 2012 with 13-year follow-up between the two arms of the study and continued to show no statistical difference between the intervention arm (organized screening) and the control arm (opportunistic screening) [58]. Recent updates from ERSPC in 2014, now with 13-year follow-up, have continued to show a survival benefit for patients undergoing PSA screening and in fact that benefit has increased modestly [59]. Their findings reported a significant 21 % relative reduction in prostate cancer in intention to screen analyses, and a 27 % relative reduction in men who actually had screening. These recent updates showed an improved benefit of PSA screening with longer follow-up demonstrated by the number needed to screen and number needed to be diagnosed with prostate cancer to prevent one prostate cancer death. As seen in the table below, Table 1.1, both numbers in the case of the ERSPC trial have become substantially lower in their most recent follow-up data at 13 years compared to the numbers reported at 11 years and 9 years of follow-up [60]. For reference, the number needed to be screened with digital mammography to save one life from breast cancer was reported as 1339 (CI: 322–7455) and 377 (CI 230 to 1050) in women aged 50–59 years old and 60–69 years old, respectively [61]. Similarly the reported number needed to screen for colorectal cancer with fecal occult blood testing is 1176 [62]. The Göteborg screening trial, which was comprised of a significant number of patients who were enrolled in the ERSPC trial, also further supported these findings and reported a number of approximately 300 patients needing to be screened to prevent one death from prostate cancer at 14 years [63]. In contrast a study that looked at the largest center that participated in ERSPC, Finland, which by itself had a larger number of study patients than PLCO, showed only a non-statistically significant benefit in prostate cancer mortality among patients in the screening arm of the study [64]. This finding along with treatment patterns favoring men in the screened arm continues to cause concern about the real benefit of PSA-based screening.
Several other groups have used modeling data to estimate the improved benefits of PSA screening with longer follow-up. Gulati et al. projected 25-year estimates of the number needed to screen and to treat to prevent one prostate cancer death for men aged 55–69 years at diagnosis using data from ERSPC and PLCO [65]. They reported that in Europe, the number needed to screen was 262 and number needed to treat was nine after 25 years. Attempting to control for rates of overdiagnosis in the USA, they reported the number needed to screen was 186–220 and number needed to treat being 2–5. These statistics are markedly lower than the most recent 13-year follow-up data from the ERSPC.
We strongly encourage the reader to become familiar with both trials as the debate regarding their results and their impact on PSA screening is likely to continue for years to come. The results of future studies, particularly the Comparison Arm for Prostate Testing for Cancer and Treatment trial (CAP/ProtecT) of 450,000 men from the United Kingdom, will likely add to our current data on the use of PSA screening and prostate cancer [66].
At the center of the PSA screening debate is the attempt to realize the beneficial and adverse effects of screening. Finding the equilibrium between these two results is unlikely to be found in the scientific or medical literature but must be valued within the political and social systems in which screening is practiced.
The Effects of Screening with PSA and Overdiagnosis
Some of the issues surrounding screening with PSA revolve around the risk of overtreatment for low grade and low-risk prostate cancer patients. With the influx of new cases in the early 1990s after the integration of regular PSA screening, there was also a natural increase in the number of patient undergoing definitive treatment. Concerns about the long-term effects of these treatments, especially those patients that are younger and those with low-risk disease, gave rise to an emerging field of study in prostate cancer, cancer survivorship. The product of early screening and treatment along with the frequency and high survival rates of prostate cancer patients has created a growing population of prostate cancer survivors [67]. Both the American Cancer Society and a recent study by Mariotto et al. estimate that there are now more than two million prostate cancer survivors living in the USA and that number is expected to climb [68, 69].
Recently several groups have published long-term data regarding the effects of prostate cancer treatment [70]. One of the largest populations that have been reported on for these effects is the Prostate Cancer Outcomes Study (PCOS) which follows 1164 men who underwent treatment with surgery and 491 who had radiotherapy. The study assessed functional status immediately after treatment and at 2, 5, and 15 years after diagnosis. Resnick et al. reported data for this group at 15 years and found the prevalence of erectile dysfunction was very high, affecting 87.0 % of men in the prostatectomy group and 93.9 % of those in the radiotherapy group [71]. This study was somewhat limited by the lack of a control group (e.g., active surveillance) and reliable pretreatment baseline data. Regardless this study and others have placed a spotlight on the long-term effects of invasive procedures needed to treat and cure prostate cancer.
Dealing with the sequelae of prostate cancer treatment, especially long-term survivors, can place a significant burden on patients, both financially and in terms of time and efforts. De Oliveria et al. looked at a population of prostate cancer survivors in Canada and found higher total health care expenses among younger patients, metastatic patients, and those who underwent treatment with surgery [72]. They also found lower costs in patients with better urinary function. Similar findings in a study of prostate cancer patients in the USA who were recently diagnosed, within 1–3 years, found total out of pocket expenses and overall costs were inversely related to most of the commonly employed prostate-specific health-related quality of life survey scores [73].
The long-term effects of prostate cancer treatment are not limited to those undergoing surgery or radiation. Morgans et al. showed that in patients undergoing prolonged androgen deprivation the risk of developing comorbidities, specifically diabetes and cardiovascular disease, is increased well above those of age matched controls [74]. This risk was especially high among those patients who already had significant comorbidities prior to treatment.
The risks of long-term morbidity from prostate cancer treatment need to be considered by both the physician and patient prior to initiating screening. Several groups have attempted to better define those patients suitable for treatment and screening. Using data from the PCOS, Daskivich et al. have published their findings in an attempt to better understand competing risk for mortality in patients with prostate cancer [75]. The cumulative incidence of other cause mortality at 14 years was modeled based on comorbidities (Table 1.2). Prostate cancer mortality at 14 years using the same analysis was 5, 8, and 23 % for men with low-, intermediate-, and high-risk disease respectively using the D’Amico classification [76].
The Evolution of Prostate Tumor Markers
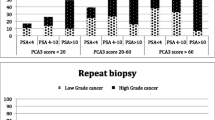
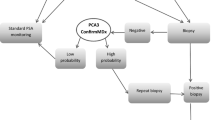
While the exact role for PSA, especially in regard to screening, continues to evolve, the ongoing development of even more specific and ideally more applicable tumor markers for prostate cancer continues to progress. Many of these improvements surround PSA itself. Of these, the prostate health index, which is an assay using the concentration of a molecular isoform of free PSA, total PSA, and proPSA, has a greater specificity than total PSA or percentage-free PSA in select patients [78]. Addition of the four kallikrein protein assay has shown promise in being able to discriminate patients at risk for high grade prostate cancer [79]. Many of these assays are being introduced and appear to be making a clinical impact in the management and diagnosis of prostate cancer patients with a particular focus on their integration into screening algorithms. How they will compare to the current methods for screening and diagnosis will need to be investigated in randomized trials [80].
Abbreviations
- PSA:
-
Prostate-specific antigen
- PAP:
-
Prostatic acid phosphatase
- DRE:
-
Digital rectal exam
- kDa:
-
Kilodaltons
- hK2:
-
Human kallikrein 2
- FDA:
-
Federal Drug Administration
- WHO:
-
World Health Organization
- IRP:
-
International Reference Preparation
- BPH:
-
Benign prostatic hyperplasia
- AUA:
-
American Urological Association
- ACA:
-
American Cancer Association
- USA:
-
United States of America
- CPDR:
-
Center for Prostate Disease Research
- SEER:
-
Surveillance epidemiology, and end results
- PLCO:
-
Prostate lung, colorectal and ovarian screening
- ERSPC:
-
European randomized study of screening for prostate cancer
- PIVOT:
-
Prostate cancer intervention versus observation trial
- PCPT:
-
Prostate cancer prevention trial
- REDEEM:
-
Reduction by dutasteride of clinical progression events in expectant management
- TRUS:
-
Transrectal ultrasound
- CAP/ProtecT:
-
Comparison arm for prostate testing for cancer and treatment trial
- PCOS:
-
Prostate cancer outcomes study
References
Gutman AB, Gutman EB. An acid phosphatase occurring in the serum of patients with metastasizing carcinoma of the prostate gland. J Clin Invest. 1938;17(1):473–9.
Huggins HR, Hodges CV. Studies on prostatic cancer: the effects of castration of estrogen and of androgen injection on serum phosphatases on metastatic carcinoma of the prostate. Cancer Res. 1941;1(1):293–7.
Fishman WH, Lerner F. A method for estimating serum acid phosphatase of prostatic origin. J Biol Chem. 1953;200(1):89–97.
Griffiths JC. Prostate-specific acid phosphatase: re-evaluation of radioimmunoassay in diagnosing prostatic disease. Clin Chem. 1980;26(3):433–6.
Li CY, Chuda RA, Lam WK, Yam LT. Acid phosphatases in human plasma. J Lab Clin Med. 1973;82(3):446–60.
Flocks R, Urich V, Patel C, Opitz J. Studies on the antigenic properties of prostatic tissue. J Urol. 1960;84:134–43.
Hara M, Koyanagi Y, Inoue T, Fukuyama T. Some physico-chemical characteristics of “ -seminoprotein”, an antigenic component specific for human seminal plasma. Forensic immunological study of body fluids and secretion. VII. Nihon Hoigaku Zasshi. 1971;25(4):322–4. Japanese.
Li TS, Beling CG. Isolation and characterization of two specific antigens of human seminal plasma. Fertil Steril. 1973;24(2):134–44.
Sensabaugh GF. Isolation and characterization of a semen-specific protein from human seminal plasma: a potential new marker for semen identification. J Forensic Sci. 1978;23(1):106–15.
Wang MC, Valenzuela LA, Murphy GP, Chu TM. Tissue specific and tumor specific antigens in human prostate. Fed Proc. 1977;36:1254.
Papsidero LD, Wang MC, Valenzuela LA, Murphy GP, Chu TM. A prostate antigen in sera of prostatic cancer patients. Cancer Res. 1980;40(7):2428–32.
Ablin RJ, Bronson P, Soanes WA, Witebsky E. Tissue- and species-specific antigens of normal human prostatic tissue. J Immunol. 1970;104(6):1329–39.
Ablin RJ, Soanes WA, Bronson P, Witebsky E. Precipitating antigens of the normal human prostate. J Reprod Fertil. 1970;22(3):573–4.
Wang MC, Valenzuela LA, Murphy GP, Chu TM. Purification of a human prostate specific antigen. Invest Urol. 1979;17(2):159–63.
Stamey TA, Yang N, Hay AR, McNeal JE, Freiha FS, Redwine E. Prostate-specific antigen as a serum marker for adenocarcinoma of the prostate. N Engl J Med. 1987;317:909–16.
Sokoll LJ, Chan DW. Prostate-specific antigen. Its discovery and biochemical characteristics. Urol Clin North Am. 1997;24(2):253–9. Review.
Ban Y, Wang MC, Watt KW, Loor R, Chu TM. The proteolytic activity of human prostate-specific antigen. Biochem Biophys Res Commun. 1984;123(2):482–8.
Lilja H. A kallikrein-like serine protease in prostatic fluid cleaves the predominant seminal vesicle protein. J Clin Invest. 1985;76(5):1899–903.
Lilja H. Structure and function of prostatic- and seminal vesicle-secreted proteins involved in the gelation and liquefaction of human semen. Scand J Clin Lab Invest Suppl. 1988;191:13–20.
Berg T, Bradshaw RA, Carretero OA, Chao J, Chao L, Clements JA, et al. A common nomenclature for members of the tissue (glandular) kallikrein gene families. Agents Actions Suppl. 1992;38(Pt 1):19–25.
Borgoño CA, Michael IP, Diamandis EP. Human tissue kallikreins: physiologic roles and applications in cancer. Mol Cancer Res. 2004;2(5):257–80. Review.
De Angelis G, Rittenhouse HG, Mikolajczyk SD, Blair Shamel L, Semjonow A. Twenty years of PSA: from prostate antigen to tumor marker. Rev Urol. 2007;9(3):113–23. Summer.
Mikolajczyk SD, Millar LS, Marker KM, Grauer LS, Goel A, Cass MM, et al. Ala217 is important for the catalytic function and autoactivation of prostate-specific human kallikrein 2. Eur J Biochem. 1997;246(2):440–6.
Stenman UH, Leinonen J, Alfthan H, Rannikko S, Tuhkanen K, Alfthan O. A complex between prostate-specific antigen and alpha 1-antichymotrypsin is the major form of prostate-specific antigen in serum of patients with prostatic cancer: assay of the complex improves clinical sensitivity for cancer. Cancer Res. 1991;51(1):222–6.
Lilja H, Christensson A, Dahlén U, Matikainen MT, Nilsson O, Pettersson K, et al. Prostate-specific antigen in serum occurs predominantly in complex with alpha 1-antichymotrypsin. Clin Chem. 1991;37(9):1618–25.
Chen Z, Chen H, Stamey TA. Prostate specific antigen in benign prostatic hyperplasia: purification and characterization. J Urol. 1997;157(6):2166–70.
Toubert ME, Guillet J, Chiron M, Meria P, Role C, Schlageter MH, et al. Percentage of free serum prostate-specific antigen: a new tool in the early diagnosis of prostatic cancer. Eur J Cancer. 1996;32A(12):2088–93.
Oesterling JE, Chan DW, Epstein JI, Kimball Jr AW, Bruzek DJ, Rock RC, et al. Prostate specific antigen in the preoperative and postoperative evaluation of localized prostatic cancer treated with radical prostatectomy. J Urol. 1988;139(4):766–72.
Myrtle JF, Klimley PG, Ivor LP, Brun JF. Clinical utility of prostate-specific antigen (PSA) in the management of prostate cancer. Advances in Cancer Diagnosis. Hybritech. 1986.
Kane RA, Littrup PJ, Babaian R, Drago JR, Lee F, Chesley A, et al. Prostate-specific antigen levels in 1695 men without evidence of prostate cancer. Findings of the American Cancer Society National Prostate Cancer Detection Project. Cancer. 1992;69(5):1201–7.
Dalkin BL, Ahmann FR, Kopp JB. Prostate specific antigen levels in men older than 50 years without clinical evidence of prostatic carcinoma. J Urol. 1993;150(6):1837–9.
Catalona WJ, Smith DS, Ratliff TL, Dodds KM, Coplen DE, Yuan JJ, et al. Measurement of prostate-specific antigen in serum as a screening test for prostate cancer. N Engl J Med. 1991;324(17):1156–61. Erratum in: N Engl J Med 1991 Oct 31;325(18):1324.
Catalona WJ, Smith DS, Ratliff TL, Basler JW. Detection of organ-confined prostate cancer is increased through prostate-specific antigen-based screening. JAMA. 1993;270(8):948–54.
Dalkin BL, Ahmann FR, Kopp JB, Catalona WJ, Ratliff TL, Hudson MA, et al. Derivation and application of upper limits for prostate specific antigen in men aged 50-74 years with no clinical evidence of prostatic carcinoma. Br J Urol. 1995;76(3):346–50.
Catalona WJ, Richie JP, Ahmann FR, Hudson MA, Scardino PT, Flanigan RC, et al. Comparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6,630 men. J Urol. 1994;151(5):1283–90.
Graves HC, Wehner N, Stamey TA. Comparison of a polyclonal and monoclonal immunoassay for PSA: need for an international antigen standard. J Urol. 1990;144(6):1516–22.
Punglia RS, D'Amico AV, Catalona WJ, Roehl KA, Kuntz KM. Effect of verification bias on screening for prostate cancer by measurement of prostate-specific antigen. N Engl J Med. 2003;349(4):335–42.
Cooner WH, Mosley BR, Rutherford Jr CL, Beard JH, Pond HS, Terry WJ, et al. Prostate cancer detection in a clinical urological practice by ultrasonography, digital rectal examination and prostate specific antigen. J Urol. 1990;143(6):1146–52. discussion 1152-4.
Brawer MK. Prostate specific antigen. New York, NY: Marcel Dekker; 2001.
Brawer MK, Chetner MP, Beatie J, Buchner DM, Vessella RL, Lange PH. Screening for prostatic carcinoma with prostate specific antigen. J Urol. 1992;147(3 Pt 2):841–5.
Carter HB, Pearson JD, Metter EJ, Brant LJ, Chan DW, Andres R, et al. Longitudinal evaluation of prostate-specific antigen levels in men with and without prostate disease. JAMA. 1992;267(16):2215–20.
Gann PH, Hennekens CH, Stampfer MJ. A prospective evaluation of plasma prostate-specific antigen for detection of prostatic cancer. JAMA. 1995;273(4):289–94.
Carter HB, Ferrucci L, Kettermann A, Landis P, Wright EJ, Epstein JI, et al. Detection of life-threatening prostate cancer with prostate-specific antigen velocity during a window of curability. J Natl Cancer Inst. 2006;98(21):1521–7.
Potosky AL, Miller BA, Albertsen PC, Kramer BS. The role of increasing detection in the rising incidence of prostate cancer. JAMA. 1995;273(7):548–52.
Plawker MW, Fleisher JM, Vapnek EM, Macchia RJ. Current trends in prostate cancer diagnosis and staging among United States urologists. J Urol. 1997;158(5):1853–8.
Sun L, Gancarczyk K, Paquette EL, McLeod DG, Kane C, Kusuda L, et al. Introduction to Department of Defense Center for Prostate Disease Research Multicenter National Prostate Cancer Database, and analysis of changes in the PSA-era. Urol Oncol. 2001;6(5):203–9.
Hankey BF, Feuer EJ, Clegg LX, Hayes RB, Legler JM, Prorok PC, et al. Cancer surveillance series: interpreting trends in prostate cancer--part I: evidence of the effects of screening in recent prostate cancer incidence, mortality, and survival rates. J Natl Cancer Inst. 1999;91(12):1017–24.
Etzioni R, Legler JM, Feuer EJ, Merrill RM, Cronin KA, Hankey BF. Cancer surveillance series: interpreting trends in prostate cancer – part III: quantifying the link between population prostate-specific antigen testing and recent declines in prostate cancer mortality. J Natl Cancer Inst. 1999;91(12):1033–9.
Albertsen PC, Fryback DG, Storer BE, Kolon TF, Fine J. Long-term survival among men with conservatively treated localized prostate cancer. JAMA. 1995;274(8):626–31.
Andriole GL, Crawford ED, Grubb 3rd RL, Buys SS, Chia D, Church TR, et al. Mortality results from a randomized prostate-cancer screening trial. N Engl J Med. 2009;360(13):1310–9.
Schröder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V, et al. Screening and prostate-cancer mortality in a randomized European study. N Engl J Med. 2009;360(13):1320–8.
Wilt TJ, Brawer MK, Jones KM, Barry MJ, Aronson WJ, Fox S, et al. Radical prostatectomy versus observation for localized prostate cancer. N Engl J Med. 2012;367(3):203–13.
Thompson IM, Goodman PJ, Tangen CM, Lucia MS, Miller GJ, Ford LG, et al. The influence of finasteride on the development of prostate cancer. N Engl J Med. 2003;349(3):215–24.
Andriole GL, Bostwick DG, Brawley OW, Gomella LG, Marberger M, Montorsi F, REDUCE Study Group, et al. Effect of dutasteride on the risk of prostate cancer. N Engl J Med. 2010;362(13):1192–202.
Pinsky PF, Black A, Kramer BS, Miller A, Prorok PC, Berg C. Assessing contamination and compliance in the prostate component of the Prostate, Lung, Colorectal, and Ovarian (PLCO) cancer screening trial. Clin Trials. 2010;7(4):303–11.
Roobol MJ, Kerkhof M, Schröder FH, Cuzick J, Sasieni P, Hakama M, et al. Prostate cancer mortality reduction by prostate-specific antigen-based screening adjusted for nonattendance and contamination in the European Randomised Study of Screening for Prostate Cancer (ERSPC). Eur Urol. 2009;56(4):584–91.
Schröder FH, Roobol MJ. ERSPC and PLCO prostate cancer screening studies: what are the differences? Eur Urol. 2010;58(1):46–52.
Andriole GL, Crawford ED, Grubb 3rd RL, Buys SS, Chia D, Church TR, et al. Prostate cancer screening in the randomized prostate, lung, colorectal, and ovarian cancer screening trial: mortality results after 13 years of follow-up. J Natl Cancer Inst. 2012;104(2):125–32.
Schröder FH, Hugosson J, Roobol MJ, Tammela TL, Zappa M, Nelen V, et al. Screening and prostate cancer mortality: results of the European Randomised Study of Screening for Prostate Cancer (ERSPC) at 13 years of follow-up. Lancet. 2014;384(9959):2027–35.
Schröder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V, et al. Prostate-cancer mortality at 11 years of follow-up. N Engl J Med. 2012;366(11):981–90.
US Preventive Services Task Force. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;151(10):716–26, W-236.
Hewitson P, Glasziou P, Irwig L, Towler B, Watson E. Screening for colorectal cancer using the faecal occult blood test. Hemoccult. Cochrane Database Syst Rev. 2007;1, CD001216. Review.
Hugosson J, Carlsson S, Aus G, Bergdahl S, Khatami A, Lodding P, et al. Mortality results from the Göteborg randomised population-based prostate-cancer screening trial. Lancet Oncol. 2010;11(8):725–32.
Kilpeläinen TP, Tammela TL, Malila N, Hakama M, Santti H, Määttänen L, et al. Prostate cancer mortality in the Finnish randomized screening trial. J Natl Cancer Inst. 2013;105(10):719–25.
Gulati R, Mariotto AB, Chen S, Gore JL, Etzioni R. Long-term projections of the harm-benefit trade-off in prostate cancer screening are more favorable than previous short-term estimates. J Clin Epidemiol. 2011;64(12):1412–7.
Lane JA, Donovan JL, Davis M, Walsh E, Dedman D, Down L, ProtecT study group, et al. Active monitoring, radical prostatectomy, or radiotherapy for localised prostate cancer: study design and diagnostic and baseline results of the ProtecT randomised phase 3 trial. Lancet Oncol. 2014;15(10):1109–18.
Heijnsdijk EA, Wever EM, Auvinen A, Hugosson J, Ciatto S, Nelen V, et al. Quality-of-life effects of prostate-specific antigen screening. N Engl J Med. 2012;367(7):595–605.
American Cancer Society: What is prostate cancer?. http://www.cancer.org/cancer/prostatecancer/. Accessed 28 Nov 2014.
Mariotto AB, Yabroff KR, Shao Y, Feuer EJ, Brown ML. Projections of the cost of cancer care in the United States: 2010-2020. J Natl Cancer Inst. 2011;103(2):117–28.
Taylor KL, Luta G, Miller AB, Church TR, Kelly SP, Muenz LR, et al. Long-term disease-specific functioning among prostate cancer survivors and noncancer controls in the prostate, lung, colorectal and ovarian cancer screening trial. J Clin Oncol. 2012;30(22):2768–75.
Resnick MJ, Koyama T, Fan KH, Albertsen PC, Goodman M, Hamilton AS, et al. Long-term functional outcomes after treatment for localized prostate cancer. N Engl J Med. 2013;368(5):436–45.
de Oliveira C, Bremner KE, Ni A, Alibhai SM, Laporte A, Krahn MD. Patient time and out-of-pocket costs for long-term prostate cancer survivors in Ontario, Canada. J Cancer Surviv. 2014;8(1):9–20.
Jayadevappa R, Schwartz JS, Chhatre S, Gallo JJ, Wein AJ, Malkowicz SB. The burden of out-of-pocket and indirect costs of prostate cancer. Prostate. 2010;70(11):1255–64.
Morgans AK, Fan KH, Koyama T, Albertsen PC, Goodman M, Hamilton AS, et al. Influence of age on incident diabetes and cardiovascular disease among prostate cancer survivors receiving androgen deprivation therapy. J Urol. 2014;pii: S0022–5347(14)04835–6.
Daskivich TJ, Fan KH, Koyama T, Albertsen PC, Goodman M, Hamilton AS, et al. Prediction of long-term other-cause mortality in men with early-stage prostate cancer: results from the Prostate Cancer Outcomes Study. Urology. 2015;85(1):92–100.
D'Amico AV, Whittington R, Malkowicz SB, Schultz D, Blank K, et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA. 1998;280(11):969–74.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83.
Loeb S, Sanda MG, Broyles DL, Shin SS, Bangma CH, Wei JT, et al. The Prostate Health Index (phi) selectively identifies clinically-significant prostate cancer. J Urol. 2014;pii: S0022–5347(14)04900–3.
Carlsson S, Maschino A, Schröder F, Bangma C, Steyerberg EW, van der Kwast T, et al. Predictive value of four kallikrein markers for pathologically insignificant compared with aggressive prostate cancer in radical prostatectomy specimens: results from the European Randomized Study of Screening for Prostate Cancer section Rotterdam. Eur Urol. 2013;64(5):693–9.
Nordström T, Vickers A, Assel M, Lilja H, Grönberg H, Eklund M. Comparison between the four-kallikrein panel and Prostate Health Index for predicting prostate cancer. Eur Urol. 2014;pii: S0302–2838(14)00752–0.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Manley, B.J., Andriole, G.L. (2016). History of Prostate-Specific Antigen, from Detection to Overdiagnosis. In: Stone, N., Crawford, E. (eds) The Prostate Cancer Dilemma. Springer, Cham. https://doi.org/10.1007/978-3-319-21485-6_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-21485-6_1
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-21484-9
Online ISBN: 978-3-319-21485-6
eBook Packages: MedicineMedicine (R0)