
Abstract
Purpose
Time and out-of-pocket (OOP) costs can represent a substantial burden for cancer patients but have not been described for long-term cancer survivors. We estimated these costs, their predictors, and their relationship to financial income, among a cohort of long-term prostate cancer (PC) survivors.
Methods
A population-based, community-dwelling, geographically diverse sample of long-term (2–13 years) PC survivors in Ontario, Canada, was identified from the Ontario Cancer Registry and contacted through their referring physicians. We obtained data on demographics, health care resource use, and OOP costs through mailed questionnaires and conducted chart reviews to obtain clinical data. We compared mean annual time and OOP costs (2006 Canadian dollars) across clinical and sociodemographic characteristics and examined the association between costs and four groups of predictors (patient, disease, system, symptom) using two-part regression models.
Results
Patients' (N = 585) mean age was 73 years; 77 % were retired, and 42 % reported total annual incomes less than $40,000. Overall, mean time costs were $838/year and mean OOP costs were $200/year. Although generally low, total costs represented approximately 10 % of income for lower income patients. No demographic variables were associated with costs. Radical prostatectomy, younger age, poor urinary function, current androgen deprivation therapy, and recent diagnosis were significantly associated with increased likelihood of incurring any costs, but only urinary function significantly affected total amount.
Conclusions
Time and OOP costs are modest for most long-term PC survivors but can represent a substantial burden for lower income patients. Even several years after diagnosis, PC-specific treatments and treatment-related dysfunction are associated with increased costs.
Implications for Cancer Survivors
Time and out-of-pocket costs are generally manageable for long-term PC survivors but can be a significant burden mainly for lower income patients. The effects of PC-specific, treatment-related dysfunctions on quality of life can also represent sources of expense for patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Studies have shown that health care costs, including time and out-of-pocket (OOP) costs, represent a substantial financial burden for many patients, even in countries with tax-supported health care systems [1–7]. In some cases, OOP costs may influence the choice of treatment; for example, breast cancer patients of lower socioeconomic status were less likely to use radiotherapy as curative or palliative treatment [8].
Although all Ontario residents have publicly funded health care insurance providing coverage for medically necessary services, including prescription drugs for those aged 65 years and older or with select medical conditions, some services (e.g., allied health, complementary and alternative medicines, and medical equipment) are not covered. Some or all of these costs may be covered under employer-based or privately purchased insurance; otherwise, they must be paid out-of-pocket. Travel and time costs are usually borne by patients and families.
Prostate cancer (PC) is the most common cancer among men in developed countries. Due to early detection and treatment, men may now live for many years after their cancer diagnosis [9]. Long-term survivors continue to experience adverse effects of treatment and may bear ongoing costs of treatment and/or treatment complications. Previously, we estimated the direct medical costs of PC patients in Ontario [10] from the perspective of the payer (Ontario Ministry of Health and Long-Term Care). Government-paid costs can be obtained relatively easily from administrative health care data in Canada [10] and databases such as SEER-Medicare [11] in the USA. These databases are less useful to estimate the costs borne by patients. While there are studies reporting time and OOP costs patients incur while undergoing treatment, few have examined these costs for survivors. Thus, the purpose of this analysis is to estimate and determine predictors of time and OOP costs incurred by long-term PC survivors in Ontario, Canada.
Methods
This study was approved by the Research Ethics Boards of the University of Toronto and University Health Network, Toronto, Ontario. All participants provided written informed consent.
Recruitment
All patients initially diagnosed with PC in 1993–1994, 1997–1998, and 2001–2002 were identified from the Ontario Cancer Registry, a population-based database maintained by Cancer Care Ontario [12]. We selected patients residing in three counties: Toronto and York, representing urban and suburban areas in southern Ontario, respectively, and Sudbury, a city/county in northern Ontario. We included all patients from York (approximately 200/year) and Sudbury (approximately 100/year) and a random selection of 200 patients per year from Toronto; only surviving patients were included in our study. By selecting years of diagnosis over a 10-year period, we sampled patients across the natural history of the disease. Recruitment occurred from January 2004 to October 2006; questionnaires and chart reviews were completed between February 2004 and November 2006.
Using patients' unique cancer registry number, we retrieved their paper pathology records to identify referring physicians. Using contact information obtained from the College of Physicians and Surgeons of Ontario (http://www.cpso.on.ca), we mailed each physician personalized patient letters explaining the study. Physicians were requested to sign the letters, provide patient contact information, and provide consent for us to review charts of consenting patients. Physicians' offices were repeatedly contacted by telephone and/or fax until they indicated their willingness to participate.
Patients were then sent the signed letters, which described the study and provided contact information for the study coordinator. If we did not hear from patients within 10 days after mailing the letters, we telephoned them to enquire about willingness to participate and have their medical chart reviewed. Patients who provided verbal consent were mailed the consent form, a questionnaire booklet, and a stamped addressed envelope for their return. The booklet included a sociodemographic questionnaire, a checklist based on the Charlson comorbidity index [13], a cost questionnaire, and four quality of life instruments including the prostate cancer index (PCI) [14] (results reported elsewhere). Completion of the questionnaires required approximately 50 min. Data obtained from medical charts included tumour grade and stage at diagnosis, PC treatments, and dates of disease progression and metastases.
Data collection
We developed a self-report questionnaire to obtain data on time and OOP costs spent visiting health professionals, OOP costs for medication, equipment, community services, and household help, and time lost from work and leisure, due to PC in the last 3 months [3] (Appendix 1). The questionnaire used simple and clear language; patients could skip questions that did not apply to them. The questionnaire was piloted in five PC patients in an ambulatory clinic at Princess Margaret Hospital, Toronto. Respondents understood the questionnaire and completed it within 20 min without problems. Most patients incurred no prostate cancer-related costs during our initial 3-month recall period. We subsequently increased the recall period to 6 months in an attempt to achieve a more complete costing sample.
Outcome variables
Our main outcomes of interest were time and OOP costs associated with PC care during the previous 6 months. OOP costs included medical costs associated with health professional visits such as diagnostic tests and treatments, and nonmedical costs such as travel, parking, food, and accommodation. OOP costs also included medication and dispensing fees, equipment, home care, and hired household help. We also captured travel time and waiting time for patients and accompanying persons and time lost by patients from chores, paid employment, and leisure. All time for patients and accompanying persons was valued according to the average hourly wages in 2006 in Ontario: $21.75 for males aged <55 years, $18.25 for females aged <55 years, and $22.31 for both sexes aged >55 years, http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/labr69g-eng.htm). We doubled all 6-month costs and times to obtain an estimate of annual costs. All costs were adjusted to 2006 Canadian dollars using the consumer price index for health care from Statistics Canada (http://www40.statcan.gc.ca/l01/cst01/econ09g-eng.htm).
Analysis
Means and standard deviations were calculated to describe continuous numeric variables, while frequencies and percentages were calculated for categorical variables.
Multiple imputation was performed on all variables with missing values so that all patients could be included in the analyses. We used the multivariate imputation by chained equations (MICE) V1.1.0 package in R [15]. Numeric variables were imputed by the predictive mean matching method; categorical variables were imputed by the logistic regression method. Five imputed datasets were generated. Regression analyses were performed on each of the five imputed datasets and results were combined using functions provided in the MICE package. Multiple imputation is prone to bias if the missing data are systematically different from the non-missing or if too few variables are used to predict and replace the missing data [16]. We believe that the data were “missing at random” and thus not a concern for our analysis.
Univariate analysis of variance tests were carried out to determine the individual effects of patient-related variables (demographics, comorbidity), disease-related variables (tumour stage, PC treatments), system-related variables (year of diagnosis, area of residence), and symptom-related variables (PCI urinary, bowel, and sexual function scores) on costs.
Multiple regression analyses were performed by sequentially adding the four groups of predictors into the model and examining the change in the goodness-of-fit of the model to determine the most important groups of cost predictors. Our cost-related outcomes were heavily zero-inflated numeric variables (because some patients reported no costs); therefore, an ordinary least squares regression model would produce biased results. To correct this problem, we used a two-part regression model [17]. Two datasets were generated from the imputed datasets: one included dichotomized cost-related outcomes indicating a zero or non-zero value, while the other included only non-zero values. The first dataset was analyzed using logistic regression, and the second dataset was analyzed using ordinary least squares (OLS) regression. In the logistic model, the independent variables predicted the odds of having a non-zero cost, while in the linear model, the independent variables predicted the amount of the non-zero costs. The log-likelihood and R-squared were reported as measures of goodness-of-fit for the logistic and OLS regressions, respectively. Statistical analyses were performed in R 2.8.0 [18] and SAS 9.1.3 [19].
Results
Cohort characteristics
We identified a stratified, population-derived sample of 1,961 patients who met our inclusion criteria. We were able to locate and send letters to the physicians of 1,323 of those patients. Using the contact information provided by the physicians, we were able to contact 1,109 patients only. Not all patients were interested in participating; 676 returned the questionnaire and we were able to analyze 585 patient responses regarding costs. We do not have information on surviving patients who did not participate as they did not complete the questionnaire. Patients diagnosed in the earlier years were more difficult to locate (their physicians were more likely to be retired or have moved or died). However, age did not seem to be a determining factor for study participation given that the patients in this study were of similar ages to those in previous studies where we recruited patients from a single clinic [20, 21]. Further details regarding the cohort selection can be found in Fig. 1.

Cohort selection process
Respondents' sociodemographic and clinical characteristics are described in Table 1. Patients ranged in age from 43 to 98 years, with a mean age of 73 years. Most were married, retired, and had attended college or university. We asked patients to report annual employment earnings and investment income, using increments of $20,000/year. We then created five categories of total personal income by summing the midpoints of the ranges (these were collapsed for the regression analyses). About 42 % of our sample reported a total annual income below $40,000. The most common treatments for PC were androgen deprivation therapy (ADT) (63 %) and radical prostatectomy (RP) (51 %). Only 3 % of patients had metastatic disease. Scores on the PCI indicated that sexual function (mean = 23.7) was much worse than urinary or bowel function (mean scores = 79.1 and 84.6, respectively)
Overall and subgroup patient costs
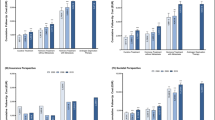
The mean annual time cost was $838 (95 % confidence interval (CI) $442–$1,233), ranging from $0 to $52,386 across individuals. Nearly 30 % of patients incurred no time costs at all, and 75 % reported time costs of $300 or less. Mean OOP costs were $200 (95 % CI $109–$290) and ranged from $0 (43 % of patients) to $20,760.
Table 2 reports mean costs by patient subgroups. Few of the differences in mean costs between patients of different characteristics were statistically significant. Most demographic variables did not significantly affect costs. In general, costs decreased with age; however, OOP costs were highest for the youngest and oldest age groups (p = 0.03). Patients who had undergone radiation therapy (RT) had lower time and total costs than those who had not (p ≤ 0.05). Patients who had received previous ADT had significantly higher OOP costs than those currently receiving ADT or those that had never received it (p = 0.03). Patients with metastatic disease incurred high time costs (mean = $3,159) and total costs ($3,333) compared to non-metastatic patients (p < 0.05). The most significant findings with respect to predictors of cost (p < 0.001) were higher costs in patients with poor urinary and bowel function.
Patient characteristics associated with time, out-of-pocket, and total costs
Time costs
Younger patients were more likely to incur time costs, but age had no significant effect on the amount incurred, among those with any costs (Table 3). Patients with recent diagnosis, no RP, any ADT, and worse urinary and sexual functions had a higher likelihood of incurring any time costs. For those patients with time costs, having metastatic disease, and worse urinary function were associated with significantly higher costs (Table 3).
OOP costs
A later cancer diagnosis, no previous RP, and worse urinary function were associated with a higher likelihood of incurring any OOP costs (Table 4). For patients that paid OOP costs, the amount increased for those that had past ADT and poor bowel function (Table 4).
Total costs
Younger patients, no previous RP, current ADT, earlier year of diagnosis, and worse urinary function were associated with increased likelihood of incurring costs (Table 5). Among patients that incurred costs, worse urinary function was associated with higher total amounts (Table 5).
Discussion
Direct medical costs for PC can be considerable and are highest after diagnosis and before death [10]; however, understanding the total economic burden also requires estimating patient-borne time and OOP costs. Time costs are rarely measured systematically [6], while OOP costs are seldom considered but frequently affect the well-being of cancer survivors [22]. Both types of costs can represent a considerable burden to patients.
At the time the questionnaire was administered, our cohort of patients was not dealing with initial cancer treatment but rather its sequelae. The time and OOP costs these patients incurred were generally low. However, for approximately 16 % of patients with an annual income below $20,000, PC-related time and OOP costs could represent 10.4 % of their income (assuming $10,000 average income); for patients in the $20,000–$39,000 range (25 % of patients), this burden would be 3.5 %. This burden decreased to 2.1 % and 0.2 % of income for patients in the $40,000–$59,000 and $100,000–$150,000 intervals, respectively. Thus, costs varied widely among individuals, from none to extremely high costs.
Our results were qualitatively similar to previous research. We found higher total health care expenses among younger patients [2], metastatic patients, and those who underwent RP [10] and lower costs in patients with better urinary function [23]. We also found that current androgen deprivation therapy and recent diagnosis were significantly associated with the likelihood of incurring any costs. However, unlike previous studies, we found no significant association between costs and area of residence [4] or comorbidity [10]. Quantitatively, our 12-month time costs are high compared to those from the USA ($1,194 vs. $341 and $270 vs. $187 for RP and RT patients, respectively) [23]; this is likely due to sample differences (our sample is older) and the use of different wage rates to value time, which do not enable a valid comparison. (Our wage rates were obtained from Statistics Canada and are in 2006 CAD; the wage rates from the US study were obtained from patients' self-reported individual income and standardized to 2009 USD.) However, our OOP cost estimates are low ($183 vs. $416 and $223 vs. $587 for RP and RT patients, respectively), even after inflation and adjusting to 2009 USD, perhaps because American patients pay for co-payments, premiums, and services not fully covered by insurance. Furthermore, our overall OOP cost estimate ($200/year) is very low compared with a monthly (30-day) OOP cost estimate of $213 for patients with prostate, breast, colorectal, and lung cancers reported by another Canadian study [1]. However, unlike our sample of long-term community-dwelling PC survivors, these patients were recruited from hospital clinics and were all receiving active treatment at the time of the survey, which would explain the higher value of costs incurred.
Previous research has shown that PC treatment-related sexual and urinary adverse effects persist up to 10 years post-diagnosis [24] and significantly affect quality of life [25, 26]. Our study indicated that poor quality of life, in terms of urinary, bowel, and sexual functions, may also be associated with higher costs. The observation that RP, with long-term side effects including incontinence and erectile dysfunction, was also associated with higher costs reinforces this finding. One study in the USA also found that these factors, and urinary and sexual bother, were inversely related to OOP and indirect costs [23]. Another study reported an association between higher quality of life scores and lower medical expenses among PC patients in Lithuania, a country with a government-sponsored health care system similar to Canada's [27]. Causal relationships cannot be determined from these associations using cross-sectional data, but patients with worse urinary, bowel, or sexual function would require doctor visits, medication, supplies such incontinence pads, and lose leisure time to deal with their problems.
The main strength of our study was our population-based sample of community-dwelling, long-term survivors of PC residing in three geographically diverse areas of a large province in Canada. This type of cohort has rarely been examined in the literature. Our main limitation concerns the self-reported nature of the data. We used a self-administered questionnaire with a relatively long recall period and assumed the 6-month period reported also represented the previous one in calculating annual costs. Some authors believe self-administered questionnaires can lead to low levels of adherence, suggesting interviews, in person or by telephone, as a preferred method to obtain data on expenses [28]. Yet, self-administered surveys can be filled out in the comfort of patients' homes with access to receipts and appointment books.
Approximately 40 to 50 patients (7 % to 8.5 %) did not answer one or more of the questions on the use of services. These data are probably missing because patients could not remember the amount of money or time they had spent and not due to the fact that questions were too personal or sensitive. There was no evidence from the patterns of missing data that patients found the questionnaire to be too long and stopped answering the questions.
Another potential concern is the sample size. Although we identified 1,961 eligible patients for this study, ultimately only 30 % returned completed questionnaires and had their medical charts reviewed and thus were included in this analysis. The main reason for the high attrition rate was that we could not locate patients or their referring physicians so many years after the original cancer diagnosis. As with any voluntary research study, the final sample of consenting survivors may have been biased towards patients who were healthier and more satisfied with treatment.
While we asked patients to report specifically about PC-related health care only, some may have reported costs associated with comorbid conditions. In some cases, it may be difficult to determine the true reason for expenses; for example, equipment for orthopedic problems may be due to PC metastases which limit mobility. Other limitations include missing data, namely PCI sexual, urinary, and bowel function questions, and the uncertainty about precise income values (calculated from two income variables, both of which had broad ranges). Finally, cancer stage at diagnosis was not available; thus, we cannot ascertain how it might have affect costs.
PC is the most common cancer among men in developed countries and has a long survivorship period. To have a full understanding of the economic impact of PC, one must consider the costs to patients and society at large. While studies have examined these costs for patients undergoing treatment, few have examined the long-term financial implications of cancer and its treatment. Our findings suggest that time and OOP costs are generally manageable for long-term PC survivors but can be a significant burden mainly for lower income patients. Furthermore, while many studies have documented the effects of PC-specific treatment-related dysfunctions on quality of life [25], our study showed that these also represent sources of expense for patients. Our study indicates that these associations merit further research to determine causal relationships.
References
Longo CJ, Fitch M, Deber RB, Williams AP. Financial and family burden associated with cancer treatment in Ontario, Canada. Support Care Cancer. 2006;14:1077–85.
Longo CJ, Deber R, Fitch M, Williams P, DeSouza D. An examination of cancer patients' monthly “out-of-pocket” costs in Ontario. Eur J Cancer Care. 2007;16:500–7.
Federico CA, Hsu PC, Krajden M, Yoshida EM, Bremner KE, Weiss AA, et al. Patient time costs and out-of-pocket costs in hepatitis C. Liver Int. 2012;32(5):815–25.
Mathews M, West R, Buehler S. How important are out-of-pocket costs to rural patients' cancer care decisions? Can J Rural Med. 2009;14(2):54–60.
Langa KM, Fendrick AM, Chernew ME, Kabeto MU, Paisley KL, Hayman JA. Out-of-pocket health-care expenditures among older Americans with cancer. Value Health. 2004;7(2):186–94.
Yabroff KR, Warren JL, Knopf K, Davis WW, Brown ML. Estimating patient time costs associated with colorectal cancer care. Med Care. 2005;43(7):640–8.
Yabroff KR, Kim Y. Time costs associated with informal care giving for cancer survivors. Cancer. 2009;115(18 Suppl):4362–73.
Huang J, Zhou S, Groome P, Tyldesley S, Zhang-Solomans J, Mackillop WJ. Factors affecting the use of palliative radiotherapy in Ontario. J Clin Oncol. 2001;19(1):137–44.
Ferlay J, Shin H-R, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–917.
Krahn MD, Zagorski B, Laporte A, Alibhai SMH, Bremner KE, Tomlinson G, et al. Healthcare costs associated with prostate cancer: estimates from a population-based study. Br J Urol Int. 2010;105(3):338–40.
Warren JL, Klabunde CN, Schrag D, Bach PB, Riley GF. Overview of the SEER-medicare data. Content, research applications, and generalizability to the United States elderly population. Med Care. 2002;40(8, Supplement):IV-3–18.
Hall S, Schulze K, Groome P, McKillop W, Holowaty E. Using cancer registry data for survival studies: the example of the Ontario cancer registry. J Clin Epidemiol. 2006;59:67–76.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis. 1987;40:373–83.
Litwin MS, Hays RD, Fink A, et al. The UCLA prostate cancer index: development, reliability, and validity of a health-related quality of life measure. Med Care. 1998;36:1002–12.
Van Buuren S, Oudshoorn CGM. Flexible multivariate imputation by MICE. Leiden: TNO Preventie en Gezondheid, TNO/VGZ/PG 99.054, 1999.
Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. Br Med J. 2009;338:b2393.
Jones AM, Rice N, Bago d’Uva T, Balia S. Applied health economics. London: Routledge; 2007.
R Development Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing Vienna, Austria.
SAS Inc. SAS 9.1.3 for Windows. Cary, N.C., USA.
Krahn M, Bremner KE, Tomlinson G, Ritvo P, Irvine J, Naglie G. Responsiveness of disease-specific and generic utility instruments in prostate cancer patients. Qualily Life Res. 2007;16:509–22.
Krahn MD, Ritvo P, Irvine J, Tomlinson G, Bremner KE, Bezjak A, et al. Patient and community preferences for outcomes in prostate cancer: implications for clinical policy. Med Care. 2003;41:153–64.
Pisu M, Azuero A, McNees P, Burkhardt J, Benz R, Meneses K. The out of pocket cost of breast cancer survivors: a review. J Cancer Survivorship. 2010;4(3):202–9.
Jayadevappa R, Schwartz JS, Chhatre S, Gallo JJ, Wein AJ, Malkowicz SB. The burden of out-of-pocket and indirect costs of prostate cancer. Prostate. 2010;70(11):1255–64.
Taylor AKL, Luta G, Miller AB, Church TR, Kelly SP, Muenz LR, et al. Long-term disease-specific functioning among prostate cancer survivors and noncancer controls in the prostate, lung, colorectal, and ovarian cancer screening trial. J Clin Oncol. 2012;30(22):2768–75.
Krahn MD, Bremner KE, Alibhai SMH, Ni A, Tomlinson G, Laporte A, Naglie G. A reference set of health utilities for long-term survivors of prostate cancer: population-based data from Ontario, Canada. Quality of Life Research. 2013. doi:10.1177/0272989X13493970.
Yabroff KR, Lawrence WF, Clauser S, Davis WW, Brown ML. Burden of illness in cancer survivors: findings from a population-based national sample. J Natl Cancer Inst. 2004;96(17):1322–30.
Mickevičienė A, Vanagas G, Ulys A, Jievaltas M, Smailytė G, Padaiga Ž. Factors affecting health-related quality of life in prostate cancer patients. Scan J Urol Nephrol. 2012;46(3):180–7.
Lauzier S, Maunsell E, Drolet M, Coyle D, Hébert-Croteau N. Validity of information obtained from a method for estimating cancer costs from the perspective of patients and caregivers. Qual Life Res. 2010;19(2):177–89.
Acknowledgments
This work was supported by a project grant from the Canadian Institutes for Health Research (CIHR, #53114), an Investigator Award from the CIHR (Dr. Krahn), the F. Norman Hughes Chair in Pharmacoeconomics (Dr. Krahn), and a Research Scientist Award from the National Cancer Institute of Canada (Dr. Alibhai).
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 79 kb)
Rights and permissions
About this article
Cite this article
de Oliveira, C., Bremner, K.E., Ni, A. et al. Patient time and out-of-pocket costs for long-term prostate cancer survivors in Ontario, Canada. J Cancer Surviv 8, 9–20 (2014). https://doi.org/10.1007/s11764-013-0305-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-013-0305-7