
Abstract
This chapter presents an overview of the role of digital pathology in medicine. After a brief history and background review, this chapter explains how the introduction of digital pathology revolutionized the teaching of pathology among medical students and residents and how it provided new opportunities to share images with remote colleagues for research, tumor boards and clinical activities such as frozen sections, consultations and quality assurance. The different technologies used in digital pathology are presented. They range from static images to whole-slide imaging and hybrid technologies. New usages using mobile devices are also presented. This chapter discusses also how digital pathology may help to improve health care in academic centers, remote hospitals, large cities and developing countries. It also deals with factors affecting the development of clinical telepathology, including technological and human barriers as well as legal, organizational and licensure issues.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Digital pathology
- Education
- Research
- Clinical
- Frozen sections
- Telepathology
- Whole-slide images
- Virtual image
- Barrier
- Facilitator
Introduction and Historical Background
Digital pathology (DP) has been implemented around the world mostly for education, clinical pathological conferences, quality control and research. Its introduction into diagnostic activities such as intraoperative consultations (frozen sections) and expert opinions (secondary consultation) is increasing steadily. The adoption for primary diagnoses and telepathology on a routine clinical basis is also increasing but at a slower pace. The College of American Pathologists (CAP) defines telepathology as “… the practice of pathology, in which the pathologist views digitized or analog video or still image(s), and renders an interpretation that is included in a formal diagnostic report or documented in the patient record” [1]. Prior to 1990, different experiences using either static image or dynamic-robotic telepathology systems were independently attempted to provide diagnostic services. Dr. Ronald Weinstein was the very first pathologist to experience telepathology as part of a multiservice between the Logan Airport and the Massachusetts General Hospital in 1968 using an analog technology [1, 2]. In 1986, a telepathology system combining a color video and a robotic microscope was used successfully between El Paso, TX and Washington, DC. This same year, the term telepathology was introduced [2]. In Europe, the very first telepathology experience for frozen sections was performed in Norway, using a dual static/dynamic system between two cities situated 420 km apart [3]. Since then, telepathology has been developed primarily to provide diagnostic service to remote regions experiencing a shortage of pathologists or to support sites in the third world, mostly in Africa, [4]. The 1990s was a decade of major digital technological breakthroughs with, for example, the introduction of automated slide scanners with image analysis algorithms for cervical cytology smears screening [5]. 1990s and 2000s were decades of intensive development of international teleconsultation platforms. The most popular were the AFIP system in Bethesda, USA, the iPATH in Basels, Switzerland, and the UICC-TPCC in Berlin [6]. More recently, an international Virtual Pathology Institute (VPI) has been created in Germany [6], a DP consultation portal (https://pathconsult.upmc.com/) has also been developed at the University of Pittsburgh Medical Center [7] as have similar brokered consultation services offered through DP companies and, in 2011, the European telepathology forum called Medical Electronic Consultation Expert System (MECES) was launched, taking advantage of the experiences of iPATH and UICC-TPCC in combination [5]. Important improvements in the quality of the images and reduced scanning times have become available in the 2000s. Since the introduction of this technology, a large number of studies clearly demonstrated that the quality of the virtual images were not inferior to the microscope [8], which paved the way to the expansion of telepathology for clinical use. Canada has been a leader in the development of patient-centered telepathology networks [9, 10], in good part because of the geographical challenges but also thanks to the initiative of a few leading pathologists and the availability of public financial support. New algorithms using the digital technology such as those allowing quantitative analysis of immunohistochemical cancer markers for estrogen receptor, progesterone receptor and HER2 were also developed in the 2000s [5]. Finally, the 1990s and 2000s are the decades of development of national and international Societies and Meetings focusing on DP. In 1992 the first European conference on telepathology took place in Heidelberg and the first international meeting on telemedicine in Tromso, Norway [5]. Later, several societies and companion meetings were created namely Pathology Visions (originally under the sponsorship of Aperio, and later the Digital Pathology Association), the International Academy of Digital Pathology, the European Congress on Digital Pathology, European Congress on Telepathology and International Congress on Virtual Microscopy, to name only a few of them.
Out of all this, several critical roles can be seen emerging in medicine. Herewith we summarize the key points of each of these.
Applications of Digital Pathology
Education
DP has made a profound impact in medical education at all levels. This began with activity from many institutions looking for ways to exploit this new technology to their advantage. As computer networks and laptop computers became more commonplace, the need for floor-space-occupying microscopy labs held at fixed times and using glass slides in varying states of cleanliness and completeness was viewed as less and less of a priority. The shift from glass to virtual slides or whole-slide images (WSI) in basic histology and pathology courses in medical, dental, veterinary and other health sciences has been dramatic and is nearly complete. Since Fred Dee reviewed the landscape in 2009 [11], the pace of the transition has not abated. Current US medical school graduates entering pathology training almost uniformly have been tutored using digital rather than glass slides, and an increasing number of international graduates as well as trainees in other disciplines. The transition has been accelerated by several factors highlighted in Table 3.1.
In the post-graduate realm, WSI have many advantages as well, such as in the creation of teaching libraries, documentation of resident competencies, and hastening skill acquisition in slide examination [12–15]. Training residents in specific disciplines, stain interpretation and other activities are enhanced with this tool [15]. WSI also offer the same access advantages to programs with multiple sites of resident activity and teaching conferences at a single site.
Post-graduate medical education paradigms are also enhanced and altered by the ready adoption of WSI. On-line slide libraries are useful to students, residents and practitioners alike (see https://digitalpathologyassociation.org/whole-slide-imaging-repository for comprehensive listing). WSI are extensively used by certifying boards in the US and elsewhere, further indicating the utility of these in the educational assessment realm. Furthermore, several journals have added WSI access capabilities to their publications to enhance learning [16] and research value.
Research
DP brings a new set of tools to the research realm. From the studying of the fundamental manner in which a diagnosis is determined to extracting new lines of data from multispectral analysis of imaged slides, DP is yielding a rich array of new knowledge. The adoption of DP for just conventional veterinary microscopy has had a profound impact on pharmaceutical work by allowing the electronic linkage of study sites and expertise, supplanting the need for moving people or samples between data collection centers. The quantitative image analysis tools that can be applied to digital images have further expanded the field and entered routine clinical care in many niches. Image search algorithms, rare event identification routines, stain quantization and similar options all now combine to offer the researcher using tissue analyses a new armamentarium.
Tumor Boards and Patient Education
Multidisciplinary patient conferences such as tumor boards benefit from inclusion of pathology materials, in the form of digital slides, accessed live in much the same manner that radiologic imaging or endoscopic data is often reviewed in these settings [17, 18]. Some technologic barriers, such as loading speeds still can pose a challenge in some fast moving conferences, but the ability to visually demonstrate microscopic anatomy and relationships in these settings enhances team-based care and builds confidence in the pathologist, as shown in Table 3.2. Likewise, digital slides open the opportunity for inclusion of links to these in patient reports which can either be shown directly to the patient, or accessed in a virtual conference format. Some evidence suggests that these kinds of educational efforts improve patient compliance and outcomes (J. Hunt, personal communication.)
Clinical Work
The penetration of DP into day to day clinical care of patients has no doubt been slower than device manufacturers would have hoped, impeded by some of the regulatory barriers, and the variations in the degree to which economic or workflow advantages have been demonstrated or apply to a given setting. Food and Drug Administration (FDA) approval of various quantification algorithms for prognostic marker reporting has allowed this DP tool to become standard practice in most clinical centers. In some settings such as consultation with disseminated specialists (e.g. Clarient’s model, see http://www.clarientinc.com/about-us/clarient-pathology-services.aspx, accessed 4 Nov 2014), DP is also routine. Opening timely access to remote technical services for immunohistochemistry (IHC) or other specialized stains has been similarly readily adopted as a DP business solution. A similar early adoption scenario has been followed for frozen section coverage of sites not continuously staffed by an on-site pathologist [19]. These now form the foundation on which telepathology using WSI is now practiced in several locations [20]. Practice guidelines for telepathology and validation guidelines for the use of WSI now exist to guide broader adoption [21–23], in advance of regulatory approval for primary diagnosis in the US though such approval does exist for Canada [23, 24]. Several compelling use cases also exist for cytopathology [25].
Technologies
Static (Store and Forward) Image Telepathology
Static image telepathology means the capture and storage of still images, whether microscopic or macroscopic, using either a microscope or a macroscopic platform with transmission of the captured images to a remote recipient. This is the most simple and certainly the cheapest modality to transmit images. Despite these clear advantages, only part of the whole slide is captured and the major limitation is the representativeness of the captured field which is dependent on the operator. Advantages and disadvantages of this form of telepathology are presented in Table 3.3.
Streaming/Dynamic/Robotic
Streaming telepathology represents the live transmission of images from a microscope or a macroscopic platform using a digital streaming camera (such as a static digital camera with streaming software or a digital video camera). A voice connection such as via telephone or teleconferencing may allow a live communication between the referring and the consulting individuals. The streaming image can be either controlled by the referring personnel with a standard microscope equipped with a digital camera or by the receiving observer with the use of a robotic microscope. Streaming telepathology may be more labor intensive than WSI, especially with the use of a robotic microscope, but recent experience shows that in certain situations, it may be somewhat faster because it skips the intermediary scanning step. In a setting of reasonable bandwidth and transmission speeds, the ready availability of screen-sharing tools may make this also the most economical option. The possibility of performing up-and-down focusing is also viewed as a major advantage in certain subspecialties such as microbiology, cytology and haematology. Dynamic telepathology appears as the mode of choice for providing immediate adequacy assessment of cytology specimens by telecytology [7]. Advantages and disadvantages of this technology are presented in Table 3.3.
Whole-Slide Images
WSI involves the use of an automated microscopic glass slide scanner that captures serial images from the entire specimen on a microscope glass slide which are ‘stitched’ together to create a virtual image . This image is then stored and can be viewed remotely via an image management software. Whole slide imaging is a complex telepathology solution but presents numerous advantages listed in Table 3.3. At this point in time, WSI appears to be the most promising modality for most applications in the anatomic pathology laboratory [21]. Extensive literature is available on the reliability of WSI for major clinical activities such as intraoperative consultations (frozen sections) [10, 26–28], secondary consultations [10, 29–31] and primary routine pathology work [8, 9, 20, 32].
Hybrid Multi-modality Telepathology Systems
Recently, despite the increasing use of WSI for clinical applications, there has been a re-emergence of interest at using dynamic-robotic telepathology systems, in part, to circumvent the lack of real-time up-and-down focusing using the WSI technology and possibly also concern over delayed FDA approval of WSI for primary diagnosis. In most if not all hybrid systems, a low magnification image is captured and forwarded to the telepathologist who, after examination of the image, uses a live telecommunications link to view areas of interest at higher magnification [33]. It is worth noting that early telepathology systems used in the 1990s were in fact examples of ‘hybrid’ multi-modality telepathology systems [2]. WSI uses the Z-stacks technology , which provides multiple images at different levels, to compensate for the lack of real-time focusing capabilities. The major disadvantages of this technology are the significantly increased scanning time required, the huge size of images and the frequent need to rescan the slide to obtain the needed level of interest. Hybrid telepathology systems combine static and dynamic technologies and, therefore, real-time focus adjustments are provided by the dynamic-robotic telepathology module. The major advantages over WSI are the shorter turnaround time needed to render an urgent diagnosis, for example in the case of a frozen section, and the possibility of live up-and-down focusing on specific areas where cell aggregates are present, such as in many cytopathology specimens.
Mobile Devices
Smartphones and other mobile devices offer a great potential to perform telepathology because they are relatively cheap compared to commercial slide scanners, they are portable, provide internet connectivity, possess excellent digital cameras and can be easily attached to a microscope. The University of Pittsburgh Medical Center recently launched an application to be used with the iPhone which provides a solution to submit DP images for expert opinion and to incorporate a diagnostic report into this web-based application [34].
Recently, the Food and Drug Administration has approved such an application for use with radiologic images [35]. Image fidelity and resolution makes the iPad potentially suitable for WSI evaluation of frozen sections or consultations. Current literature shows that the accuracy of frozen section interpretation is acceptable but difficulties with slide navigation at high magnification causes frustration leading to an increased risk of diagnostic errors and is viewed as one of the major obstacles to a more widespread use [35].
Target Population for use of Digital Pathology
Academic Centers
DP clearly resonates with the mission of the academic center on all three fronts, education, research and clinical care. As noted above, DP enhances the educational capability of the center for undergraduate, graduate and post-graduate audiences. DP expands the toolbox for researchers in academia, whether they are working on a basic science issue studying expression of characteristics on the cellular or sub-cellular level, or seeking translational data using tissue materials, or studying the outcomes of a category of patients enrolled in a clinical trial. On the clinical care realm, DP clearly offers a solution for getting diagnostic samples to the right sub-specialist consultant quickly and efficiently, whether for initial evaluation or in consultation after first viewing [19]. Clinical care conferences, which at academic centers abound, as noted above are also enhanced by use of DP, and simplify the movements of people and information.
Remote Hospitals
Access to care is the major challenge for residents in rural or remote areas, and usually this is due to the difficulty in retaining specialists, or even enough primary care-givers in the community. In Canada, for example, lack of access to pathologist frozen section support has been often cited as a reason a surgeon does not wish to practice in a small hospital [36]. The uneven quality of diagnostic services in these areas so highly dependent on the quality of a single practitioner is also problematic. Engagement in a DP-network and other networks can be part of an excellent solution for rural hospitals on the tissue and microscopic diagnosis front, as it can be in the general lab realm. In these settings the utility of DP is not limited to surgical pathology but also often needs to include other aspects of microscopy [37]. Application of DP and telehealth tools generally has been a long-term priority of the US military system in recognition of the value of this approach [38, 39].
Large Cities
Access to optimal care is often not a problem limited to rural or remote settings. As hospital or healthcare systems expand their reach and offer services in more decentralized ways, one not uncommonly encounters the demand for specialized services (frozen sections, especially) in low volume settings which would be wasteful of a full-time pathologist, or settings where sub-specialist support of a general pathologist would offer better quality care [40]. This movement towards “point of care” pathology cannot be accomplished without the benefits of DP. Such settings also underscore the need for low cost scanners or other imaging tools of varying capacity or throughput that can be deployed across the system to facilitate image exchange and consultation.
Developing Countries
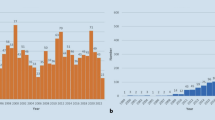
Access to care is THE problem in developing countries, stemming not just from economic disparities, but also to lack of specialists, technical and professional training opportunities, and to healthcare and social or governmental infrastructure. In any comprehensive evaluation of the solutions to this issue, the particulars may vary somewhat between locations, but engagement in a DP network is at least a part of the solution [41–45]. The accompanying figure demonstrates the dramatic difference in distribution of pathologist subspecialists in various countries of the world, and highlights a great disparity that DP can begin to bridge. Charitable, humanitarian and for-profit ventures are in progress to address or exploit these disparities (Fig. 3.1).

Distribution of pathologists and proportion of subspecialist pathologists
Barriers and Facilitators to Implementation
Despite overwhelming advantages to the use of DP for clinical use, several barriers to a more widespread adoption of the technology have been repeatedly reported [1, 5]. Evaluation studies identified technological, organizational and human factors to explain the relative resistance of pathologists, surgeons and technicians to use telepathology. Human factors remain however among the most important challenges [46]. For one thing, since glass slides are still available, many pathologists are reluctant to abandon their comfort zone and prefer to keep using the microscope. Furthermore, surgeons hesitate to trust pathologists whom they know little and, conversely, pathologists can have reservations to work with technicians they do not know. Success relies on efficient change management strategies including close tutorship and a highly coordinated effort between medical, laboratory staff, biomedical, administrative and IT support teams working on different sites. Despite all those supportive efforts, it is clear that telepathology also requires pathologists and surgeons to change their work practices, and to develop mutual confidence between distant technologists, pathologists and surgeons. The recently released guidelines on whole slide imaging validation for diagnostic purposes by the College of American Pathologists [23] and of national guidelines such as those of the Canadian Association of Pathologists [21], the Royal College of Pathologists [47] and The American Telemedicine Association [22] are among the strategies aimed at encouraging wider adoption of the technology by the world pathology community.
However, additional technological improvements are also needed to reach this goal. It is clear that the technology has not reached the same level of maturity as teleradiology, mainly with regard to software application ergonomics, more specifically to the speed and the ease of user interfaces that are often seen are inadequate [2, 12]. Furthermore, most commercially available DP solutions cannot be easily integrated with local laboratory information systems making their use laborious. Archiving and image retrieval is also an important challenge because of the size of digital images. Finally, difficulties at clearly visualizing micro-organisms and the need to rescan a fair number of slides for varying technical reasons [48] represent other barriers to a more widespread use of the technology in the routine practice. Technological advances in DP have however been significant in recent years and recent experiences confirm that pathologists are increasingly comfortable with the use of the technology [9].
Legal and Licensure Issues
Regulatory issues have been a major psychological and financial barrier to DP, drawing so much attention that scientific and organizational advances have seemed to pause [49–51]. No scanners or systems to produce WSI have been FDA approved for use as a tool for primary (initial) diagnosis. But this FDA stance, designating these devices as Class III (high risk, no comparable device) [52] has been challenged by many DP advocates as too restrictive for a tool used by licensed physicians to make a medical diagnosis. Canadian regulators classified the devices as Class II [24], and regulatory approval was obtained by three manufacturers in 2014. Indeed the FDA stance does not preclude pathologists from validating their planned use and proceeding to use WSI “off-label.” The College of American Pathologists has issued guidelines for this purpose [23]. The FDA only governs what claims the manufacturer can make in marketing their device, though in the past, the FDA has attempted to leverage vendors ability to sell to sites they had reason to believe were going to use a product for clinical off-label purposes. Scanning systems and imaging algorithms have been FDA approved for ER, PR, and Her2 scoring [53].
Centers for Medicare and Medicaid Services (CMS) and other payers in the US have not taken a position on WSI relative to reimbursement, aside from their stance on other technologies or tools that require a laboratory to validate their use prior to patient reporting and billing for services. In certain Canadian provinces, reimbursement issues have been successfully negotiated with the pathologists community [46].
Telepathology also raises unique liability issues because of its capability to transcend jurisdictions. Physician multi-jurisdictional licensure is a major issue in the United States where pathologists may be involved in several states requiring a different license. It is also an issue in other federal countries such as Canada and in unions of independent countries such as the European Union [54]. The ability of DP to allow the distant separation of the patient, the patient sample and the diagnostic images raises physician licensure issues similar to those encountered when digital radiology services began to offer round-the-clock interpretation from physicians located oceans away from the patient [55]. The general standard has been that the physician must be licensed in the location (state) where the patient is being treated. But a similar requirement is not mandated for a consultant rendering a subsequent opinion on a sample. As DP service systems begin to grow and offer much wider (initial) access to sub-specialist diagnosticians, no doubt the role of state licensure boards in assuring quality of care will come under pressure to streamline the scrutiny. The current existence of national practitioner databanks for adverse events may be the precursor of nation-wide licensure in the US. A much broader query about this issue arises in the matter of international consultation, reimbursement and licensure, a matter which is likely to undergo transition as the practices become more wide-spread.
Organizational Issues
Many aspects of DP require high levels of organization and infrastructure, particularly in informatics. The generation of a high volume, data-dense information stream from pathology imaging poses a storage and integration challenge in order to optimize the value of DP to clinical medicine, or other endeavors. Critical decisions about system and storage/viewing organization have long term implications and should be made with these considerations in mind. Device and data integration however are not the only issues as workflow, and conventional histology production must also be optimized to enable a successful transition to DP adoption, even on a limited scale [38, 56]. Workspace design and user interface issues must be addressed as well.
One difficulty at establishing a telepathology network in jurisdictions with a public health care system such as in Canada and the European Union is to bridge the gap between the need to offer consistent pathology coverage in a region and the necessity for each institution to prioritize its own in-house cases and to meet pre-defined turnaround times. Several factors such as tradition of practice, institutional regulations, shortage of pathologists and the lack of financial incentives to read distant cases, are among the major barriers to the development of such integration but the affordances of telepathology will force healthcare networks around the world to redefine the routing of surgical pathology cases and adopt a more integrated and comprehensive pathology coverage. These kinds of issues mandate the casting of a broad net of stakeholders when contemplating a project so that benefits and costs that accrue and are incurred asymmetrically can be managed successfully. Aligning competing interests in this way can predict success where otherwise a stalemate would be the result.
References
Williams S, Henricks WH, Becich MJ, Toscano M, Carter AB. Telepathology for patient care: what am I getting myself into? Adv Anat Pathol. 2010;17(2):130–49.
Weinstein RS, Graham AR, Lian F, Braunhut BL, Barker GR, Krupinski EA, et al. Reconciliation of diverse telepathology system designs. Historic issues and implications for emerging markets and new applications. APMIS. 2012;120(4):256–75.
Nordrum I, Engum B, Rinde E, Finseth A, Ericsson H, Kearney M, et al. Remote frozen section service: a telepathology project in Northern Norway. Hum Pathol. 1991;22(6):514–8.
Hitchcock CL. The future of telepathology for the developing world. Arch Pathol Lab Med. 2011;135(2):211–4.
Park S, Parwani AV, Aller RD, Banach L, Becich MJ, Borkenfeld S, et al. The history of pathology informatics: a global perspective. J Pathol Inform. 2013;4:7.
Kayser K, Borkenfeld S, Djenouni A, Kayser G. History and structures of telecommunication in pathology, focusing on open access platforms. Diagn Pathol. 2011;6:110.
Pantanowitz L, Wiley CA, Demetris A, Lesniak A, Ahmed I, Cable W, et al. Experience with multimodality telepathology at the University of Pittsburgh Medical Center. J Pathol Inform. 2012;3:45.
Bauer TW, Schoenfield L, Slaw RJ, Yerian L, Sun Z, Henricks WH. Validation of whole slide imaging for primary diagnosis in surgical pathology. Arch Pathol Lab Med. 2013;137(4):518–24.
Evans AJ, Perez-Ordonez B, Asa SL. Primary diagnosis by whole slide imaging (WSI) telepathology: University health network (UHN) goes live. Lab Investig. 2014;94:399A.
Perron E, Louahlia S, Nadeau L, Boilard F, Ing M, Orain M, et al. Telepathology for intraoperative consultations and expert opinions: the experience of the eastern Quebec telepathology network. Arch Pathol Lab Med. 2014;138(9):1223–8.
Dee FR. Virtual microscopy in pathology education. Hum Pathol. 2009;40(8):1112–21.
Pantanowitz L, Valenstein PN, Evans AJ, Kaplan KJ, Pfeifer JD, Wilbur DC, et al. Review of the current state of whole slide imaging in pathology. J Pathol Inform. 2011;2:36.
Bruch LA, De Young BR, Kreiter CD, Haugen TH, Leaven TC, Dee FR. Competency assessment of residents in surgical pathology using virtual microscopy. Hum Pathol. 2009;40(8):1122–8.
Hassell LA, Fung KM, Chaser B. Digital slides and ACGME resident competencies in anatomic pathology: an altered paradigm for acquisition and assessment. J Pathol Inform. 2011;2:27.
Li L, Dangott BJ, Parwani AV. Development and use of a genitourinary pathology digital teaching set for trainee education. J Pathol Inform. 2010;1:2.
Cagle PT, Glassy EF. Whole slide images add value to journal article figures. Arch Pathol Lab Med. 2014;138(5):592.
Tecotzky R. Digital pathology enhances hospital’s tumor board meetings. MLO Med Lab Obs. 2009;41(11):60.
Chen ZW, Kohan J, Perkins SL, Hussong JW, Salama ME. Web-based oil immersion whole slide imaging increases efficiency and clinical team satisfaction in hematopathology tumor board. J Pathol Inform. 2014;5:41.
Evans AJ, Chetty R, Clarke BA, Croul S, Ghazarian DM, Kiehl TR, et al. Primary frozen section diagnosis by robotic microscopy and virtual slide telepathology: the University Health Network experience. Semin Diagn Pathol. 2009;26(4):165–76.
Thorstenson S, Molin J, Lundstrom C. Implementation of large-scale routine diagnostics using whole slide imaging in Sweden: digital pathology experiences 2006-2013. J Pathol Inform. 2014;5:14.
Bernard C, Chandrakanth SA, Cornell IS, Dalton J, Evans A, Garcia BM, et al. Guidelines from the Canadian Association of Pathologists for establishing a telepathology service for anatomic pathology using whole-slide imaging. J Pathol Inform. 2014;5:15.
Pantanowitz L, Dickinson K, Evans AJ, Hassell LA, Henricks WH, Lennerz JK, et al. American Telemedicine Association clinical guidelines for telepathology. J Pathol Inform. 2014;5:39.
Pantanowitz L, Sinard JH, Henricks WH, Fatheree LA, Carter AB, Contis L, et al. Validating whole slide imaging for diagnostic purposes in pathology: guideline from the College of American Pathologists Pathology and Laboratory Quality Center. Arch Pathol Lab Med. 2013;137(12):1710–22.
Tetu B, Evans A. Canadian licensure for the use of digital pathology for routine diagnoses: one more step toward a new era of pathology practice without borders. Arch Pathol Lab Med. 2014;138(3):302–4.
Pantanowitz L, Hornish M, Goulart RA. The impact of digital imaging in the field of cytopathology. Cytojournal. 2009;6:6.
Evans AJ, Chetty R, Clarke BA, Croul S, Ghazarian DM, Kiehl TR, et al. Primary frozen section diagnosis by robotic microscopy and virtual slide telepathology: the University Health Network experience. Hum Pathol. 2009;40(8):1070–81.
Gould P, Saikali S, Tetu B. Teleneuropathology in Canada in 2012. Can J Neurol Sci. 2013;40(1):113–4.
Fallon MA, Wilbur DC, Prasad M. Ovarian frozen section diagnosis: use of whole-slide imaging shows excellent correlation between virtual slide and original interpretations in a large series of cases. Arch Pathol Lab Med. 2010;134(7):1020–3.
Zhao C, Wu T, Ding X. International telepathology consultation: an experience from UPMC and Kingmed (China). Lab Invest. 2014;94:404A–5A.
Bauer TW, Slaw RJ. Validating whole-slide imaging for consultation diagnoses in surgical pathology. Arch Pathol Lab Med. 2014;138(11):1459–65.
Krishnamurthy S, Mathews K, McClure S, Murray M, Gilcrease M, Albarracin C, et al. Multi-institutional comparison of whole slide digital imaging and optical microscopy for interpretation of hematoxylin-eosin-stained breast tissue sections. Arch Pathol Lab Med. 2013;137(12):1733–9.
Stathonikos N, Veta M, Huisman A, van Diest PJ. Going fully digital: perspective of a Dutch academic pathology lab. J Pathol Inform. 2013;4:15.
Thrall MJ, Rivera AL, Takei H, Powell SZ. Validation of a novel robotic telepathology platform for neuropathology intraoperative touch preparations. J Pathol Inform. 2014;5:21.
Hartman DJ, Parwani AV, Cable B, Cucoranu IC, McHugh JS, Kolowitz BJ, et al. Pocket pathologist: a mobile application for rapid diagnostic surgical pathology consultation. J Pathol Inform. 2014;5:10.
Ramey J, Fung KM, Hassell LA. Use of mobile high-resolution device for remote frozen section evaluation of whole slide images. J Pathol Inform. 2011;2:41.
Têtu B, Gagnon MP, Roch G, Fortin JP. The Eastern Quebec Telepathology Network: a support to the improvement to the public health care system. Diagn Pathol. 2013;8 Suppl 1:S8.
Ghaznavi F, Evans A, Madabhushi A, Feldman M. Digital imaging in pathology: whole-slide imaging and beyond. Annu Rev Pathol. 2013;8:331–59.
Kaplan KJ. Needs and workflow assessment prior to implementation of a digital pathology infrastructure for the US Air Force Medical Service. J Pathol Inform. 2013;4:37.
Ho J, Aridor O, Glinski DW, Saylor CD, Pelletier JP, Selby DM, et al. Needs and workflow assessment prior to implementation of a digital pathology infrastructure for the US Air Force Medical Service. J Pathol Inform. 2013;4:32.
Dunn BE, Choi H, Almagro UA, Recla DL, Davis CW. Telepathology networking in VISN-12 of the Veterans Health Administration. Telemed J E Health. 2000;6(3):349–54.
Fontelo PA, DiNino E, Johansen K, Khan A, Ackerman MJ. Virtual microscopy: potential applications in medical education and telemedicine in countries with developing economies. Proceedings of the 38th Annual Meetings of the Hawaii International Conference on System Sciences (HICSS), 3-6 Jan 2005, p 153c.
Gimbel DC, Sohani AR, Prasad Busarla SV, Kirimi JM, Sayed S, Okiro P, et al. A static-image telepathology system for dermatopathology consultation in East Africa: the Massachusetts General Hospital experience. J Am Acad Dermatol. 2012;67(5):997–1007.
Hassell LA, Fung KM. Digital pathology for educational, quality improvement, research and other settings. In: Pantanowitz L, Parwani AV, editors. Digital pathology. Chicago, IL: ASCP Press; 2014.
Settakorn J, Kuakpaetoon T, Leong FJ, Thamprasert K, Ichijima K. Store-and-forward diagnostic telepathology of small biopsies by e-mail attachment: a feasibility pilot study with a view for future application in Thailand diagnostic pathology services. Telemed J E Health. 2002;8(3):333–41.
Kadaba V, Ly T, Noor S, Chhut SV, Hinsch N, Stauch G, et al. A hybrid approach to telepathology in Cambodia. J Telemed Telecare. 2013;19(8):475–8.
Tetu B, Fortin JP, Gagnon MP, Louahlia S. The challenges of implementing a “patient-oriented” telepathology network; the Eastern Quebec telepathology project experience. Anal Cell Pathol (Amst). 2012;35(1):11–8.
Lowe J. Telepathology: guideline from the Royal College of Pathologists. 2013. http://www.rcpath.org/Resources/RCPath/Migrated%20Resources/Documents/G/G026_Telepathology_Oct13.pdf
Campbell WS, Lele SM, West WW, Lazenby AJ, Smith LM, Hinrichs SH. Concordance between whole-slide imaging and light microscopy for routine surgical pathology. Hum Pathol. 2012;43(10):1739–44.
Lange H. Digital pathology: a regulatory overview. Lab Med. 2011;42:587–91.
Hassell LA, Glassy E. The (not yet) willingly adopted tool. J Pathol Inform. 2013;4:13.
Parwani AV, Hassell L, Glassy E, Pantanowitz L. Regulatory barriers surrounding the use of whole slide imaging in the United States of America. J Pathol Inform. 2014;5:38.
Faisel T. Historical overview of FDA regulation of digital pathology imaging. 2014. www.fda.gov/…/HematologyandPathologyDevicesPanel/UCM201450.ppt. Accessed 19 Sep 2014.
Lloyd MC, Allam-Nandyala P, Purohit CN, Burke N, Coppola D, Bui MM. Using image analysis as a tool for assessment of prognostic and predictive biomarkers for breast cancer: how reliable is it? J Pathol Inform. 2010;1:29.
Dierks C. Legal aspects of telepathology. Anal Cell Pathol. 2000;21(3-4):97–9.
Leung ST, Kaplan KJ. Medicolegal aspects of telepathology. Hum Pathol. 2009;40(8):1137–42.
Patterson ES, Rayo M, Gill C, Gurcan MN. Barriers and facilitators to adoption of soft copy interpretation from the user perspective: lessons learned from filmless radiology for slideless pathology. J Pathol Inform. 2011;2:1.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Têtu, B., Hassell, L.A. (2016). Role in Medicine for Digital Pathology. In: Kaplan, K., Rao, L. (eds) Digital Pathology. Springer, Cham. https://doi.org/10.1007/978-3-319-20379-9_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-20379-9_3
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-20378-2
Online ISBN: 978-3-319-20379-9
eBook Packages: MedicineMedicine (R0)