
Abstract
Extensive limb lengthening may be indicated in patients with achondroplasia in order to improve their quality of life. However, excessive lengthening is associated with decreased ROM of the adjacent joints, decreased new bone formation, delayed weight bearing, and fractures of the regenerate bones. Many surgeons have recommended that the goal of lengthening in a bone segment should be limited to 20 ~ 30 % of its initial length. And fractures of the regenerate bones may be avoided by careful analysis of the regenerate bone in the distraction gap before removal of the apparatus.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others



Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Brief Clinical History
Eight-year-old boy patient, who diagnosed with achondroplasia, was admitted for limb lengthening surgery. He underwent bilateral 8-cm lengthening of tibia 18 months ago. At the time of visit, he was complaining about gait abnormality caused by disproportionate limb length.
2 Preoperative Clinical Photos and Radiographs

Lower extremity AP at the time of initial visit (5 years 10 months). Rt.limb:mLDFA 99°, mMPTA 85°, MAD 13 mm. Lt.limb:mLDFA 84°, mMPTA 86°, MAD 14 mm

Clinical photo of the patient

POD 1 year 6 months after 8 cm of lengthening, correctional osteotomy, and external fixator application with Ilizarov apparatus (7 years 4 months). Rt.limb:mLDFA84°, mMPTA93°, MAD 10 mm. Lt.limb:mLDFA 87°, mMPTA 97°, MAD 14 mm
3 Preoperative Problem List
-
I.
Angular deformities
(Varus tendency at the lengthening site and valgus tendency of mechanical axis)
-
II.
Soft tissue contractures of the adjacent joints
(Flexion contracture of the hip, extension contracture of the knee, tightness of the iliotibial band)
-
III.
Poor callus formation and refracture of the regenerate bones
-
IV.
Difficulty in determining removal timing of the external fixators
(Specific problems related with patients with achondroplasia)
-
(i)
Relatively short bone segment – The level of osteotomy should be located in mid-diaphyseal area.
-
(ii)
Malalignment (coxa vara) of the proximal femur – Prone to fractures of the regenerate bone.
-
(iii)
Previous tibial lengthening – Decreased potency of new bone formation in distraction osteogenesis and subsequent lateral instability of the knee joint.
-
(i)
4 Treatment Strategy
-
I.
Align the axis of external fixator according to the mechanical of axis of the lower extremity.
-
II.
Consider release of hip flexor muscles (sartorius, fascia lata, rectus femoris), quadricepsplasty for knee flexion, and Z-plasty of the iliotibial band for treatment of valgus knee.
-
III.
Avoid using wires for soft tissue impingement near the joint.
Consider half-pin insertion using the intermuscular planes.
-
IV
Evaluate properly of the quality of regenerate bones.
Use the Pixel Value Ratio (PVR) method.
-
V.
Use PVR to determine proper timing of removal of the external fixators.
(Specific treatment strategy related with patients with achondroplasia)
-
(i)
Timing of surgery – Consider significant disturbance of growth after extensive lengthening in skeletally immature patients with achondroplasia.
-
(ii)
Malalignment of the lower limb – Thorough preoperative evaluation of the patient’s rotational profile and joint orientations.
-
(i)
5 Basic Principles
-
I.
Determining the amount of lengthening
Excessive lengthening was associated with decreased new bone formation and delayed weight bearing. Large amount of lengthening more than 50 % of their initial femoral length was associated with an increased incidence of concave, lateral, and central callus shapes, adjacent joint stiffness, and fracture (Venkatesh et al. 2009).
-
II.
Avoiding angular deformity
When an external fixator is used to lengthen the femur, the device can be aligned with the mechanical or the anatomical axis. Aligning it with the anatomical axis theoretically leads to medialization of the knee joint (lateralization of the mechanical axis line). Therefore, most femoral external fixators should be aligned with the mechanical axis.
-
III.
Management of soft tissue
Excessive lengthening is associated with a decreased ROM of the adjacent joints. Knee movement is known to help to prevent muscle atrophy and adhesion of the muscles to the underlying bone regenerate and to increase the blood supply to bone and bone strength (Herzenberg et al. 1994). Excessive lengthening affects the thigh muscles by unable to keep pace with the lengthening, resulting in a decreased ROM at the knee and fixed flexion at the hip.
-
IV.
Evaluation of the regenerate bone (Pixel Value Ratio, PVR)
The pixel values of the proximal, distal, and regeneration areas could be calculated from the mean value of each area using the free line range of interest (ROI) method.
-
V.
Timing of the external fixator removal (PVR)
A pixel value ratio of 1 indicated corticalization of the regenerate in the lengthening area. The external fixators should be removed based on a PVR of at least 1.0.
6 Images During Treatment
Figs. 4, 5, 6, 7, 8, 9, and 10.

After femoral lengthening osteotomy and external fixation with monolateral fixator (8 years 2 months)

POD 3 months after 9 cm of lengthening (8 years 5 months) and Assessment of Pixel value based on a radiograph in PACS system. Note the red circle showing the pixel value of range of interest (ROI) drawn at each segment. The value M (encircled in red) indicates the mean pixel value for that segment and can be used in the computation for the PVR pixel value ratio = [(pixel value of the proximal segment + pixel value of the distal segment)/2]/pixel value of the regenerate (Song et al. 2011)

Clinical photos showing flexion contracture of the hip joint caused by excessive lengthening. He was treated with releasing of sartorius, fascia lata, straight head of rectus femoris, and psoas muscle

POD 1 year 3 months after 9 cm of lengthening (9 years 5 months) showing concave and lateral type of poor callus formation

Third operation for regenerate fracture with additional bone graft (DBM and PRP) and internal fixation (9 years 5 months)

POD 1 year (11 years 5 months) after removal of implant on left side. Rt.limb:mLDFA91°, mMPTA89°, MAD 2 mm. Lt.limb:mLDFA102°, mMPTA95°, MAD 19 mm

After bifocal femoral osteotomy and monolateral external fixator application on left limb (11 years 5 months) and monofocal femoral osteotomy and monolateral fixator application on right limb (12 years 4 months)
7 Technical Pearls
-
I.
Early physeal closure related to lengthening loss ranging from 1.5 to 4 cm after extensive tibial and femoral lengthening could occur after extensive limb lengthening in skeletally immature patients with achondroplasia (Song et al. 2012) and start lengthening after 10 years old.
-
II.
Aligning the external fixators with the mechanical axis did not guarantee anatomical alignment after lengthening. There is tendency of varus angulation due to absence of medial distraction when using monofixator and tendency of valgus knee caused by iliotibial band.
-
III.
Regular radiological examination, physiotherapy, careful adjustment of the distraction rate, and soft tissue releases should be considered during large amount of femoral lengthening. And regular stretching and the maintenance of a good ROM can help to decrease the pain and muscle spasm during lengthening.
-
IV.
The radiological features of the callus in distraction osteogenesis could be classified with regard to shape and type on the basis of the Li classification (Li et al. 2006). The shape was based on the width of the callus compared to the original osteotomy site. The type was based on the callus shapes (cylindrical, fusiform, and concave), three patterns of osteogenesis (homogeneous, heterogeneous, and lucent), and three densities (low, intermediate, and normal). When there is concave or lateral type of poor callus formation, compression is necessary until fusiform or cylinder type of callus is visible (Fig. 11).
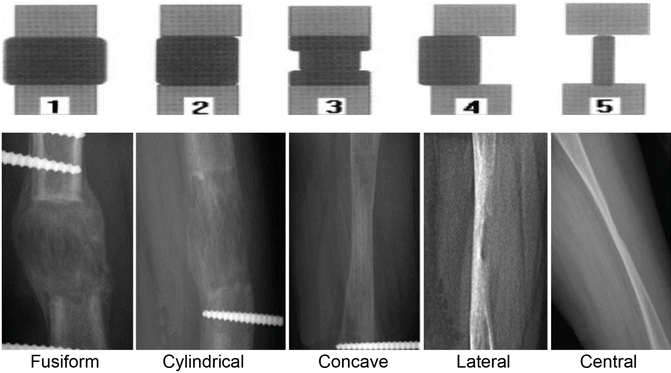
Fig. 11
Description
Name
Regeneration wider than the original bone
Fusiform
Regeneration same width as the original bone
Cylindrical
Regeneration narrower than the original bone
Concave
Regeneration mainly on one side of the distraction gap
Lateral
Regeneration a thin pillar
Central
-
V.
We can safely rely on PVR values to define the timing of fixator removal, as it exhibits a good correlation in patients with a cylindrical callus pattern regardless of whether the pathway is homogeneous or heterogeneous (Song et al. 2011).



9 Avoiding and Managing Problems
-
I.
Treating physicians should include the possibility of early physeal closure in preoperative counseling of the patients and their parents and also should be cautious in determining the amount of lengthening.
-
II.
Treating physicians should consider difference of axis between mechanical axis and anatomical axis in coronal plane and axial deviation during femoral lengthening and also their surrounding soft tissue conditions.
-
III.
Various soft tissue procedures such as release of the fascia of vastus lateralis, tensor fascia lata, psoas tendon, hamstring tendon, and iliotibial band could be used to correct joint stiffness.
10 See Also in Vol. 2
Case 8: Femoral Bone Defect
References and Suggested Reading
Herzenberg JE, Scheufele LL, Paley D, Bechtel R, Tepper S (1994) Knee range of motion in isolated femoral lengthening. Clin Orthop Relat Res 301:49–54
Li R, Saleh M, Yang L, Coulton L (2006) Radiographic classification of osteogenesis during bone distraction. J Orthop Res 24–3:339–347
Song SH, Sinha S, Kim TY, Park YE, Kim SJ, Song HR (2011) Analysis of corticalization using the pixel value ratio for fixator removal in tibial lengthening. J Orthop Sci 16-2:177–183
Song SH, Kim SE, Agashe MV, Lee H, Refai MA, Park YE, Choi HJ, Park JH, Song HR (2012) Growth disturbance after lengthening of the lower limb and quantitative assessment of physeal closure in skeletally immature patients with achondroplasia. J Bone Joint Surg Br 94-4:556–563
Venkatesh KP, Modi HN, Devmurari K, Yoon JY, Anupama BR, Song HR (2009) Femoral lengthening in achondroplasia: magnitude of lengthening in relation to patterns of callus, stiffness of adjacent joints and fracture. J Bone Joint Surg Br 91-12:1612–1617
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this entry
Cite this entry
Song, HR., Park, KW. (2015). Case 92: Refracture, Soft Tissue Contracture, and Angular Deformity After Femoral Lengthening in Achondroplasia. In: Rozbruch, S., Hamdy, R. (eds) Limb Lengthening and Reconstruction Surgery Case Atlas. Springer, Cham. https://doi.org/10.1007/978-3-319-18023-6_73
Download citation
DOI: https://doi.org/10.1007/978-3-319-18023-6_73
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-18022-9
Online ISBN: 978-3-319-18023-6
eBook Packages: MedicineReference Module Medicine