
Abstract
Background
It is important to define callus maturation and corticalization during distraction osteogenesis. Quantitative methods such as ultrasound and Q-computed tomography are sensitive but expensive. The pixel value ratio (PVR) obtained using a PACS (picture archiving and communication system) is a simple and cost-effective investigation tool. Recently, the issue of whether the PVR is correlated with quantitative methods has been studied. We investigated whether serial PVR is a useful technique for predicting corticalization in each callus segment of the regenerate, and can act as a guide for fixator removal in tibial lengthening without intramedullary nailing.
Methods
A retrospective analysis of 30 tibial segments in 18 patients was performed. The mean age of the patients was 18 years (range 5–48 years). There were 6 male patients and 12 female patients, of whom 8 patients were skeletally mature. Indications for limb lengthening were achondroplasia (8 patients), limb length discrepancy (4 patients), and miscellaneous (6 patients). The interobserver variability of the PVR was measured at each callus segment of the regenerate. Serial PVR at each callus segment was classified according to the callus pathway.
Results
The mean interobserver correlation coefficient at the regenerate was high in the posterior callus segment (0.92), the lateral callus segment (0.90), and the medial callus segment (0.70). However, there was low mean interobserver variability in the anterior callus segment (0.49) at the regenerate. A PVR of 1 at the regenerate was achieved first at the lateral callus segment, second at the posterior, third at the medial callus segment, and last at the anterior callus segment. There was no fracture at the regenerate or wire breakage in patients who began fixator removal and full weight bearing when the PVR was 1 in the three callus segments at the regenerate.
Conclusions
In tibial lengthening without nailing, serial measurement of the PVR is a reliable and cost-effective technique to assess the maturity of the callus, especially in the lateral and posterior callus segments, and assessment of the cortical pixel value can safely provide guidelines for fixator removal.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Distraction osteogenesis has become the mainstay for all lengthening procedures. More and more research is being directed towards defining callus maturation and corticalization, as it is still plagued by complications associated with fixator removal, such as refracture and subsidence. Indirect quantitative methods, including ultrasound, DEXA and QCT, have already been scrutinized and were found to be sensitive but expensive [1, 2].
The latest approach that is being used to determine callus stiffness is to evaluate the pixel value ratio [3] using a picture archiving and communication system (PACS). The pixel value ratio is the ratio of the proximal segment to that of the regenerate, and it correlates well with the BMD ratio. However, none of the above methods estimate regenerate strength directly.
However, the distraction force during limb lengthening was measured directly for a large series using a force transducer with a strain gage, and it was reported that it is at least 3 months before the callus bears most of the weight [4].
Recently, several studies have reported measurements of bone mineral density using the pixel value ratio. Using Ru Li’s classification, Song et al. analyzed the callus pattern of tibial lengthening in achondroplasia via the pixel value ratio, and found that callus mineralization occurs optimally in the homogeneous pathway, whereas the lucent pathway has a poor scenario [5, 6]. According to them, when the pixel value ratio equals 1, cortex mineralization is complete and the fixator can be safely removed. In a recent study of 17 patients who underwent tibial lengthening over I/M nail, it was suggested that full weight bearing after fixator removal is possible without complications when there are three cortices with a pixel value ratio of 1 [7].
We hypothesized that serial PVR measurements can outline and define corticalization in cases where tibial lengthening is done without intramedullary nailing. The purpose of our study was to find the correlations of serial pixel value ratio with callus shapes and with pathways separately, and to find the optimal PVR for fixator removal.
Materials and methods
We retrospectively reviewed 18 patients who underwent tibial lengthening with an Ilizarov external fixator for LLD or to increase height between 2006 and 2008. The average age of the patients at the time of surgery was 18 years (range 5–48 years).
There were 6 male patients and 12 female patients. Unilateral tibial lengthening was performed in 6 patients and bilateral tibial lengthening in 12 patients.
Indications for limb lengthening were achondroplasia in 8 patients, limb length discrepancy in 4 patients, and idiopathic short stature in 1 patients; four patients had other miscellaneous indications—one patient each with hypochondroplasia, Blount’s disease, Turner’s syndrome, genu varum and genu valgus. All patients had undergone tibial lengthening by Ilizarov external fixator without intramedullary nailing.
The purpose of the study and the radiation exposure was explained to the patients and their parents after obtaining their informed consent according to IRB approval.
Operation
All patients were operated on by a single pediatric orthopedic surgeon (H.R.S.) at our institute between 2006 and 2006. Three rings were used for distraction. Two proximal wires and one proximal half-pin were inserted and fixed at the proximal ring. Two distal wires and one distal half-pin were inserted and fixed at the distal ring. Patients underwent supervised daily physiotherapy including active and passive ranges of motion of the knee and ankle beginning 2 days after surgery. Physiotherapy was performed twice per day for 2 h during the 2 weeks of admission and 1 h per day after discharge until the end of the distraction phase. Daily walking for at least 4 h with partial weight bearing using two crutches was allowed during the distraction phase. Distraction was started 7 days postoperatively at a rate of 0.25 mm four times a day until the desired length was achieved.
Evaluation
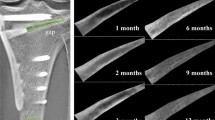
The pixel value ratio was measured on digital radiogram with StarPACS PiView Star 5.0.6.1 software (Infinitt Co., Ltd., Seoul, Korea). The pixel value was measured with the pixel lens included in the tools of the PACS (Fig. 1a). The pixel values of the proximal, distal, and regeneration areas were calculated from the mean value of each area with the free line range of interest (ROI) method (Fig. 1b). Care was taken to avoid any wire metal. We defined the medial and lateral callus segments based on the anterior–posterior radiograph and the anterior and posterior callus segments based on the lateral radiograph; they were between the cortices and anatomical axis (Fig. 2).

a Pixel value assessment based on a radiograph in a PACS workstation. Note the red circle showing the pixel value of the particular point where the marker (yellow dot) is positioned. b Free line range of interest (ROI) drawn at each segment. The value M (encircled in red) indicates the mean pixel value for that segment, and will be used in the computation for the PVR

The pixel values measured on a digital radiograph. The pixel values of the regenerate were measured at different callus segments, which were divided into medial and lateral callus segments based on the AP radiogram (a) and anterior and posterior callus segments based on the lateral radiogram (b)
The pixel value ratio of the regenerate then was calculated using the following formula: pixel value ratio = [(pixel value of the proximal segment + pixel value of the distal segment)/2]/pixel value of the regenerate. Since we measured the raw pixel value, which is inversely related to radiodensity (i.e., as radiopacity increases the pixel value decreases), an inverse ratio is used in the above formula. The stage of corticalization was decided based on the pixel value ratio. A pixel value ratio of 1 indicated corticalization of the regenerate in the lengthening area.
Two surgeons measured the pixel value ratio to test interobserver variability. Interobserver variability for the pixel value ratios was determined using Pearson correlation coefficients.
Follow-up
Three surgeons evaluated all patients clinically and radiographically every week during the distraction phase and every 4 weeks during the consolidation phase. We adjusted the rate of distraction with or without compression and distraction during the distraction period according to one of three types of callus pathways seen radiographically using the classification of Li et al.: homogeneous, heterogeneous, or lucent. In the homogeneous pathway, distraction rates were 1 mm per day when the callus had a cylindrical shape and 1.5 or 2 mm per day when the callus showed a fusiform shape to avoid premature consolidation. In the heterogeneous pathway, we adjusted the rate of distraction, starting at 0.5 mm per day for 2 weeks and then gradually increasing to 1 mm per day when new bone formation was seen on the radiographs. In the lucent pathway, we gave gradual compression until the disappearance of the radiolucent gap. After 1 week, we began the distraction at 0.5 mm per day until the segment attained an adequate amount of lengthening compared with the opposite segment.
After the desired limb length was achieved, we stop the lengthening. When the pixel value ratio reached 1 in all three callus segments, we removed the external fixator and the patients were permitted full weight bearing without crutches.
Statistical analysis
Intraobserver and interobserver variabilities were also tested with intraclass correlation analysis. An appropriate statistical analysis called the linear mixed model was used to analyze how serial pixel value ratios relate to callus patterns and pathways after adjusting for the period of follow-up and the laterality of the limb (right, left or both). When employing the linear mixed model, we considered the covariance structure as compound symmetry or autoregressive models of order 1. A similar analysis was used for each of the various callus shapes and pathways. All of the statistical analyses based on the two-sided test were performed with the SAS software suite (v.9.2, SAS Institute Inc., Cary, NC, USA.). We regarded a p value of <0.05 as statistically significant.
Results
The mean amount of lengthening was 7.7 cm (range 2.5–10.9 cm). The mean duration of Ilizarov application was 8.2 months (range 5.1–15 months).
The data on the pixel values in each callus segment were obtained by separate observers. The mean interobserver correlation coefficient at the normal bone was found to be highly significant for proximal cortex (0.91) and distal cortex (0.87). The mean interobserver correlation coefficient at the regenerate was also high in the posterior callus segment (0.92), the lateral callus segment (0.90), and the medial callus segment (0.70). However, there was low interobserver variability in the anterior callus segment (0.49) at the regenerate. This signifies that the value of PVR is not interdependent in all four callus segments.
The PVR at each callus segment of the regenerate increased during the consolidation period. A PVR of 1 at the regenerate was achieved first at the lateral callus segment, second at the posterior, third at the medial callus segment, and last at the anterior callus segment (Fig. 3). When a PVR of 1 was achieved at the medial callus segment, the three callus segments at the regenerate were considered to be corticalized.

Pixel value ratios (PVRs) in different callus segments during different periods of healing. A PVR of 1 was first achieved at the lateral callus segment, second at the posterior, third at the medial callus segment, and last at the anterior callus segment of the regenerate
The three pathways (according to Ru Li’s classification) considered in our study were as follows: the homogeneous pathway (51.75%), the heterogeneous pathway (43.86%) and the lucent pathway (4.38%). There were a few cases with a lucent pathway. We cannot show a diagram of the corticalization of each callus segment of the regenerate for the lucent pathway.
-
1.
Homogeneous pathway. A pixel value of 1 was achieved by the lateral callus segment in 10 weeks, followed by the posterior callus segment in 15 weeks, then the medial callus segment in 18 weeks, and the anterior callus segment in 22 weeks (Fig. 4)
Fig. 4 
Plot showing that there was a pixel value ratio of 1 in two callus segments by 15 weeks and in three callus segments by 18 weeks in the homogeneous pathway
-
2.
Heterogeneous pathway. Pixel values of 1 were achieved according to a similar pattern as for the homogeneous pathway, with lateral being the earliest at 18 weeks, followed by the posterior, the medial and the anterior callus segments at 26, 33, and 36 weeks, respectively (Fig. 5).
Fig. 5 
Plot showing that there was a pixel value ratio of 1 in two callus segments by 26 weeks and in three callus segments by 33 weeks in the heterogeneous pathway


We also investigated the association of the PVR with various combinations of callus shapes and pathways taken for consolidation using linear mixed model analysis. We found that the PVR was significantly correlated with the cylindrical homogeneous (p value = 0.004), cylindrical heterogeneous (p value = 0.0453) and fusiform homogeneous (p value = 0.0043) groups. However, it was not significantly correlated with the fusiform heterogeneous pathway (p value = 0.1708) or the lucent pathway (p value = 1) (Table 1).
There was no fracture at the regenerate or wire breakage in patients who began fixator removal and full weight bearing when the pixel value ratio was 1 in the three callus segments at the regenerate.
Discussion
Distraction osteogenesis has been widely used for limb lengthening, but there are worries associated with its use for major complications like refracture and bending at the regenerate. To our knowledge, no previous paper has studied the role of serial PVR measurement in all cases of tibial lengthening over an Ilizarov fixator without I/M nailing. Our study has proven that serial PVR measurement can be used to obtain the optimal time of fixator removal based on the callus pathway and the callus shape taken individually by each case [6]. We also defined which corticalization of various callus segments to observe in each pathway to allow partial or complete weight bearing.
A definition of corticalization has been attempted by many authors. Adequate corticalization is defined by Fischgrund as 2 mm of cortex with a density similar to the normal bone, and three such cortices that are visible on radiographs [8]. However, this has poor interobserver and intraobserver reliability, and there is no objective guideline to check the corticalization at the regenerate [9]. Based on these criteria, fracture rates of 30–50% [10] have been reported, although rates of 10–15% are more common [11]. Paley et al. [12] allowed partial weight bearing with two crutches until the callus bridging was visible at two cortices, and full weight bearing without crutches when there were two intact cortices seen on radiographs after femoral lengthening over I/M nail. They reported one nail and one screw breakage in 2 of 32 femoral segments. Indirect measurement techniques are used to predict the nature of callus progression and maturation. Serial measurements by a sensitive technique have always been in demand in order to understand callus progression. Eyres et al. [13] measured the BMD and BMC contents in both tibial and femoral lengthening, and removed the fixator when the value for the regenerate reached 75% of the controls (i.e., the unoperated leg). However, these investigations are expensive and the patient must undergo additional imaging. Recently, a technique that uses the pixel value on digital radiographs was introduced, which is an economical method for measuring the serial changes in callus mineralization. Shim et al. [14] studied serial pixel values of different cortices in both femoral and tibial lengthening and showed that pixel values for distraction callus conformed to a sigmoidal curve. Song et al. [15] studied the risk of complication in 22 cases with a follow-up of more than 2 years, retrospectively, and found that cases with regenerate fracture had pixel values of less than 0.8, but there was no fracture in regenerates with PVRs of >1 in a minimum of two cortices at the time of weight bearing.
Pixel value was used to measure callus mineralization at each callus segment of the regenerate in order to evaluate the corticalization, which predicts the callus stiffness and weight-bearing time of tibia distraction osteogenesis over I/M nailing. Zhao et al. [7] prospectively analyzed tibial lengthening over nail and found no complications in patients who began full weight bearing with crutches when two callus segments had PVRs of >1, and full weight bearing without crutches when the PVR was 1 in three callus segments. However, in contrast to this, Shyam et al. [16] found that patients with three regenerated callus segments at the time of fixator removal had significantly more subsidence than patients with four regenerated callus segments at the time of fixator removal when the lengthening was more than 10 cm. Hence, fixator removal should be timed such that immediate complications like regenerate fracture or delayed callus subsidence are not encountered.
In our study, we measured serial PVR separately for each callus segment and correlated these PVR values with various pathways and callus patterns of tibial lengthening over an Ilizarov fixator without I/M nailing. We had only two types of callus patterns: fusiform and cylindrical. Most of the pathways were homogeneous or heterogeneous, while the lucent pathway was present in few of our cases. The probable explanation for this is that we used an Ilizarov ring fixator with Schanz pins, which improved the stability of the construct. Also, the distraction was continuously monitored by serial digital radiographs, and it was adjusted.
Our results were different from those obtained by Zhao et al. [7] in their study of tibial lengthening over I/M nail. They found that in homogeneous and heterogeneous pathways, two callus segments exhibited pixel value ratios of 1 by 32 weeks and three callus segments showed PVRs of 1 by 40 weeks, we obtained these values at 15–18 weeks for the homogeneous pathway group and at 26–33 weeks for the heterogeneous pathway group. These values were seen much later for the lucent pathway: at 40–48 weeks in the study of Zhao et al., and at 80–90 weeks in our study.
From our data, it appears that the time required for callus consolidation is shorter when the Ilizarov fixator without I/M nailing is employed for the homogeneous and heterogeneous pathways than when the fixator is used with I/M nailing. However, the reverse is true for the lucent pathway. This is because, when the Ilizarov fixator is used for long periods, wires may lose tension and pins usually become looser. However, when lengthening over nail, the implant maintains its stability even when the fixator wire breaks or loosens. Early healing with the Ilizarov fixator without I/M nail as compared to lengthening over I/M nail can be explained by the fact that the intramedullary device can interfere with the endosteal callus formation to some extent, even though it is applied unreamed. We believe that our data are more accurate, because our technique for measuring pixel values is not affected by the presence of a nail in the vicinity of the range of interest for cases with I/M nailing.
The clinical implication of our study is that we can safely rely on the PVR to define the timing of fixator removal, as it shows good correlation [3, 16] in cases with a cylindrical callus pattern regardless of whether the pathway is homogeneous or heterogeneous. If the callus pattern follows a fusiform-homogeneous pathway, PVR can be relied upon to accurately define the timing of fixator removal. However, a lucent pathway or a fusiform-heterogeneous pathway or any callus pattern that is not cylindrical requires more meticulous monitoring and the aid of additional indirect measurements (such as from QCT or DEXA) to judge the appropriate timing.
Even when intramedullary nailing is not used for tibial lengthening, the presence of the metal wire hinders the measurement of pixel values. To avoid this problem, we followed the guidelines proposed by Young et al. [17]. We aligned the X-ray beam parallel to the plane of the ring closest to the distraction site.
Second, we measured the pixel value ratio, which is an indirect tool for measuring callus stiffness. There was also no direct measurement of callus stiffness and no mechanical study of our methods. There is a need for a study similar to that performed by Lauterberg et al. [4] in order to measure the callus stiffness directly by strain transducer.
Thirdly, we had a small number of patients in which we could not find any significant complications such as refracture after fixator removal, or in which we could not find all of the callus shapes and pathways. In other words, we could not obtain a control group for evaluation. However, we compared our data with other studies in which parameters for regenerate fractures and bone healing indices have been reported [6, 11, 15, 18]. Hence, a clear and exact cut-off value for the PVR that should be obtained before removing the fixator was not attained. The timing of fixator removal must be tailored to each patient according to the callus shape and the pathway taken when examining the radiographs serially.
This is a pilot study, and we need to perform a large prospective or retrospective study (or both) to find guideline values for complications where there is no fixator-based bias.
Conclusion
Based on the results of our study, we are propounding the serial measurement of the pixel value ratio (PVR) to monitor callus progression, and the use of the PVR to define the timing of fixator removal. This is a cheap, cost-effective and sensitive parameter for measuring callus stiffness. We also note that:
-
1.
Serial measurement of the PVR is a novel technique for indirectly assessing callus maturation, and partial weight bearing is allowable as soon as the PVR reaches 1 in the posterior and lateral callus segments. Full weight bearing is possible as soon as the third corticalized area (the medial callus segment) shows a PVR of at least 1.
-
2.
In cases with a homogeneous pathway and or a cylindrical callus shape, PVR estimation is a reliable method to use to judge the appropriate timing of fixator removal.
-
3.
Additional investigations (such as quantitative CT or DEXA) are required when deciding upon the appropriate timing of fixator removal in cases with a fusiform-heterogeneous and lucent pathways.
References
Eyres KS, Bell MJ, Kanis JA. Methods of assessing new bone formation during limb lengthening. Ultrasonography, dual energy X-ray absorptiometry and radiography compared. J Bone Joint Surg Br. 1993;75:358–64.
Romanowski CA, Underwood AC, Sprigg A. Reduction of radiation doses in leg lengthening procedures by means of audit and computed tomography scanogram techniques. Br J Radiol. 1994;67:1103–7.
Hazra S, Song HR, Biswal S, Lee SH, Jang KM, Modi HN. Quantitative assessment of mineralization in distraction osteogenesis. Skeletal Radiol. 2008;37:843–7.
Lauterburg MT, Exner GU, Jacob HA. Forces involved in lower limb lengthening: an in vivo biomechanical study. J Orthop Res. 2006;24:1815–22.
Li R, Saleh M, Yang L, Coulton L. Radiographic classification of osteogenesis during bone distraction. J Orthop Res. 2006;24:339–47.
Singh S, Song HR, Venkatesh KP, Modi HN, Park MS, Jang KM, Kim SJ. Analysis of callus pattern of tibia lengthening in achondroplasia and a novel method of regeneration assessment using pixel values. Skeletal Radiol. 2010;39:261–6.
Zhao L, Fan Q, Venkatesh KP, Park MS, Song HR. Objective guidelines for removing an external fixator after tibial lengthening using pixel value ratio: a pilot study. Clin Orthop Relat Res. 2009;467:3321–6.
Fischgrund J, Paley D, Suter C. Variables affecting time to bone healing during limb lengthening. Clin Orthop Relat Res. 1994:31–7.
Starr KA, Fillman R, Raney EM. Reliability of radiographic assessment of distraction osteogenesis site. J Pediatr Orthop. 2004;24:26–9.
Danziger MB, Kumar A, DeWeese J. Fractures after femoral lengthening using the Ilizarov method. J Pediatr Orthop. 1995;15:220–3.
Birch JG, Samchukov ML. Use of the Ilizarov method to correct lower limb deformities in children and adolescents. J Am Acad Orthop Surg. 2004;12:144–54.
Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res. 1990:81–104.
Eyres KS, Bell MJ, Kanis JA. New bone formation during leg lengthening. Evaluated by dual energy X-ray absorptiometry. J Bone Joint Surg Br. 1993;75:96–106.
Shim JS, Chung KH, Ahn JM. Value of measuring bone density serial changes on a picture archiving and communication systems (PACS) monitor in distraction osteogenesis. Orthopedics. 2002;25:1269–72.
Song HR, Oh CW, Mattoo R, Park BC, Kim SJ, Park IH, Jeon IH, Ihn JC. Femoral lengthening over an intramedullary nail using the external fixator: risk of infection and knee problems in 22 patients with a follow-up of 2 years or more. Acta Orthop. 2005;76:245–52.
Shyam AK, Singh SU, Modi HN, Song HR, Lee SH, An H. Leg lengthening by distraction osteogenesis using the Ilizarov apparatus: a novel concept of tibia callus subsidence and its influencing factors. Int Orthop. 2009;33:1753–9.
Young JW, Kovelman H, Resnik CS, Paley D. Radiologic assessment of bones after Ilizarov procedures. Radiology. 1990;177:89–93.
Stanitski DF, Shahcheraghi H, Nicker DA, Armstrong PF. Results of tibial lengthening with the Ilizarov technique. J Pediatr Orthop. 1996;16:168–72.
Acknowledgments
This study was supported by a grant from the Korea Healthcare Technology R&D Project, Ministry for Health, Welfare & Family Affairs, Republic of Korea (A090084).
Conflict of interest
All authors report that there was no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Song, SH., Sinha, S., Kim, TY. et al. Analysis of corticalization using the pixel value ratio for fixator removal in tibial lengthening. J Orthop Sci 16, 177–183 (2011). https://doi.org/10.1007/s00776-011-0036-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00776-011-0036-4