
Abstract
In recent years preoperative staging and assessment of rectal cancer has moved away from reliance on clinical and ultrasonographic assessment to detailed prognostic assessment afforded by high-resolution MRI. As with surgery and other modes of treatment, the use of preoperative staging is variable, and a minimum standard for both the technique and interpretation in staging rectal cancer needs to be followed to obtain the best results for patients. This chapter aims to highlight the important standards to establish or maintain in rectal cancer staging and the techniques in interpretation that will enable consistently accurate assessment as demonstrated in published multicentre studies.
Access provided by CONRICYT-eBooks. Download chapter PDF
Similar content being viewed by others


Introduction
In recent years preoperative staging and assessment of rectal cancer has moved away from reliance on clinical and ultrasonographic assessment to detailed prognostic assessment afforded by high-resolution MRI. As with surgery and other modes of treatment, the use of preoperative staging is variable, and a minimum standard for both the technique and interpretation in staging rectal cancer needs to be followed to obtain the best results for patients. This chapter aims to highlight the important standards to establish or maintain in rectal cancer staging and the techniques in interpretation that will enable consistently accurate assessment as demonstrated in published multicentre studies.
MRI Technique for Staging Rectal Cancer
MRI was first introduced in the early 1990s—the imaging parameters and techniques used for evaluating rectal cancer showed a wide variability in staging with a near-linear relationship between the accuracy achieved and the spatial T2-weighted resolution of the imaging utilised.
Schnall et al. showed that using an endorectal coil with a 12 cm field of view, 256 matrix and 3 mm slice thicknesses, in-plane resolution of 0.59 mm × 0.59 mm and a voxel size of <1 mm3 could be achieved. The drawback of the endorectal coil, and indeed of any endoluminal technique for assessing rectal cancers, was an inherent inability to interrogate the whole mesorectum, the potential radial margins and tumour spread laterally and above the primary tumour site. In addition passage of an intraluminal probe for bulky or stricturing tumours was impossible.
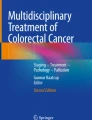
The advent and ongoing improvement of modern multichannel surface phased array coils overcame reliance on intraluminal techniques to evaluate the rectum and perirectal structures. When optimal parameters were used, an in-plane resolution could be achieved which was similar to those obtained with the endorectal coil (0.6 × 0.6 mm with a voxel size of 1.1 mm3). In order to meet these levels of resolution consistently, there needed to be a shift away from multiple noncontributory MRI sequences such as contrast enhancement, fat suppression and diffusion-weighted and T1-weighted scans to a more dedicated sequence that enabled clear delineation of the tumour with high-resolution depiction of the rectal wall, the mesorectum and the pelvic sidewall compartments in order to get genuinely prognostic and predictive staging information. The technique was developed and rolled out to radiologists at multiple institutions in the MERCURY trials and national training programmes. The scans are easily run on any generation 1.5–3T MRI system in conjunction with a multi-coil, multichannel surface array coil. The total examination duration is approximately 40 min and this is essential. Shortening the examination time by increasing the field of view, reducing the number of acquisitions or increasing the slice thickness inevitably reduces both the resolution and the consequent accuracy of the technique. The addition of further sequences also reduces the overall quality of the examination as well as prolonging patient discomfort in the scanner and for these reasons is not recommended. Figure 3.1 illustrates the difference between a high-resolution and suboptimal MRI scan. The difference in technique amounts to 3–4 min acquisition time to obtain high-resolution scans but can make a substantial improvement to staging accuracy and the ensuing appropriateness of treatment decisions.

Axial image showing the difference between a high resolution (left) and lower resolution scan in the same patient (right). The polypoidal tumour is much more clearly depicted on the high resolution scan. Similarly the anatomic layers of the bowel wall are also more clearly shown
Summary Points—for MRI Staging Technique
-
The field of view and matrix parameters should not exceed a pixel size of 0.6 × 0.6 mm, e.g. 200 × 200 mm with 384 × 384 matrix or 160 × 160 mm with a 256 × 256 matrix (note pixel size (mm) is calculated as = field of view/matrix). Voxel size mm3 = pixel size × slice thickness.
-
The surface phased array coil should be placed correctly over the lower pelvis. For low rectal cancers the distal edge of the coil should lie 10 cm below the symphysis pubis to ensure that the distal rectum is in the centre of the image (Fig. 3.2).
Fig. 3.2 
The surface phased array coil should be placed correctly over the lower pelvis. The left hand image shows incorrect placement- the coil has been positioned too high so that there is insufficient signal from the lower third of the rectum. For low and mid rectal cancers the distal edge of the coil should lie 10 cm below the symphysis pubis to ensure that the distal rectum is in the centre of the image
-
Scans should be obtained perpendicular to the rectal wall; the sagittal MRI scans are used to plan the oblique axial images (Fig. 3.3).
Fig. 3.3 
Illlustrates how the sagittal scans can be used to plan the correct scan planes for oblique axial and coronal images that are perpendicular to the rectal wall and coronal to the anal canal
-
Coronal images should be undertaken parallel to the anal canal to visualise the distal mesorectal plane (Fig. 3.3) and must also be performed using the same high-resolution parameters.
-
The use of saturation bands reduces image degradation due to abdominal wall motion, and hyoscine butylbromide given as an i.m. injection or oral mebeverine reduces small bowel peristalsis, respectively (Fig. 3.4).
Fig. 3.4 
The use of a “saturation bands” to suppress the signal from unwanted areas. For example the anterior abdominal wall produces movement degradation and so placing the saturation band over the abdominal wall (on the right hand image) reduces the image degradation. This is evident on the left hand image where no saturation band has been used
-
High-resolution coverage should include at least 5 cm above the top of the tumour and to the L5/S1 level for all tumours to ensure that discontinuous tumour deposits are visualised (Fig. 3.3).
-
T1-weighted imaging, contrast enhanced imaging and fat saturated sequences do not contribute and worsen staging accuracy and should not be used for primary rectal cancer staging.
-
Caution when using diffusion-weighted imaging for rectal cancer as it does not improve accuracy when compared with high-resolution MRI techniques.
-
The prolonged examination time caused by additional noncontributory sequences reduces the overall quality of the examination as well as prolongs patient discomfort.



Anatomic Considerations
The major utility of MRI lies in its ability to depict the surgical anatomic planes for preoperative roadmapping, thereby enabling a clear surgical approach that can be defined by the extent of tumour and its relationship to neighbouring structures.
Surgery for rectal cancers can be modified in accordance with the plane required to enable total clearance of the tumour. For the vast majority of patients presenting with rectal cancer, total mesorectal excision (TME) plane surgery enables the primary tumour and all the draining lymph nodes to be removed in an intact package with clear radial, distal and proximal margins. This approach has substantially reduced local recurrence rates from above 40% in non-TME series to 5% in patients where a clear margin is achieved and a good-quality TME specimen is shown. When all patients with rectal cancer are staged by MRI, the prevalence of potential involvement of the TME plane (mrCRM) is 26%, and the use of preoperative therapy enables tumour shrinkage that significantly reduces CRM positivity rates. For those patients that become either mr or pCRM negative as a result of preoperative therapy, the local recurrence rates are 7%, but for those with either persistence of tumour at the TME plane on imaging or pathologic involvement of the CRM, the rates of local recurrence are over 20%. Consequently, in a proportion of patients with persistence of tumour at the mesorectal margins, a beyond TME approach is required to achieve tumour-free resection margins. The major surgical landmarks for rectal cancer surgery are readily visualised using preoperative MRI.
The Mesorectum and Mesorectal Fascia
The rectum is somewhat unique having a mesenchyme that is encircled by a visceral fascial layer that encases the rectum, its draining nodes and neural and vascular structures. On MRI the fascial envelope is shown as a low signal intensity structure that encircles the mesorectum from the level of the distal levator inferiorly to the sacral promontory posteriorly. Anteriorly, the mesorectum ends at the level of the anterior insertion of the peritoneum. Therefore, anteriorly above the peritoneal insertion, the rectum is devoid of a fascia and is covered by the peritoneal serosa which gradually widens until the point of the sigmoid is reached. At this point the mesorectum is no longer anchored to the sacral concavity and is instead posteriorly surrounded by a relatively mobile sigmoid mesentery rooted by the sigmoid vascular branches to their vascular origin/confluence at the IMA and IMV.
Anteriorly Infiltrating Tumours
The peritoneum separating the pelvic and abdominal visceral compartments is seen on high-resolution scans as a low signal intensity layer. Anteriorly the peritoneum can be traced over the surface of the bladder and seminal vesicles or uterus before its attachment to the rectum in the midline. This is well seen on the sagittal images. The peritonealised surface of the rectum does not form part of the circumferential surgical resection margin, and so anterior tumours above this level are not considered as potentially margin involved but can still be infiltrating through the peritoneum. Such tumours have a risk of pelvic recurrence through transperitoneal spread.
The Ureteric Plane/Pelvirectal Space
This space is devoid of lymph node tissue but contains neurovascular structures as they pass forward from the sacrum to the anterior pelvic organs. When tumour is evident in this space, this will either be from direct spread out of mesorectal compartment, from peritoneal spread or from venous invasion.
The Rectovaginal Septum and the Urogenital Compartment
Below the peritoneal insertion anteriorly, a condensation of the rectogenital septum is manifest as a focal low signal intensity band-like thickening of the anterior mesorectum in the anterior midline. In males the fascia forms the plane separating the anterior mesorectum from the prostatic capsule and can be followed inferiorly to the perineal body in the midline (Fig. 3.5).

The arrow points to the low signal intensity rectogenital septum which forms a band-like thickening that overlies the anterior mesorectum in the anterior midline
The pelvis can thus be divided into distinct anatomic compartments based upon the boundaries of the peritoneal reflection, the visceral (or mesorectal) fascia, the presacral fascia and the pelvic floor musculature.
The Parietal Fascia and the Pelvic Parietal Compartments (Presacral and Lateral Pelvic Compartments)
Where tumours extend beyond the conventional mesorectal compartment and beyond the mesorectal fascia, patients can then be appropriately referred for a therapeutic strategy that will enable clearance of tumour from undertaking beyond TME plane surgery that could range from adjacent organ removal to total pelvic exenteration depending on the compartmental distribution of tumour as shown on the preoperative MRI.
The Infralevator Compartment (Fig. 3.6)
The levator muscle forms a single sheet of muscle forming the pelvic floor. In the midline, its posterior proximal attachment is seen at the tip of the coccyx , and laterally it forms a ‘hammock-like’ structure on both sides around the mesorectum, with a further point of fixed attachment on both sides at the ischial spines (best seen on the coronal image—Fig. 3.6); laterally the muscle fuses with the obturator fascia, and inferiorly the fibres blend with the puborectalis sling whose anterior fibres attach to the inner surfaces of the upper pubic symphysis on either side of the midline. The lower third of the rectum is defined anatomically from the point of the levator attachment at the tip of the coccyx posteriorly to the levator’s most distal point at the level of the puborectalis sling. This represents a surgically challenging portion of the TME dissection where the mesorectum starts to taper and the proximity of the rectum to the adjacent anterior urogenital compartment limits the space. For tumours arising in this lower third segment of the rectum, even minimal spread beyond the rectal wall, mesorectal fat plane is small and can result in potential CRM involvement.

The levator muscle is (arrows) a single sheet of muscle forming the pelvic floor. In the midline, its posterior proximal attachment is seen at the tip of the coccyx, and laterally it forms a ‘hammock-like’ structure on both sides around the mesorectum its most distal point is at the level of the puborectalis sling. The levator origin and its distal insertion effectively defines the anatomic lower third of the rectum where the mesorectum starts to taper resulting in the most challenging portion of surgical dissection in TME rectal cancer surgery
MRI and Local Rectal Cancer Staging
The development of high-resolution MRI and carefully validated image interpretation criteria has created the unique advantage of identifying prognostic factors that predict for the risk of local and distant failure before treatment commences. This precision in preoperative staging was previously not available and can now be used for the benefit of all patients with rectal cancer. For the surgeons and oncologist managing the patient, there is a consequent opportunity to tailor the surgical and preoperative therapeutic approach to reduce the risk of recurrence.
T Classification
For all cancers, the direct relationship between depth of tumour spread and prognosis is a well-established basis for the TNM classification. For patients with rectal cancer, there is a near-linear relationship between outcomes and degree of spread into and beyond the rectal wall. The ability to closely reproduce the low power haematoxylin and eosin stained depiction of tumour of the resection with the high-resolution T2-weighted images can afford millimetre accuracy in stage assessment that enables far more precise prognostication than the broader T categories and stage categories of the traditional AJCC/TNM systems.
Preoperative Assessment of T1 Tumours
Tumour depth into the submucosa can be measured to the nearest millimetre, and the depiction of a preserved submucosal layer can now be used to select patients for a primary local excision approach that avoids the morbidity of major radical surgery. On high-resolution scans , the submucosal layer is of brighter signal than the tumour, and its preservation enables the identification of a patient with a likely T1 cancer (Fig. 3.7).

MRI image and corresponding histopathologic section of a T1 tumour
T2 Tumour Spread
The muscularis propria is characterised by the following features: low signal (dark) intensity relative to tumour. It is formed by two layers —the circular and longitudinal muscle coat. The latter is seen as a discontinuous layer with vertically arranged low signal intensity bundles and separated from the inner circular layer by a distinct high signal layer of the myenteric plexus. The degree of muscularis propria preservation enables differentiation between an early invasive T2 and deeper T2 tumour inseparable prognostically from an early T3 tumour (Fig. 3.8).

MRI image and corresponding histopathologic section of the T2 tumour
Early T3 Tumours
As tumour advances, the degree of muscularis preservation diminishes until finally tumour is seen to completely replace the muscularis propria layer. Such tumours can be classified as full thickness T2 or T3 <1 mm. These are prognostically identical tumours with a low likelihood of spread to lymph nodes or distant spread and unless bordering the intersphincteric plane readily amenable to cure by primary surgical total mesorectal excision (Fig. 3.9).

MRI image and corresponding histopathologic section of a T3 tumour
When tumour has clearly spread beyond the muscularis propria, the depth of extramural invasion is an independent prognostic factor [1, 2]. This is defined as the depth in millimetres of tumour spread beyond the outer edge of the muscularis propria. Tumours with less than 1 mm spread have exactly the same prognosis as T2 tumours. Spread between 1 and 5 mm is also associated with cancer-specific survival rates that are similar to T2 tumours regardless of lymph node involvement. For patients with tumour spread beyond 5 mm, there is a consistent reduction in cancer-specific survival, with an increased propensity to distant metastatic disease and local recurrence.
Since the majority of rectal cancers diagnosed comprise T3 tumours, there is merit in addressing the inherent heterogeneity by taking into account the depth of extramural spread. Merkel and others [3] showed that pT3 rectal cancers could be usefully subdivided according to depth of extramural spread as follows: pT3a minimal invasion, <1 mm beyond the border of the muscularis propria; pT3b-slight invasion, 1–5 mm beyond the border of the muscularis propria; pT3c-moderate invasion, >5–15 mm beyond the border of the muscularis propria; and pT3d-extensive invasion, >15 mm beyond the border of the muscularis propria [4]. This prognostic classification based on a study of 850 patients in the Erlangen Cancer Registry was proven to predict survival regardless of nodal stage. This was an important observation as of all parameters assessable on MRI, depth of tumour spread showed the greatest agreement with pathology showing a mean agreement of 0.5 mm when compared with pathology [5]. Since survival and local recurrence outcomes for T2 and early T3 tumours are identical and with increasing use of precision depth of spread measurements afforded by preoperative high-resolution MRI, preoperative decisions regarding chemoradiotherapy (CRT) are increasingly based on the 5 mm depth of extramural spread cut-off rather than the T2/T3 boundary. As further evidence to support this practice, a 5-year follow-up from the MERCURY study, Taylor et al. showed that MRI staged rectal cancers with <5 mm depth of spread 85% 5-year overall survival and 3% local recurrence rates, thus supporting the use of a more rigorous preoperative stratification of rectal cancer patients [6].
Circumferential Resection Margin (CRM)
The importance of tumour spread within 1 mm of the surgical circumferential resection margin (CRM) is well known [7, 8]. The appearance of the predicted CRM on MRI was first described in 1999 and was shown as a low signal intensity structure surrounding the mesorectum on high-resolution imaging. High-resolution MRI is the most accurate imaging modality for consistently identifying the mesorectal fascia and thus the CRM [9]. The first prospective study was conducted in 98 patients and showed that if the distance of tumour was 1 mm or less to the mesorectal fascia, this predicted pathological CRM involvement with 92% agreement (kappa = 0.81) [10]. The high-resolution technique needed to be strictly adhered to but was considered that if the protocol was adhered to and image interpretation criteria established by Brown et al. were followed, then this could be reproduced in a multicentre setting. In 2003, the MERCURY group comprising 11 hospitals in the UK and Europe prospectively tested the hypothesis that tumour depth and distance to CRM could agree with histopathology findings in a multicentre setting. Following TME surgery 327 (94%) patients were found to have clear margins on histopathology [11]. The specificity was 92% (CI 90–95%). The group showed a high risk of pCRM involvement if tumour distance to the mesorectal fascia was 1 mm or less. In a follow-up paper evaluating outcomes of these patients, MRI proved to be as likely to predict the risk of local recurrence as pCRM involvement. When the MRI suggested that the tumour was ≤1 mm from the mesorectal fascia, there was a 20% local recurrence rate compared with 7.1% in the mrCRM ‘clear’ group [6, 12]; the local recurrence rates were identical for patients with pCRM involvement. The group also showed that increasing the threshold for risk of CRM involvement by widening this distance to 2 mm or more did not improve the prediction of likely CRM involvement and would result in substantial overtreatment and toxicity for such patients.
Node Stage
In the pre-TME era, nodal involvement was unsurprisingly a predictor for pelvic recurrence [13]. Patients undergoing non-TME surgery experienced local recurrence rates that ranged from 20 to 40% that were strongly linked to mesorectal disease left in the pelvis after suboptimal surgery. The use of preoperative radiotherapy in such patients was associated with a reduction in local recurrence rates to 20%, but this was clearly not an effective compensatory approach for poor quality surgery. The Scandinavians subsequently adopted a nationwide training and accreditation programme of TME surgery spearheaded by Lars Pahlman [14]. When an approach that employed high-quality TME resection was adopted, the local recurrence rates dramatically reduced. Thus in the TME era, lymph node status per se does not confer any additional risk of local recurrence in patients provided that tumour does not extend to within 1 mm of the mesorectal fascia [15].
The assessment of lymph node status remains important in patients with early rectal cancer treated by local excision. The benefits of the reduced morbidity and organ preservation afforded by a less radical technique must be balanced against the potential risk of small volume disease remaining in the mesorectal nodes which may relapse. It is evident that relying on nodal size alone is highly inaccurate and likely to result in incorrect assessments of nodal positivity. Firstly the favoured cut-off of 5 mm fails as the majority of patients with rectal cancer have small (<5 mm) mesorectal lymph nodes that contain a tumour [16]. There is considerable overlap between the size of reactive nodes and nodes containing tumour metastases such that no size cut-off can be relied upon. By determining mixed intranodal signal and irregularity of the border, which are features evident on high-resolution imaging, MRI can determine lymph node involvement with 85% accuracy compared with histopathology reference standard [10]. Morphological assessment has the additional advantage of displaying the anatomic distribution of nodes both within and outside the mesorectum. Another crucial advantage that had previously been unavailable to patients following local excision is that MRI can be used to serially monitor the evolution of nodal morphology such that a progressive change in morphological appearances by close monitoring will enable early identification and resection in patients with residual mesorectal disease. Hence, node morphology and serial 3 monthly high-resolution MRI evaluation is a helpful assessment technique following local excision in patients desiring an organ preservation approach.
Extramural Vascular Invasion (EMVI)
Extramural vascular invasion (EMVI) is defined as the presence of tumour in the vasculature beyond the muscularis propria and was first described by Grinnell in the 1930s. In 1980 and 1981, Ian Talbot at St Marks undertook a comprehensive histological assessment of venous invasion in patients with rectal cancer with follow-up of outcomes. He concluded that tumour invasion into ‘thick-walled’ extramural veins occurred in 52% of 703 surgical specimens from patients with adenocarcinoma of the rectum, the corrected 5-year survival rate was significantly worse and liver metastases developed more frequently when venous invasion was present with only a 33% 5-year survival [17]. Several subsequent histopathological studies confirmed the relationship between venous invasion and the risk of local failure, distant metastases and reduced survival [17,18,20]. Metastatic disease in the liver is more strongly linked to EMVI than nodal status and is now the principle cause of death in patients treated with rectal cancer. Thus a preoperative search for this feature and careful systematic follow-up of patients is certainly warranted. Unfortunately the focus on lymph node involvement has resulted in relative neglect of this important prognostic marker, and in several histopathologic audits, the identification of extramural venous invasion is generally underreported [20,21,22,24]. The strict histopathologic definition is tumour involvement of a vascular structure with a smooth muscle wall that will contain elastin on elastic staining [25]. However many laboratories do not undertake this form of assessment, and pathologists do not universally recognise the significance of an isolated tumour deposit seen close to an arterial structure, without an accompanying vein [26].
High-resolution MRI has an inherent advantage in being able to depict the anatomical course of veins as serpiginous structures that are of low signal intensity (signal void—due to flowing blood in large and small veins). Furthermore, multiplanar imaging enables tracking of the anatomic course and calibre of veins. The ability to identify EMVI on both CT and MRI had previously been unrecognised but now established as a significant prognostic indicator. The first imaging study to document this by imaging was carried out in 98 patients undergoing TME surgery with histopathologic correlation; the technique was shown to have a positive predictive value of 85% percent. The radiological characteristics of EMVI as seen on MRI have been described in detail [26]. Unlike nodal status, in TME specimens, tumour assessment of EMVI on MRI remains an important predictor of both local and distant failure [27] and will arguably make a better prognostic biomarker for the use of neoadjuvant chemotherapy.
Post-Treatment Assessment of Extramural Vascular Invasion (ymrEMVI)
A positive mrEMVI is associated with poor survival outcomes. The 3-year overall survival for mrEMVI-positive patients was 35% compared with 74% for mrEMVI-negative patients; mrEMVI-positive patients also had a fourfold increased risk of developing distant metastasis (52 vs. 12%) [26].
Yu et al. report that 78% (219/281) of patients had evidence of mrEMVI on the baseline MRI (96% of patients had ≥ mrT3c). These patients were significantly less likely to respond to CRT than mrEMVI-negative patients (OR 2.5 [CI 1.36–4.54] p = 0.02). However when preoperative chemotherapy was used with radiotherapy, mrEMVI was more likely to change from positive to negative and was associated with good overall outcomes. It is hypothesised that this subgroup of patients may benefit from the treatment intensification by the additional use of chemotherapy following chemoradiotherapy. These strategies for managing persistent ymrEMVI will be investigated as part of the phase III multicentre TRIGGER trial (NCT02704520).
Tumour Height: The Problem with Low Rectal Cancers
In determining the feasibility of sphincter preservation, a crucial assessment is the distal margin of clearance from the lowest portion of tumour to the anal verge and sphincter complex and the radial extent of tumour above the level of the sphincter complex. The height of rectal cancer is usually measured from the anal verge and can be readily assessed on clinical digital rectal examination, rigid sigmoidoscopy or endoscopic assessment. Radiological assessment permits an objective assessment of the lowermost edge of the tumour to the anatomic sphincter and anal verge.
For ease of classification , it is common to classify the rectum into three: the lower rectum 6 cm or less from the anal verge, the mid-rectum (from 7 to 11 cm) and the upper rectum (from 12 to 15 cm) [28]. These measurements are somewhat arbitrary and will be subject to usual variation depending on the patient’s body habitus. For practical purposes, the majority of patients with tumours arising at 6 cm or less from the anal verge have tumours located in the distal, tapering portion of the mesorectum and located at the anatomically challenging portion of the conventional TME dissection due to the physical narrowing of the pelvis and proximity to nearby vital structures such as the prostate, vagina and neurovascular bundle that are all vulnerable to collateral damage. Thus we can anatomically define the lower third of the rectum as the portion arising below the level of the proximal origin of the levators [29]. These tumours have been shown to be at increased risk of an involved CRM, with routine abdominal perineal excisions being undertaken with TME plane surgery. In such patients CRM positivity rates of up to 30% had been reported in nearly all series [11, 29,30,32] with higher recurrence rates [33, 34], mortality rates [33], high permanent stoma rates [35] and poor function after sphincter conservation [36, 37]. A precise preoperative staging system that could enable assessment of the radial planes and feasibility of TME plane surgery in achieving clear radial margins was proposed as a way to improve the universally poor outcomes observed in such patients. An MRI staging system was derived which involved assessment of tumour at or below the puborectalis sling and an assessment of the degree of clearance to the intersphincteric plane . For tumours with >1 mm clearance, a TME plane could be considered with potential sphincter conservation, but for tumours that extended to within 1 mm of the intersphincteric plane or beyond, a more radical approach would be needed. In addition, assessment of other factors such as extramural spread, presence of EMVI on MRI and mesorectal fascia invasion could all be combined to provide an overall prognostic risk. By testing this staging system prospectively, the MERCURY group showed that CRM positivity rates could be reduced from 30% to <15%. Furthermore, an MRI prediction of a safe TME plane without adverse prognostic features was observed in 50% of patients and was associated with pCRM risk of <2%. On the other hand, preoperative identification of high-risk features combined with preoperative therapy and good tumour regression was associated with a low risk of pCRM involvement. Finally, patients with a poor response to treatment and persistence of tumour extension into the TME plane could be identified as having a maintained risk of CRM involvement, and more radical surgery was justified in this group [38].
Magnetic Resonance Tumour Regression Grade (mrTRG)
Following chemoradiotherapy a number of radiation-induced tissue changes occur. These include oedema, inflammation, necrosis and fibrosis. The assessment of postirradiated tissue is challenging with all imaging modalities. However, advances in MRI have enabled high-resolution (3 mm) slices to be oriented through the plane of the tumour; consequently the accuracy of MRI has increased. This improved appreciation of the reactive changes that occur in normal rectal tissue after chemoradiotherapy and led to a better understanding of the appearance of residual disease on the post-treatment MRI.
The T2-weighted sequences of high-resolution MRI have a unique ability to distinguish fibrosis from tumour based on the signal intensity differences. Tumour characteristically maintains both its high signal intensity and its disruption of the anatomical layers, whereas fibrosis is characterised by low (dark) signal intensity. By examining the proportion of tumour to fibrotic signal intensity after treatment, it is possible to derive an MRI-based tumour regression grade. This scoring system is based on the pathological tumour regression grade systems and most closely resembles the Mandard pTRG [39]. In an analysis of 111 patients undergoing preoperative radiotherapy in the MERCURY trial, mrTRG was compared to other staging factors. The group reported a significant difference in disease-free survival (DFS) and overall survival (OS) between mrTRG 1–3 (good response) and mrTRG 4–5 (poor response) (p < 0.001); the 5-year DFS was 72% and 27%, respectively. Our own single-centre experience has also found a significant difference in DFS and OS: mrTRG 1 and 2 (good response), mrTRG 3 (intermediate response) and mrTRG 4–5 (poor response) had a 3-year DFS of 82%, 72% and 61%, respectively. In these independent series, mrTRG identifies prognostically distinct groups. This suggests that mrTRG can distinguish between ‘good’ and ‘poor’ responders to chemoradiotherapy.
Patients with mrTRG 4 and 5 have relatively little response to preoperative therapy. As expected this group has a significantly higher risk of CRM involvement, distant failure and poor overall survival compared with patients that have mrTRG 1–3 [40, 41]. On the other hand, mrTRG 1 and 2 are strongly predictive of pathological complete response (pCR). If surgery is performed immediately, mrTRG 1 and 2 are associated with an identical survival outcome to pCR [40]. In two further series, the interobserver reliability between radiologists has been reported as moderate to substantial with kappa values of 0.55–0.65, compared with 0.41 (a slight to fair agreement) for the ymrT assessment [40, 41]. Finally, mrTRG 1 and 2 are associated with a high probability of either no residual tumour or tumour of uncertain viability—this has been used to good effect in two scenarios: (1) in predicting clear CRM in patients with advanced low rectal cancers having a good mrTRG response as 0/33 patients with mrTRG 1–2 had involved CRM and (2) in identifying patients achieving radiological complete response as being suitable for a deferral of surgery approach. The latter is being tested in a prospective phase III trial where patients randomised to an mrTRG-based treatment pathway will be offered deferral of surgery. Comparison with pathologic complete response has shown that radiological complete response based on mrTRG 1–2 identified four times more patients with a similar outcome to pCR.
Conclusion
High-resolution dedication rectal magnetic resonance imaging plays a central role in the management of patient with rectal cancer. It is reliable for evaluating the risk for circumferential margin involvement at surgery and can identify patients who may be safely treated with surgery without radiotherapy or those requiring extended resection beyond the TME plane. The presence of MRI features such as EMVI can identify patients at high risk for systemic failure who may benefit from systemic treatment. Finally, post-treatment MRI can help to identify patients with complete treatment response who may be candidates for surgery deferral.
References
Cawthorn SJ, Parums DV, Gibbs NM, A'Hern RP, Caffarey SM, Broughton CI, Marks CG. Extent of mesorectal spread and involvement of lateral resection margin as prognostic factors after surgery for rectal cancer. Lancet. 1990;335(8697):1055–9.
Willett CG, Badizadegan K, Ancukiewicz M, Shellito PC. Prognostic factors in stage T3N0 rectal cancer: do all patients require postoperative pelvic irradiation and chemotherapy? Dis Colon Rectum. 1999;42(2):167–73.
Merkel S, Mansmann U, Siassi M, Papadopoulos T, Hohenberger W, Hermanek P. The prognostic inhomogeneity in pT3 rectal carcinomas. Int J Colorectal Dis. 2001;16(5):298–304.
Compton CC, Greene FL. The staging of colorectal cancer: 2004 and beyond. CA Cancer J Clin. 2004;54(6):295–308.
MERCURYStudyGroup. Extramural depth of tumor invasion at thin-section MR in patients with rectal cancer: results of the MERCURY study. Radiology. 2007;243(1):132–9.
Taylor FG, Quirke P, Heald RJ, Moran B, Blomqvist L, Swift I, Sebag-Montefiore DJ, Tekkis P, Brown G. Preoperative high-resolution magnetic resonance imaging can identify good prognosis stage I, II, and III rectal cancer best managed by surgery alone: a prospective, multicenter, European study. Ann Surg. 2011;253(4):711–9.
Wibe A, Rendedal PR, Svensson E, Norstein J, Eide TJ, Myrvold HE, Soreide O. Prognostic significance of the circumferential resection margin following total mesorectal excision for rectal cancer. Br J Surg. 2002;89(3):327–34.
Adam IJ, Mohamdee MO, Martin IG, Scott N, Finan PJ, Johnston D, Dixon MF, Quirke P. Role of circumferential margin involvement in the local recurrence of rectal cancer. Lancet. 1994;344(8924):707–11.
Bissett IP, Fernando CC, Hough DM, Cowan BR, Chau KY, Young AA, Parry BR, Hill GL. Identification of the fascia propria by magnetic resonance imaging and its relevance to preoperative assessment of rectal cancer. Dis Colon Rectum. 2001;44(2):259–65.
Brown G, Radcliffe AG, Newcombe RG, Dallimore NS, Bourne MW, Williams GT. Preoperative assessment of prognostic factors in rectal cancer using high-resolution magnetic resonance imaging. Br J Surg. 2003;90(3):355–64.
MERCURYStudyGroup. Diagnostic accuracy of preoperative magnetic resonance imaging in predicting curative resection of rectal cancer: prospective observational study. BMJ. 2006;333(7572):779.
Taylor FG, Quirke P, Heald RJ, Moran B, Blomqvist L, Swift I, St Rose S, Sebag-Montefiore DJ, Tekkis P, Brown G. One millimetre is the safe cut-off for magnetic resonance imaging prediction of surgical margin status in rectal cancer. Br J Surg. 2011;98(6):872–9.
SwedishRectalCancerTrial. Improved survival with preoperative radiotherapy in resectable rectal cancer. N Engl J Med. 1997;336(14):980–7.
Pahlman L, Karlbom U. Teaching efforts to spread TME surgery in Sweden. Recent Results Cancer Res. 2005;165:82–5.
Chand M, Heald RJ, Brown G. The importance of not overstaging mesorectal lymph nodes seen on MRI. Color Dis. 2013;15(10):1201–4.
Dworak O. Number and size of lymph nodes and node metastases in rectal carcinomas. Surg Endosc. 1989;3(2):96–9.
Talbot IC, Ritchie S, Leighton MH, Hughes AO, Bussey HJ, Morson BC. The clinical significance of invasion of veins by rectal cancer. Br J Surg. 1980;67(6):439–42.
Gunther K, Dworak O, Remke S, Pfluger R, Merkel S, Hohenberger W, Reymond MA. Prediction of distant metastases after curative surgery for rectal cancer. J Surg Res. 2002;103(1):68–78.
Rich T, Gunderson LL, Lew R, Galdibini JJ, Cohen AM, Donaldson G. Patterns of recurrence of rectal cancer after potentially curative surgery. Cancer. 1983;52(7):1317–29.
Smith NJ, Barbachano Y, Norman AR, Swift RI, Abulafi AM, Brown G. Prognostic significance of magnetic resonance imaging-detected extramural vascular invasion in rectal cancer. Br J Surg. 2008;95(2):229–36.
Kirsch R, Messenger DE, Riddell RH, Pollett A, Cook M, Al-Haddad S, Streutker CJ, Divaris DX, Pandit R, Newell KJ, Liu J, Price RG, Smith S, Parfitt JR, Driman DK. Venous invasion in colorectal cancer: impact of an elastin stain on detection and interobserver agreement among gastrointestinal and nongastrointestinal pathologists. Am J Surg Pathol. 2013;37(2):200–10.
Messenger DE, Driman DK, Kirsch R. Developments in the assessment of venous invasion in colorectal cancer: implications for future practice and patient outcome. Hum Pathol. 2012;43(7):965–73.
Messenger DE, Driman DK, Kirsch R. Authors’ response – the prognostic benefits of routine staining with elastica to increase detection of venous invasion in colorectal cancer specimens. J Clin Pathol. 2012;65(5):470.
Messenger DE, Driman DK, McLeod RS, Riddell RH, Kirsch R. Current practice patterns among pathologists in the assessment of venous invasion in colorectal cancer. J Clin Pathol. 2011;64(11):983–9.
Howlett CJ, Tweedie EJ, Driman DK. Use of an elastic stain to show venous invasion in colorectal carcinoma: a simple technique for detection of an important prognostic factor. J Clin Pathol. 2009;62(11):1021–5.
Smith NJ, Shihab O, Arnaout A, Swift RI, Brown G. MRI for detection of extramural vascular invasion in rectal cancer. AJR Am J Roentgenol. 2008;191(5):1517–22.
Chand M, Evans J, Swift RI, Tekkis PP, West NP, Stamp G, Heald RJ, Brown G. The prognostic significance of postchemoradiotherapy high-resolution MRI and histopathology detected extramural venous invasion in rectal cancer. Ann Surg. 2015;261(3):473–9.
Salerno G, Sinnatamby C, Branagan G, Daniels IR, Heald RJ, Moran BJ. Defining the rectum: surgically, radiologically and anatomically. Colorectal Dis. 2006;8(Suppl 3):5–9.
Moran BJ, Holm T, Brannagan G, Chave H, Quirke P, West N, Brown G, Glynne-Jones R, Sebag D, Cunningham C, Janjua AZ, Battersby N, Crane S, McMeeking A. The English national low rectal cancer development programme (LOREC): key messages and future perspectives. Color Dis. 2014;16:173.
Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AM, Heath RM, Brown JM. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet. 2005;365(9472):1718–26.
Marr R, Birbeck K, Garvican J, Macklin CP, Tiffin NJ, Parsons WJ, Dixon MF, Mapstone NP, Sebag-Montefiore D, Scott N, Johnston D, Sagar P, Finan P, Quirke P. The modern abdominoperineal excision: the next challenge after total mesorectal excision. Ann Surg. 2005;242(1):74–82.
Nagtegaal ID, van de Velde CJ, Marijnen CA, van Krieken JH, Quirke P. Low rectal cancer: a call for a change of approach in abdominoperineal resection. J Clin Oncol. 2005;23(36):9257–64.
Nagtegaal ID, Quirke P. What is the role for the circumferential margin in the modern treatment of rectal cancer? J Clin Oncol. 2008;26(2):303–12.
Jorgren F, Johansson R, Damber L, Lindmark G. Oncological outcome after incidental perforation in radical rectal cancer surgery. Int J Color Dis. 2010;25(6):731–40.
Birbeck KF, Macklin CP, Tiffin NJ, Parsons W, Dixon MF, Mapstone NP, Abbott CR, Scott N, Finan PJ, Johnston D, Quirke P. Rates of circumferential resection margin involvement vary between surgeons and predict outcomes in rectal cancer surgery. Ann Surg. 2002;235(4):449–57.
Moran BJ. Predicting the risk and diminishing the consequences of anastomotic leakage after anterior resection for rectal cancer. Acta Chir Iugosl. 2010;57(3):47–50.
Rullier E, Laurent C, Garrelon JL, Michel P, Saric J, Parneix M. Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg. 1998;85(3):355–8.
Battersby NJ, How P, Moran B, Stelzner S, West NP, Branagan G, Strassburg J, Quirke P, Tekkis P, Pedersen BG, Gudgeon M, Heald B, Brown G, MERCURY II Study Group. Prospective validation of a low rectal cancer magnetic resonance imaging staging system and development of a local recurrence risk stratification model: the MERCURY II study. Ann Surg. 2015;263:751.
Mandard AM, Dalibard F, Mandard JC, Marnay J, Henry-Amar M, Petiot JF, Roussel A, Jacob JH, Segol P, Samama G, et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer. 1994;73(11):2680–6.
Patel UB, Taylor F, Blomqvist L, George C, Evans H, Tekkis P, Quirke P, Sebag-Montefiore D, Moran B, Heald R, Guthrie A, Bees N, Swift I, Pennert K, Brown G. Magnetic resonance imaging-detected tumor response for locally advanced rectal cancer predicts survival outcomes: MERCURY experience. J Clin Oncol. 2011;29(28):3753–60.
Salerno GV, Daniels IR, Moran BJ, Heald RJ, Thomas K, Brown G. Magnetic resonance imaging prediction of an involved surgical resection margin in low rectal cancer. Dis Colon Rectum. 2009;52(4):632–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2018 Springer International Publishing AG
About this chapter

Cite this chapter
Brown, G. (2018). Magnetic Resonance Imaging of the Rectum. In: Chang, G. (eds) Rectal Cancer. Springer, Cham. https://doi.org/10.1007/978-3-319-16384-0_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-16384-0_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-16383-3
Online ISBN: 978-3-319-16384-0
eBook Packages: MedicineMedicine (R0)