
Abstract
Most of the daily dietary tryptophan (Trp) is oxidatively degraded through the kynurenine (Kyn) pathway, and the remaining may be consumed either in serotonin synthesis or in conversion into melatonin through the methoxyindole pathway. Trp degradation products along the Kyn pathway include three neuroactive metabolites: the neuroinhibitory agent kynurenic acid (KA), the free radical generator 3-hydroxykynurenine (3HK), and the excitotoxin quinolinic acid (QA). Kyn is the major metabolite of Trp and is readily transported across the blood–brain barrier into the brain where it can be further metabolized in perivascular macrophages, microglia, and astrocytes, also to generate neuroactive intermediates. In contrast to Kyn, QA, KA, and 3-hydroxyanthranilic acid (3HAA) penetrate through the blood–brain barrier only poorly due to its polar nature. Although the cytokines do not pass through the blood–brain barrier, their signals reach the brain through humoral, neural, and cellular pathways and stimulate Trp degradation by interacting with a cytokine network in the brain. The induction of Kyn pathway by indoleamine 2,3-dioxygenase (IDO) activity exhausts l-Trp in the medium and produces toxic metabolites. While Kyn to Trp ratio reflects IDO activity, Kyn to KA ratio indicates the neurotoxic challenge. Alpha7 nicotinic acetylcholine receptor (alpha7nAChR) constitutes a crucial link between excessive KA formation and reduction in glutamate. KA-induced reduction in prefrontal glutamate levels emerges as a result of alpha7nAChR inhibition. Changes in the endogenous concentrations of KA, as a potent alpha7nAChR and N-methyl-D-aspartate (NMDA) receptor antagonist, affect extracellular dopamine levels in the brain. The entire monoaminergic neurotransmission involves functional interactions between serotonin, norepinephrine, and dopamine systems (Fig. 1.1). Serotonin transporter (SERT) reuptakes biogenic amine neurotransmitters following release in the nervous systems and terminates the action of serotonin. SERT can be regulated by a membrane-bound G-protein-coupled receptor, and this occurs via nitric oxide (NO) and cyclic guanosine monophosphate (cGMP). Desensitization and re-sensitization of G-protein-coupled receptors (GPCRs) can modulate receptor responsiveness in regulation of many cellular functions. Diet restriction-induced exaggerated feedback control over serotonin synthesis decreases serotonin neurotransmission at postsynaptic sites by reducing availability of Trp. Enterochromaffin (EC) cells of the intestinal mucosa respond to chemical and mechanical stimuli by releasing serotonin. The enteric serotonin transporter plays a critical role in serotonergic neurotransmission and in the initiation of peristaltic and secretory reflexes.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Tryptophan
- Kynurenine
- Kynurenic acid
- Quinolinic acid
- Indoleamine 2,3-dioxygenase
- N-Methyl-D-aspartate receptor
- Serotonin
- Serotonin transporter
- Serotonin receptors
1.1 Introduction
Amino acids are not only regulators of gene expression and the protein phosphorylation cascade but are also cell signaling molecules. Carbon skeletons of essential amino acids cannot be synthesized by animal cells and, therefore, must be provided from the diet (Wu 2010). The average daily nutritional requirement of l-tryptophan (Trp) as an essential amino acid is 5 mg/kg. In order to improve mood or sleep, many adults may consume Trp much more, up to 4–5 g/day (60–70 mg/kg) (Fernstrom 2012). Ninety-five percent of dietary Trp is oxidatively degraded in the liver through the kynurenine (Kyn) pathway. Actually there are two rate-limiting enzymes of Kyn formation: first, tryptophan 2,3-dioxygenase (TDO) and, the second, indoleamine 2,3-dioxygenase (IDO) (Marazziti et al. 2013). TDO reaction generates nicotinamide adenine dinucleotide [NAD+] following Trp oxidation. A small amount of Trp degradation can also occur extrahepatically by the enzyme IDO. IDO is expressed by a large variety of cells and can be directly activated by proinflammatory cytokines such as interferon (IFN)-gamma and tumor necrosis factor (TNF)-alpha, whereas TDO is only located in the liver cells and is activated by stress hormones (Wirleitner et al. 2003). Degradation of Trp mainly occurs along the Kyn pathway. Eventually Kyn is metabolized along one of two catabolic branches, leading to the formation of either hydroxykynurenine (3HK) and quinolinic acid (QA) or kynurenic acid (KA). The cerebral Kyn pathway is driven mainly by blood-borne l-Kyn, which enters from the circulation to the brain using the large neutral amino acid transporter, whereas QA, KA, and 3-hydroxyanthranilic acid (3HAA) cannot pass the blood–brain barrier easily (Fig. 1.1) (Fukui et al. 1991). In the brain, l-Kyn is then rapidly taken up by astrocytes and, presumably, by microglial cells. Almost all enzymes of the Kyn pathway are primarily contained in astrocytes and microglial cells (Schwarcz 2004). However, astrocytes do not contain kynurenine 3-hydroxylase and therefore favor KA synthesis, whereas microglial cells have very little kynurenine aminotransferase (KAT) activity which catalyzes the irreversible transamination of l-Kyn to KA and preferentially forms intermediates of the QA (Guillemin et al. 2001). KA can antagonize the neuronal degeneration mediated by excessive stimulation of N-methyl-D-aspartate (NMDA) receptors in vivo (Lekieffre et al. 1990). During the stress response 100- to 1,000-fold elevations in 3HK and QA occur upon microglial cell activation or macrophage infiltration to the brain (Schwarcz 2004). 3HK generates free radical species that can cause oxidative stress and lipid peroxidation. QA-induced excitation and neurotoxicity are mediated by N-methyl-D-aspartate receptor (NMDA) receptors. Because of the absence of effective removal mechanisms for extracellular QA (Foster et al. 1984), its ability to induce concentration-dependent increases in reactive oxidative species (ROS) formation (Santamaría et al. 2001), and its specific interaction with the NMDA receptor (De Carvalho et al. 1996), QA is particularly excitotoxin, whereas KA acts as a competitive blocker of the glycine co-agonist site of the NMDA receptor (Kessler et al. 1989) and as a noncompetitive inhibitor of the alpha7 nicotinic acetylcholine receptor (alpha7nAChR) (Hilmas et al. 2001). Therefore, KA is considered to be neuroprotective.

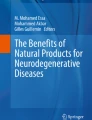
Catabolic cascade of tryptophan metabolism. A simplified version of the kynurenine, serotonin, and methoxyindole pathways demonstrating the major enzymes, intermediates, and receptors. TDO tryptophan 2,3-dioxygenase, IDO indoleamine 2,3-dioxygenase, SOCS suppressor of cytokine signaling, STAT1-alpha signal transducer and activator of transcription 1-alpha, IRF-1 interferon regulatory factor-1, NF-kappaB nuclear factor kappa B, p38-MAPK p38 mitogen-activated protein kinase, IDO-ITIM immunoreceptor tyrosine-based inhibitory motif for IDO, IFN-gamma interferon gamma, IFN-alpha, interferon alpha, TNF-alpha tumor necrosis factor alpha, IL-6 interleukin-6, ROS reactive oxygen species, RNS reactive nitrogen species, NMDAR N-methyl-D-aspartate receptor, NAD+ nicotinamide adenine dinucleotide, hpTrpH1 human peripheral tryptophan hydroxylase1, hnTrpH2 human neural tryptophan hydroxylase2, BH4 tetrahydrobiopterin, qBH2 quinonoid dihydrobiopterin, alpha7nAChR alpha7 nicotinic acetylcholine receptor, AA-NAT arylalkylamine-N-acetyltransferase, HIOMT hydroxyindole-O-methyltransferase, 5-HT2A, 5-HT2C, 5-HT1B, 5-HT1A serotonin receptors, Gi inhibitory G protein, Gs stimulatory G protein, SSRI selective serotonin reuptake inhibitor, SERT serotonin transporter, sIPSC spontaneous inhibitory postsynaptic currents, GABA gamma-aminobutyric acid, cAMP cyclic adenosine monophosphate, MT1, MT2 membrane-bound melatonin receptors
In the second metabolic pathway of l-Trp degradation, a small amount of Trp is converted to 5-hydroxytryptophan by the tetrahydrobiopterin (BH4)-dependent tryptophan hydroxylase (TrpH). Subsequently aromatic amino acid decarboxylase (AAADC) catalyzes the second step of serotonin synthesis (Chen and Miller 2012).
The third metabolic pathway of l-Trp degradation involves its conversion into melatonin through the methoxyindole pathway. Biosynthetic steps of melatonin comprise two major rate-limiting enzymes: arylalkylamine-N-acetyltransferase (AA-NAT) and hydroxyindole-O-methyltransferase (HIOMT). Although transforming of Trp into melatonin originally occurred in pinealocytes, it has been also detected in many other parts of the body, including the eyes, bone marrow, skin, lymphocytes, and enteroendocrine cells of the gastrointestinal tract (Konturek et al. 2007; Srinivasan et al. 2011). However, cytokine-driven Trp degradation pathways and how they influence each other under different physiologic and pathologic conditions are open to debate.
1.2 Cytokine-Mediated Signaling
Contrary to Kyn, cytokines are relatively large molecules that do not freely pass through the blood–brain barrier. Nevertheless, cytokine signals are able to reach the brain through humoral, neural, and cellular pathways and interact with a cytokine network in the brain consisting of neurons, microglia, and astrocytes (Capuron and Miller 2011). Considering the abovementioned issues, cytokine signals reach to the brain with five different mechanisms: (1) passage of cytokines through the leaky regions of the blood–brain barrier, (2) active transport with cytokine-specific transport molecules on brain endothelium, (3) activation of endothelial cells, (4) transmission of cytokine signals via afferent nerve fibers, and (5) entry into the brain parenchyma and involvement of microglia and astrocytes (Rivest et al. 2000; Konsman et al. 2002; Plotkin et al. 1996).
Cytokine overexpression in the brain due to inflammation is an important factor in the pathogenesis of neurotoxic disorders. However, peripheral and central cytokine compartments appear to be integrated, and their effects might synergize or inhibit each other (Szelényi 2001). Although numerous cytokines and their receptors have been identified in the brain, interleukin-1 (IL-1), IL-6, and TNF-alpha have been implicated in the central control of responses to neuroendocrine, immune, and behavioral alterations (Rothwell et al. 1996). Actually the innate and adaptive immune responses are triggered by microglia in the central nervous system including the release of proinflammatory mediators. In this case toll-like receptor (TLR)-induced activation of microglia and the release of proinflammatory molecules are responsible for neurotoxic processes (Lehnardt 2010). Following activation of the immune system pathways, a number of cytokines alone or in combination including IFN-alpha, IFN-gamma, and TNF-alpha through activation of a number of inflammatory signaling pathways such as signal transducer and activator of transcription 1-alpha (STAT1-alpha), interferon regulatory factor (IRF)-1, nuclear factor (NF) kappa B, and p38 mitogen-activated protein kinase (MAPK) stimulate IDO (Fig. 1.1) (Fujigaki et al. 2006). IDO breaks down Trp into Kyn. Kyn is preferentially converted to KA and QA in astrocytes and in microglia, respectively (Schwarcz and Pellicciari 2002). As mentioned above, activated microglia is a chronic source of multiple neurotoxic molecules, including TNF-alpha, nitric oxide (NO), IL-1beta, and ROS, which cause progressive neuron damage (Lull and Block 2010). Initially released cytokines, IL-1beta and TNF-alpha, signal neuroendocrine, autonomic, limbic, and cortical areas of the central nervous system to control neural activity, behaviors, hormone release, and autonomic functions (Lorton et al. 2006).
Acute activation of pattern-recognition receptors, TLR-4 and TLR-2, by exposing to bacterial lipopolysaccharide and peptidoglycan, respectively, also increases circulating levels of IFN-gamma and potently activates IDO in both the periphery and the brain (Lestage et al. 2002). Indeed glial cells and TLRs are vital components of immune response in the central nervous system. Intrauterine infection/inflammation promotes inflammatory processes in glial cells by upregulating cytokines and by activating signaling pathways and transcriptional factors (Yuan et al. 2010).
Response to cytokines seems to be related to the hypothalamic–pituitary–adrenal (HPA) axis activation. Thus IL-1 administration increases noradrenaline secretion and stimulates indoleamine metabolism and most prominently increases the metabolism of serotonin (5-hydroxytryptamine, 5-HT). IL-6 also induces a short-lived activation of the HPA axis. Its effects on Trp and serotonin metabolism are similar to those of IL-1 (Dunn et al. 1999). Furthermore suppressors of cytokine signaling (SOCS) proteins are critical modulators of cytokine-mediated processes, and janus kinase 2 (JAK)–STAT–SOCS signaling modules can have diverse effects on inflammatory diseases (O’Shea and Murray 2008). In the long term, IL-6-dependent upregulation of SOCS3 is responsible for inhibiting the IFN-gamma-driven transcriptional expression of IDO (Fig. 1.1) (Orabona et al. 2004). Hence, an inverse correlation between SOCS3 and IDO expression is evident. Immunomodulatory mechanisms extensively use negative regulators in the form of signaling proteins bearing one or more immunoreceptor tyrosine-based inhibitory motifs (ITIMs). IL-6 upregulates SOCS3 and promotes SOCS3 binding to ITIMs of IDO. This process causes shortening of the half-life and proteasome-mediated degradation of IDO (Orabona et al. 2008).
1.3 IDO-Mediated Signaling
The extrahepatic Trp degradation enzyme IDO is induced by IFN-gamma-mediated effects of the STAT1-alpha and IRF-1. The induction of IDO can also be mediated through an IFN-gamma-independent mechanism which may be related to the activity of the p38-MAPKinase pathway and NF-kappaB (Fujigaki et al. 2006). Actually the enzymatic activity of IDO is enhanced in conditions of acute or chronic activation of the immune system, including immunotherapy, acquired immunodeficiency syndrome, atherosclerosis and coronary heart disease, rheumatoid arthritis, and obesity (Wirleitner et al. 2003). In particular secretion of IFN-gamma is significantly higher in the obese than that of the control subjects. Initially this might be partly dependent on the action of leptin that shifts T-helper (Th) cells toward a Th1 phenotype. A shift to Th1-cytokine profile is dominated by the production of IFN-gamma and is related to insulin resistance in obesity (Pacifico et al. 2006). Hereby T cells and IFN-gamma participate in the regulation of the chronic inflammatory response in obese individuals (Rocha et al. 2008). Chronic inflammation might trigger and maintain the transcriptional induction of IDO-mediated Trp catabolism. Consequently chronic immune activation is the cause for reduced Trp plasma levels in morbidly obese patients (Brandacher et al. 2007). In case of obesity, activation of IDO simultaneously causes excessive synthesis of kynurenines (Brandacher et al. 2006). Furthermore, decrease in Trp levels and subsequent reduction in serotonin due to shift to Kyn pathway provoke satiety dysregulation and ultimately lead to increase in caloric intake and favor obesity (Brandacher et al. 2007). Even after weight reduction in morbidly obese patients, Trp depletion persists (Brandacher et al. 2006). The induction of the Kyn pathway by IDO activity and subsequent decrease in the Trp availability in the brain results in the IFN-alpha-induced depressive symptoms. While Kyn to Trp ratio reflects IDO activity, the Kyn/KA indicates the neurotoxic challenge (Wichers et al. 2005). Higher IDO activity has also been implicated in immune tolerance because it can inhibit the immune response, either by exhausting l-Trp in the medium or producing toxic metabolites. Trp metabolites in the Kyn pathway, such as 3HAA and QA, induce the selective apoptosis in vitro of murine thymocytes and of Th1 but not Th2 cells (Fallarino et al. 2002). As stated above IDO activity is characterized best by the Kyn to Trp ratio, but considering the immune tolerance, it should be correlated with the concentration of immune activation marker such as neopterin (Schröcksnadel et al. 2006).
Until recently, the conversion of Trp to N-formylkynurenine was thought to be performed by either of two enzymes, TDO and IDO. However a third enzyme, indoleamine 2,3-dioxygenase-2 (IDO2) [indoleamine 2,3-dioxygenase-like protein (INDOL1) or proto-indoleamine 2,3-dioxygenase (proto-IDO)], with the Trp degradation activity has been described (Ball et al. 2009). Although IDO2 is not as widely expressed as IDO (IDO1), it is also expressed in antigen-presenting dendritic cells where Trp catabolism drives immune tolerance. Like IDO, IDO2 catabolizes Trp and triggers phosphorylation of the translation initiation factor eIF2alpha. Trp restoration switches off this signaling pathway when activated by IDO, but not IDO2, arguing that IDO2 has a distinct signaling role (Metz et al. 2007). IDO2 has 43 % similarity to classical IDO protein and shares the same critical catalytic residues. Although IDO2 enzyme activity is weaker than IDO, it is less sensitive to dextro-methyl tryptophan inhibition than IDO. Thus a more recent study indicated that human CD4+ and CD8+ T-cell proliferation was inhibited by IDO2, but both levo-1-methyl tryptophan and dextro-methyl tryptophan which are the gold standard inhibitors of IDO enzyme activity could not reverse IDO2-mediated arrest of cell proliferation, even at high concentrations (Qian et al. 2012). In fact, IDO-dependent tolerogenic effects induced by transforming growth factor beta (TGF-beta) are abolished by IDO gene silencing, but not by the use of 1-methyltryptophan. TGF-beta/IDO/phosphotyrosine phosphatase SHP-1 axis activates the anti-inflammatory NF-kappaB pathway by inhibiting the IL-1 receptor-associated kinase-1 (Orabona et al. 2012).
1.4 Aryl Hydrocarbon Receptor Activation
Gene transcription in response to xenobiotics can be stimulated by aryl hydrocarbon receptor (AhR) which is one of the several ligand-dependent intracellular responsive elements (Denison and Nagy 2003). In this respect Trp photoproducts modulate light-dependent regulation of circadian rhythm through triggering of AhR signaling. Thus these by-products, including 6-formylindolo(3,2-b)carbazole, have high affinity for AhR (Mukai and Tischkau 2007). Ligand activation provokes the AhR to migrate from cytosol to the nucleus and form a complex with the aryl hydrocarbon nuclear translocator (ARNT) that can bind dioxin-responsive elements in the promoter regions of xenobiotic-metabolizing cytochrome P450 (CYP1A) enzymes and 2,3,7,8-tetrachlorodibenzo-p-dioxin-inducible poly (ADP-ribose) polymerase (PARP7) (TiPARP) (Diani-Moore et al. 2010). TiPARP is an AhR target gene that can mediate a 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) toxicity. TCDD suppresses glucose metabolism-related pathways such as hepatic glucose production, expression of key gluconeogenic genes, phosphoenolpyruvate carboxykinase, and glucose-6-phosphatase activities, and NAD+ levels. Nicotinamide, a known precursor of NAD+, is an AhR antagonist. There is a link between signaling pathways for AhR toxicity and nutrient homeostasis NAD+/peroxisome proliferator-activated receptor gamma coactivator 1 alpha (PGC1alpha), regulator of mitochondrial biogenesis, and function/silent mating type information regulation 2 homolog 1 [(SIRT1), NAD-dependent deacetylase sirtuin-1] via the AhR target gene TiPARP (Diani-Moore et al. 2010). Consequently the effects of TCDD are mediated through its binding to the AhR, as a ligand-activated transcription factor. Subsequent to binding AhR, TCDD inhibits CD4+ T-cell differentiation into T helper (Th)1, Th2, and Th17 effector cells while inducing forkhead transcription factor (Foxp3)-negative and/or preserving Foxp3+ regulatory T cells (Tregs) (Marshall and Kerkvliet 2010). The AhR is a key transcriptional regulator of Th17-cell differentiation. Th17 cells express kynurenine 3-monooxygenase, which is an enzyme involved in catabolism of the Trp metabolite Kyn (Stephens et al. 2013). On the other hand, activation of AhR induces IDO and IDO2 expression of dendritic cells. Hence AhR activation is an important signaling pathway for IDO expression and displays a critical role in the mechanism leading to the generation of Tregs. Eventually induction of Tregs mediates the immune suppression through the activation of AhRs (Vogel et al. 2008).
1.5 Glutamate Neurotransmission
Inflammatory cytokines and their signaling pathways have significant effects on the synthesis, release, and reuptake of serotonin, dopamine, and glutamate (Miller et al. 2013). In this context, higher glutamate receptor, mGluR1alpha, and lower guanine nucleotide-binding protein (G-protein)-coupled receptor, regulator of G-protein signaling 4 (RGS4) mRNA levels, play an important role in regulating gamma-aminobutyric acid (GABA) and glutamate neurotransmission in the brain cortex by initiating intracellular signaling cascade (Fig. 1.1). Suppression of GABA release in GABA neurons of the prefrontal cortex and diminished glutamate neurotransmission due to NMDA receptor hypofunction are evident in certain cognitive deficits (Volk et al. 2010). Activation of serotonin 5-HT1A receptors or dopamine D (4) receptors downregulates the function of NMDA receptor channel in pyramidal neurons of the prefrontal cortex. Blocking RGS4 function significantly potentiates the 5-HT1A regulation of NMDA receptor. Conversely, overexpression of RGS4 couples RGS4 to serotonin signaling in cortical neurons and attenuates the 5-HT1A effect (Gu et al. 2007). Furthermore elevated levels of KA in the prefrontal cortex may contribute to the abnormal glutamatergic and nicotinic functions in cognitive deficits (Schwarcz et al. 2001; Erhardt et al. 2009). This concept is partly based on the finding that endogenous KA is an astrocyte-derived metabolite of Trp degradation via Kyn pathway (Kiss et al. 2003). As already mentioned above, Trp degradation products along the Kyn pathway include three neuroactive metabolites: the neuroinhibitory agent KA, the free radical generator 3HK, and the excitotoxin QA. Inhibition of kynurenine 3-hydroxylase shifts Kyn pathway metabolism from 3HK formation toward enhanced KA formation in the mature brain. Therefore acute kynurenine 3-hydroxylase inhibition effectively increases KA formation (Ceresoli-Borroni et al. 2007). Following the systemic administration of Kyn, a significant reduction in prefrontal glutamate occurs. Alpha7nAChRs constitutes a crucial link between excessive KA formation and reduction in glutamate. Subsequent to peripheral administration, Kyn penetrates the blood–brain barrier and dose dependently raises extracellular KA levels in the prefrontal cortex. Actually systemic Kyn administration duplicates the reduction in extracellular glutamate seen after a local perfusion of Kyn in the prefrontal cortex. Resultant KA-induced reduction in prefrontal glutamate levels emerges as a result of alpha7nAChRs inhibition (Konradsson-Geuken et al. 2010). The cognitive deficits are likely related to abnormal glutamatergic and cholinergic neurotransmission in the prefrontal cortex. These defects may be secondary to increased levels of the astrocyte-derived KA, which inhibits alpha7AChR and may thereby reduce glutamate release. Fluctuations in endogenous KA formation bidirectionally influence cortical glutamate concentrations. Consequently selective attenuation of cerebral KA production by increasing glutamatergic tone might improve cognitive functions (Wu et al. 2010). Endogenous glutamate acts locally within the striatum via ionotropic receptors to control impulse-independent and transporter-mediated mode of dopamine release. When the KA inhibits the release of glutamate, low glutamate level may inhibit the secretion of dopamine (Borland and Michael 2004). Modulation of glutamate release by the alpha7nAChRs on striatal glutamatergic terminals, in turn, activates presynaptic ionotropic glutamate receptors on striatal dopaminergic nerve terminals (Kaiser and Wonnacott 2000). Decrease in extracellular levels of striatal dopamine due to KA-induced blockade of alpha7nAChRs can be enhanced by stimulating the endogenous formation of KA via kynurenine 3-hydroxylase inhibition (Rassoulpour et al. 2005). Blood-derived Kyn rapidly accesses to KAT II-containing astrocytes, and KA synthesis takes place in astrocytes (Guidetti et al. 2007). Fluctuations in KA indirectly regulate extracellular dopamine levels in the striatum. Acute inhibition of KAT II reduced the de novo synthesis of KA; thus, KAT II is a critical determinant of functionally relevant KA fluctuations (Amori et al. 2009). On the other hand, cytokine-activated Kyn pathway not only depletes Trp but also generates neuroactive metabolites that can significantly influence the regulation of dopamine and glutamate (Miller et al. 2013). Excitotoxic damage is a common pathologic event in a number of neurologic diseases occurring after accumulation of excess extracellular glutamate in the central nervous system and subsequent overstimulation of glutamate receptors. High extracellular glutamate increases risk of glutamate excitotoxicity. However, astrocytes can take up synaptically released glutamate and maintain glutamate homeostasis (Pitt et al. 2003). Nevertheless astrocytes can release glutamate together with the various chemical transmitters which may mediate communication between neurons and astrocytes (Ida et al. 2008). There are complex cross talks between microglia and astrocytes during neuroinflammatory insults which would influence glutamate-dependent responses in astrocytes (Tilleux et al. 2007). Astrocytosis due to the destruction of neurons is accompanied by microglial activation. Actually in proinflammatory processes, activated microglia stimulates the increase in number of astrocytes and enhances mRNA expression of IL-6 (Röhl et al. 2007). Cytokine release from microglia also causes downregulation of mGluR5, mGluR5 protein, and mRNA expression in astrocytes (Tilleux et al. 2007). On the other hand, the inhibition of inducible nitric oxide synthase (iNOS) eliminates the cytokine-induced enhancement of glutamate release, whereas treatment with a NO donor, even in the absence of cytokines, increases glutamate release (Ida et al. 2008). Nonspecific NOS inhibitors decrease the homocysteine-induced lipid peroxidation more than does the selective neuronal nitric oxide synthase (nNOS) inhibitor. In this case homocysteine can induce oxidative injury to nerve terminals, and this effect involves the NMDA receptor stimulation, NOS activation, and associated free radical formation (Jara-Prado et al. 2003). Higher concentration of QA induces concentration-dependent increases in ROS formation in all synaptosomes, but the increase in the production of peroxidized lipids only emerges in the striatum and the hippocampus. These findings suggest that the excitotoxic action of QA involves regional selectivity in the oxidative status of brain synaptosomes (Santamaría et al. 2001). However, NMDA receptor antagonists completely inhibit the increase of QA-induced lipid peroxidation (Santamaría and Ríos 1993).
1.6 Serotonin Neurotransmission
Trp is only available in the diet. It is therefore likely that excessive diet restriction and malnutrition decrease brain serotonin stores. Evidence shows that diet restriction-induced exaggerated feedback control over serotonin synthesis and the smaller availability of Trp decrease serotonin neurotransmission at postsynaptic sites, leading to hyperactivity, depression, and behavioral disorders (Haleem 2012). Conversely excessive l-Trp ingestion raises brain Trp levels and stimulates its conversion to serotonin in neurons. Adverse effects may be seen at higher doses (70–200 mg/kg) and include tremor, nausea, and dizziness. When Trp is taken alone or with a drug that enhances serotonergic effects, it may provoke side effects (Fernstrom 2012). In fact serotonin neurotransmission comprises multiple consecutive processes including synthesis, storage/release, signaling, reuptake, and metabolism, of which the first step, synthesis, is a critical modulator of serotonin neurotransmission (Chen and Miller 2012). Serotonin is synthesized by a two-step enzymatic reaction. Firstly, the essential amino acid l-Trp is hydroxylated into 5-hydroxy-l-tryptophan by the limiting enzyme TrpH. Two isoforms of TrpH enzyme, TrpH1 and TrpH2, have been characterized so far: TrpH1 is mainly expressed in the gastrointestinal tract and the pineal gland, whereas TrpH2 is primarily expressed in the central nervous system (Watts 2009). TrpH2 polymorphisms directly influence serotonergic function and thus impact on mood disorders. TrpH2-deficient mice display alterations in anxiety-like behavior which is accompanied by adaptational changes of 5-HT1A receptors and its associated signaling pathway (Waider et al. 2011). Genetic inactivation of TrpH2 function in mice led to the identification of phenotypic changes, ranging from growth retardation and late-onset obesity to enhanced conditioned fear response, increased aggression, and depression-like behavior (Lesch et al. 2012). In fact TrpH, a BH4-dependent amino acid hydroxylase, is the key regulator of serotonin biosynthesis (Carkaci-Salli et al. 2006). 5-Hydroxy-l-tryptophan is converted to serotonin by AAADC. Actually AAADC deficiency is a severe genetic neuro-metabolic disorder that is characterized with combined deficiency of serotonin, dopamine, and catecholamines (Manegold et al. 2009). Furthermore endothelial AAADC plays an important role in cardiac synthesis of serotonin and possibly in serotonin-dependent regulation of NO generation. 5-Hydroxy-l-tryptophan administration in mice increased phosphorylation of aortic endothelial NOS (eNOS) at Ser-1177 as well as accumulation of nitrates in cardiac tissue (Rouzaud-Laborde et al. 2012). eNOS is known to be stimulated by serotonin via 5-HT1B receptor/eNOS pathway (McDuffie et al. 1999). Phosphorylation of eNOS produces NO without requiring any changes in [Ca2+]i (Boo et al. 2003). Actually 5-HT2B receptor stimulation plays a critical role in the phosphorylation of both extracellular signal-regulated kinase 1/2 (ERK1/2) and eNOS (Asada et al. 2009). In human endothelial cells, serotonin markedly stimulates eNOS expression and the phosphorylation of eNOS, Akt, and ERK1/2. Consequently serotonin induces angiogenesis through activation of Akt in endothelial cells. Selective inhibition of 5-HT2A causes induction of the eNOS/Akt pathway via the endothelial 5-HT1B receptors and enhances vasodilation in diabetes mellitus (Iwabayashi et al. 2012).
Increased activity of the liver enzyme TDO is stimulated by an excess of circulating corticosteroids. In hypercortisolemic conditions, metabolism of Trp turns to the Kyn pathway from serotonin synthesis. Upregulation of the Trp-Kyn pathway and diminished availability of Trp are the primary causes of serotonin deficiency (Oxenkrug 2010). Hypercortisolism affects the gene encoding TrpH2 and the expression of TrpH2. Also chronic corticosterone intake disrupts the diurnal variation of TrpH2 mRNA expression in the brain stem dorsal raphe nucleus and of plasma adrenocorticotropin and corticosterone levels in a dose-dependent manner (Donner et al. 2012). The hippocampus plays a central role in regulation of the HPA axis and release of endogenous glucocorticoids. Exposure to serotonin increases the glucocorticoid receptor mRNA levels in hippocampal neurons. Eventually synthetic and endogenous glucocorticoids, as well as serotonin, influence glucocorticoid receptor expression during hippocampal development (Erdeljan et al. 2005). Stress significantly increases extracellular serotonin release in the basolateral amygdaloid nucleus and the prefrontal cortex (Kawahara et al. 1993). Indeed serotonin dramatically enhances frequency and amplitude of spontaneous inhibitory postsynaptic currents (sIPSCs) in the basolateral amygdala through 5-HT2A receptors. Because of the basolateral amygdaloid GABAergic inhibition is blocked by selective 5-HT2A receptor antagonists, the stress-induced effect appeared to be specific to 5-HT2A receptor downregulation (Jiang et al. 2009).
Monoaminergic neurotransmission involves functional interactions between serotonin, norepinephrine, and dopamine systems. First of all serotonin system exerts negative effect on norepinephrine system through 5-HT2A and on dopamine system through 5-HT2C receptor-mediated mechanisms. Positive and negative effect of norepinephrine system on serotonin neurotransmission is mediated through alpha1- and alpha2-adrenergic receptors, respectively (Hamon and Blier 2013). Actually BH4 is an essential cofactor in the synthesis of serotonin, dopamine, epinephrine, norepinephrine, and NO. BH4 availability influences many cells, including neurons. Following peripheral nerve damage, BH4 dramatically increases in sensory neurons and causes pain hypersensitivity (Latremoliere and Costigan 2011). Fatigue and impaired executive functions are commonly linked to disturbed cerebral dopaminergic and noradrenergic neurotransmission. Moreover selective serotonin reuptake inhibitors (SSRIs) contribute to fatigue, which is a common residual symptom associated with depression (Stenman and Lilja 2013). During the prolonged exercise, fatigue is attributed to the muscle glycogen depletion. “Central fatigue hypothesis” previously was based on the increase in the concentration of brain serotonin during exercise. However according to the revised central fatigue hypothesis, an increase in central ratio of serotonin to dopamine is associated with feelings of tiredness and lethargy (Meeusen and Piacentini 2003). Actually a complex interplay between the different neurotransmitter systems induces fatigue: dopamine and noradrenaline rather than serotonin alone (Roelands and Meeusen 2010).
Diet restriction-induced exaggerated feedback control over serotonin synthesis and the reduced availability of Trp decrease serotonin neurotransmission at postsynaptic sites. A compensatory upregulation of postsynaptic 5-HT1A receptors and hypophagic serotonin receptors may be involved in suppression of appetite (Haleem 2012). In this case although the levels of Trp in the plasma and of serotonin in the hypothalamus decrease, no effect is found on the levels of Trp in the hypothalamus. Diet restriction-induced decrease of serotonin is due to an increase in the responsiveness of negative feedback control over serotonin, not due to smaller availability of Trp (Haleem 2009). Likewise 20–25 % reduction in body weight due to food restriction decreases serotonin concentration in the brain of male but not female rats (Haider and Haleem 2000). Conversely in sugar-diet-treated rats, when the cumulative food intakes increase, body weights decrease. Hyperphagic effects of selective 5-HT1A agonist are greater in normal diet than sugar-diet-treated rats. However serotonin and 5-hydroxyindole acetic acid levels are not changed. Desensitization of pre- as well as postsynaptic 5-HT1A receptors in rats treated with sugar diet causes the precipitation of obesity (Jabeen and Haleem 2008). Actually long-term consumption of sugar diet results in a decrease in the effectiveness of pre- as well as postsynaptic 5-HT1A receptor-dependent responses (Inam et al. 2006). Malnourished offspring have a significant elevation of l-Trp, TrpH activity, and serotonin in the brain stem. Both isoforms of TrpH (TrpH1 and TrpH2) are expressed at birth in both groups; however, TrpH1 expression is significantly higher in offspring with intrauterine malnutrition when compared to the controls. Malnourished offspring show reduced expression of TrpH2 compared to controls. Thus it has been confirmed that intrauterine malnutrition produces an increase in serotonin in the brain stem and also shows increased expression of TrpH1 at birth, with decreased expression of TrpH2 (Manjarrez-Gutiérrez et al. 2012).
The dorsal raphe nucleus (DRN) is the largest serotonin-containing nucleus in the brain and has extensive ascending projections that innervate most forebrain structures. Targets of DRN innervation receive input from both serotonergic and nonserotonergic cells. Selective serotonergic neurotoxins, including 5,7-dihydroxytryptamine (5,7-DHT), have been shown to disrupt axonal transport in serotonergic neurons (Callahan et al. 2001; Araneda et al. 1980). Human LIM homeobox transcription factor 1-beta (Lmx1b)-encoded gene is essential for the development of central serotonergic neurons. This gene is required for the normal biosynthesis of serotonin in the adult brain and for regulating normal functions of central serotonergic neurons. Lmx1b deletion in the adult brain leads to reduction in central serotonin levels. However the overall number of serotonergic neurons is not affected by deleting Lmx1b, and Pet1 promoter expression in the adult brain is independent of Lmx1b. Reduction in central serotonin levels seems to be the consequence of TrpH2 downregulation (Song et al. 2011). In fact Pet1 in the brain is necessary for terminal differentiation of serotonergic neuron phenotype during embryonic development (Hendricks et al. 2003). Considering the serotonergic signaling mechanisms, ETS domain transcription factor Pet1 is also required for maintaining the serotonergic neurotransmitter system during adult stages as well as for expression of the presynaptic 5-HT1B autoreceptor. Therefore adult central nervous system expression of TrpH2 and serotonin transporter (SERT) is restricted to Pet1-expressing serotonin neurons and is rate limiting for the essential serotonergic functions of serotonin synthesis and reuptake (Liu et al. 2010). Pet1 RNA co-localizes with TrpH-positive neurons in raphe nuclei. Loss of Pet1 in the serotonergic neurons leads to a decrease of TrpH2 expression but no change in Lmx1b expression (Song et al. 2011). Virtually serotonergic and nonserotonergic axons innervate distinct but partially overlapping fields within vestibular nuclei (Halberstadt and Balaban 2007). Both local GABAergic and glutamatergic cells project onto DRN serotonergic neurons (Jolas and Aghajanian 1997). 5-HT1A receptors are present on nonserotonergic as well as serotonergic DRN neurons. While the majority of serotonin-immuno-positive cells are double-labeled for 5-HT1A receptor, small but significant population of serotonin-immuno-negative cells express the 5-HT1A receptor (Kirby et al. 2003). Both 5-HT1A and alpha1b adrenergic mRNA are highly expressed throughout the DRN, and the vast majority of serotonergic neurons express both receptors. A smaller percentage of GABAergic neurons also express 5-HT1A or alpha1b adrenergic mRNA. A small amount of catecholaminergic cells express either 5-HT1A or alpha1b adrenergic mRNA (Day et al. 2004).
Hence, serotonin not only affects neuronal excitability through activating postsynaptic receptors (Guo and Rainnie 2010) but also affects presynaptic excitatory or inhibitory neurotransmission in the central nervous system, because of the serotonin activating 5-HT1A and/or 5-HT1B receptors located on the presynaptic terminals. Serotonin exerts significant control over the synaptic inputs and the autonomous activity of subcortical pallidal neurons (Bouryi and Lewis 2003; Hashimoto and Kita 2008). The serotonin receptors have been divided into 7 subfamilies, 6 of which include 13 different genes for G-protein-coupled receptors (GPCR). Post-genomic modifications create 20 more G-protein-coupled serotonin receptors. Consequently there are at least 30 distinct serotonin receptors that signal through G proteins (Raymond et al. 2001). 5-HT1A and 5-HT1B receptors interface primarily with inhibitory G proteins (Gi) to decrease adenylyl cyclase activity. Subsequently the action of the SSRI is mediated through the 5-HT1A receptor (Blier and Ward 2003; Monaca et al. 2003). While SSRI inhibiting the SERT density and function, it maintains the normal firing rates and release of serotonin and immediately increases activation of postsynaptic serotonin receptors (Nemeroff and Owens 2003). All of the seven specific serotonin receptors mediate SSRI effects; however, the second-class receptors, 5-HT6 and 5-HT7, primarily interact with stimulatory G proteins (Gs) to increase adenylyl cyclase activity. In particular the 5-HT6 receptor is involved in neuronal serotonergic transmission and may have effects on anxiety and mood (Yoshioka et al. 1998). The 5-HT7 receptor is involved in hippocampal function (Gill et al. 2002), and has been implicated in the regulation of the glucocorticoid receptors (Laplante et al. 2002). SSRIs also affect the function of the 5-HT2C receptor (Bristow et al. 2000) with some adverse effects potentially mediated by 5-HT2C. Other than for the 5-HT3 receptor, most of the downstream effects of serotonin are mediated by G proteins (Raymond et al. 2001). Actually G proteins are a family of guanine nucleotide-binding regulatory components that couple neurotransmitter receptors to various types of intracellular effector systems. Gs/Gi mediates stimulation/inhibition of adenylate cyclase system, which forms cyclic adenosine monophosphate (cyclic AMP) as a second messenger (Lesch and Lerer 1991). There are 16 genes for G-protein alpha subunits, 5 for beta, and 12 for gamma (Downes and Gautam 1999). SSRIs have been associated with increased transcription of adenylyl cyclase 1. 5-HT1A receptor mediates inhibition of basal and Gs-induced cAMP formation in the absence of adenylyl cyclase 2. 5-HT1A activation decreases activity of neuronal adenylyl cyclase 2 (Albert et al. 1999). Among serotonin receptors, the 5-HT3 receptor is a member of the Cys-loop family of ligand-gated ion channels and located in both the peripheral and central nervous systems. Chronic activation of 5-HT3 receptor produces significant desensitization of 5-HT3 and postsynaptic 5-HT1A receptors without major changes in the expression of SERT and TrpH-2 genes (Kondaurova et al. 2012).
Human SERT reuptakes biogenic amine neurotransmitters following release in the nervous systems and terminates the action of serotonin (Murphy et al. 2004).
SERTs are tightly controlled by multiple signaling pathways, including G-protein-coupled receptor-linked pathways (Blakely et al. 2005). Two protein kinase G (PKG)-dependent pathways have been proposed to support rapid SERT regulation by A3 adenosine receptors (ARs). The first enhances SERT surface trafficking to clear serotonin following vesicular release, and the second is a separate, p38 MAPK-dependent process which augments SERT intrinsic activity (Zhu et al. 2004). p38 MAPK activation downstream of PKG via SERT catalytic regulatory pathway in a trafficking-independent mode is distinct from events controlling SERT surface density. Protein phosphatase 2A is a critical component of the pathway responsible for p38 MAPK upregulation of SERT catalytic activity (Zhu et al. 2005). Thus A3 ARs activation stimulates serotonin uptake via PKG- and p38 MAPK-linked pathway (Zhu et al. 2004). MAP kinase kinase (MAPKK) superfamily molecules, MKK3, MKK3b, and MAPKK6, can act as a specific activator for p38. Furthermore as a major activator for p38, the MAPKK6/p38 kinase cascade is activated strongly by TNF-alpha and H2O2 (Moriguchi et al. 1996). Eventually PKG-linked and p38 MAPK-linked pathways provide a rapid increase in SERT surface expression and function. In contrast, the activity of protein phosphatase 2A inhibitors attenuates MAPK or other signal transduction pathways and facilitates the stimulation of serotonin transport (Zhu et al. 2005), whereas activated protein kinase C (PKC) interacts with SERT and alters the subcellular localization of the transporter resulting in a reduction of serotonin transport. SERT proteins are rapidly phosphorylated in parallel with transporter redistribution and loss of functional uptake capacity. Indeed loss of surface SERT protein after PKC activation reflects transporter redistribution rather than irreversible loss of transporter protein via degradation (Haase et al. 2001; Blakely et al. 1998). In brief, one of the well-known mechanisms in the termination of the stimulation of monoamine neurotransmitters is the removal from the synapse by transporter molecules. Transporters are located within the plasma membrane of presynaptic cells and may be readily regulated by a variety of receptor-mediated intracellular signals.
SERT can be rapidly regulated by a membrane-bound G-protein-coupled receptor and this occurs via NO and cyclic guanosine monophosphate (cGMP). A3 AR is coupled to NO and cGMP (Miller and Hoffman 1994). ARs, A1, A2A, A2B, and A3, are widely distributed throughout the brain and periphery (Fredholm et al. 2001) and have been implicated in a variety of physiological and pathological conditions, including modulation of neural signaling (Okada et al. 1999). It was shown that IL-1 receptors couple via the p38 MAPK pathway to activate SERT. Regulation of SERT is achieved by the multiple AR subtypes in the brain (Fredholm et al. 2005). In particular, A3 AR activation stimulates SERT function in the brain. Inhibition A3 ARs may be able to selectively diminish elevations in SERT activity in a region-dependent manner without affecting basal serotonin clearance or steady-state serotonin levels (Zhu et al. 2007). Consequently A3 AR activation leads to the induction of the serotonin transport by a p38 MAPK-dependent pathway. Stimulation of SERT by A3 AR activation in the brain suggests a functional relationship between A3 AR activation, SERT activity, and serotonin signaling (Zhu et al. 2007). SERT does not have a significant contribution to serotonin uptake in vascular smooth muscle cells of human brain and peripheral vessels. The lack of SERT activity in these vascular smooth muscle cells suggests that different mechanisms may be responsible for serotonin uptake in different vascular beds. In this regard more likely candidates responsible for non-SERT-dependent serotonin uptake are organic cation transporters (OCTs). The polyspecific organic cation transporters OCT1, OCT2, and OCT3 mediate bidirectional diffusion of small organic cations such as acetylcholine and monoamine neurotransmitters (Lee et al. 2009). The mRNA of OCT3 is also called “extraneuronal monoamine transporter” and is expressed in vascular smooth muscle cells of the human brain but not OCT1 and OCT2. In addition to OCT3, most probably the mRNA of plasma membrane monoamine transporter is expressed and contributes to serotonin uptake in these cells (Li et al. 2013).
1.7 Desensitization and Re-sensitization of Serotonin Receptors
Desensitization and re-sensitization of GPCRs can modulate receptor responsiveness in regulation of many cellular functions. These processes depend on the availability of functional receptors at the cell surface and on their mode of activation. Chronic stimulation of receptor agonists causes GPCR desensitization. Actually receptor desensitization can occur by a series of events such as downregulation of the receptor, internalization of the receptor, or uncoupling of the receptor from its signaling proteins (Sibley et al. 1987; Damjanoska et al. 2004). Desensitization process is well described for serotonin receptors. The 5-HT1A is expressed both as a pre- and postsynaptic receptor in neurons. The presynaptic receptor is preferentially desensitized compared to postsynaptic receptors. Desensitization is dependent on internal Ca2+ ions and PKC-dependent agonist-induced uncoupling of the 5-HT1A receptors (Wu et al. 2013). In a similar manner chronic treatment with 5-HT2A/2C receptor agonists disrupts the receptor-to-G-protein interaction. Possible mechanism underlying this desensitization process may be phosphorylation of the 5-HT2A receptor and/or G alpha q/11 proteins. The desensitization of 5-HT2A receptors is most likely due to posttranslational modifications of the 5-HT2A receptor and G alpha q/11 proteins altering the 5-HT2A receptor-to-G alpha q/11 protein interface (Damjanoska et al. 2004). Activation of 5-HT2A receptors stimulates activation of G alpha q/11, which in turn activates effector enzyme phospholipase C (PLC). Desensitization of 5-HT2A receptor-stimulated PLC activity is dependent on activation of the JAK–STAT pathway and is associated with increases in RGS7 protein levels. This increase in RGS7 protein plays a role in the desensitization of 5-HT2A receptor signaling by terminating the activated G alpha q/11 proteins (Singh et al. 2009). Recycled internalized receptors return to the cell surface and recover their ability to couple with G proteins that involve in the re-sensitization process (Bhattacharyya et al. 2002). On the other hand in the absence of serotonin, PKC-activated receptors also recycle to the cell surface. Even in the presence of 5-HT, blocking the activation of PKC prevents the receptor internalization. Therefore PKC activation is necessary for the internalization of serotonin receptors. In order to internalize the receptor, PKC-mediated phosphorylation occurs in the absence of serotonin or G-protein activation (Bhattacharyya et al. 2002). Eventually 5-HT2A receptors become available again at the cell surface after both serotonin- and PKC-mediated processes.
1.8 Enterochromaffin Cell and Serotonergic Signaling
Actually one of the predominant sites of serotonin synthesis, storage, and release is the enterochromaffin (EC) cells of the intestinal mucosa. Serotonin released from EC cells activates neural reflexes associated with intestinal secretion, motility, and sensation. In this respect 5-HT3 and 5-HT4 are the two important receptors for serotonin signaling in pathologic conditions (Costedio et al. 2007). Hence serotonin is not taken up by mucosal nerve fibers (Gershon and Sherman 1982). EC cells activate both intrinsic and extrinsic primary afferent neurons through their release of serotonin. Upon stimulation of 5-HT1P receptors by serotonin, submucosal intrinsic primary afferent neurons trigger peristaltic and secretory reflexes. Serotonin also enhances the release of transmitters through 5-HT4 receptors in prokinetic reflex pathways. However in inflammatory conditions, serotonergic signaling is specifically diminished within the mucosa due to decrease of transcripts encoding tryptophan hydroxylase-1 and 5-HT reuptake transporter. Stimulation of serotonin secretion and desensitization of its receptor can account for the symptoms seen in diarrhea-predominant and constipation-predominant irritable bowel syndrome, respectively (Gershon 2004).
Th17 cells, a novel subtype of proinflammatory T-helper cell, seem to have an important role in the development of inflammatory bowel diseases (Brand 2009). Increase in the plasma IL-17 and mRNA levels of the Th17-specific transcription factor, retinoic acid-related orphan receptor gammat (RORgammat), is an evident finding in patients with active ulcerative colitis. The levels of p-STAT3 and p-STAT5 in peripheral blood mononuclear cells, as well as the ratio of p-STAT3/p-STAT5, are also elevated in these patients. Rising circulating Th17 and the aberrant activation of the STAT pathway may be effective in the progression of inflammatory bowel diseases (Dong et al. 2013). Despite the importance of STAT3 signaling, it should be emphasized that this stimulus alone is not sufficient to drive Th17 differentiation. STAT3 is necessary but not sufficient for IL-17 expression (Chen et al. 2007). Thus IL-27 inhibits the development of proinflammatory Th17 cells by suppressing in a STAT1-dependent manner the expression of the Th17-specific transcription factor of RORgammat (Diveu et al. 2009). Stimulation of intestinal epithelial cells with IL-27 results in the activation of the MAPK signaling pathways p38 and ERK as well as of the phosphoinositol-3-kinase (PI3K)-Akt pathway. IL-27 also activates the transcription factors STAT1, STAT3, and STAT6. IL-27-mediated IDO1 enzymatic activity is also strongly dependent on STAT1 as determined by the IL-27-induced Kyn levels. While silencing of STAT3 has a weak positive effect on IDO1 mRNA and protein expression, silencing of STAT6 does not influence IL-27-activated IDO expression and enzymatic activity (Diegelmann et al. 2012). STAT1 DNA-binding site in the IDO promoter is identical to a described STAT1-binding site following IFN-gamma stimulation (Chon et al. 1995). The response of the IDO gene promoter region to IFN-gamma is dependent on two regulator elements IFN-gamma-activated site and the IFN-stimulated response element. The location of the IFN-gamma-activated site-related sequence is important in relation to the IFN-stimulated response element sequence for a response to IFN-gamma. A cooperative role of IFN-gamma-IRF1 and STAT1 is described in the induction of the IDO1 gene by IFN-gamma (Chon et al. 1996).
EC cells are the sensory transduction elements in the gastrointestinal mucosa and respond to chemical and mechanical stimuli by releasing serotonin. The uptake of serotonin by SERT-dependent mechanisms is a key factor in controlling serotonin availability in the gastrointestinal tract. EC cell numbers increase in the ileum of these rats (Bertrand et al. 2011). In obesity a significant decrease in the total number of EC cells per crypt and a reduction in the levels of serotonin occur in western type of diet-fed rats compared with in chow-fed rats. SERT protein levels and SERT-dependent uptake of serotonin are constant. Although there is no change in tryptophan hydroxylase 1 mRNA, SERT mRNA increases. Reduction of serotonin availability is associated with decreased intestinal motility in vivo (Bertrand et al. 2012). The enteric SERT is the only transporter expressed in the bowel with a high affinity for serotonin. In SERT deficient bowel expresses dopamine transporter (DAT) and OCT3 that transport serotonin, although they lack the selectivity and affinity of SERT for 5-HT. DAT and the OCTs might thus compensate, at least partially, for the absence of SERT. Although there is an excessive increase in colonic motility and watery diarrhea in the majority of SERT-deficient subjects, a striking decrease in colonic motility and constipation may be evident in a minority of these animals (Chen et al. 2001). No difference in OCT1 expression is detected between SERT deficient and control animals. Upregulation of OCT3 expression and enhanced low-affinity serotonin uptake may limit the adverse effects of elevated extracellular serotonin in the absence of SERT (Schmitt et al. 2003). Consequently OCT3 contributes to serotonin clearance if the expression of the SERT is low or absent.
As mentioned already, OCTs and the plasma membrane monoamine transporters are capable of clearing biogenic amines from extracellular fluid and may serve to buffer the effects of selective serotonin reuptake inhibitors (Daws 2009). Proliferation of intestinal mucosal cells is significantly greater in mice with lack of the serotonin reuptake transporter and in mice given selective serotonin reuptake inhibitors. On the other hand serotonin promotes growth and turnover of the intestinal mucosal epithelium. These processes are mediated by neuronal rather than mucosal serotonin (Gross et al. 2012). Likewise, constitutive gastrointestinal motility depends on neuronal rather than on mucosal serotonin, and the development of dopaminergic, GABAergic, and calcitonin gene-related peptide (CGRP)-expressing enteric neurons requires neuronal serotonin (Li et al. 2011).
Since EC cells are sensitive to oxygen, alterations in oxygen levels differentially activate hypoxia-inducible factor 1alpha (HIF-1alpha) and TpH1, as well as NF-kappaB signaling. Changes in the amount of serotonin production and secretion determine the oxygen sensing role of EC cells. Decrease in oxygen concentration elevates serotonin secretion by 2–3.2-fold, as well as protein levels of HIF-1alpha by 1.7–3-fold. Whereas rising of the oxygen concentration to 100 % reduces serotonin secretion, inhibits hypoxia transcriptional response element (HRE)-mediated signaling, and significantly lowers HIF-1alpha levels. NF-kappaB signaling is also elevated during hypoxia by 1.2–1.6-fold (Haugen et al. 2012).
1.9 Taste Receptor Signaling
GPCRs are key transmembrane recognition molecules for regulatory signals such as light, odors, taste hormones, and neurotransmitters. In addition to activating G proteins, GPCRs associate with a variety of GPCR-interacting proteins (GIPs) (Bockaert et al. 2010). GIPs influence the targeting, trafficking, and signal transduction properties of serotonin receptors (Marin et al. 2012). Three currently recognized types of taste bud cells exhibit distinct morphological features and cellular functions: nucleoside triphosphate diphosphohydrolases (NTPDase)2 and glial glutamate/aspartate transporter (GLAST) co-localized type I cells (Bartel et al. 2006), the taste-specific G-protein α-gustducin expressed type II cells (Yang et al. 2000a), and serotonin, neuron-specific enolase, ubiquitin carboxyl terminal hydrolase, and neural cell adhesion molecule expressed type III taste cells (Yee et al. 2001). Adenosine triphosphate (ATP) activated presynaptic (type III) cells release serotonin and norepinephrine following ATP secretion from receptor (type II) taste bud cells during taste stimulation. Subsequently, serotonin released from presynaptic (type III) cells provides a negative paracrine feedback onto receptor cells by activating 5-HT1A receptors. Finally, taste-evoked Ca2+ mobilization is inhibited from receptor cells (Huang et al. 2009). Salts and acids utilize apically located ion channels for transduction, while bitter, sweet, and umami (l-glutamate and 5′-ribonucleotides) stimuli utilize GPCRs and second messenger signaling pathways (Kinnamon 2012). Two classes of taste GPCRs have been identified: the first group type 1 taste receptors (T1Rs) for sweet and umami (l-glutamate and 5′-ribonucleotides) stimuli and the second group T2Rs for bitter stimuli (Bachmanov and Beauchamp 2007). Transient receptor potential cation channel subfamily M member 5 (melastatin 5 or TRPM5) depolarizes taste cells. TRPM5 leads to the release of ATP, which activates ionotropic purinergic receptors on gustatory afferent nerve fibers (Finger et al. 2005).
Cells expressing alpha-gustducin and phospholipase C isoform beta2 (PLC-beta 2) localize at multiple cardiorespiratory and CO2/H+ chemosensory sites. Especially in the medullary raphe, alpha-gustducin and PLC-beta2 are co-localized with TrpH-immunoreactive serotonergic neurons. It has been shown that different bitter-responsive T2Rs associate with G-protein alpha-gustducin, PLC-beta2, and TRPM5 in the brain stem of rats (Dehkordi et al. 2012). Mammalian taste cells normally contain serotonin, and taste cells can take up 5-hydroxytryptophan and convert it to serotonin. Subsequently serotonin functions as a neuromodulator or neurotransmitter in vertebrate taste buds. Diffuse, cytoplasmic syntaxin-1-like immunoreactivity is present in type III cells, and taste cell synapses use syntaxin-1 for neurotransmitter release (Kim and Roper 1995; Yang et al. 2000b; Yang et al. 2007). Serotonin-like immunoreactivity cells resemble syntaxin-1-like immunoreactivity cells in both shape and structure and have been shown to co-localize with a subset of syntaxin-1-like immunoreactive type III cells. Synapses are only observed from type III taste cells onto ionotropic ligand-gated ion channel receptors (P2X2)-like immunoreactivity nerve processes (Yang et al. 2012).
Synapses between gustatory receptor cells and primary sensory afferent fibers transmit the output signal from taste buds to the central nervous system. Actually several transmitter candidates have been proposed for these synapses, including serotonin, glutamate, acetylcholine, ATP, and peptides. Serotonin is one of the important neurotransmitters released by taste cells in response to gustatory stimulation (Huang et al. 2005). However, only serotonin and ATP are secreted by separate classes of taste cells. While presynaptic (type III) taste cells release serotonin upon stimulation (Huang et al. 2007), receptor (type II) taste bud cells secrete ATP during taste stimulation. In turn, ATP activates adjacent presynaptic (type III) cells to release serotonin and norepinephrine. Serotonin released from presynaptic (type III) cells provides negative paracrine feedback onto receptor cells by activating 5-HT(1A) receptors, inhibiting taste-evoked Ca2+ mobilization in receptor cells, and reducing ATP secretion (Huang et al. 2009). Majority of or all presynaptic (type III) taste cells secrete serotonin upon stimulation, but approximately one-third of them co-release norepinephrine with serotonin. In other words there are three to five times as many serotonergic presynaptic cells as there are norepinephrine/serotonin-secreting cells (Huang et al. 2008).
1.10 Conclusion
The Kyn pathway is the principle route of l-Trp metabolism and involves several mechanisms which trigger various metabolic pathways and transcription factors. Kyn produces neurotoxic and neuroprotective metabolic precursors before complete oxidation to NAD+. Particularly QA-induced excitation and neurotoxicity are mediated by the overactivation of NMDA receptors, whereas KA is an antagonist of NMDA and alpha7nACh receptors and, thus, a potential neuroprotectant. While Kyn to Trp ratio reflects IDO activity, the Kyn to KA ratio indicates the neurotoxic challenge. Through the catabolic cascade of Trp metabolism, monoaminergic neurotransmission involves functional interactions between serotonin, norepinephrine, and dopamine systems. Serotonin not only affects neuronal excitability through activating postsynaptic receptors but also affects presynaptic excitatory or inhibitory neurotransmission in the central nervous system. However human SERT reuptakes biogenic amine neurotransmitters following release in the nervous systems and terminates the action of serotonin. OCT contributes to serotonin clearance if the expression of the SERT is low or absent. OCTs and the plasma membrane monoamine transporters are capable of clearing biogenic amines from extracellular fluid and may serve to buffer the effects of SSRIs. Desensitization and re-sensitization depend on the availability of functional receptors at the cell surface and on their mode of activation. Reviewing the dynamic aspects of Trp signaling intermediates helps to explain the mutual interaction of Kyn, serotonin, and melatonin pathways and opens up new vistas regarding the mechanism of diseases.
References
Albert PR, Sajedi N, Lemonde S, Ghahremani MH (1999) Constitutive G(i2)-dependent activation of adenylyl cyclase type II by the 5-HT1A receptor. Inhibition by anxiolytic partial agonists. J Biol Chem 274:35469–35474
Amori L, Wu HQ, Marinozzi M, Pellicciari R, Guidetti P, Schwarcz R (2009) Specific inhibition of kynurenate synthesis enhances extracellular dopamine levels in the rodent striatum. Neuroscience 159:196–203
Araneda S, Bobillier P, Buda M, Pujol JF (1980) Retrograde axonal transport following injection of [3H]serotonin in the olfactory bulb. I. Biochemical study. Brain Res 196:405–415
Asada M, Ebihara S, Yamanda S, Niu K, Okazaki T, Sora I, Arai H (2009) Depletion of serotonin and selective inhibition of 2B receptor suppressed tumor angiogenesis by inhibiting endothelial nitric oxide synthase and extracellular signal-regulated kinase 1/2 phosphorylation. Neoplasia 11:408–417
Bachmanov AA, Beauchamp GK (2007) Taste receptor genes. Annu Rev Nutr 27:389–414
Ball HJ, Yuasa HJ, Austin CJ, Weiser S, Hunt NH (2009) Indoleamine 2,3-dioxygenase-2; a new enzyme in the kynurenine pathway. Int J Biochem Cell Biol 41:467–471
Bartel DL, Sullivan SL, Lavoie EG, Sévigny J, Finger TE (2006) Nucleoside triphosphate diphosphohydrolase-2 is the ecto-ATPase of type I cells in taste buds. J Comp Neurol 497:1–12
Bertrand RL, Senadheera S, Markus I, Liu L, Howitt L, Chen H, Murphy TV, Sandow SL, Bertrand PP (2011) A Western diet increases serotonin availability in rat small intestine. Endocrinology 152:36–47
Bertrand RL, Senadheera S, Tanoto A, Tan KL, Howitt L, Chen H, Murphy TV, Sandow SL, Liu L, Bertrand PP (2012) Serotonin availability in rat colon is reduced during a Western diet model of obesity. Am J Physiol Gastrointest Liver Physiol 303:G424–G434
Bhattacharyya S, Puri S, Miledi R, Panicker MM (2002) Internalization and recycling of 5-HT2A receptors activated by serotonin and protein kinase C-mediated mechanisms. Proc Natl Acad Sci U S A 99:14470–14475
Blakely RD, Ramamoorthy S, Schroeter S, Qian Y, Apparsundaram S, Galli A, DeFelice LJ (1998) Regulated phosphorylation and trafficking of antidepressant-sensitive serotonin transporter proteins. Biol Psychiatry 44:169–178
Blakely RD, Defelice LJ, Galli A (2005) Biogenic amine neurotransmitter transporters: just when you thought you knew them. Physiology (Bethesda) 20:225–231
Blier P, Ward NM (2003) Is there a role for 5-HT1A agonists in the treatment of depression? Biol Psychiatry 53(3):193–203
Bockaert J, Perroy J, Bécamel C, Marin P, Fagni L (2010) GPCR interacting proteins (GIPs) in the nervous system: roles in physiology and pathologies. Annu Rev Pharmacol Toxicol 50:89–109
Boo YC, Sorescu GP, Bauer PM, Fulton D, Kemp BE, Harrison DG, Sessa WC, Jo H (2003) Endothelial NO synthase phosphorylated at SER635 produces NO without requiring intracellular calcium increase. Free Radic Biol Med 35:729–741
Borland LM, Michael AC (2004) Voltammetric study of the control of striatal dopamine release by glutamate. J Neurochem 91:220–229
Bouryi VA, Lewis DI (2003) The modulation by 5-HT of glutamatergic inputs from the raphe pallidus to rat hypoglossal motoneurons, in vitro. J Physiol 553:1019–1031
Brand S (2009) Crohn’s disease: Th1, Th17 or both? The change of a paradigm: new immunological and genetic insights implicate Th17 cells in the pathogenesis of Crohn’s disease. Gut 58:1152–1167
Brandacher G, Winkler C, Aigner F, Schwelberger H, Schroecksnadel K, Margreiter R, Fuchs D, Weiss HG (2006) Bariatric surgery cannot prevent tryptophan depletion due to chronic immune activation in morbidly obese patients. Obes Surg 16:541–548
Brandacher G, Hoeller E, Fuchs D, Weiss HG (2007) Chronic immune activation underlies morbid obesity: is IDO a key player? Curr Drug Metab 8:289–295
Bristow LJ, O’Connor D, Watts R, Duxon MS, Hutson PH (2000) Evidence for accelerated desensitisation of 5-HT(2C) receptors following combined treatment with fluoxetine and the 5-HT(1A) receptor antagonist, WAY 100,635, in the rat. Neuropharmacology 39:1222–1236
Callahan BT, Cord BJ, Ricaurte GA (2001) Long-term impairment of anterograde axonal transport along fiber projections originating in the rostral raphe nuclei after treatment with fenfluramine or methylenedioxymethamphetamine. Synapse 40:113–121
Capuron L, Miller AH (2011) Immune system to brain signaling: neuropsychopharmacological implications. Pharmacol Ther 130:226–238
Carkaci-Salli N, Flanagan JM, Martz MK, Salli U, Walther DJ, Bader M, Vrana KE (2006) Functional domains of human tryptophan hydroxylase 2 (hTPH2). J Biol Chem 281:28105–28112
Ceresoli-Borroni G, Guidetti P, Amori L, Pellicciari R, Schwarcz R (2007) Perinatal kynurenine 3-hydroxylase inhibition in rodents: pathophysiological implications. J Neurosci Res 85:845–854
Chen GL, Miller GM (2012) Advances in tryptophan hydroxylase-2 gene expression regulation: new insights into serotonin-stress interaction and clinical implications. Am J Med Genet B Neuropsychiatr Genet 159B:152–171
Chen JJ, Li Z, Pan H, Murphy DL, Tamir H, Koepsell H, Gershon MD (2001) Maintenance of serotonin in the intestinal mucosa and ganglia of mice that lack the high-affinity serotonin transporter: abnormal intestinal motility and the expression of cation transporters. J Neurosci 21:6348–6361
Chen Z, Laurence A, O’Shea JJ (2007) Signal transduction pathways and transcriptional regulation in the control of Th17 differentiation. Semin Immunol 19:400–408
Chon SY, Hassanain HH, Pine R, Gupta SL (1995) Involvement of two regulatory elements in interferon-gamma-regulated expression of human indoleamine 2,3-dioxygenase gene. J Interferon Cytokine Res 15:517–526
Chon SY, Hassanain HH, Gupta SL (1996) Cooperative role of interferon regulatory factor 1 and p91 (STAT1) response elements in interferon-gamma-inducible expression of human indoleamine 2,3-dioxygenase gene. J Biol Chem 271:17247–17252
Costedio MM, Hyman N, Mawe GM (2007) Serotonin and its role in colonic function and in gastrointestinal disorders. Dis Colon Rectum 50:376–388
Damjanoska KJ, Heidenreich BA, Kindel GH, D’Souza DN, Zhang Y, Garcia F, Battaglia G, Wolf WA, Van de Kar LD, Muma NA (2004) Agonist-induced serotonin 2A receptor desensitization in the rat frontal cortex and hypothalamus. J Pharmacol Exp Ther 309:1043–1050
Daws LC (2009) Unfaithful neurotransmitter transporters: focus on serotonin uptake and implications for antidepressant efficacy. Pharmacol Ther 121:89–99
Day HE, Greenwood BN, Hammack SE, Watkins LR, Fleshner M, Maier SF, Campeau S (2004) Differential expression of 5HT-1A, alpha 1b adrenergic, CRF-R1, and CRF-R2 receptor mRNA in serotonergic, gamma-aminobutyric acidergic, and catecholaminergic cells of the rat dorsal raphe nucleus. J Comp Neurol 474:364–378
De Carvalho LP, Bochet P, Rossier J (1996) The endogenous agonist quinolinic acid and the nonendogenous homoquinolinic acid discriminate between NMDAR2 receptor subunits. Neurochem Int 28:445–452
Dehkordi O, Rose JE, Fatemi M, Allard JS, Balan KV, Young JK, Fatima S, Millis RM, Jayam-Trouth A (2012) Neuronal expression of bitter taste receptors and downstream signaling molecules in the rat brainstem. Brain Res 1475:1–10
Denison MS, Nagy SR (2003) Activation of the aryl hydrocarbon receptor by structurally diverse exogenous and endogenous chemicals. Annu Rev Pharmacol Toxicol 43:309–334
Diani-Moore S, Ram P, Li X, Mondal P, Youn DY, Sauve AA, Rifkind AB (2010) Identification of the aryl hydrocarbon receptor target gene TiPARP as a mediator of suppression of hepatic gluconeogenesis by 2,3,7,8-tetrachlorodibenzo-p-dioxin and of nicotinamide as a corrective agent for this effect. J Biol Chem 285:38801–38810
Diegelmann J, Olszak T, Göke B, Blumberg RS, Brand S (2012) A novel role for interleukin-27 (IL-27) as mediator of intestinal epithelial barrier protection mediated via differential signal transducer and activator of transcription (STAT) protein signaling and induction of antibacterial and anti-inflammatory proteins. J Biol Chem 287:286–298
Diveu C, McGeachy MJ, Boniface K, Stumhofer JS, Sathe M, Joyce-Shaikh B, Chen Y, Tato CM, McClanahan TK, de Waal MR, Hunter CA, Cua DJ, Kastelein RA (2009) IL-27 blocks RORc expression to inhibit lineage commitment of Th17 cells. J Immunol 182:5748–5756
Dong Z, Du L, Xu X, Yang Y, Wang H, Qu A, Qu X, Wang C (2013) Aberrant expression of circulating Th17, Th1 and Tc1 cells in patients with active and inactive ulcerative colitis. Int J Mol Med 31:989–997
Donner NC, Montoya CD, Lukkes JL, Lowry CA (2012) Chronic non-invasive corticosterone administration abolishes the diurnal pattern of tph2 expression. Psychoneuroendocrinology 37:645–661
Downes GB, Gautam N (1999) The G protein subunit gene families. Genomics 62:544–552
Dunn AJ, Wang J, Ando T (1999) Effects of cytokines on cerebral neurotransmission. Comparison with the effects of stress. Adv Exp Med Biol 461:117–127
Erdeljan P, Andrews MH, MacDonald JF, Matthews SG (2005) Glucocorticoids and serotonin alter glucocorticoid receptor mRNA levels in fetal guinea-pig hippocampal neurons, in vitro. Reprod Fertil Dev 17:743–749
Erhardt S, Olsson SK, Engberg G (2009) Pharmacological manipulation of kynurenic acid. CNS Drugs 23:91–101
Fallarino F, Grohmann U, Vacca C, Bianchi R, Orabona C, Spreca A, Fioretti MC, Puccetti P (2002) T cell apoptosis by tryptophan catabolism. Cell Death Differ 9:1069–1077
Fernstrom JD (2012) Effects and side effects associated with the non-nutritional use of tryptophan by humans. J Nutr 142:2236S–2244S
Finger TE, Danilova V, Barrows J, Bartel DL, Vigers AJ, Stone L, Hellekant G, Kinnamon SC (2005) ATP signaling is crucial for communication from taste buds to gustatory nerves. Science 310:1495–1499
Foster AC, Vezzani A, French ED, Schwarcz R (1984) Kynurenic acid blocks neurotoxicity and seizures induced in rats by the related brain metabolite quinolinic acid. Neurosci Lett 48:273–278
Fredholm BB, IJzerman AP, Jacobson KA, Klotz KN, Linden J (2001) International Union of Pharmacology. XXV. Nomenclature and classification of adenosine receptors. Pharmacol Rev 53:527–552
Fredholm BB, Chen JF, Masino SA, Vaugeois JM (2005) Actions of adenosine at its receptors in the CNS: insights from knockouts and drugs. Annu Rev Pharmacol Toxicol 45:385–412
Fujigaki H, Saito K, Fujigaki S, Takemura M, Sudo K, Ishiguro H, Seishima M (2006) The signal transducer and activator of transcription 1alpha and interferon regulatory factor 1 are not essential for the induction of indoleamine 2,3-dioxygenase by lipopolysaccharide: involvement of p38 mitogen-activated protein kinase and nuclear factor-kappaB pathways, and synergistic effect of several proinflammatory cytokines. J Biochem 139:655–662
Fukui S, Schwarcz R, Rapoport SI, Takada Y, Smith QR (1991) Blood-brain barrier transport of kynurenines: implications for brain synthesis and metabolism. J Neurochem 56:2007–2017
Gershon MD (2004) Review article: serotonin receptors and transporters – roles in normal and abnormal gastrointestinal motility. Aliment Pharmacol Ther 20(Suppl 7):3–14
Gershon MD, Sherman DL (1982) Identification of and interactions between noradrenergic and serotonergic neurites in the myenteric plexus. J Comp Neurol 204:407–421
Gill CH, Soffin EM, Hagan JJ, Davies CH (2002) 5-HT7 receptors modulate synchronized network activity in rat hippocampus. Neuropharmacology 42:82–92
Gross ER, Gershon MD, Margolis KG, Gertsberg ZV, Li Z, Cowles RA (2012) Neuronal serotonin regulates growth of the intestinal mucosa in mice. Gastroenterology 143:408–417
Gu Z, Jiang Q, Yan Z (2007) RGS4 modulates serotonin signaling in prefrontal cortex and links to serotonin dysfunction in a rat model of schizophrenia. Mol Pharmacol 71:1030–1039
Guidetti P, Hoffman GE, Melendez-Ferro M, Albuquerque EX, Schwarcz R (2007) Astrocytic localization of kynurenine aminotransferase II in the rat brain visualized by immunocytochemistry. Glia 55:78–92
Guillemin GJ, Kerr SJ, Smythe GA, Smith DG, Kapoor V, Armati PJ, Croitoru J, Brew BJ (2001) Kynurenine pathway metabolism in human astrocytes: a paradox for neuronal protection. J Neurochem 78:842–853
Guo JD, Rainnie DG (2010) Presynaptic 5-HT(1B) receptor-mediated serotonergic inhibition of glutamate transmission in the bed nucleus of the stria terminalis. Neuroscience 165:1390–1401
Haase J, Killian AM, Magnani F, Williams C (2001) Regulation of the serotonin transporter by interacting proteins. Biochem Soc Trans 29:722–728
Haider S, Haleem DJ (2000) Decreases of brain serotonin following a food restriction schedule of 4 weeks in male and female rats. Med Sci Monit 6:1061–1067
Halberstadt AL, Balaban CD (2007) Selective anterograde tracing of the individual serotonergic and nonserotonergic components of the dorsal raphe nucleus projection to the vestibular nuclei. Neuroscience 147:207–223
Haleem DJ (2009) Exaggerated feedback control decreases brain serotonin concentration and elicits hyperactivity in a rat model of diet-restriction-induced anorexia nervosa. Appetite 52:44–50
Haleem DJ (2012) Serotonin neurotransmission in anorexia nervosa. Behav Pharmacol 23:478–495
Hamon M, Blier P (2013) Monoamine neurocircuitry in depression and strategies for new treatments. Prog Neuropsychopharmacol Biol Psychiatry 45:54–63
Hashimoto K, Kita H (2008) Serotonin activates presynaptic and postsynaptic receptors in rat globus pallidus. J Neurophysiol 99:1723–1732
Haugen M, Dammen R, Svejda B, Gustafsson BI, Pfragner R, Modlin I, Kidd M (2012) Differential signal pathway activation and 5-HT function: the role of gut enterochromaffin cells as oxygen sensors. Am J Physiol Gastrointest Liver Physiol 303:G1164–G1173
Hendricks TJ, Fyodorov DV, Wegman LJ, Lelutiu NB, Pehek EA, Yamamoto B, Silver J, Weeber EJ, Sweatt JD, Deneris ES (2003) Pet-1 ETS gene plays a critical role in 5-HT neuron development and is required for normal anxiety-like and aggressive behavior. Neuron 37:233–247
Hilmas C, Pereira EF, Alkondon M, Rassoulpour A, Schwarcz R, Albuquerque EX (2001) The brain metabolite kynurenic acid inhibits alpha7 nicotinic receptor activity and increases non-alpha7 nicotinic receptor expression: physiopathological implications. J Neurosci 21:7463–7473
Huang YJ, Maruyama Y, Lu KS, Pereira E, Plonsky I, Baur JE, Wu D, Roper SD (2005) Mouse taste buds use serotonin as a neurotransmitter. J Neurosci 25:843–847
Huang YJ, Maruyama Y, Dvoryanchikov G, Pereira E, Chaudhari N, Roper SD (2007) The role of pannexin 1 hemichannels in ATP release and cell-cell communication in mouse taste buds. Proc Natl Acad Sci U S A 104:6436–6441
Huang YA, Maruyama Y, Roper SD (2008) Norepinephrine is co-released with serotonin in mouse taste buds. J Neurosci 28:13088–13093
Huang YA, Dando R, Roper SD (2009) Autocrine and paracrine roles for ATP and serotonin in mouse taste buds. J Neurosci 29:13909–13918
Ida T, Hara M, Nakamura Y, Kozaki S, Tsunoda S, Ihara H (2008) Cytokine-induced enhancement of calcium-dependent glutamate release from astrocytes mediated by nitric oxide. Neurosci Lett 432:232–236
Inam QU, Haleem MA, Haleem DJ (2006) Effects of long term consumption of sugar as part of meal on serotonin 1-a receptor dependent responses. Pak J Pharm Sci 19:94–98
Iwabayashi M, Taniyama Y, Sanada F, Azuma J, Iekushi K, Kusunoki H, Chatterjee A, Okayama K, Rakugi H, Morishita R (2012) Role of serotonin in angiogenesis: induction of angiogenesis by sarpogrelate via endothelial 5-HT1B/Akt/eNOS pathway in diabetic mice. Atherosclerosis 220:337–342
Jabeen B, Haleem DJ (2008) Desensitization of pre and post synaptic 5-HT-1A receptor responses following long term consumption of sugar rich diet: implications for sugar-induced obesity. Pak J Pharm Sci 21:327–332
Jara-Prado A, Ortega-Vazquez A, Martinez-Ruano L, Rios C, Santamaria A (2003) Homocysteine-induced brain lipid peroxidation: effects of NMDA receptor blockade, antioxidant treatment, and nitric oxide synthase inhibition. Neurotox Res 5:237–243
Jiang X, Xing G, Yang C, Verma A, Zhang L, Li H (2009) Stress impairs 5-HT2A receptor-mediated serotonergic facilitation of GABA release in juvenile rat basolateral amygdala. Neuropsychopharmacology 34:410–423
Jolas T, Aghajanian GK (1997) Opioids suppress spontaneous and NMDA-induced inhibitory postsynaptic currents in the dorsal raphe nucleus of the rat in vitro. Brain Res 755:229–245
Kaiser S, Wonnacott S (2000) Alpha-bungarotoxin-sensitive nicotinic receptors indirectly modulate [(3)H]dopamine release in rat striatal slices via glutamate release. Mol Pharmacol 58:312–318
Kawahara H, Yoshida M, Yokoo H, Nishi M, Tanaka M (1993) Psychological stress increases serotonin release in the rat amygdala and prefrontal cortex assessed by in vivo microdialysis. Neurosci Lett 162:81–84
Kessler M, Terramani T, Lynch G, Baudry M (1989) A glycine site associated with N-methyl-D-aspartic acid receptors: characterization and identification of a new class of antagonists. J Neurochem 52:1319–1328
Kim DJ, Roper SD (1995) Localization of serotonin in taste buds: a comparative study in four vertebrates. J Comp Neurol 353:364–370
Kinnamon SC (2012) Taste receptor signalling – from tongues to lungs. Acta Physiol (Oxf) 204:158–168
Kirby LG, Pernar L, Valentino RJ, Beck SG (2003) Distinguishing characteristics of serotonin and non-serotonin-containing cells in the dorsal raphe nucleus: electrophysiological and immunohistochemical studies. Neuroscience 116:669–683
Kiss C, Ceresoli-Borroni G, Guidetti P, Zielke CL, Zielke HR, Schwarcz R (2003) Kynurenate production by cultured human astrocytes. J Neural Transm 110:1–14
Kondaurova EM, Naumenko VS, Popova NK (2012) Effect of chronic activation of 5-HT3 receptors on 5-HT3, 5-HT(1A) and 5-HT(2A) receptors functional activity and expression of key genes of the brain serotonin system. Neurosci Lett 522:52–56
Konradsson-Geuken A, Wu HQ, Gash CR, Alexander KS, Campbell A, Sozeri Y, Pellicciari R, Schwarcz R, Bruno JP (2010) Cortical kynurenic acid bi-directionally modulates prefrontal glutamate levels as assessed by microdialysis and rapid electrochemistry. Neuroscience 169:1848–1859
Konsman JP, Parnet P, Dantzer R (2002) Cytokine-induced sickness behaviour: mechanisms and implications. Trends Neurosci 25:154–159
Konturek SJ, Konturek PC, Brzozowska I, Pawlik M, Sliwowski Z, Cześnikiewicz-Guzik M, Kwiecień S, Brzozowski T, Bubenik GA, Pawlik WW (2007) Localization and biological activities of melatonin in intact and diseased gastrointestinal tract. J Physiol Pharmacol 58:381–405
Laplante P, Diorio J, Meaney MJ (2002) Serotonin regulates hippocampal glucocorticoid receptor expression via a 5-HT7 receptor. Brain Res Dev Brain Res 139:199–203
Latremoliere A, Costigan M (2011) GCH1, BH4 and pain. Curr Pharm Biotechnol 12:1728–1741
Lee WK, Wolff NA, Thévenod F (2009) Organic cation transporters: physiology, toxicology and special focus on ethidium as a novel substrate. Curr Drug Metab 10:617–631
Lehnardt S (2010) Innate immunity and neuroinflammation in the CNS: the role of microglia in toll-like receptor-mediated neuronal injury. Glia 58:253–263
Lekieffre D, Plotkine M, Allix M, Boulu RG (1990) Kynurenic acid antagonizes hippocampal quinolinic acid neurotoxicity: behavioral and histological evaluation. Neurosci Lett 120:31–33
Lesch KP, Lerer B (1991) The 5-HT receptor–G-protein–effector system complex in depression. I. Effect of glucocorticoids. J Neural Transm Gen Sect 84:3–18
Lesch KP, Araragi N, Waider J, van den Hove D, Gutknecht L (2012) Targeting brain serotonin synthesis: insights into neurodevelopmental disorders with long-term outcomes related to negative emotionality, aggression and antisocial behaviour. Philos Trans R Soc Lond B Biol Sci 367:2426–2443
Lestage J, Verrier D, Palin K, Dantzer R (2002) The enzyme indoleamine 2,3-dioxygenase is induced in the mouse brain in response to peripheral administration of lipopolysaccharide and superantigen. Brain Behav Immun 16:596–601
Li Z, Chalazonitis A, Huang YY, Mann JJ, Margolis KG, Yang QM, Kim DO, Côté F, Mallet J, Gershon MD (2011) Essential roles of enteric neuronal serotonin in gastrointestinal motility and the development/survival of enteric dopaminergic neurons. J Neurosci 31:8998–9009
Li RW, Yang C, Kwan YW, Chan SW, Lee SM, Leung GP (2013) Involvement of organic cation transporter-3 and plasma membrane monoamine transporter in serotonin uptake in human brain vascular smooth muscle cells. Front Pharmacol 4:14
Liu C, Maejima T, Wyler SC, Casadesus G, Herlitze S, Deneris ES (2010) Pet-1 is required across different stages of life to regulate serotonergic function. Nat Neurosci 13:1190–1198
Lorton D, Lubahn CL, Estus C, Millar BA, Carter JL, Wood CA, Bellinger DL (2006) Bidirectional communication between the brain and the immune system: implications for physiological sleep and disorders with disrupted sleep. Neuroimmunomodulation 13:357–374
Lull ME, Block ML (2010) Microglial activation and chronic neurodegeneration. Neurotherapeutics 7:354–365
Manegold C, Hoffmann GF, Degen I, Ikonomidou H, Knust A, Laass MW, Pritsch M, Wilichowski E, Hörster F (2009) Aromatic L-amino acid decarboxylase deficiency: clinical features, drug therapy and follow-up. J Inherit Metab Dis 32:371–380
Manjarrez-Gutiérrez G, Martínez-Radilla K, de Oca Boyzo-Montes A, Orozco-Suárez S, Hernández-Rodríguez J (2012) Increased expression of tryptophan-5-hydroxylase 1, but not 2, in brainstem as a result of intrauterine malnutrition. Int J Dev Neurosci 30:445–450
Marazziti D, Baroni S, Picchetti M, Piccinni A, Silvestri S, Dell’Osso L (2013) New developments on the serotonin hypothesis of depression: shunt of tryptophan. Riv Psichiatr 48:23–34
Marin P, Becamel C, Dumuis A, Bockaert J (2012) 5-HT receptor-associated protein networks: new targets for drug discovery in psychiatric disorders? Curr Drug Targets 13:28–52
Marshall NB, Kerkvliet NI (2010) Dioxin and immune regulation: emerging role of aryl hydrocarbon receptor in the generation of regulatory T cells. Ann N Y Acad Sci 1183:25–37
McDuffie JE, Coaxum SD, Maleque MA (1999) 5-hydroxytryptamine evokes endothelial nitric oxide synthase activation in bovine aortic endothelial cell cultures. Proc Soc Exp Biol Med 221:386–390
Meeusen R, Piacentini MF (2003) Exercise, fatigue, neurotransmission and the influence of the neuroendocrine axis. Adv Exp Med Biol 527:521–525
Metz R, Duhadaway JB, Kamasani U, Laury-Kleintop L, Muller AJ, Prendergast GC (2007) Novel tryptophan catabolic enzyme IDO2 is the preferred biochemical target of the antitumor indoleamine 2,3-dioxygenase inhibitory compound D-1-methyl-tryptophan. Cancer Res 67:7082–7087
Miller KJ, Hoffman BJ (1994) Adenosine A3 receptors regulate serotonin transport via nitric oxide and cGMP. J Biol Chem 269:27351–27356
Miller AH, Haroon E, Raison CL, Felger JC (2013) Cytokine targets in the brain: impact on neurotransmitters and neurocircuits. Depress Anxiety 30:297–306
Monaca C, Boutrel B, Hen R, Hamon M, Adrien J (2003) 5-HT 1A/1B receptor-mediated effects of the selective serotonin reuptake inhibitor, citalopram, on sleep: studies in 5-HT 1A and 5-HT 1B knockout mice. Neuropsychopharmacology 28:850–856
Moriguchi T, Toyoshima F, Gotoh Y, Iwamatsu A, Irie K, Mori E, Kuroyanagi N, Hagiwara M, Matsumoto K, Nishida E (1996) Purification and identification of a major activator for p38 from osmotically shocked cells. Activation of mitogen-activated protein kinase kinase 6 by osmotic shock, tumor necrosis factor-alpha, and H2O2. J Biol Chem 271:26981–26988
Mukai M, Tischkau SA (2007) Effects of tryptophan photoproducts in the circadian timing system: searching for a physiological role for aryl hydrocarbon receptor. Toxicol Sci 95:172–181
Murphy DL, Lerner A, Rudnick G, Lesch KP (2004) Serotonin transporter: gene, genetic disorders, and pharmacogenetics. Mol Interv 4:109–123
Nemeroff CB, Owens MJ (2003) Neuropharmacology of paroxetine. Psychopharmacol Bull 37(Suppl 1):8–18
O’Shea JJ, Murray PJ (2008) Cytokine signaling modules in inflammatory responses. Immunity 28:477–487
Okada M, Kawata Y, Murakami T, Wada K, Mizuno K, Kondo T, Kaneko S (1999) Differential effects of adenosine receptor subtypes on release and reuptake of hippocampal serotonin. Eur J Neurosci 11:1–9
Orabona C, Grohmann U, Belladonna ML, Fallarino F, Vacca C, Bianchi R, Bozza S, Volpi C, Salomon BL, Fioretti MC, Romani L, Puccetti P (2004) CD28 induces immunostimulatory signals in dendritic cells via CD80 and CD86. Nat Immunol 5:1134–1142
Orabona C, Pallotta MT, Volpi C, Fallarino F, Vacca C, Bianchi R, Belladonna ML, Fioretti MC, Grohmann U, Puccetti P (2008) SOCS3 drives proteasomal degradation of indoleamine 2,3-dioxygenase (IDO) and antagonizes IDO-dependent tolerogenesis. Proc Natl Acad Sci U S A 105:20828–20833
Orabona C, Pallotta MT, Grohmann U (2012) Different partners, opposite outcomes: a new perspective of the immunobiology of indoleamine 2,3-dioxygenase. Mol Med 18:834–842
Oxenkrug GF (2010) Tryptophan kynurenine metabolism as a common mediator of genetic and environmental impacts in major depressive disorder: the serotonin hypothesis revisited 40 years later. Isr J Psychiatry Relat Sci 47:56–63
Pacifico L, Di Renzo L, Anania C, Osborn JF, Ippoliti F, Schiavo E, Chiesa C (2006) Increased T-helper interferongamma-secreting cells in obese children. Eur J Endocrinol 154:691–697
Pitt D, Nagelmeier IE, Wilson HC, Raine CS (2003) Glutamate uptake by oligodendrocytes: implications for excitotoxicity in multiple sclerosis. Neurology 61:1113–1120
Plotkin SR, Banks WA, Kastin AJ (1996) Comparison of saturable transport and extracellular pathways in the passage of interleukin-1 alpha across the blood-brain barrier. J Neuroimmunol 67:41–47
Qian F, Liao J, Villella J, Edwards R, Kalinski P, Lele S, Shrikant P, Odunsi K (2012) Effects of 1-methyltryptophan stereoisomers on IDO2 enzyme activity and IDO2-mediated arrest of human T cell proliferation. Cancer Immunol Immunother 61:2013–2020
Rassoulpour A, Wu HQ, Ferre S, Schwarcz R (2005) Nanomolar concentrations of kynurenic acid reduce extracellular dopamine levels in the striatum. J Neurochem 93:762–765
Raymond JR, Mukhin YV, Gelasco A, Turner J, Collinsworth G, Gettys TW, Grewal JS, Garnovskaya MN (2001) Multiplicity of mechanisms of serotonin receptor signal transduction. Pharmacol Ther 92:179–212
Rivest S, Lacroix S, Vallières L, Nadeau S, Zhang J, Laflamme N (2000) How the blood talks to the brain parenchyma and the paraventricular nucleus of the hypothalamus during systemic inflammatory and infectious stimuli. Proc Soc Exp Biol Med 223:22–38
Rocha VZ, Folco EJ, Sukhova G, Shimizu K, Gotsman I, Vernon AH, Libby P (2008) Interferon-gamma, a Th1 cytokine, regulates fat inflammation: a role for adaptive immunity in obesity. Circ Res 103:467–476
Roelands B, Meeusen R (2010) Alterations in central fatigue by pharmacological manipulations of neurotransmitters in normal and high ambient temperature. Sports Med 40:229–246
Röhl C, Lucius R, Sievers J (2007) The effect of activated microglia on astrogliosis parameters in astrocyte cultures. Brain Res 1129:43–52
Rothwell NJ, Luheshi G, Toulmond S (1996) Cytokines and their receptors in the central nervous system: physiology, pharmacology, and pathology. Pharmacol Ther 69:85–95
Rouzaud-Laborde C, Hanoun N, Baysal I, Rech JS, Mias C, Calise D, Sicard P, Frugier C, Seguelas MH, Parini A, Pizzinat N (2012) Role of endothelial AADC in cardiac synthesis of serotonin and nitrates accumulation. PLoS One 7:e34893
Santamaría A, Ríos C (1993) MK-801, an N-methyl-D-aspartate receptor antagonist, blocks quinolinic acid-induced lipid peroxidation in rat corpus striatum. Neurosci Lett 159:51–54
Santamaría A, Galván-Arzate S, Lisý V, Ali SF, Duhart HM, Osorio-Rico L, Ríos C, St’astný F (2001) Quinolinic acid induces oxidative stress in rat brain synaptosomes. Neuroreport 12:871–874
Schmitt A, Mössner R, Gossmann A, Fischer IG, Gorboulev V, Murphy DL, Koepsell H, Lesch KP (2003) Organic cation transporter capable of transporting serotonin is up-regulated in serotonin transporter-deficient mice. J Neurosci Res 71:701–709
Schröcksnadel K, Wirleitner B, Winkler C, Fuchs D (2006) Monitoring tryptophan metabolism in chronic immune activation. Clin Chim Acta 364:82–90
Schwarcz R (2004) The kynurenine pathway of tryptophan degradation as a drug target. Curr Opin Pharmacol 4:12–17
Schwarcz R, Pellicciari R (2002) Manipulation of brain kynurenines: glial targets, neuronal effects, and clinical opportunities. J Pharmacol Exp Ther 303:1–10
Schwarcz R, Rassoulpour A, Wu H-Q, Medoff D, Tamminga CA, Roberts RC (2001) Increased cortical kynurenate content in schizophrenia. Biol Psychiatry 50:521–530
Sibley DR, Benovic JL, Caron MG, Lefkowitz RJ (1987) Regulation of transmembrane signaling by receptor phosphorylation. Cell 48:913–922
Singh RK, Dai Y, Staudinger JL, Muma NA (2009) Activation of the JAK-STAT pathway is necessary for desensitization of 5-HT2A receptor-stimulated phospholipase C signalling by olanzapine, clozapine and MDL 100907. Int J Neuropsychopharmacol 12:651–665
Song NN, Xiu JB, Huang Y, Chen JY, Zhang L, Gutknecht L, Lesch KP, Li H, Ding YQ (2011) Adult raphe-specific deletion of Lmx1b leads to central serotonin deficiency. PLoS One 6:e15998
Srinivasan V, Pandi-Perumal SR, Brzezinski A, Bhatnagar KP, Cardinali DP (2011) Melatonin, immune function and cancer. Recent Patents Endocr Metab Immune Drug Discov 5:109–123
Stenman E, Lilja A (2013) Increased monoaminergic neurotransmission improves compliance with physical activity recommendations in depressed patients with fatigue. Med Hypotheses 80:47–49
Stephens GL, Wang Q, Swerdlow B, Bhat G, Kolbeck R, Fung M (2013) Kynurenine 3-monooxygenase mediates inhibition of Th17 differentiation via catabolism of endogenous aryl hydrocarbon receptor ligands. Eur J Immunol 43:1727–1734
Szelényi J (2001) Cytokines and the central nervous system. Brain Res Bull 54:329–338
Tilleux S, Berger J, Hermans E (2007) Induction of astrogliosis by activated microglia is associated with a down-regulation of metabotropic glutamate receptor 5. J Neuroimmunol 189:23–30
Vogel CF, Goth SR, Dong B, Pessah IN, Matsumura F (2008) Aryl hydrocarbon receptor signaling mediates expression of indoleamine 2,3-dioxygenase. Biochem Biophys Res Commun 375:331–335
Volk DW, Eggan SM, Lewis DA (2010) Alterations in metabotropic glutamate receptor 1α and regulator of G protein signaling 4 in the prefrontal cortex in schizophrenia. Am J Psychiatry 167:1489–1498
Waider J, Araragi N, Gutknecht L, Lesch KP (2011) Tryptophan hydroxylase-2 (TPH2) in disorders of cognitive control and emotion regulation: a perspective. Psychoneuroendocrinology 36:393–405
Watts SW (2009) The love of a lifetime: 5-HT in the cardiovascular system. Am J Physiol Regul Integr Comp Physiol 296:R252–R256
Wichers MC, Koek GH, Robaeys G, Verkerk R, Scharpé S, Maes M (2005) IDO and interferon-alpha-induced depressive symptoms: a shift in hypothesis from tryptophan depletion to neurotoxicity. Mol Psychiatry 10:538–544
Wirleitner B, Neurauter G, Schrocksnadel K, Frick B, Fuchs D (2003) Interferon-gamma-induced conversion of tryptophan: immunologic and neuropsychiatric aspects. Curr Med Chem 10:1581–1591
Wu G (2010) Functional amino acids in growth, reproduction, and health. Adv Nutr 1:31–37
Wu HQ, Pereira EF, Bruno JP, Pellicciari R, Albuquerque EX, Schwarcz R (2010) The astrocyte-derived alpha7 nicotinic receptor antagonist kynurenic acid controls extracellular glutamate levels in the prefrontal cortex. J Mol Neurosci 40:204–210
Wu X, Kushwaha N, Banerjee P, Albert PR, Penington NJ (2013) Role of protein kinase C in agonist-induced desensitization of 5-HT1A receptor coupling to calcium channels in F11 cells. Eur J Pharmacol 706:84–91
Yang R, Crowley HH, Rock ME, Kinnamon JC (2000a) Taste cells with synapses in rat circumvallate papillae display SNAP-25-like immunoreactivity. J Comp Neurol 424:205–215
Yang R, Tabata S, Crowley HH, Margolskee RF, Kinnamon JC (2000b) Ultrastructural localization of gustducin immunoreactivity in microvilli of type II taste cells in the rat. J Comp Neurol 425:139–151
Yang R, Ma H, Thomas SM, Kinnamon JC (2007) Immunocytochemical analysis of syntaxin-1 in rat circumvallate taste buds. J Comp Neurol 502:883–893
Yang R, Montoya A, Bond A, Walton J, Kinnamon JC (2012) Immunocytochemical analysis of P2X2 in rat circumvallate taste buds. BMC Neurosci 13:51
Yee CL, Yang R, Böttger B, Finger TE, Kinnamon JC (2001) “Type III” cells of rat taste buds: immunohistochemical and ultrastructural studies of neuron-specific enolase, protein gene product 9.5, and serotonin. J Comp Neurol 440:97–108
Yoshioka M, Matsumoto M, Togashi H, Mori K (1998) Central distribution and function of 5-HT6 receptor subtype in the rat brain. Life Sci 62:1473–1477
Yuan TM, Sun Y, Zhan CY, Yu HM (2010) Intrauterine infection/inflammation and perinatal brain damage: role of glial cells and toll-like receptor signaling. J Neuroimmunol 229:16–25
Zhu CB, Hewlett WA, Feoktistov I, Biaggioni I, Blakely RD (2004) Adenosine receptor, protein kinase G, and p38 mitogen-activated protein kinase-dependent up-regulation of serotonin transporters involves both transporter trafficking and activation. Mol Pharmacol 65:1462–1474
Zhu CB, Carneiro AM, Dostmann WR, Hewlett WA, Blakely RD (2005) p38 MAPK activation elevates serotonin transport activity via a trafficking-independent, protein phosphatase 2A-dependent process. J Biol Chem 280:15649–15658
Zhu CB, Steiner JA, Munn JL, Daws LC, Hewlett WA, Blakely RD (2007) Rapid stimulation of presynaptic serotonin transport by A(3) adenosine receptors. J Pharmacol Exp Ther 322:332–340
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Engin, A. (2015). Tryptophan-Related Signaling Molecules: Targets and Functions. In: Engin, A., Engin, A. (eds) Tryptophan Metabolism: Implications for Biological Processes, Health and Disease. Molecular and Integrative Toxicology. Humana Press, Cham. https://doi.org/10.1007/978-3-319-15630-9_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-15630-9_1
Publisher Name: Humana Press, Cham
Print ISBN: 978-3-319-15629-3
Online ISBN: 978-3-319-15630-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)