
Abstract
Osteochondral lesion (OCL) of the ankle joint is an injury involving the chondral layer and, secondarily, the subchondral bone, usually traumatic in etiology. The sprains and the mechanism of action may strongly influence the OCL pattern and the subsequent prognosis. OCL is frequently symptomatic, causing a mild persistent pain in chronic lesions. MRI is the most reliable diagnostic tool for preoperative evaluation. Athletes require effective treatments for OCL, with a rapid sport comeback and durable chondral restoration. This aim can be achieved only through regenerative techniques. These procedures, due to biological reasons, need longer time to heal. Although clear guidelines for OCL in athletes do not exist, Giannini’s classification, relying on the area and the depth of the lesion, could be successfully proposed. Conservative treatment should be suggested only in very small, not painful OCL. Debridement in small acute OCL and fixation in larger defects are two effective procedures. Microfractures could be advised in symptomatic, small chronic OCL (1.5–2 cm2). Larger chronic lesions may pose a serious challenge: microfractures may not achieve long-term, satisfying results. If regenerative techniques are suggested, athletes should be clearly warned of the longer times needed for rehabilitation after such procedures.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
52.1 Definition
Osteochondral lesion (OCL) of the ankle joint is an injury involving the chondral layer and, secondarily, the subchondral bone. It is usually localized on the talar dome, less frequently on the tibial plafond [1, 2].
52.1.1 Etiology
Ankle OCLs are usually traumatic in origin, mostly subsequent to ankle sprains or repetitive microtraumas [1]. Chondral lesions are present in 50 % of the acute ankle sprains and may be traced in 23 % of the lateral chronic instability of the ankle, causing persisting pain even after ligament reconstruction [3, 4]. Regarding the location, lateral lesions recognize a traumatic etiology in 93–98 % of the cases, whereas medial defects reported an ankle injury in only 60–71 % [1]. In a recent work by Orr, OCLs were centro-lateral (49 %) or centro-medial (33 %): specifically, the centro-lateral lesions were sent to surgery more frequently than the medial ones, which, nevertheless, tended to be larger [5]. The nontraumatic etiology can be confirmed for a small amount of cases, which have been addressed to various (weak) hypotheses as, for example, embolic, hereditary, endocrine, and idiopathic [6, 7].
52.1.2 Injury Mechanism and Natural History
Traumas causing lateral OCLs are ankle inversion or inversion-dorsiflexion [1, 8]. As described by Berndt-Hardy, the forced inversion causes the talar dome to impact on fibular surface, damaging the articular surface through a shearing force. In this case, the lesion looks superficial and oval [1, 8]. Medial OCL is less correlated to traumas; nevertheless, a combined torsional impaction and axial loading (plantar flexion, anterior displacement, and internal rotation of the talus on tibia during inversion) is the advocated preponderant etiology. It usually appears deeper than the lateral one and is described as cup shaped [8]. The most affected areas are the centro-medial and centro-lateral, with the last localization seriously injured by the rotational forces. So, the centro-lateral lesions are more prone to a surgical treatment, despite the lower surface involved [5].
The OCL may be limited to the chondral tissue, or it may involve the subchondral bone or, after intense traumas, may even isolate a loose body [1]. From a histological perspective, after the impact, the chondral layer is found to be softened, with a significant chondrocyte apoptosis and matrix degeneration. The hyaline cartilage is progressively replaced by fibrocartilage during the healing process. The subchondral bone is strongly reshaped by an increased osteoclastic activity, with an ultimate bone stock loss [9]. The presence of bone bruise is a significant prognostic factor of chondral damage, causing cartilage irregularities, chondrocyte apoptosis, and matrix degeneration [10]. Classically, OCL may evolve to osteoarthritis and, when symptomatic and large defects are found, should be addressed to surgery in order to avoid progression [6–8]. The work by Guettler highlighted that not only OCL provides a local osteochondral disruption but alters the biomechanics of the surrounding cartilage as well, predisposing to arthritis [11]. In a work by Choi, in line with the classical theory of Berndt-Hardy, a critical size defect was traced at 150 mm2 OCL, with good healing for defects with lower area [4, 8].
52.2 Clinical and Diagnostic Examination
Acute OCLs are frequently reported by young patients following a major trauma or ankle sprain during sport activity [1, 7, 12]. Swelling, pain, and symptoms related to lateral ligament lesions may be present. Locking, or catching, is associated with displaced fragments. Pain and limited range of motion (ROM) usually persist over 4–6 weeks after the acute event [1, 8, 12].
Chronic OCL most frequent symptom is a mild, continuous pain, mostly associated with physical activity [1, 8, 12]. Asymptomatic cases are not uncommon. Walking on uneven ground may increase the symptoms. Swelling, stiffness, weakness, and reduced ROM may be present, mostly in degenerated OCL. Patients may complain for the inability to load on the joint and, in case of loose bodies, for catching, locking, or clicking [1, 8, 12].
Palpation often evokes tenderness on posterior-medial or anterior-lateral areas of the talus [1, 8, 12]. The range of motion may be limited in half of the cases. Limpness, or antalgic gait, is relatively common. Anterior drawer and talar tilt test should be performed as sprains usually underlie OCL. Other tendon, vascular, and neurological pathologies should be ruled out (Table 52.1).
Routine X-ray is the first-line diagnostic tool also in order to rule out a fracture in acute cases [13]. Nevertheless, apart large lesions, OCL can easily be undiagnosed [14].
CT is valuable for the detection of subchondral bone injuries: it may clearly detect the size, shape, and extent of the localization (Fig. 52.1) [15].

Coronal view of a CT scan performed for OCL preoperative evaluation. CT scan is very useful to improve subchondral bone visualization
MRI is the gold standard for OCL diagnosis, providing information about bone bruise, cartilage status, and soft tissues [15]. The sensitivity of MRI is high when correlated to arthroscopic findings (81–83 % or even higher) [16]. The most frequent features compatible with OCL are decreased signal intensity on T1-weighted images and increased intensity on T2-weighted images. In case of incomplete separation of the fragment, T2-weighted images may be confusing due to a high signal, with lower percentage of correlation with arthroscopic findings (55.6 %). In this case, the cartilage break discriminates (Fig. 52.2) [16].

Coronal view of MRI scan performed for chronic medial OCL. MRI is the best diagnostic tool, as it can visualize the cartilage and the subchondral bone as well as other soft tissue as ligaments
52.3 Treatment Strategy
No widely shared guidelines exist for OCL treatment [14, 17, 18]. A valid classification, focused on arthroscopic/MRI findings and corresponding treatments, considering the area and the depth of the lesions as well, was made by Giannini [19].
52.3.1 Acute Lesions
Conservative treatment is not successful in acute lesions, requiring arthroscopic procedures. Debridement and fragment excision are advised in case of acute lesions with fragment’s dimensions inferior to 1 cm [19, 20]. Fragment fixation is performed in case of larger OCL using bioresorbable screws: good long-term results are achieved thanks to an effective vascular restoration [21]. Excision for larger fragment can dramatically raise osteoarthritis rates at long-term follow-up [20]. Recently osteochondral autografts have been adopted, with good results even in acute lesions [21].
52.3.2 Chronic Lesions
52.3.2.1 Conservative Treatment
The aim of conservative treatment is unloading the osteochondral layer, preventing the necrosis, and resolving the bone edema. To date, it should be reserved to small lesions with no fragment isolation in almost-asymptomatic patients [14, 17, 22]. In these cases, 45 % of the patients may benefit from a conservative approach. A possible beneficial approach in athletes may consist in rest, with sport activity restriction, and even a limited period of non-weight-bearing, lasting only a few weeks, according to the gravity of the lesion. In a work by Mei-Dan, hyaluronate and platelet-rich plasma (PRP) were injected intra-articularly in OCL, improving the clinical outcomes, with long-lasting results for PRP (at least 6 months) [23]. Intra-articular injections may be functional in athletes to delay the surgical treatment even in symptomatic lesions with no fragment isolation.
52.3.2.2 Retrograde Drilling
Retrograde drilling is mostly effective in lesions 0 according to Giannini’s classification, with modest subchondral bone involvement and chondral layer continuity and viability [19]. The rationale consists in a stimulation of the repair depending on subchondral bone marrow cells [19, 24, 25]. The approach is made through sinus tarsi, drilling the subchondral bone without damaging the articular surfaces. An autologous calcaneal bone graft is then performed. Retrograde drilling may avoid the necrotic effect of the anterograde approach, preserving the chondral tissue [25]. Good results were reached in case of viable cartilage; nevertheless, it has been applied even in revision surgery [25].
52.3.2.3 Microfractures
Widely diffused microfractures are effective in OCL inferior to 1.5 cm2 [6, 7, 19, 26]. The technique can be easily performed arthroscopically, penetrating the subchondral bone every 3–4 mm, using an awl [26]. Thanks to bone marrow stimulation, this procedure allows a good and rapid restoration of the osteochondral layer, but it generates fibrocartilage, with lower biomechanical properties and durability [14, 24]. Good clinical outcomes were reported by many authors, but medial lesions and larger and deep OCL tended to worsen over the time [26, 27].
52.3.2.4 Mosaicplasty
Osteochondral plugs, obtained from non-weight-bearing areas of the knee and, possibly, ankle, are implanted to restore the proper osteochondral layer [22, 24, 28]. This procedure often requires a malleolar osteotomy to improve the exposure. In the report by Hangody [22], the best OCL to treat is defined as approximately 10 mm large, positioned on the medial or lateral dome (not the central part of the talus), in a non-arthritic ankle. Clinical and bioptic results were promising, achieving remarkable outcomes even in athletes (63 % of the patients came back to sport activity at the same level, only 9 % gave up sport), with a slight deterioration over time, at around 10 years from the surgical procedure [28]. Nevertheless, mosaicplasty faces some drawbacks. First, it is a technical demanding technique, which includes a donor-site morbidity. Between osteochondral plugs, fibrocartilage is frequently found; moreover, not all lesions are successfully treated due to challenging locations (Fig. 52.3) [22, 24, 28].

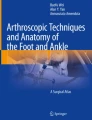
Intraoperative arthroscopic images during BMDCT. This procedure can be performed using an arthroscopic one-step technique. First, the lesion is debrided, reaching a healthy subchondral bone. Then the biomaterial, a collagen membrane loaded with autologous mesenchymal stem cells, is implanted. Then a layer of PRF is sprayed on the biomaterial, to improve the stability of the implant and the cell differentiation and growth
52.3.2.5 Autologous Chondrocyte Implantation
Autologous chondrocyte implantation (ACI) has been intensively applied for OCL of the ankle, with successful clinical outcomes (90 %) [18]. Although no clear superiority has been established, ACI is considered the gold standard in regenerative procedures [18, 19]. The first-generation procedure was technically demanding, requiring an open-field approach, a malleolar osteotomy, and a periosteal flap suture [18, 29]. The second-generation procedure was performed arthroscopically, thanks to the development of specific instrumentation and scaffold [29]. Arthroscopic technique is performed with a two-step approach, with a first arthroscopy to debride the lesion and harvest the autologous chondrocytes doomed to expansion. A source of viable chondrocytes is the osteochondral fragment, the area around the OCL, or even a non-weight-bearing area of the knee [29, 30]. After the first arthroscopy, the chondrocytes are expanded in culture and seeded on a hyaluronate membrane. After 3 weeks, the second step takes place, and the biomaterial is arthroscopically implanted onto the lesion. The hyaline regeneration was confirmed by histological and radiological outcomes [29, 30].
52.3.2.6 Bone Marrow-Derived Cell Transplantation
Bone marrow-derived cell transplantation (BMDCT) is a regenerative technique for bony and chondral layer, based on mesenchymal stem cells [19, 24, 31]. This technique may be performed in one step, in a same surgical session, or with more steps, with cells culture and enrichment: good results were achieved also in degenerated joints [19, 24, 31]. In the one-step technique, the cells are harvested from the iliac crest using a bone marrow needle. During the concentration, a standard arthroscopy of the ankle is performed; the joint and the defect is debrided. The cell concentrate is loaded on a collagen (or hyaluronate) membrane and then implanted in the joint using a specific instrumentation [31]. Then, a layer of platelet-rich fibrin (PRF) is sprayed on the biomaterial, to improve growth and differentiation and stability of the implant. Clinical results at medium-term follow-up are encouraging, with excellent outcomes even in athletes. Hyaline cartilage regeneration has been appreciated in bioptic samples and MRI qualitative scans [19, 31].
52.3.2.7 Allograft
Ankle allograft is a biological reconstruction, which should be reserved to high degenerated joints: it can be partial or total [19, 24]. Ankle may be approached laterally or anteriorly, with a fixation of both the articular surfaces using articular pins. The clinical and radiological outcomes are encouraging, and there is evidence of hyaline cartilage presence and colonization of host cells [19, 24]. Nevertheless, the indications of this procedure are selective and encompass young, active people with disrupted anatomy of the ankle [19].
52.4 Rehabilitation and Return to Play
Very few evidences about rehabilitation and return to play exist in literature, and many confounding factors may vary the outcomes [32]. Youth, small lesions, and lower BMI have been advocated as positive prognostic factors in a precocious sport comeback [32]. Nowadays, the two key points in cartilage rehabilitation are continuous passive motion, which may provide a good chondral nutrition, and careful weight-bearing, which may avoid the deleterious effects of overloading. Positive results may be achieved, thanks to pulse electromagnetic fields, bisphosphonates, or injective therapy with hyaluronate or platelet-rich plasma [23, 32]. A personalized program should always be recommended in athletes.
52.4.1 Fragment Fixation
A posterior splint or cast is advised in the first 2 weeks, then a passive continuous motion is recommended, and a partial weight-bearing, possibly with ankle in brace, is allowed not before 4 weeks [21].
52.4.2 Drilling
Active movements are encouraged since the day after surgery, while weight-bearing is proscribed for 6 weeks [25].
52.4.3 Microfractures
Rehabilitation after microfractures requires non-weight-bearing in ankle brace for 3 weeks. A progressive weight-bearing is then allowed, promoting exercises for proprioception and range of motion. Return to sport was advised not before 12 weeks [26]. In a work by Lee, early or delayed weight-bearing (after 1 week or 6 weeks) after microfractures for OCL did not influence the final outcome [33].
52.4.4 Mosaicplasty
Continuous passive motion is allowed the day after surgery, but the ankle is kept non-weight-bearing for 3 weeks (6 weeks in case of osteotomy), which is necessary for graft incorporation [22, 28]. A progressive, partial weight-bearing is allowed. After 6 weeks complete weight-bearing is allowed, and athletic activities can be started after 6 months after surgery [22, 28].
52.4.5 ACI and BMDCT
Regenerative techniques require a specific timetable for rehabilitation, due to biological properties of the implanted cells [34]. For a large division and initial incorporation, chondrocytes require 6 weeks. Between 3 and 6 months, a primitive extracellular matrix is produced [19, 24, 34]. After 6 months, a progressive integration of the biomaterial with the subchondral bone occurs. Remodeling and maturation continue for 2–3 years [34]. The rehabilitation protocol for regenerative techniques should take into account this process, resulting in a mix of continuous passive motion, progressive weight-bearing, and muscular strengthening. Personalized schemes should be encouraged, but they have to share a precise program. The day after surgery, continuous passive motion is advised, and a Walker ankle brace is applied [34]. The period of non-weight-bearing lasts about 6 weeks; then a period of partial, progressive weight-bearing of 2 weeks follows. After 4 months from surgery, low-impact sport activities (swimming, cycling, etc.) can be safely performed. A progressive return to running and high-impact sport activities is not allowed before 10 months.
52.5 Conclusions
Athletes required effective treatments for OCL, with a rapid sport comeback. This aim is quite difficult to be achieved, as a good restoration of qualitative and durable hyaline cartilage can be achieved only through regenerative techniques. These procedures, due to biological reasons, need longer time to heal. Although clear guidelines for OCL in athletes do not exist, conservative treatment should be proposed only in very small, not painful OCL. Debridement in small acute OCL and fixation in larger defects are two effective procedures. Microfractures could be advised in symptomatic, small chronic OCL (1.5–2 cm2). Larger chronic lesions may pose a serious challenge: microfractures may not achieve satisfying results. If regenerative techniques are suggested, athletes should be clearly warned of the longer times needed for rehabilitation after such procedures.
References
van Dijk CN, Reilingh ML, Zengerink M et al (2010) Osteochondral defects in the ankle: why painful? Knee Surg Sports Traumatol Arthrosc 18(5):570–580. doi:10.1007/s00167-010-1064-x
Schachter AK, Chen AL, Reddy PD, Tejwani NC (2005) Osteochondral lesions of the talus. J Am Acad Orthop Surg 13(3):152–158
Saxena A, Eakin C (2007) Articular talar injuries in athletes: results of microfracture and autogenous bone graft. Am J Sports Med 35(10):1680–1687
Choi WJ, Park KK, Kim BS, Lee JW (2009) Osteochondral lesion of the talus: is there a critical defect size for poor outcome? Am J Sports Med 37(10):1974–1980. doi:10.1177/0363546509335765
Orr JD, Dutton JR, Fowler JT (2012) Anatomic location and morphology of symptomatic, operatively treated osteochondral lesions of the talus. Foot Ankle Int 33(12):1051–1057. doi:10.3113/FAI.2012.1051
Murawski CD, Kennedy JG (2013) Operative treatment of osteochondral lesions of the talus. J Bone Joint Surg Am 95(11):1045–1054. doi:10.2106/JBJS.L.00773
Talusan PG, Milewski MD, Toy JO et al (2014) Osteochondritis dissecans of the talus: diagnosis and treatment in athletes. Clin Sports Med 33(2):267–284. doi:10.1016/j.csm.2014.01.003
Canale ST, Belding RH (1980) Osteochondral lesions of the talus. J Bone Joint Surg Am 62(1):97–102
Koch S, Kampen WU, Laprell H (1997) Cartilage and bone morphology in osteochondritis dissecans. Knee Surg Sports Traumatol Arthrosc 5(1):42–45
Johnson DL, Urban WP Jr, Caborn DN et al (1998) Articular cartilage changes seen with magnetic resonance imaging-detected bone bruises associated with acute anterior cruciate ligament rupture. Am J Sports Med 26(3):409–414
Guettler JH, Demetropoulos CK, Yang KH et al (2004) Osteochondral defects in the human knee: influence of defect size on cartilage rim stress and load redistribution to surrounding cartilage. Am J Sports Med 32(6):1451–1458
van Dijk CN, Reilingh ML, Zengerink M et al (2010) The natural history of osteochondral lesions in the ankle. Instr Course Lect 59:375–386
Dheer S, Khan M, Zoga AC et al (2012) Limitations of radiographs in evaluating non-displaced osteochondral lesions of the talus. Skeletal Radiol 4:415–421
Navid DO, Myerson MS (2002) Approach alternatives for treatment of osteochondral lesions of the talus. Foot Ankle Clin 7(3):635–649
Ferkel RD, Flannigan BD, Elkins BS (1991) Magnetic resonance imaging of the foot and ankle: correlation of normal anatomy with pathologic conditions. Foot Ankle 11:289–305
Bae S, Lee HK, Lee K et al (2012) Comparison of arthroscopic and magnetic resonance imaging findings in osteochondral lesions of the talus. Foot Ankle Int 33(12):1058–1062. doi:10.3113/FAI.2012.1058
Verhagen RA, Struijs PA, Bossuyt PM et al (2003) Systematic review of treatment strategies for osteochondral defects of the talar dome. Foot Ankle Clin 8(2):233–242, viii–ix
Niemeyer P, Salzmann G, Schmal H et al (2012) Autologous chondrocyte implantation for the treatment of chondral and osteochondral defects of the talus: a meta-analysis of available evidence. Knee Surg Sports Traumatol Arthrosc 20(9):1696–1703. doi:10.1007/s00167-011-1729-0
Giannini S, Buda R, Faldini C et al (2005) Surgical treatment of osteochondral lesions of the talus in young active patients. J Bone Joint Surg Am 87(Suppl 2):28–41
Badekas T, Takvorian M, Souras N (2013) Treatment principles for osteochondral lesions in foot and ankle. Int Orthop 37(9):1697–1706. doi:10.1007/s00264-013-2076-1
Liu W, Liu F, Zhao W et al (2011) Osteochondral autograft transplantation for acute osteochondral fractures associated with an ankle fracture. Foot Ankle Int 32(4):437–442. doi:10.3113/FAI.2011.0437
Hangody L (2003) The mosaicplasty technique for osteochondral lesions of the talus. Foot Ankle Clin 8(2):259–273
Mei-Dan O, Carmont MR, Laver L et al (2012) Platelet-rich plasma or hyaluronate in the management of osteochondral lesions of the talus. Am J Sports Med 40(3):534–541. doi:10.1177/0363546511431238
Giannini S, Vannini F (2004) Operative treatment of osteochondral lesions of the talar dome: current concepts review. Foot Ankle Int 25(3):168–175
Taranow WS, Bisignani GA, Towers JD et al (1999) Retrograde drilling of osteochondral lesions of the medial talar dome. Foot Ankle Int 20:474–480
Ventura A, Terzaghi C, Legnani C et al (2013) Treatment of post-traumatic osteochondral lesions of the talus: a four-step approach. Knee Surg Sports Traumatol Arthrosc 21(6):1245–1250. doi:10.1007/s00167-012-2028-0
Yoshimura I, Kanazawa K, Takeyama A et al (2013) Arthroscopic bone marrow stimulation techniques for osteochondral lesions of the talus: prognostic factors for small lesions. Am J Sports Med 41(3):528–534. doi:10.1177/0363546512472979
Hangody L, Dobos J, Baló E et al (2010) Clinical experiences with autologous osteochondral mosaicplasty in an athletic population: a 17-year prospective multicenter study. Am J Sports Med 38(6):1125–1133. doi:10.1177/0363546509360405
Giannini S, Buda R, Ruffilli A et al (2014) Arthroscopic autologous chondrocyte implantation in the ankle joint. Knee Surg Sports Traumatol Arthrosc 22(6):1311–1319. doi:10.1007/s00167-013-2640-7
Battaglia M, Vannini F, Buda R et al (2011) Arthroscopic autologous chondrocyte implantation in osteochondral lesions of the talus: mid-term T2-mapping MRI evaluation. Knee Surg Sports Traumatol Arthrosc 19(8):1376–1384. doi:10.1007/s00167-011-1509-x
Giannini S, Buda R, Battaglia M et al (2013) One-step repair in talar osteochondral lesions: 4-year clinical results and t2-mapping capability in outcome prediction. Am J Sports Med 41(3):511–518. doi:10.1177/0363546512467622
van Eekeren IC, Reilingh ML, van Dijk CN (2012) Rehabilitation and return-to-sports activity after debridement and bone marrow stimulation of osteochondral talar defects. Sports Med 42(10):857–870. doi:10.2165/11635420-000000000-00000
Lee DH, Lee KB, Jung ST (2012) Comparison of early versus delayed weightbearing outcomes after microfracture for small to midsized osteochondral lesions of the talus. Am J Sports Med 40(9):2023–2028. doi:10.1177/0363546512455316
Nho SJ, Pensak MJ, Seigerman DA et al (2010) Rehabilitation after autologous chondrocyte implantation in athletes. Clin Sports Med 29(2):267–282, viii. doi:10.1016/j.csm.2009.12.004
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Giannini, S., Buda, R.E., Cavallo, M., Gherardo, P., Francesco, C., Vannini, F. (2016). Ankle Osteochondral Lesions. In: Volpi, P. (eds) Arthroscopy and Sport Injuries. Springer, Cham. https://doi.org/10.1007/978-3-319-14815-1_52
Download citation
DOI: https://doi.org/10.1007/978-3-319-14815-1_52
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-14814-4
Online ISBN: 978-3-319-14815-1
eBook Packages: MedicineMedicine (R0)