
Abstract
During Th1-type immune response, tryptophan-degrading enzyme indoleamine 2,3-dioxygenase (IDO) becomes activated and accelerates the breakdown of tryptophan, as expressed by a higher kynurenine to tryptophan ratio. Lowered tryptophan concentrations were detected in patients suffering from immunopathologies like virus infections, autoimmune syndromes, and certain types of cancer, and in some of these clinical conditions, an association between enhanced tryptophan breakdown and mood disturbances was observed. Tryptophan is required for the biosynthesis of 5-hydroxytryptamine (serotonin), and the availability of tryptophan in the blood is linked to its concentration in the brain, as tryptophan can cross the blood-brain barrier. In patients at risk for cardiovascular disease, higher concentrations of neopterin are associated with lower concentrations of vitamins C and E and other antioxidants. Data may indicate that chronic immune activation leads to an enhanced degradation of oxidation-sensitive biomolecules. Likewise, additional antioxidant vitamin supplementation might be able to counteract the inflammation process. However, this concept is mainly derived from in vitro data, whereas in vivo findings remain scarce. In vitro, it was also documented that several antioxidant compounds including vitamins C and E and stilbene resveratrol but also food preservatives and colorants are able to slow down Th1-type immune activation leading to a suppression of IDO activity. Similar effects were observed for extracts of beverages known to be rich in antioxidants like wine, beer, cacao, and coffee. The suppressive effects of antioxidant molecules and extracts on tryptophan breakdown could relate to their mood-enhancing properties.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Antioxidants
- Immune activation
- Indoleamine 2,3-dioxygenase
- Inflammation
- Interferon-γ
- Neopterin
- Reactive oxygen species
- Serotonin
- Tryptophan
- Vitamins
Introduction
Tryptophan is one of the essential amino acids in humans, which means that the human organism is incapable of synthesizing it by itself. Therefore, nutrition is most relevant for tryptophan supply. Alternatively, it can be recruited only via degradation of proteins. Because tryptophan is also the least abundant amino acid in food, the availability of tryptophan is an important regulator of protein biosynthesis. Additionally, tryptophan is the precursor of two important biochemical pathways, which in a first step involve either enzyme tryptophan 5-monoxygenase (tryptophan 5-hydroxylase) that initializes the synthesis of neurotransmitter 5-hydroxytryptamine (serotonin) or tryptophan 2,3-dioxygenase (TDO) and indoleamine 2,3-dioxygenases (IDO1 and IDO2). The latter enzymes introduce tryptophan into the so-called tryptophan-kynurenine pathway, which is named after its first stable intermediate kynurenine.
Further downstream metabolites are kynurenic acid, 3-hydroxykynurenine, 3-hydroxyanthranilic acid, picolinic and quinolinic acid, and nicotinamide adenine dinucleotide (NAD) [1]. It has to be mentioned that substrate specificity of IDO is less than that of TDO, which solely accepts tryptophan as a substrate, whereas IDO also degrades other indoleamine derivatives like serotonin, albeit with lesser efficacy.
TDO is mainly expressed in hepatocytes, but TDO activity can rarely be detected outside the liver. Enzyme activity is regulated by the tryptophan level in the blood and upregulated by corticosteroids. The conversion of tryptophan to kynurenine leads to a rather constant kynurenine to tryptophan (Kyn/Trp) ratio in the blood, which in human is around 27 ± 8.1 μmol/mmol (tryptophan 73 ± 15 μmol/L and kynurenine 1.9 ± 0.58 μmol/L), women presenting with approximately 15 % higher levels than men [2]. In the normal situation, expression and activity of IDO are low, but can be increased severalfold during inflammatory conditions by pro-inflammatory mediators like lipopolysaccharides (LPS) or specific cytokines, whereby Th1-type cytokine interferon-γ (IFN-γ) is the strongest inducer [3–5]. This explains why increased tryptophan breakdown, as indicated by increased Kyn/Trp concentrations, is commonly observed in patients under treatment with interferons or other stimulatory cytokines like interleukin-2 [6], but also in patients suffering from viral infections like HIV-1, autoimmune syndromes such as systemic lupus erythematosus [7], malignant cancers like malignant melanoma [8], or adult T-cell leukemia [9]. In such clinical conditions, significant correlation between Kyn/Trp ratio and concentrations of immune activation markers like serum soluble cytokine receptors sTNF-R75 and sIL-2R or of the macrophage product neopterin further substantiates the conclusion that the increased tryptophan breakdown rate is due to cytokine-induced IDO activity rather than TDO [10].
The alterations of Kyn/Trp ratio are usually more significant than the absolute kynurenine concentrations. Still significant association between concentrations of kynurenine and immune activation marker neopterin was observed in patients with HIV-1 infection, but it was not significant in patients with colorectal cancer [11], or adult T-cell leukemia [9], or in healthy pregnant women [12]. Thus, even when increased Kyn/Trp ratio shows that the conversion of tryptophan to kynurenine is accelerated, kynurenine does not accumulate much because most likely in the liver the compound is rapidly converted to downstream products of the kynurenine pathway as mentioned above [1] and these concentrations increase [13]. However, for example, in the absence of sufficient supply with B vitamins, the conversion of kynurenine by downstream enzymes kynurenine monooxygenase and kynurenine aminotransferases is decreased, and kynurenine concentrations might accumulate [14].
Tryptophan Breakdown and Immunity
During Th1-type immune response, IDO becomes activated mainly by IFN-γ and manifests in increased Kyn/Trp concentrations (Fig. 6.1). Tryptophan breakdown and deprivation are part of the antiproliferative strategy of the immune system to halt growth of pathogens and of malignant cells. Restrictions of essential nutrient availability as well as metabolic reprogramming are universal strategies to mediate growth inhibition. For example, iron and zinc pools in circulation can be reduced by increasing renal excretion or storage at other body sites. Also, the supply of lipids becomes disturbed in inflammatory conditions [15].

Upon stimulation of type 1 T-helper cells (T cell) by, e.g., mitogen phytohemagglutinin (PHA), cytokine interferon-γ (IFN-γ) is released that activates [“+”] antimicrobial strategies and immunoregulatory cascades in target cells like macrophages (hMφ) and dendritic cells (DC). Among them are the production of cytotoxic reactive oxygen species (ROS) and the induction of tryptophan-degrading enzyme indoleamine 2,3-dioxygenase (IDO) and GTP cyclohydrolase (GCH), which usually leads to the formation of tetrahydrobiopterin (BH4), the necessary cofactor of inducible nitric oxide synthase (iNOS), but in human monocyte-derived cells like hMφ and hDC gives rise to the production of neopterin at the expense of BH4. Diminished blood tryptophan levels due to IDO activity will slow down production of serotonin in the brain and lower mood. The possible direct effect of IDO degrading serotonin further strengthens the influence of IDO activation on neuropsychiatric performance of patients suffering from inflammatory conditions
Already in 1984, it has been clearly shown by E.R. Pfefferkorn that the growth of Toxoplasma gondii was inhibited upon treatment with IFN-γ [16], and the induction of tryptophan degradation was responsible for this effect: as a “note added in proof,” the involvement of IDO in this biochemical alteration was suggested. Moreover, this study showed that the growth of T. gondii could be reestablished, when tryptophan was added back to culture, and it could be excluded that the accumulation of toxic tryptophan breakdown products was important for growth inhibition. In parallel, tryptophan breakdown was found to be accelerated in patients with cancer under treatment with IFN-γ [6], and in many clinical conditions, which go along with activated T-cell/macrophage responses, e.g., infections, autoimmune syndromes, and cancer, an enhanced Kyn/Trp ratio was observed in serum, plasma, and other body fluids such as cerebrospinal fluid [10].
Activated IDO by pro-inflammatory cytokines like IFN-γ represents the background for lowered tryptophan concentrations in patients suffering from certain types of cancer [10]; although a few tumor cell lines were observed to spontaneously express IDO, TDO, or both and degrade tryptophan, the IDO activity is enhanced severalfold in the presence of IFN-γ [17, 18]. Frequently, a higher tryptophan breakdown rate is associated with a reduced residual lifespan in patients, which seems to indicate a diminished functional immune response. In fact, patients with poor prognosis are characterized by several signs of an activated immune system, including elevated neopterin concentrations and tryptophan breakdown rates. Thus, it turns out that the antiproliferative effects of tryptophan deprivation also interfere with the development and proliferation of T cell and their responsiveness. Moreover, the accumulation of immunotoxic tryptophan breakdown products like quinolinic acid and 3HAA seems to be of major relevance for the induction of T-cell apoptosis [19] and generation of regulatory T cells (Treg) [20].
Tryptophan and Mood in Inflammatory Conditions
Signs of depression are common in patients suffering from a wide range of inflammatory conditions including infections, autoimmune pathologies like systemic lupus erythematosus, cardiovascular disease, and cancer, but also in elderly people that are characterized by lower levels of tryptophan. In general, the development of neuropsychiatric disturbances seems to represent a sign of poor outcome. In some of these clinical conditions, an association between enhanced tryptophan breakdown and increase of neuropsychiatric symptoms was observed [21–26].
Also, the treatment with cytokines like IFN-γ of patients with hepatitis C virus infection or malignant melanoma is associated with an increased risk for developing mood changes. Under treatment with IFNs, the enhanced tryptophan breakdown rate, which is already common in untreated patients, is further enhanced [6]. Likewise, in patients with malignant melanoma, an association was observed between depression development and the decline of tryptophan during follow-up of therapy [27]. In the same way, studies showed an association between lower blood tryptophan levels in cancer patients and higher degree of fatigue and quality of life scores, in, e.g., patients with colorectal cancer [11, 25]. In older individuals, several significant relationships were observed between tryptophan metabolic alterations in the blood and signs of mood alterations [28–30]. However, in most of these studies, either the absolute tryptophan concentrations or Kyn/Trp ratio revealed significant relationships, but the alterations of the absolute kynurenine levels were not significant. It appears that the kynurenine produced out of tryptophan becomes rapidly converted to its downstream products in the pathway like quinolinic acid, quinolinic acid concentrations themselves correlating rather well with neopterin levels [13]. Interestingly, in suicide attempters with major depression, plasma kynurenine levels were higher than in those without [31].
Also studies performed in animal models were able to show an association between tryptophan breakdown and the development of depressive behavior as, e.g., in the forced swim test or tail suspension test with mice, when tryptophan breakdown was induced upon exposure to Bacillus Calmette-Guerin [32]. In conclusion, pro-inflammatory cytokines like IFN-γ that are released during Th1-type immune activation and inflammation restrict tryptophan availability, and thus, also serotonin production is hampered, and the risk of low mood and depression can be increased. From the existing literature, it appears that IDO activity is a key player in the pathogenesis of depressive mood that are associated with inflammation and immune activations, although also biochemistry downstream of kynurenine may play a role as it is claimed in individuals with depression but excluding inflammation [33]. Neuroactive kynurenine downstream metabolites such as kynurenic acid, quinolinic acid, and 3-hydroxykynurenine are involved in several important regulatory processes in the brain, and besides their involvement in the development of depression and other psychiatric disorders, dysregulated production of these metabolites is associated also with several neurologic disorders and neurodegeneration. The levels of brain kynurenine pathway metabolites are at least partially dependent on peripheral concentrations of tryptophan, kynurenine, and 3-hydroxyanthtranilic acid, as these compounds can cross the blood-brain barrier. Additionally, other immunocompetent cells within the brain such as microglia are able to activate the tryptophan-kynurenine pathway themselves in response to immune activation signals.
One might hypothesize that the association between inflammatory conditions and an accelerated tryptophan breakdown could also be related with partnering behavior of individuals, when partners are selected depending on their mood level [34]. Many studies revealed that individuals with humor and positive mood are more likely to be chosen as partners than those with opposite attitudes, suggesting that a partner with positive thoughts, optimistic views, and fun is more likely free of infectious or inflammatory conditions and thus having a longer residual lifespan. Such partners may present with positive mood due to higher tryptophan levels which indicate less inflammation activity and lower risk of malignant or infectious diseases, i.e., higher probability of togetherness for a longer period of time, because such individuals are less likely to suffer from inflammatory conditions. However, potential associations of tryptophan levels, personality profiles, and partner selection have still to be analyzed.
Anti-inflammatory and Antioxidant Compounds Slow Down Tryptophan Breakdown
From in vitro and in vivo, it is well established that pro-inflammatory cytokines like IFN-γ, LPS, and TNF-α induce IDO and thus tryptophan breakdown in human macrophages and dendritic cells and also in other cells like fibroblasts or tumor cell lines [17, 18]. In monocyte-derived macrophages, IFN-γ was noted to be the strongest inducer [3, 5]; whereas, in dendritic cells and astrocytes, IFN-α, IFN-β, and IFN-γ were found to be of equal potency [35, 36]. In contrast, immunosuppressants like cyclosporine A and rapamycin [37], anti-inflammatory compounds like acetylsalicylic acid and salicylic acid [38], and also statins [39] slow down Th1-type immune response, and thus, tryptophan breakdown ceases. Because IFN-γ is also the strongest inducer for the production of reactive oxygen species (ROS) in human macrophages [40] together with neopterin, the induction of the cells during Th1-type immune response is usually accompanied by a high output of ROS, and when antioxidant pools become wiped out, oxidative stress will develop. Moreover, the formation of ROS further enhances the formation of pro-inflammatory cytokines in an autocrine manner via translocation of the nuclear factor-κB (NF-κB), the central signal transduction element in the expression of various pro-inflammatory cytokines like TNF-α [41], and also specific enzymes like the inducible nitric oxide synthase (iNOS) [42].
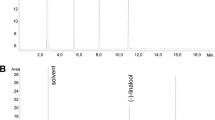
Antioxidant compounds are therefore able to counteract the pro-inflammatory cytokine cascade at least in the in vitro setting and are considered to be of help in clinical situations that are associated with excess ROS production as it is the case in inflammatory conditions and chronic immune activation. In vitro studies have also shown that antioxidant compounds like vitamins C and E, the stilbene resveratrol, and also food preservatives like sodium sulfite or benzoate and colorants like curcumin and beet root juice suppress the production of IFN-γ [43, 44], and in turn, the activity of IDO is diminished (Fig. 6.2). As a consequence, tryptophan levels rise. Similar effects were observed for extracts of beverages known to be rich in antioxidants like wine, beer, or cacao and coffee. Thereby, the antioxidative effects of flavonoid compounds contained in such beverages are considered to be of major relevance for the immunosuppressive properties [45]. Thus, the increased use of dietary supplements including preservatives and colorants may contribute to a suppression of Th1-type immune response. In freshly isolated human peripheral blood mononuclear cells in vitro, it was shown that antioxidant compounds like vitamins C and E but also food preservatives and colorants exert significant suppressive effects on the Th1 immune activation cascade [46, 47]. The effects observed may be based on the interaction of antioxidant compounds with pro-inflammatory cascades involving important signal transduction elements such as NF-κB. Likewise, in dendritic cells, the antioxidant vitamins C and E have been demonstrated to promote production of Th2-type cytokines IL-4 and IL-10 in a dendritic cell coculture system, and it was shown that the T cells expressed FoxP3 and, besides being anergic, might have acquired Treg properties [48].

Antioxidant compounds are able to neutralize reactive oxygen species (ROS) and slow down (“−”) Th1-type immune activation cascades. This is especially true if compounds are added in high concentrations as food supplements (= extra vitamins) and also in the form of food preservatives and colorants. Such supplements suppress IDO activity, which on the one hand counteracts immune defense and thus may increase malignant growth and on the other hand will enhance serotonin availability and improve mood
In vivo, for example, in patients at risk for cardiovascular disease, higher concentrations of vitamins C and E and other antioxidant biomolecules like lycopene, lutein, zeaxanthin, and carotenes were found to be associated with lower neopterin concentrations [49]. One might conclude that insufficient supply with such vitamins could feed the inflammation process and additional antioxidant vitamins might be able to counteract it. Alternatively, data may relate to the fact that chronic immune activation leads to an enhanced degradation of oxidation-labile biomolecules such as antioxidant vitamins. On the other hand, recent studies indicated that antioxidant treatments often treat only symptoms but not disease causes, and moreover, the excessive use of antioxidants may lead to adverse outcomes, e.g., development of allergies in children or even increased mortality [46].
When the immune activation process is suppressed by such food compounds, not only the neopterin levels decline, but also tryptophan breakdown ceases. As a consequence, tryptophan levels rise, and its transport into the brain may increase allowing a higher rate of serotonin production. Thus, typical mood food compounds such as antioxidant vitamins and flavonoids and also omega-3 fatty acids are contained in high concentrations in chocolate, berries, and nuts [50–53], but also in beverages like tea, wine, beer, cacao, and coffee [43, 44, 54] which possess the ability to improve tryptophan availability as a source for serotonin production. Consequently, mood might be enhanced after the intake of such beverages. This sequence of events that can be induced by the antioxidants contained in beverages could represent a major aspect why such nutrients possess their mood-enhancing ability and why such beverages became popular for recreation throughout centuries. From the PREDIMED study, it was concluded that moderate consumption of wine may reduce the incidence of depression, while heavy drinkers seem to be at higher risk [55].
For wine and beer, it was demonstrated in vitro that similar effects can be obtained with their alcohol-free analogs. So the alcohol (alone) is not what makes one feel good and maybe even dependent on such beverages; the contained antioxidants appear to be important as well or may be even more important than the alcohol. Ethanol became important to increase the suitability for storage of beverages, and ethanol will contribute to the enhancement of mood solely by increasing the solubility and resorption of compounds in the gut. The potential influence of antioxidant contents in alcoholic beverages to the drinking behavior may also shed some new light on the development of depression during and after alcohol withdrawal, when the decline of antioxidants will abrogate the suppression of immune responses and IDO activity [56]. As a consequence, tryptophan breakdown will increase, and tryptophan and serotonin availability may suffer. Thus, supplementation with tryptophan might help alcoholics under withdrawal to slow down depressive symptoms similar to selective serotonin reuptake inhibitors (SSRI).
Interestingly, smoking, as another widespread lifestyle behavior (although all victims are aware of the eventual negative side effects), can influence tryptophan availability because carbon monoxide (CO) is a potent inhibitor of Th1-type immune response and thus suppresses production of IFN-γ. Enzyme heme oxygenase 1 exerts its anti-inflammatory effects via the release of CO [57], and also in vivo exposure to low to moderate concentrations of CO was found to increase survival expectations in patients with sepsis [58]. Accordingly, among patients with cardiovascular disease, smokers were found to present with lower neopterin levels [59], and also lower tryptophan breakdown rates were observed [60]. So the resulting higher tryptophan levels in smokers may be associated with higher serotonin availability and improve their mood and make them feel better.
Antioxidant Compounds and Obesity
Depressive mood appears to modulate nutrition behavior, and it is thought that the reverse is also true, i.e., that low mood is associated with carbohydrate graving and that carbohydrate intake increases mood by several means. Enhanced serotonin levels appear to represent an important aspect, because the consumption of carbohydrate causes an increase of tryptophan in the plasma and the brain and of serotonin in the brain [61]. Thus, the availability of tryptophan in the blood represents an important aspect for the serotonin supply as does the ratio of tryptophan to branched chained amino acids for the transport of tryptophan into the brain. The higher intake of calories due to carbohydrate craving in situations of low mood may contribute to overeating and weight gain.
After smoking cessation, there is an increased risk for weight gain [62]. Although cardiovascular risks decrease after quitting smoking, body weight often increases in the early period after smoking cessation [63]. In light of the effects of smoking and CO on Th1-type immunity and IDO activity, smoking cessation seems to result in an increase of IDO activity, and as a consequence tryptophan and serotonin availability decreases, which leads to a higher intake of carbohydrates and fat. Because of the intake of such calorie-rich foods, victims will regain weight. However, this represents not the only the mechanistic aspect; several other biochemical pathways relevant for nutrition behavior are affected by antioxidant compounds. This is also particularly true for the adipokine leptin, an important regulator of food intake [64]. In the normal situation, higher leptin levels cause a reduced food intake as a kind of feedback mechanism initialized by fat tissue, in the sense of a saturation signal. The influence of antioxidant compounds, e.g., food preservatives and colorants, was investigated in the in vitro model of the mouse embryonic fibroblast cell line NIH 3 T3, and the compounds were found to significantly suppress the leptin production rate in an inflammatory environment [65]. Thus, the increased intake of food supplemented with antioxidant compounds including antioxidant vitamins could play an important role in the obesity epidemic in the Western world. Also spices contain powerful antioxidant compounds like curcumin, piperine, and capsaicin which were found to exert similar anti-inflammatory effects on NF-κB expression and on pro-inflammatory cytokines [66]. Spices are in use to improve taste of food and these compounds make you feel good. This effect may be again due to their influence on the tryptophan biochemistry, and they are also prone to enhance the amount of food and thus calories to be taken in [67].
Naturally, a lifestyle with less movement and exercise is also an important denominator in the obesity epidemic. The most secure way to ensure human health is to provide individuals the required dosage of nutrients and exercise in a most exact way, never too little and never too much, first expressed by Plato 428–347 bc. Accordingly, overweight and obese individuals are often referred to weight reduction programs which include intake of lower calories per day and to perform exercise [26, 68, 69]. However, the adherence of victims to these programs is often limited, and they may quit before reaching their goals. In a recent study, we observed that low-calorie weight loss diet lowered not only leptin levels, but also levels of essential amino acid tryptophan decreased significantly [70]. The disturbed metabolism of tryptophan might affect biosynthesis of serotonin and could thereby increase the susceptibility for mood disturbances and carbohydrate craving, increasing the cessation probability of weight reduction programs. Supplementation with tryptophan while dieting [71] could be helpful in improving mood status and preventing uncontrolled weight gain or neuropsychiatric symptoms.
Adverse Effects of Antioxidant Compounds
There is accumulating evidence that large-scale supplementation with antioxidant compounds may increase infectious risks when they may counteract the killing strategies of immunocompetent cells. Moreover, in vitro results indicate that the anti-inflammatory property of compounds could shift the Th1–Th2-type immune balance toward Th2-type immunity. Thus, in particular the increasing use of antioxidant food supplements including preservatives and colorants may relate to the increase of allergies in the Western world [46]. Moreover, increased Th2-type immune response was shown to include the risk of weight gain [67] and chronic disease development like diabetes mellitus.
Conclusion
There are manifold influences of antioxidant compounds on the expression and inhibition of biochemical and immunobiological pathways that are widely accepted. Usually, the consequences are considered only in a mono-directed way, when antioxidants are considered promising to combat inflammatory diseases. However, as ever there is nothing beneficial without negative side effects. Their influence on tryptophan biochemistry by slowing down Th1-type immune activation and production of pro-inflammatory cytokines like IFN-γ seems to be of major relevance for influencing mood. A role of tryptophan breakdown in the precipitation of mood disturbances is well acknowledged since the last two decades, when reduced tryptophan availability during inflammatory conditions was found to be associated with mood lowering and precipitating depression. In line with this, treatment with SSRI is well established and helpful at least in half of the patients. Certainly, there are more than just tryptophan metabolic disturbances, which play a role in the pathogenesis of depressive mood and depression, and the dopaminergic and adrenergic/noradrenergic pathway is of major importance. Interestingly enough, also this pathway is hampered by inflammation when ROS and other mechanisms seem to interfere with supply of 5,6,7,8-tetrahydrobiopterin, the necessary cofactor of important monooxygenases in this pathway [72, 73]. Unfortunately, animal models used to mimic what is going on in humans in such diseases are not well representative, because humans and mice differ regarding the potential influence of nitric oxide (NO) to inhibit IDO activity and because human macrophages produce less NO as compared with cells of other species like mice and rats, and thus, IDO plays a greater role in humans than in these animal species [74]. Alternatively, NO biochemistry is more important in murine macrophages than in human cells. As a consequence, any animal model used for studies of tryptophan metabolism is less than perfect to investigate the roles of tryptophan metabolism in human diseases.
Abbreviations
- GCH:
-
GTP cyclohydrolase I
- IDO:
-
Indoleamine 2,3-dioxygenase
- IFN-γ:
-
Interferon-γ
- iNOS:
-
Inducible nitric oxide synthase
- Kyn/Trp:
-
Kynurenine to tryptophan ratio
- NAD:
-
Nicotinamide adenine dinucleotide
- NF-κB:
-
Nuclear factor-κB
- ROS:
-
Reactive oxygen species
- TDO:
-
Tryptophan 2,3-dioxygenase
- TNF:
-
Tumor necrosis factor
References
Chen Y, Guillemin GJ. Kynurenine pathway metabolites in humans: disease and healthy states. Int J Tryptophan Res. 2009;2:1–19.
Widner B, Werner ER, Schennach H, Wachter H, Fuchs D. Simultaneous measurement of serum tryptophan and kynurenine by HPLC. Clin Chem. 1997;43:2424–6.
Werner ER, Bitterlich G, Fuchs D, Hausen A, Reibnegger G, Szabo G, et al. Human macrophages degrade tryptophan upon induction by interferon-gamma. Life Sci. 1987;41:273–80.
Werner-Felmayer G, Werner ER, Fuchs D, Hausen A, Reibnegger G, Wachter H. Tumour necrosis factor-alpha and lipopolysaccharide enhance interferon-induced tryptophan degradation and pteridine synthesis in human cells. Biol Chem Hoppe Seyler. 1989;370:1063–9.
Werner-Felmayer G, Werner ER, Fuchs D, Hausen A, Reibnegger G, Wachter H. Neopterin formation and tryptophan degradation by a human myelomonocytic cell line (THP-1). Cancer Res. 1990;50:2863–7.
Byrne GI, Lehmann LK, Kirschbaum JG, Borden EC, Lee CM, Brown RR. Induction of tryptophan degradation in vitro and in vivo: a gamma-interferon-stimulated activity. J Interferon Res. 1986;64:389–96.
Widner B, Sepp N, Kowald E, Ortner U, Wirleitner B, Fritsch P, et al. Enhanced tryptophan degradation in systemic lupus erythematosus. Immunobiology. 2000;201:621–30.
Weinlich G, Murr C, Richardsen L, Winkler C, Fuchs D. Decreased serum tryptophan concentration predicts poor prognosis in malignant melanoma patients. Dermatology. 2007;214:8–14.
Giusti RM, Maloney EM, Hanchard B, Morgan OSC, Steinberg SM, Wachter H, et al. Differential patterns of serum biomarkers of immune activation in human T-cell lymphotropic virus type I-associated myelopathy/tropical spastic paraparesis and adult T-cell leukemia/ lymphoma. Cancer Epidemiol Biomark Prev. 1996;5:699–709.
Schroecksnadel K, Wirleitner B, Winkler C, Fuchs D. Monitoring tryptophan metabolism in chronic immune activation. Clin Chim Acta. 2006;364:82–90.
Huang A, Fuchs D, Widner B, Glover C, Henderson DC, Allen-Mersh TG. Serum tryptophan decrease correlates with immune activation and impaired quality of life in colorectal cancer. Br J Cancer. 2002;86:1691–6.
Schröcksnadel H, Baier-Bitterlich G, Dapunt O, Wachter H, Fuchs D. Decreased plasma tryptophan in pregnancy. Obstet Gynecol. 1996;88:47–50.
Heyes MP, Saito K, Crowley JS, Davis LE, Demitrack MA, Der M, et al. Quinolinic acid and kynurenine pathway metabolism in inflammatory and non-inflammatory neurological disease. Brain. 1992;115:1249–73.
Theofylaktopoulou D, Ulvik A, Midttun O, Ueland PM, Vollset SE, Nygård O, et al. Vitamins B2 and B6 as determinants of kynurenines and related markers of interferon-γ-mediated immune activation in the community-based Hordaland Health Study. Br J Nutr. 2014;8:1–8.
Fuchs D, Jamnig H, Heininger P, Klieber M, Schroecksnadel S, Fiegl M, et al. Decline of exhaled isoprene in lung cancer patients correlates with immune activation. J Breath Res. 2012;6:027101.
Pfefferkorn ER. Interferon gamma blocks the growth of Toxoplasma gondii in human fibroblasts by inducing the host cells to degrade tryptophan. Proc Natl Acad Sci U S A. 1984;81:908–12.
Werner-Felmayer G, Werner ER, Fuchs D, Hausen A, Reibnegger G, Wachter H. Characteristics of interferon induced tryptophan metabolism in human cells in vitro. Biochim Biophys Acta. 1989;1012:140–7.
Uyttenhove C, Pilotte L, Théate I, Stroobant V, Colau D, Parmentier N, et al. Evidence for a tumoral immune resistance mechanism based on tryptophan degradation by indoleamine 2,3-dioxygenase. Nat Med. 2003;9:1269–74.
Fallarino F, Grohmann U, Vacca C, Bianchi R, Orabona C, Spreca A, et al. T cell apoptosis by tryptophan catabolism. Cell Death Differ. 2002;9:1069–77.
Trabanelli S, Ocadlikova D, Evangelisti C, Parisi S, Curti A. Induction of regulatory T Cells by dendritic cells through indoleamine 2,3-dioxygenase: a potent mechanism of acquired peripheral tolerance. Curr Med Chem. 2011;18:2234–9.
Widner B, Ledochowski M, Fuchs D. Interferon-gamma-induced tryptophan degradation: neuropsychiatric and immunological consequences. Curr Drug Metab. 2000;1:193–204.
Widner B, Laich A, Sperner-Unterweger B, Ledochowski M, Fuchs D. Neopterin production tryptophan degradation and mental depression: what is the link? Brain Behav Immun. 2002;16:590–5.
Capuron L, Dantzer R. Cytokines and depression: the need for a new paradigm. Brain Behav Immun. 2003;17 Suppl 1:S119–24.
Stone TW, Darlington LG. The kynurenine pathway as a therapeutic target in cognitive and neurodegenerative disorders. Br J Pharmacol. 2013;169:1211–27.
Botwinick IC, Pursell L, Yu G, Cooper T, Mann JJ, Chabot JA. A biological basis for depression in pancreatic cancer. HPB (Oxford). 2014;16:740–3.
Allison DJ, Ditor DS. The common inflammatory etiology of depression and cognitive impairment: a therapeutic target. J Neuroinflammation. 2014;11:151.
Capuron L, Neurauter G, Musselman DL, Lawson DH, Nemeroff CB, Fuchs D, et al. Interferon- alpha-induced changes in tryptophan metabolism. Relationship to depression and paroxetine treatment. Biol Psychiatry. 2003;54:906–14.
Capuron L, Schroecksnadel S, Féart C, Aubert A, Higueret D, Barberger-Gateau P, et al. Chronic low grade immune activation in the elderly is associated with increased tryptophan catabolism and altered phenylalanine turnover: role in neuropsychiatric symptomatology. Biol Psychiatry. 2011;70:175–82.
Oxenkrug GF. Metabolic syndrome, age-associated neuroendocrine disorders, and dysregulation of tryptophan-kynurenine metabolism. Ann N Y Acad Sci. 2010;1199:1–14.
Capuron L, Geisler S, Kurz K, Leblhuber F, Sperner-Unterweger B, Fuchs D. Activated immune system and inflammation in healthy ageing: relevance for tryptophan and neopterin metabolism. Curr Pharm Des (in press).
Sublette ME, Galfalvy HC, Fuchs D, Lapidus M, Grunebaum MF, Oquendo MA, et al. Plasma kynurenine levels are elevated in suicide attempters with major depressive disorder. Brain Behav Immun. 2011;25(6):1272–8.
O'Connor JC, Lawson MA, André C, Briley EM, Szegedi SS, Lestage J, et al. Induction of IDO by Bacille Calmette-Guérin is responsible for development of murine depressive-like behavior. J Immunol. 2009;182:3202–12.
Myint AM. Kynurenines: from the perspective of major psychiatric disorders. FEBS J. 2012;279(8):1375–85.
McGee E, Shevlin M. Effect of humor on interpersonal attraction and mate selection. J Psychol. 2009;143:67–77.
Wirleitner B, Reider D, Ebner S, Böck G, Widner B, Jaeger M, et al. Monocyte-derived dendritic cells release neopterin. J Leukoc Biol. 2002;72:1148–53.
Cano OD, Neurauter G, Fuchs D, Shearer GM, Boasso A. Differential effect of type I and type II interferons on neopterin production and amino acid metabolism in human astrocytes-derived cells. Neurosci Lett. 2008;438:22–5.
Schroecksnadel S, Sucher R, Kurz K, Fuchs D, Brandacher G. Influence of immunosuppressive agents on tryptophan degradation and neopterin production in human peripheral blood mononuclear cells. Transplant Immunol. 2011;25:119–23.
Schroecksnadel K, Winkler C, Wirleitner B, Schennach H, Fuchs D. Aspirin down-regulates tryptophan degradation in stimulated human peripheral blood mononuclear cells in vitro. Clin Exp Immunol. 2005;140:41–5.
Neurauter G, Wirleitner B, Laich A, Schennach H, Weiss G, Fuchs D. Atorvastatin suppresses interferon-γ-induced neopterin formation and tryptophan degradation in human peripheral blood mononuclear cells and in monocytic cell lines. Clin Exp Immunol. 2003;131:264–7.
Nathan CF, Murray HW, Wiebe ME, Rubin BY. Identification of interferon-gamma as the lymphokine that activates human macrophage oxidative metabolism and antimicrobial activity. J Exp Med. 1983;158:670–89.
Schreck R, Rieber P, Baeuerle PA. Reactive oxygen intermediates as apparently widely used messengers in the activation of the NF-kappa B transcription factor and HIV-1. EMBO J. 1991;10:2247–58.
Schobersberger W, Hoffmann G, Grote J, Wachter H, Fuchs D. Induction of inducible nitric oxide synthase expression by neopterin in vascular smooth muscle cells. FEBS Lett. 1995;377:461–4.
Jenny M, Klieber M, Zaknun D, Schroecksnadel S, Kurz K, Ledochowski M, et al. In vitro testing for anti-inflammatory properties of compounds employing peripheral blood mononuclear cells freshly isolated from healthy donors. Inflamm Res. 2011;60:127–35.
Gostner J, Ciardi C, Becker K, Fuchs D, Sucher R. Immunoregulatory impact of food antioxidants. Curr Pharm Des. 2014;20:840–9.
Gostner JM, Schroecknsadel S, Jenny M, Klein A, Ueberall F, Schennach H, et al. Coffee extracts suppress tryptophan breakdown in mitogen-stimulated peripheral blood mononuclear cells. J Am Coll Nutr (in press).
Zaknun D, Schroecksnadel S, Kurz K, Fuchs D. Potential role of antioxidant food supplements, preservatives and colorants in the pathogenesis of allergy and asthma. Int Arch Allergy Immunol. 2012;157:113–24.
Winkler C, Schroecksnadel K, Schennach H, Fuchs D. Vitamin C and E suppress mitogen-stimulated peripheral blood mononuclear cells in vitro. Int Arch Allergy Immunol. 2007;142:127–32.
Tan PH, Sagoo P, Chan C, Yates JB, Campbell J, Beutelspacher SC, et al. Inhibition of NF-kappa B and oxidative pathways in human dendritic cells by antioxidative vitamins generates regulatory T cells. J Immunol. 2005;174:7633–44.
Murr C, Winklhofer-Roob BM, Schroecksnadel K, Maritschnegg M, Mangge H, Böhm BO, et al. Inverse association between serum concentrations of neopterin and antioxidants in patients with and without angiographic coronary artery disease. Atherosclerosis. 2009;202:543–9.
Hulsken S, Märtin A, Mohajeri MH, Homberg JR. Food-derived serotonergic modulators: effects on mood and cognition. Nutr Res Rev. 2013;26:223–34.
Gómez-Pinilla F. Brain foods: the effects of nutrients on brain function. Nat Rev Neurosci. 2008;9:568–78.
Grosso G, Galvano F, Marventano S, Malaguarnera M, Bucolo C, Drago F, et al. Omega-3 fatty acids and depression: scientific evidence and biological mechanisms. Oxidative Med Cell Longev. 2014;2014:313570.
Sánchez-Villegas A, Martínez-González MA, Estruch R, Salas-Salvadó J, Corella D, Covas MI, et al. Mediterranean dietary pattern and depression: the PREDIMED randomized trial. BMC Med. 2013;11:208.
Jenny M, Santer E, Klein A, Ledochowski M, Schennach H, Ueberall F, et al. Cacao extracts suppress tryptophan degradation of mitogen-stimulated peripheral blood mononuclear cells. J Ethnopharmacol. 2009;207:75–82.
Gea A, Beunza JJ, Estruch R, Sánchez-Villegas A, Salas-Salvadó J, Buil-Cosiales P, et al. Alcohol intake, wine consumption and the development of depression: the PREDIMED study. BMC Med. 2013;11:192.
Gleissenthall GV, Geisler S, Malik P, Kemmler G, Benicke H, Fuchs D, et al. Tryptophan metabolism in post-withdrawal alcohol-dependent patients. Alcohol Alcohol. 2014;49:251–5.
Mougiakakos D, Jitschin R, Johansson CC, Okita R, Kiessling R, Le Blanc K. The impact of inflammatory licensing on heme oxygenase-1-mediated induction of regulatory T cells by human mesenchymal stem cells. Blood. 2011;117:4826–35.
Ryter SW, Choi AM. Heme oxygenase-1/carbon monoxide: novel therapeutic strategies in critical care medicine. Curr Drug Targets. 2010;11:1485–94.
Walter RB, Fuchs D, Weiss G, Walter TR, Reinhard WH. HMG-CoA reductase inhibitors are associated with decreased serum neopterin levels in stable coronary artery disease. Clin Chem Lab Med. 2003;41:1314–19.
Pedersen ER, Midttun Ø, Ueland PM, Schartum-Hansen H, Seifert R, Igland J, et al. Systemic markers of interferon-g-mediated immune activation and long-term prognosis in 2380 patients with stable coronary artery disease. Arterioscler Thromb Vasc Biol. 2011;31:698–704.
Fernstrom JD, Wurtman RJ. Brain serotonin content: increase following ingestion of carbohydrate diet. Science. 1971;174:1023–5.
Liverant GI, Sloan DM, Pizzagalli DA, Harte CB, Kamholz BW, Rosebrock LE, et al. Associations among smoking, anhedonia, and reward learning in depression. Behav Ther. 2014;45:651–63.
Komiyama M, Wada H, Ura S, Yamakage H, Satoh-Asahara N, Shimatsu A, et al. Analysis of factors that determine weight gain during smoking cessation therapy. PLoS One. 2013;8(8), e72010.
Farr OM, Tsoukas MA, Mantzoros CS. Leptin and the brain: influences on brain development, cognitive functioning and psychiatric disorders. Metabolism. 2014, pii: S0026-0495(14)00199-1.
Ciardi C, Jenny M, Tschoner A, Überall F, Patsch J, Pedrini M, et al. Food additives sodium sulfite, sodium benzoate and curcumin inhibit leptin release in lipopolysaccharide-treated murine adipocytes in vitro. Br J Nutr. 2012;107:826–33.
Aggarwal BB, Shishodia S. Suppression of the nuclear factor-kappaB activation pathway by spice-derived phytochemicals: reasoning for seasoning. Ann N Y Acad Sci. 2004;1030:434–41.
Mangge H, Summers KL, Meinitzer A, Zelzer S, Almer G, Prassl R, et al. Obesity-related dysregulation of the tryptophan-kynurenine metabolism: role of age and parameters of the metabolic syndrome. Obesity (Silver Spring). 2014;22:195–201.
Lee H, Ohno M, Ohta S, Mikami T. Regular moderate or intense exercise prevents depression-like behavior without change of hippocampal tryptophan content in chronically tryptophan-deficient and stressed mice. PLoS One. 2013;8, e66996.
Melancon MO, Lorrain D, Dionne IJ. Changes in markers of brain serotonin activity in response to chronic exercise in senior men. Appl Physiol Nutr Metab. 2014;23:1–7.
Strasser B, Berger K, Fuchs D. Effects of a caloric restriction weight loss diet on tryptophan metabolism and inflammatory biomarkers in overweight adults. Eur J Nutr (in press).
Steinert RE, Luscombe-Marsh ND, Little TJ, Standfield S, Otto B, Horowitz M, et al. Effects of intraduodenal infusion of l-tryptophan on ad libitum eating, antropyloroduodenal motility, glycemia, insulinemia, and gut peptide secretion in healthy men. J Clin Endocrinol Metab. 2014;99:3275–84.
Neurauter G, Schröcksnadel K, Scholl-Bürgi S, Sperner-Unterweger B, Schubert C, Ledochowski M, et al. Chronic immune stimulation correlates with reduced phenylalanine turn-over. Curr Drug Metab. 2008;9:622–7.
Haroon E, Raison CL, Miller AH. Psychoneuroimmunology meets neuropsychopharmacology: translational implications of the impact of inflammation on behavior. Neuropsychopharmacology. 2012;37:137–62.
Fuchs D, Murr C, Reibnegger G, Weiss G, Werner ER, Werner-Felmayer G, et al. Nitric oxide synthase and antimicrobial armature of human macrophages. J Infect Dis. 1994;169:224.
Acknowledgments
There are no conflicts of interest and no financial interests.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Gostner, J.M., Becker, K., Sperner-Unterweger, B., Überall, F., Fuchs, D., Strasser, B. (2015). Role of Tryptophan Metabolism in Mood, Behavior, and Cognition. In: Mittal, S. (eds) Targeting the Broadly Pathogenic Kynurenine Pathway. Springer, Cham. https://doi.org/10.1007/978-3-319-11870-3_6
Download citation
DOI: https://doi.org/10.1007/978-3-319-11870-3_6
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-11869-7
Online ISBN: 978-3-319-11870-3
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)