
Abstract
The airway acts as a conduit to bridge the environment with the gas exchange site. Flow of air under involuntary control occurs to bring oxygen to the gas exchange site and carbon dioxide produced in the body out to the environment. This flow is possible with the process of breathing through a patent airway. Patency of the airway is maintained with tonic control of pharyngeal muscles, constant mucus production with mucociliary clearance and occasional sneezing and coughing. The work done in sustaining this flow regularly is minimal at only less than 3 % of total body energy consumption but can increase substantially with airway obstruction or in the presence of poor compliance of the lung. Depending on the site of airway obstruction, manoeuvres to reduce the obstruction include the use of Heimlich’s, suctioning and use of bronchodilators.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
Introduction
The airway is the conduit that links the outside environment to the gas exchange site. This conduit allows oxygen to be brought in and carbon dioxide to be brought out. The process is by bulk flow [1] which allows the transfer of adequate volumes to keep up with the needs of the body. In order for this flow to be maintained, the airway must be kept patent.
Patency is maintained by tonic control of pharyngeal muscles, mucus production, mucociliary clearance, sneezing and coughing.
Flow in the airway is involuntarily controlled by the autonomic nervous system [2]. The process is complex and loss of control can occur due to a variety of reasons including obstruction and inability to create the sub-atmospheric conditions [3] necessary for the movement of air. The latter includes interruption of neuronal control, weakness of the respiratory muscles, pain and loss of consciousness.
Flow in the Airway
The airway serves as the only conduit to allow transfer of oxygen and carbon dioxide between the environment and the gas exchange site.
The flow in the airway is intermittent with the flow inwards during inspiration and outwards during expiration. With each breath, the flow averages 25–30 L/min but since each breath is only slightly over a second, about 0.5 L or 500 ml flow into the gas exchange area with the breath.
In normal low flow breathing, the flow rate is slightly higher during inspiration than expiration at 25 L/min. At peak inspiratory and expiratory flow rates, the expiratory flow can become as high [4] as 280 L/min whilst the inspiratory flow rate 160 L/min. This increased flow is especially useful during exercise [5] to bring in the very much larger volumes of oxygen needed for the efficient conversion of energy sources to ATPs needed for activity in the muscles. The oxygen needs during these periods of time can be up to 10–20 times the basal metabolic requirement of oxygen.
This flow to bring oxygen to the gas exchange site is mandatory to sustain life. Interruption to this flow may be due to a variety of causes, chief of which is obstruction in the airway. Obstruction in the upper airways depending on the cause of the obstruction can be circumvented by providing a passage below the obstruction. Obstruction in the lower airways must be assisted by bronchodilatation, removal of secretions with positional drainage or assistance with chest physiotherapy. If circumvention below the site of obstruction is not an option, cardiopulmonary bypass to bring oxygen directly into the cardiovascular system which then brings it to the tissues, can be a temporary alternative strategy.
Flow is delineated by the Hagen Poiseuille’s relation:
- Q:
-
flow
- P:
-
driving pressure
- r:
-
radius of conduit
- η:
-
viscosity of gas
- l:
-
length of conduit
Whilst the flow in the main distributing part of the airway may be turbulent, this formula helps in understanding some of the clinical applications we use to overcome obstruction in the airway.
Partial obstruction can be circumvented by increasing the pressure of the gas delivered inwards to increase flow. This is widely used in continuous positive air pressure (CPAP) ventilation and bi-level positive airway pressure (BiPAP) ventilation [6]. Similarly flow can be increased by decreasing the viscosity of the gas used to carry the oxygen inwards. Instead of using air which is an oxygen nitrogen mixture, oxygen is used with helium. The latter has a lower density and hence viscosity. This would improve flow in the conduit when used as a carrier gas [7–9].
Inability to create the negative pressure to induce flow can be due to weakness of the muscles either the muscles of the diaphragm or of the intercostals. Paralysis of the nerves supplying the muscles may also be responsible for the dysfunction.
Flow in an Obstructed Airway
Airway obstruction can occur anywhere along the length of the airway. Management strategies differ when managing obstruction in the upper as opposed to the lower airway. In order to distinguish the site of the obstruction, the flow volume loop examinations of patients are useful in assessment [10, 11].
Upper Airway Obstruction
The upper airway is that part of the airway until the level of the carina. The upper airway can be divided into the extrathoracic and the intrathoracic airway. The diameter of the airway is sensitive to the transmural pressure on it and changes during the phase of respiration.
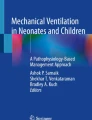
For the extrathoracic airway [10] (Fig. 1.1), the extrinsic pressure on it is related to the unchanging atmospheric pressure. During inspiration in those who are obstructed, the negative pressure in the airway tends to collapse the airway resulting in reduced flow. During expiration, the positive pressure allows the airway to stay fully patent and there is no reduction in flow.

Extrathoracic airway obstruction. Note the reduced flow (dashed black lines) during inspiration whilst the flow remains unchanged from normal during expiration
For the intrathoracic airway [10] however, the negative intrapleural pressure during inspiration ensures that it stays patent with no diminution in flow during inspiration. The positive intrapleural pressure during expiration may collapse the airway in those who are obstructed causing the expiratory flow to be reduced (Fig. 1.2).

Intrathoracic airway obstruction. Note that the flow (dashed black lines) is normal during inspiration but reduced during expiration when the airway collapses from the positive intrapleural pressure
When the obstruction is fixed [10] (Fig. 1.3), i.e. when there is no change in diameter of the airway during both phases of respiration, limitations of flow will occur during both inspiration and expiration.

Fixed airway obstruction. Note the decrease in flow (dashed black lines) both during inspiration and expiration
Lower Airway Obstruction
In patients with airway obstruction in the peripheral airways, restriction of flow occurs during the terminal volume of the expiration (Fig. 1.4). In asthma and chronic obstructive pulmonary disease (COPD) the reduced expiratory flow results in air trapping producing an auto-positive end expiratory pressure (auto-PEEP) which in the COPD patients give rise to the barrel chests often seen in them.

Peripheral airway obstruction. Note the flow (dashed black lines) is reduced in the terminal phase of expiration
In smaller airway obstruction, the distribution [12] of the inspired flow is also affected. The gases in the periphery will move away from the obstructed sites and move through unblocked collateral channels to the gas exchange site. Smaller airway obstruction can be picked up by the single breath nitrogen washout test following an inspiratory breath of 100 % oxygen. In a patient with peripheral obstruction, the alveolar plateau (phase lll of the curve) will no longer be flat but will show a rising nitrogen concentration (Fig. 1.5).

Following a single inspiratory breath of 100 % oxygen, the nitrogen washout concentration of a normal person can be divided into several phases reflecting the distribution of the oxygen previously inspired. Note the non plateau nature of phase lll in those with COPD
Distribution of the Airflow in the Lung and Gas Exchange Area
A greater proportion of the flow is distributed to the lower lungs in the upright position. The alveoli in the bottom portion of the lung are at the ascending or near ascending portion (has high compliance) of the lung compliance curve. The alveoli at the upper end are already fully inflated (has low compliance) or are nearly fully inflated and cannot distend anymore (Fig. 1.6).

The alveoli at the bottom portion of the lung has high compliance and those at the top have low compliance
Flow Velocity
As we move from the larger airways to the more distal part, the total cross-sectional area of the smaller airways increases. Flow stays constant but the linear flow velocity decreases as we move further downstream. The linear flow velocity is the flow divided by the total cross sectional area of a given generation of airway.
Turbulent and Laminar Flow
The linear flow velocity, being larger in the larger airways, causes the flow there to be turbulent. In the smaller airway as the flow velocity decreases, the flow tends to become laminar (Fig. 1.7).

The type of flow present in the airways
Pressures in the Airway: Spontaneous Respiration and Controlled Respiration
Inspiratory or expiratory flow is induced by difference in pressure between bronchus/bronchioles and the environment. In a spontaneously breathing person, the negative pressure at the start of inspiration is due to increasing negative pressure in the pleural cavity being induced by the descent of the diaphragm and the outward movement of the thoracic chest wall.
The pressure changes during spontaneous respiration in the airway averages around +2 mmHg during expiration and −2 mmHg during inspiration. In controlled respiration, the airway pressure during inspiration may average around 15–20 mmHg and move onto 0 mmHg during expiration.
Work of Breathing
Work done to induce flow during inspiration is for overcoming the elastic forces and to overcome resistance in the airway (Fig. 1.8a and d). The energy of the work done to overcome elastic forces is stored in the lung tissues as potential energy for the subsequent expiration.

The representation of the amount of work done for inspiration and expiration in a a normal patient, b chronic obstructive pulmonary disease, c a patient with restrictive disease. The key d outlines the nature of the work for the various phases of respiration. Note the intrapleural pressures represent increasingly negative values in the direction of the arrows
The expiratory work to allow flow of air to move from the gas exchange site to the outside environment is only to accommodate forces due to airway resistance and it comes from the potential energy stored with inspiration. With this arrangement, inspiration is active and expiration passive.
In the presence of airway obstruction (Fig. 1.8b), the patient needs to do more work during inspiration to generate a higher differential pressure to overcome the obstruction. This is done by a more forceful generation of increasing negative pressure in the airways when a patient is breathing spontaneously. This generation of a more negative intrathoracic pressure may predispose an unconscious patient (without protective airway reflexes) in a partially obstructed airway situation to aspiration. The intraabdominal pressure may be very much higher than the intrathoracic pressure facilitating the movement of stomach contents into the oesophagus.
In patients with restrictive disease (Fig. 1.8c) however more work is done to overcome the elastic forces in the lungs while the work against resistance remains the same. As the lung is very compliant in a normal patient, the work done does not consume a lot of the body’s energy needs and the amount of daily energy expended is less than 3 % of total body energy requirement [13].
Keeping the Airway Clear
Mucous Production and Clearance in the Airway
With volumes of about 300–400 L/h of air, flowing into the lungs, many unwanted particles can be brought in. Mucous forms the first line of defence to trap [14] microbes, dust and other particles brought in during inhalation before they can go further into the gas exchange site. Mucous also prevents the airway from getting dehydrated [14].
Mucous [14] is a collection of polypeptides, cells and cellular debris bound together by mucin. The latter is made of glycoproteins with glycosylated carbohydrates. Mucins [14] can be either membrane bound for functions of cellular adhesion and pathogen binding or secreted to provide the viscoelastic properties of mucous.
Mucous hypersecretion [14, 15] however causes mucociliary impairment leading to airway obstruction which can then lead to limitation of airflow.
Mucociliary Clearance
Ciliary action is the first line of defence in moving the mucus in the airway. This is especially so in the more distal generation of airways where cough is not a predominant feature in clearance of the airway.
Mucociliary clearance is impaired in the elderly [16]. This may explain why they are more vulnerable and have an increased likelihood of developing lower respiratory tract infection.
Cough
Cough [17] is an extremely important defense mechanism in the airway to keep it clean and healthy. As previously mentioned, normal expiration is a passive process where the airway pressure is not high enough to generate a high enough expiratory flow to remove substances brought in by inspiration. A productive cough can do exactly that.
Cough [18] starts with a deep inspiration usually up to the total lung capacity (inspiratory phase), followed by a closure of the glottis to bring the pressure up to 50 cm H2O [19] (compressive phase) and then an explosive phase where the flow is many times higher than the normal expiratory flow to facilitate removal of the substance collected in the airway.
In the normal patient, it is the expectoration of mucus that is the main function of a cough [19]. The high velocity flow generated is higher in the central airways (decreased total cross sectional area) than in the periphery. A cough therefore impacts mucus secretion in the proximal airways up to the 7 to 12th generation of airways [19].
The high flow generated in an effective cough breaks the mucus free of the epithelial lining of the airway and brings it into the main air stream to be brought out to the exterior. Thick and tenacious mucus however may need an extremely high flow to do this and explains why they are more likely to be difficult to remove [20].
As the first phase of cough requires the generation of a large inspired volume almost to the total lung volume, patients with muscle weakness are unable to produce effective cough. These patients may have a higher risk of developing atelectasis, post operative pneumonia and onward to respiratory inadequacy [19].
Sneezing
Sneezing like a cough, is another protective airway reflex that allows the creation of a high airway pressure during expiration [21] with the generation of a high flow [22] to remove airway irritants.
A sneeze starts with the activation of afferent nerve endings of the trigeminal nerve in the nasal mucosa and areas around the conjunctiva, cornea, oral mucosa and face [23]. Nerve impulses are transmitted to the sneezing centre in the lateral part of the medulla [24] via the trigeminal ganglion [25].
As in a cough, a sneeze in the efferent limb [21] starts with a deep inspiration followed by an initial closed glottis so that a high pressure up to about 176 mmHg [26] can be generated to expel foreign irritants in the airway through the open mouth and a closed nostril.
Airway Closure
Airway closure is usually linked to the lung capacity existing at the time where there is no longer air flow from the gas exchange site. In the normal patient, airway closure [27] is below normal tidal volume range of respiration or within the functional residual capacity volume. Lungs which are functioning at this range of capacity for air closure are working optimally. There is no work wasted to inflate the closed alveoli where there is need to recruit alveoli to make up the tidal volume.
For those patients who are obese and for those who are elderly (especially when they lie flat) airway closure occurs within the normal tidal range or above the functional residual capacity [28]. In these patients, the work of breathing is increased especially when they are in the supine position as wasted work is needed to open up the alveoli with each tidal breath.
Surfactant and Airway Closure
Surfactant which is produced by the type II epithelial cells [29] reduces the surface tension. A reduced surface tension reduces the pressure inside the alveolus and prevents it from emptying its contents into an adjacent alveolus with lower airway pressure. Surfactant prevents the alveoli from collapsing during expiration.
Surfactant [30] stabilises the alveoli and prevents early airway closure. This therefore reduces the work of breathing as it pre-empts the need to work on opening the collapsed alveoli.
Artificial Control of the Activities in the Airway
In the awake and conscious patient, the process of breathing creates the flow in the airway and this is an involuntary process [2] under the control of the respiratory centre. As this flow is so efficiently carried out and the energy requirement is so minimal, it is not a burden to life. However when there is increased work of breathing, the patient becomes conscious of the burden of the work.
In the unconscious patient, the control of the flow in the airway may be lost. The ability to conduct the other protective activities to keep the airway healthy is similarly lost. Care providers have to assume these two roles in managing the airway in order to sustain life.
Role of the Heimlich Manoeuvre
In a patient who has aspirated a foreign body, it is usual for providers at the scene to try to remove the foreign body to assist respiration. The choking algorithm is well described in most resuscitation manuals [31] but often the care provider is unable to remember the proper sequence of events required for the proper handling of this potential life threat.
When caught in such a situation [32], it is important to determine if the patient is able to cough or speak in complete sentences. Ability to do so indicate the foreign body is not causing a life threatening airway obstruction. Attempts to remove foreign bodies especially a coin with inadequate back up facilities can transform a non life threatening obstruction to a complete obstruction. A patient who is still able to control his airway demonstrated by his ability to cough or speak, should be monitored closely for his adequacy of respiratory effort until adequate facilities/expert help is available in the hospital setting.
If he is unable to cough [31], then the need to remove the foreign body becomes more urgent. If he is still conscious, one can use the Heimlich manoeuvre which requires the rescuer (standing at the back of the patient) to lock both his hands anterior to the abdomen of the patient and apply an upward thrust at the diaphragm to increase the intrathoracic pressure in an attempt to dislodge the foreign body with the raised intrathoracic pressure.
If the patient is unconscious however, the same manoeuvre is done straddling the unconscious patient [32] who is placed supine on the floor and applying the upward diaphragmatic thrust from the front. After the foreign body is dislodged, it is manually removed and respiration and cardiac massage applied if cardiopulmonary arrest has ensued as a result of the obstruction.
Role of Suctioning of Secretions from the Airway
Sucking of secretions to clear the airway is an important activity undertaken in the critical care of ill patients. The practice varies widely in terms of what is actually being practised [33]. It has to be done under sterile conditions to assist those who are unable to expectorate their secretions.
The most common complication that can accrue from improper suctioning is hypoxemia [34–36]. This can be prevented by preoxygenation, hyperoxygenation and hyperinflation, suctioning for less than 15 s using pressures of −80 to −120 mmHg and limiting the size of the suction catheter to 14 Gauge or less. Careful suctioning reduces damage to the tracheal mucosa [35].
Role of Bronchodilators
Bronchoconstriction in the peripheral airways is best managed with bronchodilators that act on the smooth muscles in the distal airways responsible for the problem. Newer focus has been on 2 different agents [37, 38] to provide synergistic effects of bronchodilatation. They include long acting muscarinic antagonists (LAMA) e.g. Tiotropium, Glycopyrronium and long acting beta agonists (LABA) e.g. Formoterol, Indacaterol.
Common Diseases of the Airway
Asthma and Chronic Obstructive Pulmonary Disease (COPD) constitute the 2 most common airway diseases affecting mainly the peripheral airways. Asthma burdens 300 million people world-wide [39] whilst COPD causes 4–5 % of adult mortality [40]. The main thrust of management is to keep the peripheral airway obstruction under control so that the affected patients can have adequate flow in the airway and keep up with their usual activities of daily living.
Asthma
Whilst most of us understand asthma as a condition with intermittent, reversible high peripheral airway resistance, it is also a disease characterised by tidal volume airway closure [28] where the closing volume is higher than the end expiratory lung volume. This is as a result of inflammation in the peripheral airway mainly associated with airway eosinophilia [41]. Markers of inflammation including exhaled nitric oxide may be of some use to determine the extent of the disease [42, 43] to allow more effective control of bronchodilatation management.
Chronic Obstructive Airway Disease
This is a disease characterised by airflow limitations [40] with acute exacerbations from respiratory infections where peripheral airway obstruction together with parenchyma destruction cause respiratory dysfunction increasing with age. Many have mucous hypersecretions [44] which are difficult to control. Acute exacerbations [45] is best managed with a combination of bronchodilators, corticosteroids and antibiotics together with non-invasive positive pressure ventilation to tide over the period of increased work of breathing.
Conclusion
The airway is a conduit that links the environment with the gas exchange site. Flow is sustained by the process of breathing and can be done with ease when the airway is patent. Patency is maintained by many physiological processes including mucous production and clearance, sneezing and coughing. In addition as providers we may facilitate by suctioning of the proximal airway and use bronchodilators to improve patency of the peripheral airway. In a patient with choking the process of correctly applying the choking algorithm is important in order for the patient to survive.
Understanding the physiological concepts surrounding flow in the airway is certainly an important step in providing appropriate care during the crucial stages of sustaining life. Asthma and COPD are two very common airway diseases that affect a fair segment of the population and pharmacological means to maintain patency of the airway remain the mainstay of management.
References
Muir DCF (1966) Bulk flow and diffusion in the airways of the lung. Br J Dis Chest 60(4):169–176
Taylor EW, Jordan D (1999) Coote JH Central control of the cardiovascular and respiratory systems and their interactions in vertebrates. Physiol Rev 70(3):855–916
Vassilakopoulos T, Sakynthinos S, Roussos C (1996) Respiratory muscles and weaning failure. Eur Respir J 9:2383–2400
Viani L, Jones AS (1990) ClarkeR Nasal airflow in inspiration and expiration. J Laryngol Otol 104:473–476
Burton DA, Stokes K, Hall GM (2004) Physiological effects of exercise BJA 4(6):185–188
Putensen C, Wrigge H (2004) Clinical review: biphasic positive airway pressure and airway pressure release ventilation. Crit Care 8(6):492–497
McGee DL, Wald DA, Hinchliffe S (1997) Helium–oxygen therapy in the emergency department J Emerg Med 15(3):291–68
L’Her E, Renault A, Mouline J, Garo B (1997) Boles JM Use of helium–oxygen gas mixtures in a acute obstructive respiratory insufficiencies. Reve Pneumol Clin 53(4):177–184
Jaber S, Fodil R, Carlucci A, Boussarsar M, Pigeot J, Lemaire F et al (2000) Noninvasive ventilation with helium-oxygen in acute exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med 161:1191–1200
Brookes GB, Fairfax AJ (1982) Chronic upper airway obstruction: value of the flow volume loop examination in assessment and management. J R Soc Med 75:425–434
Kapteijns EF, Kwakkel-van Erp JM, Vos PU, van den Elshout FJ (2006) Dyspnoea caused by upper airway obstruction: simple diagnosis by establishing a flow-volume loop. Ned Tijdschr Geneeskd 150(18):993–998
Macklem PT (1998) The physiology of small airways. Am J Respir Care Med 157:S181–S183
Kress JP, Pohlman AS, Alverdy J, Hall JB (1999) The impact of morbid obesity on oxygen cost of breathing at rest. Am J Respir Crit Care Med 160:883–886
Williams OW, Sharafkhaneh A, Kim V, Dickey BF, Evans CM (2006) Airway mucus. Am J of Respir Cell Mol Biol 34(5):527–536
Roger DF (2007) Physiology of airway mucus secretion and pathophysiology of hypersecretion. Respir Care 52(9):1134–1146
Ho JC, Chan KN, Hu WH et al (2001) The effect of aging on nasal mucociliary clearance, beat frequency and ultrastructure of respiratory cilia. J Respir Crit Care Med. 163:983–988
Chang AB (2006) The physiology of cough. Paediatr Respir Rev 7(1): 2–8
Shah MD, Shah SM (2001) The applied physiology of cough. Indian J Pediatr 68(Suppl 2):S3–S10
McCool FD (2006) Global physiology and pathophysiology of cough: ACCP evidence—based clinical practice guidelines. Chest 129(Suppl 1):48S–53S
McCool FD (1987) Leith DE Pathophysiology of cough. Clin Chest Med 8(2):189–195
Batsel HL, Lines AJ (1975) Neural mechanisms of sneeze. Am J Physiol 229:770–776
Nishino T (2000) Physiological and pathophysiological implications of upper airway reflexes in humans. Jpn J Physiol 50:3–14
Widdicombe JG (1990) Nasal pathophysiology. Resp Med 84(Suppl A):3–9
Suranyi L (2001) Localization of the sneeze center. Neurology 57:161
Wallios F, Macron JM, Jounieaux V, Duron B (1991) Trigeminal afferents implied in the triggering or inhibition of sneezing in cats. Neurosci Lett 122:145–147
Gwaltney JM Jr, Hendley JO, Phillips CD, Bass CR, Mygind N, Winther B (2000) Nose blowing propels nasal fluid into the paranasal sinuses. Clin Infect Dis. 30:387–391
Pelosi P, Rocco PRM (2007) Airway closure: the silent killer of peripheral airways. Crit Care 11(1):114
Milic-Emili J, Torchio R, D’Angelo E (2007) Closing volume: a reappraisal (1967–2007). Eur J Appl Physiol 99(6):567–583
Otis DR Jr, Johnson M, Pedley TJ, Kamm RD (1993) Role of surfactant in airway closure: a computational study. J Appl Physiol 75(3):1323–1333
Hills BA (1981) What is the true role of surfactant in the lung? Thorax 36:1–4
Berg RA, Hemphill R, Abella BS, Aufderheide TP, Tom P, Cave DM et al (2010) Part 5: Adult Basic Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 122(Suppl 3):S685–S705
Chan YK (2012) Physiology of the airway. In: Chan YK, Kwee Peng Ng (eds) Physiological basis of acute Care. Saunders Elsevier Singapore pp 19–27
Sole ML, Byers JF, Ludy JE, Zhang Y, Banta CM, Brummel K (2003) A multisite survey of suctioning techniques and airway management practices Am J Crit Care 12:220–230
Oh H, Seo W (2003) A meta-analysis of the effects of various interventions in preventing endotracheal suction induced hypoxemia. J Clin Nurs 12:912–924
Brodsky L, Reidy M, Stanievich JF (1987) The effects of suctioning techniques on the distal tracheal mucosa in intubated low birth weight infants. Int J Pediatri Otorhinolaryngol 14:1–14
Kerem E, Yatsiv I, Goitein KJ (1990) Effect of endotracheal suctioning on arterial blood gases in children. Intensive Care Med 16(2):95–99
Cazzola M, Matera MG (2009) Emerging inhaled bronchodilators: an update. Eur Respir J 34:757–769
Tashkin DP, Ferguson GT (2013) Combination bronchodilator therapy in the management of chronic obstructive pulmonary disease. Available from http://respiratory-research.com/content/14/1/49. Accessed 4th September 2013
Braman SS (2006) The global burden of asthma Chest 130(1 Suppl):4S–12S
Mannino DM, Buist AS (2007) Global burden of COPD: risk factors, prevalence, and future trends. Lancet 370:765–773
Payne DNR, Adcock IM, Wilson NM, Oates T, Scallan M (2001) Bush A. Relationship between exhaled nitric oxide and mucosal eosinophilic inflammation in children with difficult asthma, after treatment with oral prednisolone Am J Respir Crit Care Med 164:1376–1381
Wedes SH, Khatri SB, Zhang R, Wu W, Comhair SA, Wenzel S et al (2009) Noninvasive markers of airway inflammation in asthma. Clin Transl Sc 2(2):112–117
Pan Y, Huang KW, Ye Q, Liu XS, Wu BM, Zhang J et al (2009) Airway inflammation and peripheral airway function in asthmatic patients with different control levels. Zhonghua Jie He He Hu Xi Za Zhi 32(9):679–684
Rogers DF (2005) The role of airway secretions in COPD: pathophysiology, epidemiology and pharmacotherapeutic options. COPD 2(3):341–353
McCrory DC, Brown C, Gelfand SE, Bach PB (2001) Management of acute exacerbations of COPD: a summary and appraisal of published evidence. Chest 119:1190–1209
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Chan, Y.K. (2014). Physiology of the Airway. In: Khan, Z. (eds) Airway Management. Springer, Cham. https://doi.org/10.1007/978-3-319-08578-4_1
Download citation
DOI: https://doi.org/10.1007/978-3-319-08578-4_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-08577-7
Online ISBN: 978-3-319-08578-4
eBook Packages: MedicineMedicine (R0)