
Abstract
The epithelial cells of prostate tissue produce a protein known as prostate-specific antigen (PSA), whose function is to liquefy the ejaculated semen and convert it into an adequate medium in which the sperm can move freely. It is also believed that another of its tasks is to dissolve the vaginal and cervical mucus in order to facilitate the entry of the sperm, allowing them to reach their destination. It is a protein substance that initially was discovered in the seminal fluid; it has now also been found in other tissues such as pancreas and breast tissue, though in minimal quantities.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
-
PSA analysis
-
Elevated PSA
-
Total PSA compared to free PSA
-
Future tumor markers for prostate cancer
The epithelial cells of prostate tissue produce a protein known as prostate-specific antigen (PSA), whose function is to liquefy the ejaculated semen and convert it into an adequate medium in which the sperm can move freely. It is also believed that another of its tasks is to dissolve the vaginal and cervical mucus in order to facilitate the entry of the sperm, allowing them to reach their destination. It is a protein substance that initially was discovered in the seminal fluid; it has now also been found in other tissues such as pancreas and breast tissue, though in minimal quantities.
The prostate-specific antigen is produced in the prostate and circulates in the blood throughout the whole body. The amount circulating in the blood can increase for different reasons, among which are: prostate cancer, the benign growth of the gland (relating to aging), and certain infectious processes that affect the prostate (Fig. 3.1).

PSA test
The prostate-specific antigen was discovered in 1979, but its clinical utility was not identified until a decade later. Until this was known, urologists used only the digital rectal examination and a few indirect blood tests, such as the prostatic acid phosphatase, when prostate cancer was suspected. Today, the PSA is the tumor marker most widely used in contemporary medicine, and along with the digital rectal examination and transrectal prostate ultrasound, it’s the best means of identifying patients with a high risk of suffering from prostate cancer, especially in the early stages when the possibilities of cure are greatest (Fig. 3.2).

Men older than 50
In developed countries, it is estimated that three out of every four men older than 50 have had a PSA study at some point, which has made it possible to diagnose and treat patients with prostate cancer in early stages and thereby diminish mortality from prostate cancer.
FormalPara FactTumor markers are those substances that can be detected in blood, urine, or tissues, and whose presence in a higher than normal concentration can indicate the existence of a cancerous tumor. Although that abnormal concentration may suggest the presence of cancer, it is not itself sufficient to diagnose it, and for this reason its utility is reduced to providing a clue for diagnosis or for evaluating the evolution of a tumor already detected by other procedures. Most tumor markers can also be produced by normal cells and thereby give false positives. Likewise, some non-cancerous diseases can cause the levels of certain markers to rise.
PSA Analysis
We already know that PSA can be produced either by a benign prostate cell or from a cancerous prostate cell. For this reason it is very important to know how to interpret the presence and the characteristics of the antigen detected in the blood. Because of this, and due to the fact that up to 25 % of all cancers do not alter the PSA concentration, it is important to distinguish between the behavior of this substance in cancer and its behavior in other benign diseases of the prostate.
The results of the PSA analyses indicate its concentration in the blood. It is not necessary to fast before the laboratory test. The results are generally reported in nanograms of PSA per milliliter of blood (ng/ml) and can vary somewhat from one laboratory to another.
Some drugs, such as Finasteride and Dutasteride (used to treat benign prostate disease), certain infectious disorders such as prostatitis, and even urethral trauma (such as from placement of catheters or dilators, or such as occurs in high-performance cyclists) can modify the PSA values. It’s important to take into account that ejaculation in men over 50 years of age momentarily increases the levels of both the free antigen as well as the total. These return to their normal values in 24 h. For this reason, patients should refrain from intercourse for at least 2 days before the extraction of blood for the study. Contrary to what was believed for many years, the digital rectal examination does not significantly alter PSA levels.
All of the circumstances described above show that an abnormal analysis does not necessarily indicate that a prostate biopsy should be performed or that there is cancer; nevertheless, the higher the PSA concentration the greater the probability of a malignant tumor.
Since the discovery of the prostate-specific antigen, several of its isoforms have been isolated and studied. The most common are bound PSA (which is bound to a plasma protease inhibitor) and free PSA (which circulates without being attached to any other molecule.) Together they add up to the total PSA.
Total PSA
The total PSA is the result of the sum of the antigen that circulates freely and the antigen that circulates bound to proteins. It is estimated that normal values are around 0.7 ng/ml in men under 50 years, 0.9 ng/ml in men between 50 and 60 years of age, 1.2 ng/ml in men from 60 to 70 years, and 1.5 ng/ml in men older than 70. Clearly the natural aging process increases the size of the prostate gland and consequently raises the quantity of total PSA in the blood (Fig. 3.3).

Value of total PSA
Benign-growth prostate cancer
The natural aging process increases the size of the prostate gland and consequently raises the quantity of total PSA in the blood.
Bound PSA (attached to another protein)
Patients with prostate cancer have less free PSA and therefore have a diminished PSA ratio (PSAR).
Total PSA Compared to Free PSA
Approximately 5–35 % of the total PSA is found in the free form; that is, it circulates in the blood without being bound to any protein. Patients with prostate cancer show less free PSA because most of the antigen is bound to proteins while it circulates. This detail is extremely important since it can help distinguish between a patient with cancer and one with benign growth of the prostate. Both have a high total PSA, but the one with cancerous cells shows less free PSA.
Free PSA includes at least three isoforms currently under study. Those studies will probably increase the possibility of making more trustworthy diagnoses in the future.
Besides the concentrations of total PSA and free PSA, other characteristics of the antigen are also analyzed for diagnostic purposes. These characteristics or “indicators” are as follows:
-
1.
Static indicators
-
PSA density (PSAD): It is known that each gram of healthy prostate tissue liberates a certain quantity of PSA into the blood. Therefore, it is expected that patients with prostates of a larger volume have a total PSA higher than normal. The density of the prostate-specific antigen (PSAD) is the relation that exists between the total PSA and the size of the prostate. Its value is obtained by dividing the total PSA by the weight in grams of the prostate. It is necessary to take into account that the larger the prostate gland, the more PSA-producing cells it will have and this will result in a larger value; but if the gland is not so large and has a high PSA, there is a greater possibility that this increase is due to a cancer, because the cancerous tissue produces more PSA than normal tissue. Current statistics determine that a man with a PSAD higher than 0.15 is at greater risk for cancer than the general population. On the other hand, patients with large prostates, larger than 80 g, may have a high total PSA but a PSAD lower than 0.10.
-
PSA ratio (PSAR): This percentage is found by dividing the value of the free PSA by the total PSA. The lower the result the greater possibility of prostate cancer, especially when it is lower than 0.15 or 15 %. This is because when there is cancerous prostate tissue, most of the circulating antigen is bound to proteins and there is very little free PSA, thus the PSAR is also diminished (Fig. 3.4).
Figure 3.4 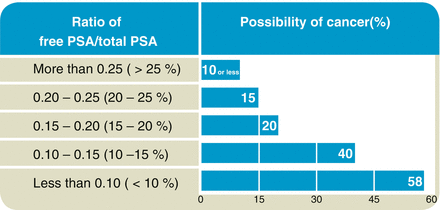
Ratio of free PSA/Total PSA
-
-
2.
Dynamic indicator
-
PSA velocity (PSAV): This is an evaluation of the PSA over time, requiring at least three studies over 18 months. It is accepted that the PSA may rise up to 0.25 ng/ml per year in men between 40 to 59 years, 0.4 ng/ml per year in men from 60 to 70 years, and up to 0.75 ng/ml per year in men older than 70. Antigen increases greater than these values; and if persistent at any age, increase the suspicion of prostate cancer (Fig. 3.5).
Figure 3.5 
PSA normal estimated value
-


Future Tumor Markers for Prostate Cancer
The discovery and development of new tumor markers for prostate cancer is a great challenge for medical science. Although there are constantly new advances, their application tends to take time. One needs only to remember that more than a decade had to pass after its discovery before PSA was applied in modern clinical settings, and in the same way a decade later it is recognized that it’s still not the ideal tumor marker. New bodily substances identified as playing a role in the functioning and/or disease of the prostate, often at a molecular level, must be developed to permit the differentiation of degrees of tumor aggressiveness and with this information, discover the best treatments.
At present, many research projects are underway that are concentrating on studying different bodily substances that might become future tumor markers for prostate cancer. Here are some of the most important:
-
Isoforms of PSA: Free PSA is comprised of at least three varieties of isoforms that have shown diagnostic utility in prostate cancer. The most important are ProPSA (pro-prostate-specific antigen) and the BPSA (B-prostate-specific antigen). The presence of the isoform ProPSA is related to aggressive varieties of prostate cancer. Diagnostic tests that detect it might in the future diminish the need to do biopsies. The BPSA isoform traditionally represents benign prostate tissue, so that the ratio between ProPSA and BPSA helps improve the timely detection of prostate cancer.
-
AMACR ( alpha-methylacyl-CoA racemase ): This is an enzymatic substance expressed in practically all types of prostate cancer. It is detected by special histopathological stains and is currently used to confirm the diagnosis in tissue samples obtained through biopsy.
-
Autoantibodies (AA): Recently, multiple specific antigens for prostate cancer have been discovered, as well as the corresponding autoantibodies, in the plasma of patients whose cancer has already been diagnosed.
-
PCA3 (prostate cancer antigen): This is a gene detected in the urine obtained after a digital rectal examination. It is estimated that in patients with prostate cancer, the concentration of this gene is up to 95 % greater than in patients with healthy prostate tissue; thus it promises to be a very sensitive test in the timely detection of prostate tumors.
Fact
Although the measurement of PSA is used principally for the early detection of prostate cancer, it is also clinically useful in other situations; for example, in patients with prostatitis who present initially with a high PSA but then receive medical treatment, the PSA levels tend to decrease as the treatment takes effect and the symptoms of the inflammation of the gland improve. Likewise, patients with prostate cancer who have already undergone surgery, radiation therapy, or other treatments and who continue the PSA tests as part of a follow-up screening are more likely to accurately determine whether the treatment has been successful or whether there is a relapse of the disease, taking into account that the PSA takes 4–6 weeks to fall to its definitive level. These and other details will be explained at length in the following chapters.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this chapter
Cite this chapter
Sotelo, R., Azhar, R.A., Guajardo, M.J.S. (2015). Prostate-Specific Antigen (PSA). In: Sotelo, R., Arriaga, J., Azhar, R., Gill, I. (eds) Prostate Cancer. Springer, Cham. https://doi.org/10.1007/978-3-319-05600-5_3
Download citation
DOI: https://doi.org/10.1007/978-3-319-05600-5_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-05599-2
Online ISBN: 978-3-319-05600-5
eBook Packages: MedicineMedicine (R0)