
Abstract
Cancer is an environmental disease and skin cancer (melanoma and non-melanoma) is the most common of all cancers. Epidemiological and experimental evidence suggest “chronic inflammation” to be one of the hallmarks in solar ultraviolet radiation and several other environmental agent-mediated skin cancers. The identification of transcription factors, mainly nuclear factor-kappa B (NF-κB), signal transducer and activator of transcription 3 (STAT3), hypoxia-inducible factor-1 alpha (HIF-1α) and their gene products i.e. prostaglandins, cyclooxygenase-2 (COX-2), cytokines [tumor necrosis factor- alpha (TNF-α)], chemokines [CXC-chemokine ligand (CXCL)] and chemokine receptors suggest critical role of inflammation in skin carcinogenesis. Considering the potential role of inflammation in tumor initiation and its major role in promotion/progression, as well as tumor angiogenesis and metastasis; inflammatory pathways may become attractive targets for skin cancer prevention. Hence this review focuses on compiling available evidence and understanding the role of chronic inflammation in the development of skin cancer.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Skin
- Chronic inflammation
- Causative agents
- Risk factors
- Skin cancer
- Basal cell carcinoma
- Squamous cell carcinoma
- Melanoma
- Molecular mechanism(s)
- Prevention
- Treatment
17.1 Introduction
Exposure to a wide variety of natural and/or man-made agents/substances in the environment accounts for majority of cases of cancer. These environmental factors include lifestyle choices such as use of tobacco, alcohol, poor diet, and excessive sunlight exposure. Other factors include exposure to certain drugs, hormones, radiation, specific viruses/bacteria, and environmental chemicals that may be present in the air, water, food, and workplace. The chance that an individual will develop cancer in response to exposure to a specific environmental agent depends on complex interactions between environmental and host factors (genetic/acquired susceptibility/protective), how long and how often a person is exposed to a particular substance, exposure to other agents, genetic factors, diet, lifestyle, health, age and gender, etc.
The environmental agent(s)-mediated cancers have been observed to share ten common traits that govern the transformation of normal cells to cancer cells (Hanahan and Weinberg 2011). Accumulating evidence has resulted in the acceptance of “chronic inflammation” to be one of the ten hallmarks of cancer. Cancers caused by environmental agents frequently occur in tissues with the greatest surface exposure to the agent(s), e.g., lungs, gastrointestinal tract, and skin (Loeb and Harris 2008). Skin cancer is the most common of all cancers. Therefore, this review focuses mainly on compiling available evidence and understanding the role of chronic inflammation in the development of skin cancer. Before presenting the available evidence on (a) the role of inflammatory molecules in the development of skin cancer in vitro and in vivo, and (b) observations on inhibitors of inflammation for the prevention and treatment of skin cancer, brief description of skin structure, function, types and prevalence of skin cancer, causative agents and risk factors, treatment modalities and survival, etc., has been included for enhancing the understanding and clarity of the presentation.
17.1.1 Skin Structure and Function
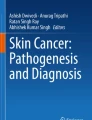
The skin is the largest and dynamic organ of the body, making up 16 % of body weight, with a surface area of 1.8 m2 and situated at the interface between the body and environment. Skin serves as the armors for the body against mechanical, thermal, and physical injury and hazardous substances (Proksch et al. 2008). There are three structural layers of the skin: epidermis, dermis, and subcutaneous layer (Fig. 17.1).

Schematic presentation of skin structure, cell types, causes, and risk factors associated with skin cancer
Epidermis is an external and continually regenerative, stratified epithelium devoid of blood or nerve supplies of approximately 5–100 μm thickness. It is composed of several distinct cell populations, keratinocytes and melanocytes being the main constituents. Keratinocytes, which comprise 95 % of the epidermis, are arranged in four layers. The inner layer is the stratum germinativum (stratum basale, basal layer), from which columnar-shaped keratinocytes divide to migrate to the next layer. The stratum spinosum (spinous layer) is composed of polygonal keratinocytes that become eventually more condensed. Further differentiation of the cells leads to the stratum granulosum (granular layer), which contains basophilic granules. In thick skin areas, such as the soles of feet or the palms of hands, there is a clear layer of flattened cells called the stratum lucidum. The outermost layer is the stratum corneum (horny layer), which contains keratin and dead cells that confer to the skin its barrier function. Melanocytes are cells of neural crest embryogenic origin whose primary function is to produce melanin, the pigment that determines skin and hair color. They are located in the basal layer of the epidermis, which comprise from 5 to 10 % of the cells and in hair follicles, and are also found in other anatomical areas such as the inner ear, the eye, and the meninges (Costin and Hearing 2007).
Dermis, the middle layer of the skin found below the epidermis, is composed of a tough, supportive cell matrix. The dermis contains fibroblasts, which produce collagen, elastin, and structural proteoglycans, together with immune-competent mast cells and macrophages. Collagen fibers, which make up 70 % of the dermis, give skin its strength, elasticity, and toughness. Dermis contains hair follicles, sweat glands, blood vessels, and nerves that are held in place by collagen.
Subcutis or subcutaneous layer consists of loose connective tissue and fat. It helps the body conserve heat and has a shock-absorbing effect that helps protect the body’s organs from injury.
Skin has several functions, the most important being to form a physical barrier to the environment, allowing and limiting the inward and outward passage of water, electrolytes, and various substances while providing protection against microorganisms, ultraviolet radiation (UVR), toxic agents, and mechanical insults. Its other functions are insulation, temperature regulation, sensation, and synthesis of vitamin D and the protection of vitamin B folates.
17.1.2 Types of Skin Cancer
There are four different types of skin cancer: basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) collectively referred to as non-melanoma skin cancers (NMSC) or keratinocyte carcinoma; melanoma and other non-epithelial skin cancer. BCC and SCC account for approximately 80 and 16 % of all NMSC, respectively. Melanoma accounts for only 10 % of skin cancer cases, but it is the most serious type, which can also occur in other body organs (Ibanez et al. 2011). Along with melanoma and keratinocyte cancers, there are some other less common types of skin cancer, e.g., Merkel cell carcinoma, Kaposi’s sarcoma, cutaneous (skin) lymphoma, skin adnexal tumors, dermatofibrosarcoma protuberans, and angiosarcoma.
17.1.3 Prevalence
Skin cancer is the most common malignancy in the USA, Australia, and New Zealand with substantially associated morbidity and cost, as well as relatively smaller but significant mortality (Rogers et al. 2010). Australia and New Zealand have the highest rates of skin cancer incidence in the world, almost four times the rates registered in the USA, the UK, and Canada. Skin cancer is 10 times more common in whites than in African Americans. It is estimated that one American dies every hour from skin cancer, whereas the incidence of UV-induced NMSC has increased dramatically worldwide accounting for more than 40 % of all human cancers in the USA, with about 1.3 million new cases being diagnosed annually of which roughly 20–30 % is of SCC (Madan et al. 2010).
17.1.4 Causative Agents and Risk Factors
UVR from sun exposure is the main cause of skin cancer, accounting for at least 65 % of melanomas worldwide. The geographic variation and risk of development of NMSC are associated with ambient sun irradiance, genotypic, phenotypic, and environmental factors. Risk is greatest in residents of high ambient solar irradiance who have markers of UV susceptibility, such as light skin, eye and hair color, or an inability to tan, and those with benign sunlight-related skin disorders, e.g., actinic keratosis (AK) and solar lentigines. Incidence within countries is associated with increasing proximity to the equator. The thinner ozone layer and shorter distance traversed by UVB at lower latitudes than at high latitudes make residents of these regions most vulnerable to the effects of this radiation (Madan et al. 2010).
Individuals with familial genetic syndromes, viral infections such as human immunodeficiency virus (HIV), human herpesvirus 8 (HHV8), and human papilloma virus (HPV) or exposed to artificial UVR (tanning beds and lamps), aging, diet, and smoking are attributed risks. Some treatment modalities, including radiotherapy, phototherapy, psoralen, long-wave ultraviolet radiation (PUVA), and immunosuppressant drugs (cyclosporin A, methotrexate) besides work-related exposures such as arsenic, tar product, and chemical carcinogens (petroleum refining, pesticide manufacturing, etc.), also predispose individuals to skin cancers (Fig. 17.1) (IARC 1987; Boffetta et al. 2001). Skin cancers are also attributed to chronically injured or non-healing wounds and scars or ulcers that occur at sites of previous burns, sinuses, trauma, osteomyelitis, prolonged heat (Kangri cancer) and chronic friction (Saree/Dhoti cancer) (Aziz et al. 1998; Patil et al. 2005; Saladi and Persaud 2005). The incidence of malignancy in scar tissues is 0.1–2.5 %.
17.1.5 Treatment for Skin Cancer
A variety of modalities for the treatment of skin cancer is available, including surgery, radiation therapy, chemotherapy, photodynamic therapy (PDT), and biological therapy. Surgical options, including curettage with electrodessication, Mohs micrographic surgery, and surgical excision, are the most frequently used treatments, providing a high control rate and satisfactory cosmetic results. Radiation therapy, including brachytherapy techniques and external beam radiations such as superficial/orthovoltage X-rays, megavoltage photons, and electron beam radiation, has been used as primary and post-surgical adjuvant therapy for skin cancers. Chemotherapy includes the topical agents (in the form of ointment) such as fluorouracil, diclofenac sodium, and imiquimod. In PDT, a photosensitive drug and a certain type of laser light are used to kill cancer cells. However, in biological therapy (biotherapy or immunotherapy), substances such as interferon and imiquimod (made by the body or in a laboratory) are used to boost, direct, or restore the body’s natural defenses against cancer.
17.1.6 Survival
Although the incidence of skin cancer is increasing, it is curable especially if it is detected or treated early and considered one of the most preventable types of cancer. The 5- and 10-year relative survival rates for persons with melanoma which is more likely than other skin tumors to spread to other parts of the body, are 91 and 89 %, respectively. For localized melanoma (84 % of cases), the 5-year survival rate is 98 %; survival declines to 62 and 15 % for regional- and distant-stage disease, respectively. BCC and SCC are highly treatable, and survival rates for NMSC are very high. The mortality rate of NMSC is around 0.3 %, causing 2,000 deaths per year in USA (American Cancer Society 2013).
17.1.7 Inflammation and Skin Cancer
Inflammation is a signal-mediated response to cellular insult by infectious agents, toxins, and physical stresses. Inflammation is caused by physical agents (e.g., UVR), mechanical injuries, chemical agents (tar products, arsenic, immunomodulatory drugs, toxins), biological agents (bacteria, viruses, fungi, parasites), immunologic disorders (hypersensitivity reactions, autoimmunity, immunodeficiency states), etc. Inflammation can be acute or chronic with distinct characteristics (see Table 17.1) (Mueller 2006; Aggarwal et al. 2009). Acute inflammation is a rapid, self-limiting process, maybe prolonged and transformed to chronic inflammation. Chronic inflammation being more insidious lies at the basis of various diseases, including cardiovascular diseases, cancer, diabetes, arthritis, Alzheimer’s disease, pulmonary diseases, and autoimmune diseases (Aggarwal et al. 2009).
As early as 1863, Virchow noted leukocytes in neoplastic tissues and made a connection between inflammation and cancer. He suggested that the “lymphoreticular infiltrate” reflected the origin of cancer at sites of chronic inflammation (Mantovani et al. 2008). The correlation between cancer and inflammation has been recognized for decades, but only in recent years, evidence begun to suggest that the inflammation is a prerequisite rather than a consequence of tumorigenesis (Balkwill and Coussens 2004). It is estimated that underlying infections and inflammatory responses are linked to 15–20 % of all deaths from cancer worldwide (Lu et al. 2006; Parkin 2006; Mantovani et al. 2008). Several clinical conditions such as discoid lupus erythematosus, dystrophic epidermolysis bullosa, and chronic wound sites are associated with cutaneous inflammation and appear to predispose the individual to increased susceptibility for skin cancer (Nickoloff et al. 2005).
Injury to the skin initiates a cascade of events including inflammation, new tissue formation, and tissue remodeling which leads to wound repair. In chronic inflammation, active inflammation, tissue destruction, and attempts at repair proceed simultaneously. The inflammatory response involves three major stages: dilation of capillaries to increase blood flow; microvascular structural changes and escape of plasma proteins from the bloodstream; and leukocyte transmigration through endothelium and accumulation at the site of injury (http://bme.virginia.edu/ley/). In addition to the defense functions [production of proteinase and reactive oxygen species (ROS)], inflammatory cells are also an important source of growth factors and cytokines such as interleukin-1 (IL-1) and tumor necrosis factor-alpha (TNF-α) that are necessary for cell recruitment, activation, and proliferation (Nickoloff et al. 2005; Mueller 2006). However, while normal inflammation, e.g., during wound healing, is a rapid self-limiting process, deregulation of the profile and level of any of cytokines/chemokines that persists at sites of inflammation result in the development of various pathologies including cancer. The mechanisms include induction of genomic instability, alterations in epigenetic events and subsequent inappropriate gene expression, enhanced proliferation of initiated cells, resistance to apoptosis, unlimited replicative potential, sustained angiogenesis (tumor neovascularization), tissue invasion, and metastasis (Colotta et al. 2009).
17.2 Inflammatory Signaling Pathways Associated with Skin Cancer
Inflammation is associated with different stages of tumor development, including initiation, promotion, malignant conversion, invasion, and metastasis (Fan et al. 2013). Cancer-related inflammation, which has been suggested to represent the seventh hallmark of cancer (Hanahan and Weinberg 2011), affects all the important aspects of cancer such as proliferation and survival of cancer cells, tumor response to chemotherapeutic drugs and hormones, metastasis and angiogenesis similar to that seen in chronic inflammatory responses, and tissue remodeling/repair (Kamp et al. 2011; Mantovani et al. 2008).
Two pathways connect cancer and inflammation: the intrinsic and extrinsic pathways (Fig. 17.2). The intrinsic pathway is activated by genetic events that cause neoplasia, including the activation of oncogenes (H-ras, N-ras, BRAF, c-MYC, human counterpart of MDM2 [HDM2], C-erbB) by mutation, chromosomal rearrangement or amplification, and inactivation of tumor suppressor genes (p16/INKA4 [cyclin-dependent kinase inhibitor 2A], p14/ARF [ADP ribosylation factor]) (Soehnge et al. 1997; Hocker et al. 2008; Hanahan and Weinberg 2011). Cells, which are transformed in this manner, produce inflammatory mediators, thereby generating an inflammatory microenvironment in tumors. Moreover, there are other gene products frequently observed in skin cancer (mainly melanoma and NMSC) such as protein-patched homolog 1 (PTCH1), PTCH2, sonic hedgehog (Shh), cyclin-dependent kinase 4 (CDK4) and CDK6, melanocortin 1 receptor (MC1R), microphthalmia-associated transcription factor (MITF), cytochrome p450 (CYP), glutathione S-transferase theta 1 (GSTT1), Ras, xeroderma pigmentosum, complementation group C (XPC), and tumor protein 53 (TP53). Genes involved in UVR-induced skin cancer include the tumor suppressor gene p53, PTCH, and the ras oncogenes (Hocker et al. 2008; Madan et al. 2010).

Signaling pathways associated with inflammation and skin cancer
In contrast, the extrinsic pathway represents inflammatory leukocytes and soluble mediators leading to conditions, which increase cancer risk (Fig. 17.2). The chronic inflammation related to malignancy is induced by infections with pathogens (HHV), mechanical, radiation, and chemical insults, which results in the production of oxidative stress (Del Prete et al. 2011). The two pathways unite, resulting in the activation of transcription factors, mainly nuclear factor kappa B (NF-κB), signal transducer and activator of transcription 3 (STAT3) and hypoxia-inducible factor-1 alpha (HIF-1α) in tumor cells. These transcription factors coordinate the production of pro-inflammatory mediators, including cytokines (TNF-α, IL-6, IL-1), chemokines (chemokine [C-C motif] ligand 2 [CCL2], CXC chemokine ligand 8 [CXCL8]), as well as the production of cyclooxygenase-2 (COX-2) (which, in turn, results in the production of prostaglandins [PG]) (Mantovani et al. 2008; Del Prete et al. 2011). Pro-inflammatory cytokines, the important mediators of inflammation, have distinguished roles in skin cancer development and along with nitric oxide (NO) act as cell-to-cell messenger as well as help in the activation of NF-κB (Kundu and Surh 2008). The cytokines activate the same key transcription factors in inflammatory cells, stromal cells, and tumor cells, resulting in more mediators’ production and cancer-related inflammatory microenvironment being generated.
In extrinsic pathway, exposure of skin to various physical, chemical, or biological agents induces infiltration of neutrophils at site of tissue injury which are key producers of ROS and reactive nitrogen species (RNS). ROS, an inherent part of the anabolism and catabolism of various body tissues, including skin, play important roles in the stimulation of molecules for metabolism, cell cycle, and intercellular transduction pathways (Ibanez et al. 2011) and are involved in all the three stages of carcinogenesis, viz. initiation, promotion, and progression. Furthermore, transient levels of ROS can activate cellular proliferation or survival signaling pathways, such as the NF-κB, activator protein-1 (AP-1), extracellular signal-regulated kinase-/mitogen-activated protein kinase (ERK/MAPK), and phosphoinositide 3-kinase/Akt8 virus oncogene cellular homolog (PI3K/Akt) pathways. In addition, ROS induce both the activation and synthesis of AP-1, a regulator of cell growth, proliferation, and apoptosis, and transcription factors such as STAT3, HIF-1α, and p53 (Reuter et al. 2010).
NF-κB and STAT3 are two most important transcription factors in inflammatory pathways that play major roles in tumorigenesis because they are constitutively active in most cancers, including skin (melanoma, SCC, Kaposi’s sarcoma). Moreover, most gene products linked to inflammation, survival, proliferation, invasion, angiogenesis, and metastasis are regulated by NF-κB and STAT3, and most chemopreventive agents mediate their effects through inhibition of NF-κB and STAT3 activation pathways (Aggarwal et al. 2009; Zhu et al. 2011).
Many stimuli can induce NF-κB activity, such as TNF-α, IL-1β, bacterial lipopolysaccharides (LPS), UV, ionizing radiation, ROS, several skin-related microorganisms such as Borrelia burgdorferi, Neisseria gonorrhoeae, Staphylococcus aureus, herpes simplex virus (HSV), measles virus, and HIV-1 (Pahl 1999; Bell et al. 2003). NF-κB activation as core transcriptional mediator of inflammation is a central component of pro-carcinogenic innate immune responses. Functional nuclear NF-κB is necessary for the growth inhibition control during upward cellular migration and differentiation of epidermal cells, which have central role in skin carcinogenesis (Bell et al. 2003). Several NF-κB-dependent genes present in the skin are essential to the initiation of cutaneous inflammation, including genes for different chemokines (IL-1, IL-6, TNF) and cytokines, intercellular adhesion molecule-1 (ICAM-1), vascular cell adhesion molecule-1 (VCAM-1), urokinase plasminogen activator (uPA), and E-selectin (Pahl 1999; Bell et al. 2003). NF-κB also regulates pro-inflammatory enzymes, such as inducible nitric oxidase synthase (iNOS) and COX-2, which are involved in chronic inflammation of the skin and later in skin carcinogenesis. Additionally, NF-κB controls the expression of the genes linked with apoptosis (cellular inhibitor of apoptosis [c-IAP], XIAP, B cell lymphoma 2 [Bcl-2], Bcl-xL, cellular FLICE-like inhibitory protein [c-FLIP], survivin), proliferation (cyclins, c-Myc), invasion, angiogenesis, and metastasis (e.g., matrix metalloproteinase [MMP], vascular endothelial growth factor [VEGF], CXCL12, C-X-C chemokine receptor type 4 [CXCR4]) of cancer. Based on these evidences, NF-κB is believed to be closely associated with the whole process of tumorigenesis (Prasad et al. 2010; Zhu et al. 2011).
STATs are proteins that are activated by extracellular signaling proteins, growth factors such as epidermal growth factor receptor (EGFR), cytokines (IL-6, IL-17, IL-22), and various peptides (Zhu et al. 2011). STAT3 regulates the expression of genes that mediate survival (survivin, Bcl-xl, myeloid cell leukemia sequence 1 [mcl-1], c-FLIP), proliferation (c-fos, c-myc, cyclin D1), invasion (MMP-2), and angiogenesis (VEGF) (Aggarwal et al. 2009). Along with NF-κB, STAT3 is a point of convergence for numerous oncogenic signaling pathways. Maintenance of NF-κB activation in tumors requires STAT3 which is constitutively activated both in tumors and in immune cells and plays a role in carcinogenesis (Colotta et al. 2009).
17.3 Role of Inflammatory Molecules in the Development of Skin Cancer: Evidence from In Vitro Studies
17.3.1 Role of Inflammatory Molecules in the Transformation of Skin Cells
Causal association between environmental (chemical/physical/biological) agent(s) in cancer development has been well established, while understanding and acceptance of the role of inflammation in cancer development are relatively recent. Due to this, evidence from available in vitro and/or in vivo experimental model systems pertaining to the role of inflammation in initiation of carcinogen-induced tumorigenicity is not clearly and conclusively addressed. One of the main reasons being non-inclusion of this aspect in the scope and planning of the experiments to address the question and/or complexity of experimental/real-life systems, wherein role of inflammation among multiple factors cannot easily be identified. Most of the environmental skin cancer-causing agents have been shown to induce spectrum of changes such as genotoxicity, cytotoxicity, and inflammation in cells exposed in vitro, and hence, biological significance and criticality of exact role of inflammation in the initiation of carcinogenesis are not established. Available evidence suggests the role of inflammatory molecules in the promotion of carcinogenesis in cells which have been initiated, wherein some products generated during inflammation do possess ability to damage/modify DNA, proteins, and lipids (Lu et al. 2006).
Several studies support the hypothesis that regulation of chemokines in certain cells in the presence of persistent autocrine and paracrine stimulation with specific CXC chemokine ligands can promote preneoplastic to neoplastic cellular transformation. Over-expression of CXCL1 (melanoma growth stimulatory activity/growth-regulated protein α) induced by IL-1, LPS, and TNF-α in immortalized melanocytes resulted in the transformation of these cells that had capability to form tumors in nude/SCID mice (Dhawan and Richmond 2002).
RAS-mediated tumor formation is commonly associated with up-regulation of cytokines and chemokines that mediate an inflammatory response relevant to oncogenesis (Cataisson et al. 2012). Over-expression of any of three normal Ras genes, N-Ras, H-Ras, or K-Ras, leads to in vitro transformation (Crespo and Leon 2000; Dhawan and Richmond 2002). Studies using in vitro transformation assay have demonstrated that N-Ras could induce cellular transformation in a manner similar to CXCL1 in controlling melanocyte cells (Dhawan and Richmond 2002), indicating that CXCL1-mediated transformation requires Ras activation in melanocytes. Using both genetic and pharmacological approaches, it has been observed that the differentiation and pro-inflammatory effects of oncogenic RAS in keratinocytes require the establishment of an autocrine loop through IL-1α, IL-1R, and myeloid differentiation primary response gene (88) (MyD88), leading to the phosphorylation of IκBα (inhibitor of κBα) and NF-κB activation. Thus, MyD88 exerts a cell-intrinsic function in RAS-mediated transformation of keratinocytes (Cataisson et al. 2012).
The modulation of IL-1α production in the HaCaT keratinocyte cell line, wherein UVR induces keratinocytes to secrete other pro-inflammatory and immunomodulatory mediators, promotes inflammation and skin tumor development (Magcwebeba et al. 2012). Maximal production of these mediators appears to be due to over-expression of the slug (snail homolog 2 or zinc finger 2 [Snai2]) transcription factor in keratinocytes and normal human melanocytes, thereby stimulating growth and migration (Shirley et al. 2012). UVB exposure led to significant increase in the production of IL-1α in a dose-dependent manner with minimal necrotic and apoptotic effects. Moreover, induction of IL-6 production following short-wave UVR in normal human epidermal keratinocytes and epidermoid carcinoma cell line is mediated by DNA damage and that IL-6 release has been shown to be associated with enhanced levels of IL-6 mRNA transcripts (Petit-Frere et al. 1998).
In primary mouse keratinocyte cultures, prostaglandin E2 (PGE2) activated the EGFR and its downstream signaling pathways as well as increased cAMP production and activated the cAMP response element binding protein (CREB). Inhibitors of ERK1/2 and PI3K pathway attenuated the PGE2-induced proliferation, NF-κB, AP-1, and CREB binding to the promoter regions of the cyclin D1 and VEGF genes and expression of cyclin D1 and VEGF in primary mouse keratinocytes (Ansari et al. 2008).
Nuclear factor of activated T cells (NFAT), known to be expressed in both immune and non-immune cells, plays an essential role in inflammatory responses by regulating the expression of a wide range of pro-inflammatory cytokines. It has been demonstrated that NFAT transcriptional activity is preferentially induced by UVB wavelengths in HaCaT keratinocytes and retroviral Phoenix amphotropic (RPA) cells. Inhibiting UV-induced NFAT activation in keratinocytes led to reduced COX-2 protein induction and an increase in UV-induced apoptosis (Flockhart et al. 2008).
Pro-inflammatory cytokines have been shown to activate NF-κB by activating an NF-κB-inducing kinase (NIK)/MEKK–IκB kinase (IKK)–IκB signaling pathway in many cell types. Studies have reported that the suppression of phosphorylation of NF-κB/p65 on Ser536 reduced the activation and nuclear translocation of NF-κB and functionally led to the resistance of JB6 cells to TNF-α-induced transformation (Hu et al. 2005; Lu et al. 2006).
Different proteases also play important role in the transformation of skin cancer cells. Serpins constitute the most broadly distributed super family of protease inhibitors described in humans. Expression profiling of normal epidermal keratinocytes and transformed SCC cell lines revealed up-regulation of SerpinA1 in the latter and that the level of SerpinA1 mRNA has shown marked up-regulation as analyzed by quantitative RT-PCR. SerpinA1 production by SCC cells appears to be dependent on p38 MAPK activity and up-regulated by EGF, TNF-α, interferon-gamma (IFN-γ), and IL-1β (Farshchian et al. 2011). Other important protease is stromelysin-2 (MMP-10), which is known to be involved in the growth of skin tumors. The level of MMP-10 was up-regulated in a cutaneous SCC cell line (UT-SCC-7) by TNF-α and keratinocyte growth factor and by IFN-γ in combination with transforming growth factor (TGF)-β1 and TNF-α both in UT-SCC-7 and in HaCaT cells (Kerkela et al. 2001).
HPV are known to be additional cofactors in the development of cutaneous SCC. Several studies have evaluated the ability of the E6 and E7 proteins of HPV to transform cells in vitro. HPV 10 and HPV 20 E7 proteins do not display in vitro transforming activities. Moreover, E6 and E7 of HPV 38 have been shown to immortalize primary human keratinocytes, suggesting a role of HPV 38 infection in skin carcinogenesis. High-risk HPV E5 is considered tumorigenic because it transforms murine fibroblasts and keratinocytes in tissue culture, enhances the immortalization potential of E6 and E7, and, in cooperation with E7, stimulates the proliferation of human and mouse primary cells (IARC 2007).
17.3.2 Role of Inflammatory Molecules in the Survival and Proliferation of Skin Cancer Cells
Available experimental evidence suggests that the inflammatory response plays a role in providing survival and proliferative signals to initiated cells, thereby leading to tumor promotion (Balkwill and Coussens 2004). While NF-κB protein is a key player in inflammation, other molecular targets comprise cytokines, chemokines, ROS, oncogenes, inflammatory enzymes (COX-2, 5-lipoxygenase [5-LOX], MMP), anti-apoptotic proteins, transcription factors (STAT3, AP-1, CREB, nuclear factor erythroid 2-related factor 2 [Nrf2]) that regulate tumor cell proliferation, transformation, and survival (Shanmugam et al. 2012).
Expression of NF-κB has been shown to promote cell proliferation and contribute to cell survival mechanism. Cell lines from SCC are reported to constitutively express activated NF-κB (Balkwill and Coussens 2004). Definitive evidence that STAT3 (which is inducible by IL-6 signaling) contributes to oncogenesis has shown that interrupting STAT3 signaling blocks the transformation of fibroblasts by SRC oncoprotein (Yu et al. 2007; Hanahan and Weinberg 2011). Constitutively activated STAT3 is known to support tumor cell survival and proliferation by up-regulating expression of the anti-apoptotic protein, Bcl-2, in diverse human cancer cell lines, including melanoma cells. STAT3 also controls expression of cyclins D1, D2, and B, as well as the proto-oncogene c-Myc, and through them, it may stimulate cell proliferation (Yu et al. 2007).
The tumor- and progression-promoting effect of inflammatory cytokines is substantiated by the enhanced tumor growth of IL-6-transfected human BCC as well as by the malignant progression that is associated with the expression of G-colony-stimulating factor (G-CSF) and granulocyte/macrophage colony-stimulating factor (GM-CSF) in HaCaT keratinocyte cells (Mueller 2006). Studies on TNF-α signaling, the most extensively studied pro-inflammatory cytokines in skin carcinogenesis, revealed an involvement of both TNF-α receptor subtypes, as well as of protein kinase C-alpha (PKC-α) and transcription factors of the AP-1 family in tumor promotion-mediated inflammation and proliferation as well as angiogenesis and invasion (Balkwill and Coussens 2004; Mueller 2006; Mantovani et al. 2008). Cytokines also control the inflammatory milieu to either favor anti-tumor immunity (IL-12, TNF-related apoptosis-inducing ligand [TRAIL], IFN-γ) or enhance tumor progression (IL-6, IL-17, IL-23) and also have direct effects on cancer cell growth and survival (TRAIL, FasL, TNF-α, EGFR ligands, TGF-β, IL-6) as in the case of melanoma cells (Haghnegahdar et al. 2000).
Tumor progression locus 2 (Tpl2) is a MAP3 kinase at the crossroad of various pro-inflammatory and oncogenic signals with a major role in promoting cell proliferation and transformation through activation of the ERK MAPK. Studies have reported a link between naturally occurring high levels of Tpl2 expression and ERK phosphorylation in melanoma cell lines. The over-expression of Tpl2 in melanoma cells carrying mutated B-Raf is associated with resistance to the Raf kinase inhibitor PLX4720. Tpl2 can also stimulate the activation of JNK and to a lesser extent p38c and ERK5 by directly phosphorylating their upstream kinases MKK4, MKK6, and MEK5 (Vougioukalaki et al. 2011). Ras, which is mutated in approximately 25 % of all malignancies, promotes cell proliferation and tumor growth of malignant cells. During inflammatory stimuli, Ras induces the expression of various inflammatory gene products, including the pro-inflammatory cytokines IL-1, IL-6, and IL-11, and the chemokine IL-8. ROS have been reported to be tumorigenic by virtue of their ability to increase cell proliferation, survival, and cellular migration through the activation and synthesis of AP-1, a regulator of cell growth, proliferation, and apoptosis (Reuter et al. 2010).
PGE2, which plays a key role in normal skin homeostasis, has been shown to be a critical player mediating the contribution of the COX-2 pathway to cancer development and acts as a tumor promoter, controlling many of the behaviors typical of cancer cells. Studies have shown increased E prostanoid 1 (EP) receptor levels in murine skin tumor cells and that this receptor is critical for the mitogenic effects of PGE2 on these cells in vitro, a finding that has also been demonstrated in NIH-3T3 cells (Tober et al. 2006).
In vitro studies have implicated Bmx (bone marrow tyrosine kinase gene in chromosome X) gene signaling in cell migration and survival. Bmx over-expression accelerates keratinocyte proliferation and wound re-epithelialization and also induces chronic inflammation in the skin and that this occurs via cytokine-mediated recruitment of inflammatory cells (Paavonen et al. 2004).
Cylindromatosis (CYLD), which encodes a 956 amino acid enzyme that is ubiquitously expressed, contains a deubiquitinating domain at the C-terminus. Mutations that inactivate the carboxyl-terminal-deubiquitinating domain of CYLD deregulate the NF-κB activity, underlying the development of skin appendage tumors in humans (Brummelkamp et al. 2003; Trompouki et al. 2003). It was demonstrated that the expression in tumorigenic epidermal cells of a catalytically inactive form of CYLD (CYLDC/S) that mimics the identified mutations of cyld in human tumors and competes with the endogenous CYLD results in enhanced cell proliferation and inhibition of apoptosis. These indicate an increased oncogenicity of the tumorigenic epidermal CYLDC/S mutant cells in vitro. The loss of CYLD in keratinocytes has been linked to hyperproliferation and elevation in cyclin D1 levels because of increased nuclear activity of Bcl-3-associated NF-κB p50 and p52 (Massoumi et al. 2006). A decrease in CYLD function results in an increase in the malignant behavior of the tumor epidermal cells and progression of skin carcinomas, as seen by an enhancement in proliferation and survival of the cells expressing the mutant CYLDC/S. Tumor epidermal cells expressing CYLDC/S also show an important increase in the nuclear localization of Bcl-3, p52, and β-catenin.
Tumor formation involves epigenetic modifications and microenvironmental changes as well as cumulative genetic alterations encompassing somatic mutations, loss of heterozygosity, and aneuploidy. The role of NF-κB in epidermal hyperproliferation arising from p120 loss appears rooted in its impact on epidermal microenvironment because p120-null keratinocytes display a growth-arrested phenotype in culture due to mitotic alterations and chronic inflammatory responses, resulting in unstable, binucleated cells in vitro (Perez-Moreno et al. 2008).
17.3.3 Role of Inflammatory Molecules in the Invasion, Metastasis, and Angiogenesis of Skin Cancer Cells
Several clinical observations and experimental findings indicate that the process of metastasis is non-random and involves a sequence of multistep events targeted for therapy. Metastatic cancer cells exploit the mechanisms of the inflammation process, which successfully migrate into distant organs. This implies a pivotal role for specific adhesive interactions between cancer cells and vascular endothelial cells and activation of migratory pathways in the cancer cells (Laferriere et al. 2002). The tumor cells follow the extravasation strategy of leukocytes in their migration toward inflammatory sites (Witz 2006). For instance, VCAM-1, an integrin receptor located on an endothelial cell, binds to the integrin α4 β1 (VLA-4—very late antigen-4), which are normally expressed on leukocyte plasma membranes, but they do not adhere to their appropriate ligands until the leukocytes are activated by chemotactic agents or other stimuli (Schadendorf et al. 1995).
Selectins have been involved in the progression of cancer. In fact, several types of tumor cells express functional ligands of selectins and contact selectins expressed on blood vessel walls (Laferriere et al. 2002; Witz 2006; Barthel et al. 2007). Keratinocyte cell lines—A431, HaCaT, SVK14—express selectin ligands including sialyl Lewis X and S-Le(a) expression, whereas normal human keratinocytes do not. These findings suggest a potential role for selectin-mediated events in the early and late metastasis (Groves et al. 1993). To this end, the study of the role of selectins in leukocyte and tumor cell extravasation merits particular attention in understanding the pathophysiology of inflammation and cancer and is substantiated by a number of recent studies (Witz 2006; Barthel et al. 2007). There is also growing awareness that platelets and leukocytes may potentiate and even enhance the hematogenous dissemination of cancer cells, suggesting a link between inflammation and cancer progression. Indeed, the tumor microenvironment often contains infiltrates of platelets, macrophages, dendritic cells, and lymphocytes (Mantovani et al. 2008). These cells may be critical sources of pro-inflammatory cytokines, including TGF-β, TNF-α, IL-1β, and IL-6, all of which may promote the up-regulation of selectin expression on the vascular wall and synergize with chemokines, such as IL-8, secreted by tumor cells.
Tumor invasion and metastasis represent a multistep process that depends on the activity of many proteins (Hua et al. 2011; Shanmugam et al. 2012; Ravi and Piva 2013). Several classes of proteases, including MMPs, serine proteases like furin, and cysteine proteases such as cathepsin have been implicated in the tumor cell-invasive process. Of these, MMPs appear to be primarily responsible for extracellular matrix (ECM) degradation observed during invasive processes (Hua et al. 2011; Pytliak et al. 2012; Ravi and Piva 2013). They contribute to tumor growth by degradation of the ECM as well as by the release of sequestered growth factors such as VEGF, b-fibroblast growth factor (b-FGF), or TGFβ, the suppression of tumor cell apoptosis and the destruction of immune-modulating chemokine gradients (Ravi and Piva 2013). In normal skin, MMPs are not constitutively expressed but can be induced temporarily in response to exogenous signals such as UVR. UVR is known to elevate the expression of MMP-1, MMP-3 (stromelysin-1), and MMP-9 in human skin. MMP-2 and MMP-9 have been frequently associated with the invasive and metastatic potential of tumor cells (Ramos et al. 2004; Dong et al. 2008; Ravi and Piva 2013).
Furin is a serine protease that is frequently over-expressed in several cancer cell lines and malignancies, including several murine cell lines derived from chemically induced skin tumors (Fu et al. 2012). Its activity results in proteolytic cleavage of substrates, leading to the activation of many cancer-related proteins including important growth factors and receptors such as insulin growth factor-1 (IGF-1) and its receptor IGF-1R, TGF-β, and VEGF. (Siegfried et al. 2003; Ravi and Piva 2013). Furin is also involved in the maturation of both TNF-alpha-converting enzyme (TACE) and MMP within skin cells and mainly activate MT1-MMP, which directly contributes to the motility and invasiveness of the tumor cell, thereby indicating that furin activity has an influence on the inflammation seen in the skin, following exposure to UVR (Ravi and Piva 2013). It has been shown that furin mRNA, protein, and enzyme activity increase immediately after UVA and UVB treatment in human epidermal keratinocytes (HaCaT cells). Furin/PC processing of substrates has been shown to contribute to tumor progression, aggressiveness, metastasis, and angiogenesis (Arsenault et al. 2012; Fu et al. 2012; Ravi and Piva 2013).
Cytokines play a crucial role in tumor progression. Pro-inflammatory cytokine, TNF-α, stimulates the secretion of active MMP-2, an enzyme that degrades type IV collagenase, in organ-cultured full-thickness human skin. TNF-α also induces MMP-2 activation in human skin and thus induces angiogenesis with the MMPs involved in wound healing or cancer cell invasion. As basement membrane components, type IV collagen and laminin are potential substrates for MMP-2, and activation of a type IV collagenase by this cytokine may provide a mechanistic explanation for the role of TNF-α during metastasis and angiogenesis (Han et al. 2001). TNF-α up-regulates malignant melanoma invasion and migration in vitro. In melanoma, TNF-α may exert its pro-invasive effect on human cutaneous melanoma cell line via an integrin-dependent mechanism as well as a modest up-regulation of degradative enzyme activity not readily detected in general protease assays (Katerinaki et al. 2003).
IL-6 is also one of the pro-inflammatory cytokines induced by UVR in keratinocytes (Schwarz and Luger 1989; Chung et al. 1996). IL-6 induced angiogenesis in human BCC cell line by up-regulation of bFGF via both Janus kinase (JAK)/STAT3 and PI3-kinase/Akt pathways. Blockage of COX-2 by siRNA reduced angiogenic activity in IL-6 over-expressing BCC cells, suggesting that COX-2 also plays a role in IL-6-induced angiogenesis (Jee et al. 2004). IL-6 also plays important role in tumor progression from benign to malignant, in invasive tumors in the HaCaT model of human skin carcinoma by activating STAT3, and directly stimulates proliferation and migration of the benign non-invasive HaCaT-ras A-5 cells in vitro. Furthermore, IL-6 induces inflammatory and angiogenic factors such as IL-8, GM-CSF, and CSF as well as VEGF and monocyte chemotactic protein-1 (MCP-1) in the tumor cells, leading to tumor cell invasion in organotypic cultures in vitro. Tumor invasion is supported by the IL-6 induced over-expression of MMP-1 in vitro and in vivo, thus demonstrating a key function of IL-6 in the progression of skin SCC by regulating a complex cytokine and protease network (Lederle et al. 2011).
A majority of cancers over-express COX-2, an enzyme responsible for the biosynthesis of PG metabolites. Enhanced production of PGs, and particularly PGE2, has been linked with tumor progression, invasion, and metastasis. Human epidermis actively synthesizes PGs, and previous studies have demonstrated that PGE2 generation can regulate epidermal cell proliferation in vitro. Elevated levels of PGE2 observed in SCC and BCC of the skin may correlate with an increased propensity for metastatic and invasive behavior (Singh and Katiyar 2011).
VEGF is known to be a key regulator of cutaneous angiogenesis and as such plays a role in several physiological and disease processes in the skin, including hair growth, cancer development, and psoriasis as well as wound healing. It has been shown that VEGF is essential for tumor development in multistage models of skin carcinogenesis, and the mechanism of action has been primarily attributed to the induction of angiogenesis (Johnson and Wilgus 2012). VEGFR-1, expressed in mouse and human skin tumor cells and in SCC cell lines, suggests that VEGF could affect tumor cells directly. UV up-regulates VEGF production in keratinocyte-derived cell lines both directly through transcription factor activation and indirectly through cytokine release. VEGF has also been shown to induce the migration of primary keratinocytes in vitro (Zhu et al. 2013).
17.4 Role of Inflammatory Molecules in the Development of Skin Cancer: Evidence from In Vivo Studies
Chemically induced mouse skin tumors using inflammatory agent, 12-O-tetradecanoylphorbol-13-acetate (TPA), for tumor promotion greatly contributed to our understanding of multistage carcinogenesis and have given important insights into the functional interaction between inflammatory microenvironment and epithelial tumor, especially when used in combination with transgenic animals. Data from these and additional new model systems clearly emphasize that the tumor-promoting microenvironment is indispensable for tumor formation and progression.
The two-stage mouse skin carcinogenesis and UV-induced photocarcinogenesis are well established in vivo models for the understanding of the multistage nature of tumor development to design novel therapeutic concepts for human epithelial neoplasia. In two-stage mouse skin model, tumor initiation is accomplished through a single topical application of a carcinogen, typically 7,12-dimethylbenz(a)anthracene (DMBA) that results in an initiated state of the epidermal keratinocytes, which frequently harbor one single genetic mutation (e.g., ras activation) and are more susceptible to subsequent genetic alterations (Mueller 2006). Tumor promotion achieved by repeated treatment with phorbol esters, such as TPA, resulted in benign papillomas, some of which spontaneously progress into malignant SCC. TPA activates a series of PKC isoenzymes and induces a pleiotropic tissue response, resulting in a strong inflammatory reaction (Rundhaug and Fischer 2010).
Tumor promoters, whether UV, chemicals, or endogenous factors, usually interact at the cell surfaces with specific receptors or other cell components that elicit several processes/responses, including enhanced DNA synthesis, increased production of eicosanoids, cytokines and growth factors, a pro-oxidant state, and alterations in cell surface properties, leading to changes in cell adhesion and cell-to-cell communication (Rundhaug and Fischer 2010).
Chronic exposure to UV leads to the up-regulation of COX-2 expression and chronic inflammation along with the accumulation of DNA damage and mutations, all of which combine to induce malignant changes in epidermal keratinocytes and skin cancers (Rundhaug and Fischer 2010). Topical application of a prototype tumor promoter, TPA, induces expression of COX-2 and its mRNA transcript in mouse skin in vivo by activating eukaryotic transcription factors such as NF-κB and AP-1. These in turn are regulated by a series of upstream kinases collectively known as MAP kinases such as ERK, p38 MAPK, and JUN amino-terminal kinase (JNK) (Chun et al. 2006; Kundu et al. 2006), thereby contributing to the inflammatory responses mediated by TPA and in arachidonic acid metabolite production (Kundu et al. 2006). Inappropriate up-regulation of COX-2 also prolongs the survival of malignant or transformed cells and leads to phenotypic changes associated with metastatic potential (Surh et al. 2001). COX-2 also has roles in keratinocyte differentiation, and the absence of COX-2 causes premature terminal differentiation of initiated keratinocytes and reduced tumor formation in DMBA/TPA-induced mouse skin carcinogenesis (Tiano et al. 2002). Increase in COX-2 results in a subsequent increase in the level of PGs, which inappropriately up-regulated in various premalignant and malignant tissues. Elevated levels of some PGs, especially PGE2 and PGF2-α, are functionally related to mouse skin tumor promotion (Furstenberger et al. 1989). Even topical application of a COX-2 product, 15-deoxy-D12,14-prostaglandin J2, has been shown to potentiate DMBA/TPA-induced mouse skin tumorigenesis (Millan et al. 2006), which indicated the important role of COX-2 in tumor promotion in vivo (Kundu et al. 2006). This was also evident by using transgenic mouse model, wherein COX-2 over-expressing transgenic mice (Muller-Decker et al. 2002) are highly susceptible to spontaneous skin tumor formation, while COX-2 knockout animals (Tiano et al. 2002) are less prone to experimentally induced tumorigenesis.
TGFβ1 and TNF-α, which play crucial role in the inflammatory process during wound healing, are the most comprehensively studied pro-inflammatory cytokines in skin carcinogenesis (Urban et al. 1986). TGFβ1 up-regulates PG generation and COX-1 and COX-2 expressions of mast cells and significantly affects skin tumor promotion by paradoxically enhancing epidermal proliferation, besides stimulating inflammation within a developing tumor (Perez-Lorenzo et al. 2010). This was evident by abrogation of TGF-β signaling by knocking out Smad3 (mothers against decapentaplegic homolog 3), which results in resistance to chemical carcinogenesis (Li et al. 2004; Mueller 2006).
TNF-α has been shown to activate neutrophils and mediate the cytotoxic effects of activated macrophages (Urban et al. 1986). The pro-inflammatory effect of TNF-α seems to be important for early stages of tumor promotion. This is evident from the observations, wherein TNF-α-deficient mouse is resistant to the development of benign and malignant skin tumors induced by repeated DMBA exposure or initiation with DMBA and promotion with TPA/okadaic acid. The resistance was associated with a clearly decreased inflammatory response in the dermis of the transgenic animals. Later stages of carcinogenesis were not affected by TNF-α as tumors in wild-type and TNF-α-deficient mice showed similar rates of malignant progression (Scott et al. 2004; Mueller 2006). TNF-α initiates the activation of NF-κB signaling through its receptor, TNFR1, by recruiting the IKK complex and through PKCζ and PI3K/Akt phosphorylation (Martin et al. 2001; Rundhaug and Fischer 2010). NF-κB signaling leads to the induction of a variety of anti-apoptotic factors. Another TNFR1-mediated signaling pathway is the activation of the JNK cascade. The activated JNK phosphorylates the AP-1 transcription factor, leading to transcriptional up-regulation of AP-1-responsive genes, such as GM-CSF, MMP-3, and MMP-9, which are involved in proliferation, differentiation, and apoptosis and promote inflammation and angiogenesis as well as invasion of tumor keratinocytes (Scott et al. 2004; Rundhaug and Fischer 2010).
IL-1 is another important cytokine secreted by monocytes and macrophages, which drive the acute phase of inflammation. Many cell types produce IL-1 after stimulation by microorganisms, cytokines, or other environmental insults. IL-1α activates adjacent cells (or IL-1β on distant cells) to induce the expression of additional pro-inflammatory genes, including IL-6, COX-2, and iNOS (Apte et al. 2006). Various skin tumor promoters induce IL-1α mRNA and protein expression in the epidermis in vivo (Oberyszyn et al. 1993; Lee et al. 1994). Blocking the activity of IL-1α with intradermal injections of a neutralizing antibody inhibits TPA-induced vascular permeability, inflammatory cell infiltration, and epidermal hyperplasia, which demonstrates the central role of IL-1α in mediating these tumor promoter-related events (Lee et al. 1994). Transgenic mice over-expressing IL-1α in basal keratinocytes (K14 promoter) develop spontaneous inflammatory skin lesions, as well as dermal neutrophil infiltration even in non-lesional skin (Groves et al. 1995). Moreover, stable over-expression of antagonist of IL-1 (IL-1Ra) in mouse skin carcinoma cell line results in down-regulated COX-2 expression and slower in vitro and in vivo growth. These results indicate that IL-1 is contributing to malignant cell proliferation (Rundhaug and Fischer 2010). IL-12 and IL-23 also play role in skin tumorigenesis, wherein IL-12 acts as a tumor suppressor by inducing immune surveillance and IL-23 promotes skin tumorigenesis by driving inflammation and reducing immune surveillance. While IL-12p35-null mice develop papillomas earlier and more frequently than wild-type mice, IL-23p19-null mice, as well as p40-null mice, are resistant to DMBA/TPA induction of skin tumorigenesis (Langowski et al. 2006). In addition, IL-12p35- and IL-12p40-null mice are more sensitive to UV-induced skin carcinogenesis, with reduced repair of UV-induced DNA damage, increased number of tumors per mouse, more rapid growth, and greater malignant potential than wild-type mice. UV-induced tumors from IL-12p35-null mice also have increased angiogenesis and up-regulated expression of pro-inflammatory IL-6 and IL-23 (Meeran et al. 2007). Thus, IL-12 counteracts UV-induced immunosuppression, inflammation, and skin carcinogenesis.
Proteinases such as MMP-2 and MMP-9, provided by mast cells as well as granulocyte neutrophils in inflammatory microenvironment, play important roles as regulators of development, angiogenesis, and tumor progression. The essential role of stromal MMP-9 for tumor development in K14-HPV16 transgenic mice showed that mice deficient for MMP-9 resulted in decreased tumor incidence (Coussens et al. 1996). In addition, lack of MMP-9 was associated with delayed activation of angiogenesis in the stroma of the lesions (Mueller 2006). In another study, it has been shown that MMP-9 expressed by inflammatory cells is functionally involved in distinct processes of epithelial carcinogenesis such as regulation of oncogene-induced keratinocyte hyperproliferation, progression to invasive cancer, and end-stage malignancy (Coussens et al. 2000).
17.5 Evidence from Patients for the Role of Inflammation in Skin Cancer
The association between chronic inflammation and cancer including epithelial skin tumors was illustrated by epidemiologic and clinical studies for years (Lu et al. 2006). One of the earliest descriptions for the relationship between chronic inflammation and epithelial skin tumors is Marjolin’s ulcer, which describes a relatively uncommon ulcerative condition associated with a thermal injury in which malignant transformation occurs within a chronic inflammatory focus. Various other similar associations have been observed for lupus erythematosus, leg ulcerations, osteomyelitis, perineal inflammatory disease, ulcerative lichen planus, and epidermolysis bullosa, where SCC development with inflammatory disorders had been seen in non-healing wounds. Inflammation also plays an important role in skin cancer progression. It is evident in a study, where progression of AK to SCC preceded by a short inflammatory phase in the AK. This is paralleled by an increase in the number of cells expressing detectable levels of p53 and Bcl-2 and a decrease in the number of cells expressing FasL, suggesting increasing resistance to cell cycle arrest and apoptosis (Mueller 2006).
It is established knowledge that there may be a mild-to-moderate chronic inflammatory cell infiltrate at the periphery of the tumors. In the cohort study of patients with head and neck cutaneous SCC, a dense infiltrate of lymphocytes was found in the dermis in 84/315 index tumors. Notably, the proportion of the presence of this infiltrate was significantly higher in those tumors that recurred (Kyrgidis et al. 2010). Moreover, peri-neoplastic inflammation in intraepithelial SCC is pronounced both in immune-competent patients and in organ transplant recipients (OTRs). Inflammation increases further in invasive SCC. OTRs show reduced proportions of regulatory T cells and CD123+ plasmacytoid dendritic cells. This distinct inflammatory infiltrate may result in the increased cutaneous carcinogenesis and more aggressive behavior of SCC in OTRs (Muhleisen et al. 2009).
In response to systemic inflammation, and in particular to elevated IL-6 levels, the liver produces C-reactive protein (CRP) used as a marker of systemic inflammation, which binds to dead or dying cells to activate the complement system. Elevated CRP concentration increases the risk for “all-cause” mortality compared to other subjects (Marsik et al. 2008). Cancer patients with highly elevated CRP showed increased mortality by a factor of 28, which confirms correlation between cancer progression and inflammation. Mikirova et al. (2012) observed that twenty-eight out of forty-five subjects had sharply elevated CRP levels in cancer patients, suggesting that inflammation is a prevalent problem for cancer patients. This is especially important since other reports indicate that inflammation, particularly elevated CRP, is a marker of a poor prognosis (St Sauver et al. 2009). They also observed higher level of pro-inflammatory cytokines IL-1α, IL-2, IL-8, TNF-α, chemokine eotaxin, which were reduced after treatment for vitamin C (Mikirova et al. 2012).
Prostaglandins generated by the arachidonic acid cascade particularly PGE2 have been involved in various models for tumorigenesis (Vanderveen et al. 1986). Squamous cell skin cancer appears to link with chronic activation of the PG biosynthetic pathway resulting from recurrent UVB exposure. In the series of tumor biopsies evaluated, COX-2 was highly expressed in SCC within the overlying sun-exposed epidermis as well as within the tumor nests. Positive staining was also observed within the endothelium and smooth muscle layers of the blood vessels and infiltrative macrophages of SCC biopsies (Buckman et al. 1998).
Taken together, the association of inflammation with enhanced tumor formation and tumor progression has been supported by a large number of clinical studies; however, these studies do not allow any insight in the cellular and molecular mechanisms that lie at the basis of the tumor and progression-promoting effect of inflammation in epithelial skin cancers.
17.6 Inhibitors of Inflammation for the Prevention and Treatment of Skin Cancer
Evidence suggests that inflammation is causally linked to carcinogenesis (Balkwill and Coussens 2004). COX-2, the rate-limiting enzyme in arachidonic acid metabolism leading to PG synthesis, is up-regulated in murine and human NMSC. Inhibition of COX-2 by biochemical inhibitors or genetic deletion decreases chemical- or UV-induced skin tumor development (Wright et al. 2006). A number of animal models have shown that inhibition of COX-2 helps prevent skin cancer, including UVR-induced skin carcinogenesis and two-stage skin carcinogenesis model in mice.
17.6.1 Non-steroidal Anti-inflammatory Drugs (NSAIDs)
Drugs of this class include celecoxib, diclofenac, indomethacin, sulindac, aspirin, and ibuprofen. They act by repressing prostaglandin biosynthesis through inhibition of COX (Bode and Dong 2000). The expression of COX-2 is linked to excessive activation of intracellular signal transduction pathways comprising proline-directed serine/threonine kinases and their downstream transcription factors. There is an important relation between MAPK signaling and COX-2 expression, which further supports the idea that agents modulating MAPK signaling pathways can be effective in chemoprevention of skin cancer (Shrotriya et al. 2010).
Celecoxib, a COX-2 inhibitor, decreases macrophage and neutrophil infiltration into skin tumors, as well as inflammation induced by 50 Gy radiation (Liang et al. 2003). Celecoxib at the doses, determined to be equivalent to twice-daily doses in humans, was effective at increasing tumor latency and decreasing multiplicity in hairless mice exposed to UVR. This study showed a decrease in PG synthesis in the epidermis, as well as a statistically significant decrease in tumor yield (Fischer et al. 1999). Oral or topical administration of celecoxib has been reported to prevent new tumor formation after the onset of UV-induced photocarcinogenesis in hairless mice (Wilgus et al. 2003), while also suppressing PGE2 production induced by UVB. Such sensitization appears to be mediated through inhibition of AP-1, JNK, and p38 signaling pathways. In DMBA-initiated/TPA-promoted female ICR mouse skin, application of celecoxib also significantly reduced the multiplicity of papillomas, which was associated with decreased expression of COX-2 and VEGF, as well as inhibition of CCAAT (cytidine–cytidine–adenosine–adenosine–thymidine)/C/EBP (enhancer binding protein) activation (Chun et al. 2006). Oral administration of celecoxib is also effective in the prevention of SCC and BCC in individuals who have extensive actinic damage and are at high risk for the development of NMSC (Elmets et al. 2010).
Topical application of etodolac one week prior to and after the tumor initiation resulted in a significant delay of the tumor induction and inhibition of the tumor burden as well as multiplicity in the DMBA/TPA-induced skin tumorigenesis in ICR mouse. Treatment with oxyphenbutazone in drinking water increased the tumor latency period and decreased the tumor incidence as well as tumor burden in the peroxynitrite-induced/TPA-promoted skin tumors in the HOS-HR-1-specific pathogen-free mice (Kapadia et al. 2010).
The prototypical COX inhibitor, aspirin, blocks enzymatic activity covalently through the acetylation of Ser-530 in COX-1 and Ser-516 in COX-2 (Wennogle et al. 1995). Aspirin inhibits both UVC- and UVB-induced AP-1 activity in a dose-dependent manner, when the cells are treated with aspirin or before exposure to UVR. The inhibition of UVB-induced AP-1 activity appears to mediate through their ability to block the activation of ERKs, JNKs, and P38 kinases, whereas the inhibitory effect on UVC-induced AP-1 activity seems to be mediated only through the inhibition of JNKs. In the skin of AP-1/luciferase transgenic mice, topical pretreatment of mouse skin with aspirin blocked the UVB-induced AP-1 transactivation in vivo (Huang et al. 1997).
Topical application of indomethacin reduced skin tumor development by ~30 % in the DMBA/TPA-induced mouse skin tumorigenesis (Slaga et al. 1977). Indomethacin has also been shown to reduce photocarcinogenesis in mice and when administered through diet led to the decrease in tumor yield by 78 % in UV-induced skin tumor development in SKH:HR-1 hairless mice and also blocked PG synthesis in the epidermis (Fischer et al. 1999).
Diclofenac, a non-selective NSAID, is widely used in the treatment of AK. In a study of 32 organ transplant recipients with 3 or more AK, patients randomized to twice-daily treatment with 3 % diclofenac showed decrease in lesions and no patients in the diclofenac group had developed SCC in the treated areas. Thus, diclofenac may prevent the cancerous transformation of AK (Ulrich et al. 2010).
Sulindac is NO-releasing NSAIDs, which when synthesized reduces gastrointestinal and cardiovascular toxicities of NSAIDs and possess anti-proliferative, pro-apoptotic, and anti-cancer activities. In the skin, topical application of sulindac reduces UVB-induced cutaneous phototoxicity and significantly decreased the development of UVB-induced skin tumor in SKH-1 hairless mice, as indicated by a substantial reduction in tumor number and tumor volume. The inhibitory effect was corroborated by increase in Bax:Bcl-2 ratio and the expression of pro-apoptotic BCL-2-associated X protein (Bax), decrease in anti-apoptotic Bcl-2 expression indicating increased apoptosis, and reduced cell proliferation as evident by decreased expression of proliferating cell nuclear antigen (PCNA) and cyclin D1. Sulindac diminished UVB-induced inflammatory responses as observed by a remarkable reduction in the levels of phosphorylated MAPK such as ERK1/2, p38, and JNK1/2. It also inhibited NF-κB by enhancing IκBα as evidenced by the reduced expression of iNOS and COX-2, the direct NF-κB transcription target proteins. Moreover, sulindac also significantly reduced the progression of benign lesions to invasive carcinomas by suppressing the tumor aggressiveness and retarding epithelial–mesenchymal transition. Thus, sulindac is a potent inhibitor of UVB-induced and chemically induced skin carcinogenesis and acts by targeting proliferation regulatory pathways (Kim et al. 2006; Chaudhary et al. 2013).
17.6.2 Naturally Occurring Plant Products
Dietary polyphenols which are widely present in fruits, vegetables, dry legumes, and beverages (such as tea, coffee, juice, wine, beer) have gained considerable attention for the prevention of UV-induced skin photodamage including the risk of skin cancer. Experimental and epidemiologic studies have suggested that polyphenols protect the skin from the adverse effects of UV radiation. Polyphenols have been shown to (a) scavenge radical species such as ROS/RNS, e.g., O2 −, H2O2, OH•, ONOO−; (b) suppress ROS/RNS formation by inhibiting some enzymes or chelating trace metals involved in free radical production; and (c) up-regulate or protect antioxidant defense (Patel et al. 2007).
Oral administration of green tea polyphenols (GTPs) to SKH-1 hairless mice resulted in significant inhibition of UVR-induced cutaneous edema, erythema, and bifold skin thickness (a biomarker of inflammation). Administration of GTPs in drinking water decreased COX-2, PGE2, PCNA, and cyclin D1 and also significantly reduced the levels of various pro-inflammatory cytokines in chronically UVB-exposed skin/skin tumors of mice (Meeran et al. 2009). Topical treatment with GTPs prior to UV exposure reduced the UV-induced hyperplastic response, myeloperoxidase (MPO) activity, and the numbers of infiltrating inflammatory leukocytes in the skin (Afaq et al. 2003). Moreover, similar administration of both agents in the untanned backs of humans resulted in significantly less development of erythema as compared to the UV-irradiated skin that was not treated with GTPs (Katiyar et al. 2001). Topical application of EGCG, an active constituent of green tea, in mice and humans, resulted in the inhibition of UVB-induced production of PG metabolites (PGE2, PGF2-α, and PGD2), which play a critical role in inflammatory disorders, free radical generation, proliferative skin diseases, and skin tumor promotion (Katiyar et al. 2001; Katiyar and Mukhtar 2001). The inhibitory effects of GTPs on these biomarkers of inflammation in UV-exposed skin provide mechanistic evidence of the anti-carcinogenic effects of GTPs. Studies have also shown that topical pretreatment with polymeric black tea polyphenols in Swiss bare mouse skin decreased TPA-induced inflammatory protein (COX-2) and cellular proliferation through decreasing activation of cellular kinases (JNK, ERK, p38, and Akt) and transcription factors (AP-1 and NF-κB) as well as apoptosis (Patel et al. 2008). The above in vivo observations generated using both animal and human systems provide insights into the possible protective mechanisms involved in the anti-initiating and/or anti-inflammatory effects of tea polyphenols.
Dietary intake or topical treatment of silymarin as well as resveratrol in UVR-exposed mice also resulted in similar inhibitory effects in terms of inflammation-related biomarkers as observed with GTPs (Gu et al. 2007). These products also inhibited the expression of ornithine decarboxylase (ODC), an enzyme required for polyamine biosynthesis, which has a role in tumor promotion in UVB-exposed skin. Moreover, topical pretreatment with resveratrol in mouse skin is reported to inhibit the TPA-induced (a) AP-1 (c-jun and c-fos) via modulation of p38 and JNK; (b) nuclear translocation of p65 and subsequent DNA binding of NF-κB by blocking the degradation of IκBα; (c) phosphorylation of p65 and its interaction with CREB-binding protein (CBP)/p300, rendering NF-κB transcriptionally inactive; and (d) mRNA levels of COX-1, COX-2, c-myc, c-fos, c-Jun, TGF-β1, and TNF-α and protein levels of COX-2 (Jang and Pezzuto 1999; Kundu et al. 2006). Topical application of rosemary was observed to decrease TPA-induced tumor promotion through inhibition of hyperplasia, ODC activity, and inflammatory responses (Osakabe et al. 2004).
Bromelain derived from pineapple, when applied topically, resulted in delay in onset and thereby inhibition of tumor development in DMBA-initiated/TPA-promoted skin tumors in female Swiss albino mice. The mechanism involved in anti-carcinogenic activity is underlined by induction of p53, shift in Bax/Bcl-2 ratio, induction of caspases, decrease in COX-2 expression, and inhibition of NF-κB pathway by regulating MAPK and Akt/PKB pathways (Bhui et al. 2009). Pretreatment with oligonol has been shown to significantly inhibit the expression of COX-2 in skin papillomas and carcinomas in DMBA/TPA-induced skin carcinogenesis (Kundu et al. 2009).
Administration of polyphenol fraction from dried fruits of Crataegus pinnatifida (CF-TP), diallyl trisulfide (DATS), organosulfur compounds from garlic, and D-limonene exhibited an inhibitory effect on DMBA/TPA-mediated mouse skin tumorigenesis. These effects are evidenced by reduction in TPA-mediated inflammatory responses (edema, hyperplasia, COX-2, iNOS expression), activation of ODC, and oxidative stress, which were attributed to the inhibition of Ras/Raf/ERK1/2 signaling pathway, blockade of AP-1 activation via downregulation of upstream Akt and JNK signaling pathways, and promotion to pro-apoptotic state (Chaudhary et al. 2012; Shrotriya et al. 2010). Moreover, CF-TP inhibited the activation of NF-κB and AP-1 induced by TPA in JB6 P+ cells as well as benzo[a]pyrene (B[a]P)/TPA-induced skin tumor formation and decreased the incidence of tumor. CF-TP also suppressed TPA-induced MPO activation, which is used as a marker to quantitate the extent to which leukocytes that have infiltrated into the dermis produce reactive oxygen intermediates in response to topical stimuli (Kao et al. 2007). Apigenin exerts chemopreventive effects on UVB-induced COX-2 and skin inflammation in JB6 P+ mouse epidermal cells and SKH-1 hairless mice by directly suppressing Src kinase activity (Byun et al. 2013).
Topical application of euphol isolated from the roots of Euphorbia kansui markedly inhibited TPA-induced ear edema and skin inflammation in DMBA/TPA-treated male CD 1 mice (Yasukawa et al. 2000). Euphol also inhibited activation of downstream signaling proteins, namely PKC and MAPKs, which in turn decreased the levels of CXC chemokines and COX-2, following topical application of TPA. Thus, euphol exhibits strong topical anti-inflammatory actions on mouse ear through a mechanism that involves its ability to regulate PKC and ERK activation, resulting in reduced COX-2, MIP-2, and CXCL1/KC up-regulation and leukocyte infiltration (Passos et al. 2013).
Female Swiss albino mice pretreated topically with geraniol (GOH) prior to TPA administration significantly inhibited TPA-induced lipid peroxidation (LPO), inflammatory responses, pro-inflammatory cytokine release, reduced glutathione (GSH) content, and the activity of different antioxidant enzymes. GOH attenuated early tumor promotional changes through TPA-induced altered expression of NF-κB (p65) and COX-2 and inhibited TPA-induced altered activity of p38 MAPK. GOH also effectively suppresses the production of the TNF-α, IL-1β, and IL-6 cytokines (Khan et al. 2013).
Topical treatment of UVB-induced mice with honokiol, magnolol, or silibinin decreased tumor multiplicity and volume. These effects are corroborated by decrease in the UVB-induced expression of markers of inflammation and proliferation, e.g., COX-2, PGE2, PCNA, cyclins, Cdc25B, and associated Cdks (2, 4, 6) besides phosphorylation and nuclear translocation of STAT3 (Tyr 705, Ser536) and NF-κB/its DNA-binding activity, which are potential upstream regulators of iNOS and COX-2 in the skin/skin tumors of mice. Moreover, these products increased the levels of CDK-interacting protein 1 (Cip)/p21, Kip/p27, cleavage of caspase-8, and poly-ADP-ribose polymerase (PARP) by inhibiting the levels of PI3K and the phosphorylation of Akt (Mallikarjuna et al. 2004; Vaid et al. 2010; Chilampalli et al. 2011). Treatment with honokiol also significantly inhibited UVB-induced expression of pro-inflammatory cytokines, such as TNF-α, IL-1β, and IL-6, in the mouse skin/skin tumors and that may have contributed in the inhibition of tumor development (Vaid et al. 2010). Topical pretreatment with delphinidin inhibits the UVB-induced MAPKK and PI3K activity directly to suppress COX-2 over-expression in mouse skin (Kwon et al. 2009).
Caffeine is effective in inhibiting the UVB-induced AKT/COX-2 pathway independent of ATR in human HaCaT keratinocyte, which results in the induction of UVB-induced apoptosis. Blocking the AKT/COX-2 signaling by caffeine specifically eliminates UVB-damaged keratinocytes without complete DNA repair through apoptosis (Han et al. 2011).
Benzene fraction of Selaginella bryopteris inhibited the expression of the inflammatory cytokines IL-8, IL-1β, and TNF-α in methyl isocyanate-stimulated HEK-293 cells. In a parallel study involving a two-stage protocol of DMBA/croton oil-induced skin carcinogenesis, oral administration of the flavonoid-rich benzene fraction of S. bryopteris prior to croton oil application caused significant reduction in tumor incidence and multiplicity with significant delay in the latency period, providing evidence to the effect of polyphenolic flavonoids as anti-carcinogenic and/or anti-tumor-promoting agents (Mishra et al. 2011).
Collectively, the results concerning the inhibitory effects of these naturally occurring plant products on UV- and phorbol ester-induced inflammatory responses revealed that anti-carcinogenic activity of naturally occurring plant products is mediated in part through their anti-inflammatory effects.
17.7 Conclusions and Future Directions
Melanoma and non-melanoma skin cancers are among the most prevalent cancers in human. Epidemiological and experimental evidence suggests “chronic inflammation” to be one of the hallmarks in solar UVR and several other environmental agent-mediated skin cancers. The identification of transcription factors, i.e., NF-κB, STAT3, and HIF-1α, and their gene products, i.e., COX-2, cytokines, chemokines, and chemokine receptors, suggests critical role of inflammation in skin carcinogenesis. Considering the potential role of inflammation in initiation and its major as well as convincing role in promotion, progression as well as tumor angiogenesis and metastasis, inflammatory pathways may become attractive targets for skin cancer prevention. Efforts to prevent or minimize the exposure to known skin carcinogens and ongoing studies on evaluating the role of various pro-inflammatory mediators in carcinogenesis and assessing them as potential targets for chemoprevention of skin cancers need to be enhanced/encouraged.
References
Afaq F, Ahmad N, Mukhtar H (2003) Suppression of UVB-induced phosphorylation of mitogen-activated protein kinases and nuclear factor kappa B by green tea polyphenol in SKH-1 hairless mice. Oncogene 22(58):9254–9264. doi:10.1038/sj.onc.1207035
Aggarwal BB, Vijayalekshmi RV, Sung B (2009) Targeting inflammatory pathways for prevention and therapy of cancer: short-term friend, long-term foe. Clin Cancer Res: Official J Am Assoc Cancer Res 15(2):425–430. doi:10.1158/1078-0432.CCR-08-0149
American Cancer Society (2013) Cancer facts and figures 2013. American Cancer Society, Atlanta
Ansari KM, Rundhaug JE, Fischer SM (2008) Multiple signaling pathways are responsible for prostaglandin E2-induced murine keratinocyte proliferation. Mol Cancer Res 6(6):1003–1016. doi:10.1158/1541-7786.MCR-07-2144
Apte RN, Krelin Y, Song X, Dotan S, Recih E, Elkabets M, Carmi Y, Dvorkin T, White RM, Gayvoronsky L, Segal S, Voronov E (2006) Effects of micro-environment- and malignant cell-derived interleukin-1 in carcinogenesis, tumour invasiveness and tumour-host interactions. Eur J Cancer 42(6):751–759. doi:10.1016/j.ejca.2006.01.010
Arsenault D, Lucien F, Dubois CM (2012) Hypoxia enhances cancer cell invasion through relocalization of the proprotein convertase furin from the trans-Golgi network to the cell surface. J Cell Physiol 227(2):789–800. doi:10.1002/jcp.22792
Aziz SA, Hussain KS, Ahmad KN, Ahmed M, Kharadi MY, Bhat JR (1998) Profile of Kangari cancer: a prospective study. Burns: J Int Soc Burn Injuries 24(8):763–766
Balkwill F, Coussens LM (2004) Cancer: an inflammatory link. Nature 431(7007):405–406. doi:10.1038/431405a
Barthel SR, Gavino JD, Descheny L, Dimitroff CJ (2007) Targeting selectins and selectin ligands in inflammation and cancer. Expert Opin Ther Targets 11(11):1473–1491. doi:10.1517/14728222.11.11.1473
Bell S, Degitz K, Quirling M, Jilg N, Page S, Brand K (2003) Involvement of NF-kappaB signalling in skin physiology and disease. Cell Signal 15(1):1–7
Bhui K, Prasad S, George J, Shukla Y (2009) Bromelain inhibits COX-2 expression by blocking the activation of MAPK regulated NF-kappa B against skin tumor-initiation triggering mitochondrial death pathway. Cancer Lett 282(2):167–176. doi:10.1016/j.canlet.2009.03.003
Bode AM, Dong Z (2000) Signal transduction pathways: targets for chemoprevention of skin cancer. Lancet Oncol 1:181–188
Boffetta P, Gridley G, Lindelof B (2001) Cancer risk in a population-based cohort of patients hospitalized for psoriasis in Sweden. J Invest Dermatol 117(6):1531–1537. doi:10.1046/j.0022-202x.2001.01520.x
Brummelkamp TR, Nijman SM, Dirac AM, Bernards R (2003) Loss of the cylindromatosis tumour suppressor inhibits apoptosis by activating NF-kappaB. Nature 424(6950):797–801. doi:10.1038/nature01811
Buckman SY, Gresham A, Hale P, Hruza G, Anast J, Masferrer J, Pentland AP (1998) COX-2 expression is induced by UVB exposure in human skin: implications for the development of skin cancer. Carcinogenesis 19(5):723–729
Byun S, Park J, Lee E, Lim S, Yu JG, Lee SJ, Chen H, Dong Z, Lee KW, Lee HJ (2013) Src kinase is a direct target of apigenin against UVB-induced skin inflammation. Carcinogenesis 34(2):397–405. doi:10.1093/carcin/bgs358
Cataisson C, Salcedo R, Hakim S, Moffitt BA, Wright L, Yi M, Stephens R, Dai RM, Lyakh L, Schenten D, Yuspa HS, Trinchieri G (2012) IL-1R-MyD88 signaling in keratinocyte transformation and carcinogenesis. J Exp Med 209(9):1689–1702. doi:10.1084/jem.20101355
Chaudhary SC, Siddiqui MS, Athar M, Alam MS (2012) D-Limonene modulates inflammation, oxidative stress and Ras-ERK pathway to inhibit murine skin tumorigenesis. Hum Exp Toxicol 31(8):798–811. doi:10.1177/0960327111434948
Chaudhary SC, Singh T, Kapur P, Weng Z, Arumugam A, Elmets CA, Kopelovich L, Athar M (2013) Nitric oxide-releasing sulindac is a novel skin cancer chemopreventive agent for UVB-induced photocarcinogenesis. Toxicol Appl Pharmacol 268(3):249–255. doi:10.1016/j.taap.2012.12.009
Chilampalli C, Guillermo R, Zhang X, Kaushik RS, Young A, Zeman D, Hildreth MB, Fahmy H, Dwivedi C (2011) Effects of magnolol on UVB-induced skin cancer development in mice and its possible mechanism of action. BMC Cancer 11:456. doi:10.1186/1471-2407-11-456
Chun KS, Kundu JK, Park KK, Chung WY, Surh YJ (2006) Inhibition of phorbol ester-induced mouse skin tumor promotion and COX-2 expression by celecoxib: C/EBP as a potential molecular target. Cancer Res Treat: Official J Korean Cancer Assoc 38(3):152–158. doi:10.4143/crt.2006.38.1.152
Chung JH, Youn SH, Koh WS, Eun HC, Cho KH, Park KC, Youn JI (1996) Ultraviolet B irradiation-enhanced interleukin (IL)-6 production and mRNA expression are mediated by IL-1 alpha in cultured human keratinocytes. J Invest Dermatol 106(4):715–720
Colotta F, Allavena P, Sica A, Garlanda C, Mantovani A (2009) Cancer-related inflammation, the seventh hallmark of cancer: links to genetic instability. Carcinogenesis 30(7):1073–1081. doi:10.1093/carcin/bgp127
Costin GE, Hearing VJ (2007) Human skin pigmentation: melanocytes modulate skin color in response to stress. FASEB J: Official Publ Fed Am Soc Exp Biol 21(4):976–994. doi:10.1096/fj.06-6649rev
Coussens LM, Hanahan D, Arbeit JM (1996) Genetic predisposition and parameters of malignant progression in K14-HPV16 transgenic mice. Am J Pathol 149(6):1899–1917
Coussens LM, Tinkle CL, Hanahan D, Werb Z (2000) MMP-9 supplied by bone marrow-derived cells contributes to skin carcinogenesis. Cell 103(3):481–490
Crespo P, Leon J (2000) Ras proteins in the control of the cell cycle and cell differentiation. Cell Mol Life Sci: CMLS 57(11):1613–1636
Del Prete A, Allavena P, Santoro G, Fumarulo R, Corsi MM, Mantovani A (2011) Molecular pathways in cancer-related inflammation. Biochemia Med: Casopis Hrvatskoga Drus Medicinskih Biokemicara/HDMB 21(3):264–275
Dhawan P, Richmond A (2002) Role of CXCL1 in tumorigenesis of melanoma. J Leukoc Biol 72(1):9–18
Dong KK, Damaghi N, Picart SD, Markova NG, Obayashi K, Okano Y, Masaki H, Grether-Beck S, Krutmann J, Smiles KA, Yarosh DB (2008) UV-induced DNA damage initiates release of MMP-1 in human skin. Exp Dermatol 17(12):1037–1044. doi:10.1111/j.1600-0625.2008.00747.x
Elmets CA, Viner JL, Pentland AP, Cantrell W, Lin HY, Bailey H, Kang S, Linden KG, Heffernan M, Duvic M, Richmond E, Elewski BE, Umar A, Bell W, Gordon GB (2010) Chemoprevention of nonmelanoma skin cancer with celecoxib: a randomized, double-blind, placebo-controlled trial. J Natl Cancer Inst 102(24):1835–1844. doi:10.1093/jnci/djq442
Fan Y, Mao R, Yang J (2013) NF-κB and STAT3 signaling pathways collaboratively link inflammation to cancer. Protein Cell 4(3):176–185. doi:10.1007/s13238-013-2084-3
Farshchian M, Kivisaari A, Ala-Aho R, Riihila P, Kallajoki M, Grenman R, Peltonen J, Pihlajaniemi T, Heljasvaara R, Kahari VM (2011) Serpin peptidase inhibitor clade A member 1 (SerpinA1) is a novel biomarker for progression of cutaneous squamous cell carcinoma. Am J Pathol 179(3):1110–1119. doi:10.1016/j.ajpath.2011.05.012
Fischer SM, Lo HH, Gordon GB, Seibert K, Kelloff G, Lubet RA, Conti CJ (1999) Chemopreventive activity of celecoxib, a specific cyclooxygenase-2 inhibitor, and indomethacin against ultraviolet light-induced skin carcinogenesis. Mol Carcinog 25(4):231–240
Flockhart RJ, Diffey BL, Farr PM, Lloyd J, Reynolds NJ (2008) NFAT regulates induction of COX-2 and apoptosis of keratinocytes in response to ultraviolet radiation exposure. FASEB J: Official Publ Fed Am Soc Exp Biol 22(12):4218–4227. doi:10.1096/fj.08-113076
Fu J, Bassi DE, Zhang J, Li T, Nicolas E, Klein-Szanto AJ (2012) Transgenic overexpression of the proprotein convertase furin enhances skin tumor growth. Neoplasia 14(4):271–282
Furstenberger G, Gross M, Marks F (1989) Eicosanoids and multistage carcinogenesis in NMRI mouse skin: role of prostaglandins E and F in conversion (first stage of tumor promotion) and promotion (second stage of tumor promotion). Carcinogenesis 10(1):91–96
Groves RW, Allen MH, Ross EL, Ahsan G, Barker JN, MacDonald DM (1993) Expression of selectin ligands by cutaneous squamous cell carcinoma. Am J Pathol 143(4):1220–1225
Groves RW, Mizutani H, Kieffer JD, Kupper TS (1995) Inflammatory skin disease in transgenic mice that express high levels of interleukin 1 alpha in basal epidermis. Proc Natl Acad Sci USA 92(25):11874–11878
Gu M, Singh RP, Dhanalakshmi S, Agarwal C, Agarwal R (2007) Silibinin inhibits inflammatory and angiogenic attributes in photocarcinogenesis in SKH-1 hairless mice. Cancer Res 67(7):3483–3491. doi:10.1158/0008-5472.CAN-06-3955
Haghnegahdar H, Du J, Wang D, Strieter RM, Burdick MD, Nanney LB, Cardwell N, Luan J, Shattuck-Brandt R, Richmond A (2000) The tumorigenic and angiogenic effects of MGSA/GRO proteins in melanoma. J Leukoc Biol 67(1):53–62
Han W, Ming M, He YY (2011) Caffeine promotes ultraviolet B-induced apoptosis in human keratinocytes without complete DNA repair. J Biol Chem 286(26):22825–22832. doi:10.1074/jbc.M111.222349
Han YP, Tuan TL, Wu H, Hughes M, Garner WL (2001) TNF-alpha stimulates activation of pro-MMP2 in human skin through NF-(kappa) B mediated induction of MT1-MMP. J Cell Sci 114(Pt 1):131–139
Hanahan D, Weinberg RA (2011) Hallmarks of cancer: the next generation. Cell 144(5):646–674. doi:10.1016/j.cell.2011.02.013
Hocker TL, Singh MK, Tsao H (2008) Melanoma genetics and therapeutic approaches in the 21st century: moving from the benchside to the bedside. J Invest Dermatol 128(11):2575–2595. doi:10.1038/jid.2008.226
Hu J, Haseebuddin M, Young M, Colburn NH (2005) Suppression of p65 phosphorylation coincides with inhibition of IκBα polyubiquitination and degradation. Mol Carcinog 44(4):274–284. doi:10.1002/mc.20142
Hua H, Li M, Luo T, Yin Y, Jiang Y (2011) Matrix metalloproteinases in tumorigenesis: an evolving paradigm. Cell Mol Life Sci: CMLS 68(23):3853–3868. doi:10.1007/s00018-011-0763-x
Huang C, Ma WY, Hanenberger D, Cleary MP, Bowden GT, Dong Z (1997) Inhibition of ultraviolet B-induced activator protein-1 (AP-1) activity by aspirin in AP-1-luciferase transgenic mice. J Biol Chem 272(42):26325–26331
IARC (1987) Overall evaluations of carcinogenicity. An updating IARC monographs, vols 1–42. IARC monographs evaluation carcinogenic risk chemicals humans, Suppl 7, Lyon
IARC (2007) Molecular mechanisms of HPV-induced carcinogenesis. Monograoh on human papilloma virus, vol 90. IARC monographs evaluation carcinogenic risk chemicals humans, Lyon, pp 432–465
Ibanez IL, Notcovich C, Policastro LL, Duran H (2011) Reactive oxygen species in the biology of melanoma. Breakthroughs in Melanoma Research. InTech
Jang M, Pezzuto JM (1999) Cancer chemopreventive activity of resveratrol. Drugs Exp Clin Res 25(2–3):65–77
Jee SH, Chu CY, Chiu HC, Huang YL, Tsai WL, Liao YH, Kuo ML (2004) Interleukin-6 induced basic fibroblast growth factor-dependent angiogenesis in basal cell carcinoma cell line via JAK/STAT3 and PI3-kinase/Akt pathways. J Invest Dermatol 123(6):1169–1175. doi:10.1111/j.0022-202X.2004.23497.x
Johnson KE, Wilgus TA (2012) Multiple roles for VEGF in non-melanoma skin cancer: angiogenesis and beyond. J Skin Cancer 2012:483. doi:10.1155/2012/483439
Kamp DW, Shacter E, Weitzman SA (2011) Chronic inflammation and cancer: the role of the mitochondria. Oncology (Williston Park) 25(5):400–410, 413
Kao ES, Wang CJ, Lin WL, Chu CY, Tseng TH (2007) Effects of polyphenols derived from fruit of Crataegus pinnatifida on cell transformation, dermal edema and skin tumor formation by phorbol ester application. Food Chem Toxicol: Int J Publ Br Ind Biol Res Assoc 45(10):1795–1804. doi:10.1016/j.fct.2007.03.016
Kapadia GJ, Azuine MA, Shigeta Y, Suzuki N, Tokuda H (2010) Chemopreventive activities of etodolac and oxyphenbutazone against mouse skin carcinogenesis. Bioorg Med Chem Lett 20(8):2546–2548. doi:10.1016/j.bmcl.2010.02.093
Katerinaki E, Evans GS, Lorigan PC, MacNeil S (2003) TNF-α increases human melanoma cell invasion and migration in vitro: the role of proteolytic enzymes. Br J Cancer 89(6):1123–1129. doi:10.1038/sj.bjc.6601257
Katiyar SK, Afaq F, Perez A, Mukhtar H (2001) Green tea polyphenol (−)-epigallocatechin-3-gallate treatment of human skin inhibits ultraviolet radiation-induced oxidative stress. Carcinogenesis 22(2):287–294
Katiyar SK, Mukhtar H (2001) Green tea polyphenol (−)-epigallocatechin-3-gallate treatment to mouse skin prevents UVB-induced infiltration of leukocytes, depletion of antigen-presenting cells, and oxidative stress. J Leukoc Biol 69(5):719–726
Kerkelä E, Ala-Aho R, Lohi J, Grénman R, Saarialho-Kere U (2001) Differential patterns of stromelysin-2 (MMP-10) and MT1-MMP (MMP-14) expression in epithelial skin cancers. Br J Cancer 84(5):659–669. doi:10.1054/bjoc.2000.1634
Khan AQ, Khan R, Qamar W, Lateef A, Rehman MU, Tahir M, Ali F, Hamiza OO, Hasan SK, Sultana S (2013) Geraniol attenuates 12-O-tetradecanoylphorbol-13-acetate (TPA)-induced oxidative stress and inflammation in mouse skin: Possible role of p38 MAP Kinase and NF-kappaB. Exp Mol Pathol 94(3):419–429. doi:10.1016/j.yexmp.2013.01.006
Kim DJ, Prabhu KS, Gonzalez FJ, Peters JM (2006) Inhibition of chemically induced skin carcinogenesis by sulindac is independent of peroxisome proliferator-activated receptor-beta/delta (PPARbeta/delta). Carcinogenesis 27(5):1105–1112. doi:10.1093/carcin/bgi346
Kundu JK, Hwang DM, Lee JC, Chang EJ, Shin YK, Fujii H, Sun B, Surh YJ (2009) Inhibitory effects of oligonol on phorbol ester-induced tumor promotion and COX-2 expression in mouse skin: NF-kappaB and C/EBP as potential targets. Cancer Lett 273(1):86–97. doi:10.1016/j.canlet.2008.07.039
Kundu JK, Shin YK, Surh YJ (2006) Resveratrol modulates phorbol ester-induced pro-inflammatory signal transduction pathways in mouse skin in vivo: NF-kappaB and AP-1 as prime targets. Biochem Pharmacol 72(11):1506–1515. doi:10.1016/j.bcp.2006.08.005
Kundu JK, Surh YJ (2008) Inflammation: gearing the journey to cancer. Mutat Res 659(1–2):15–30. doi:10.1016/j.mrrev.2008.03.002
Kwon JY, Lee KW, Kim JE, Jung SK, Kang NJ, Hwang MK, Heo YS, Bode AM, Dong Z, Lee HJ (2009) Delphinidin suppresses ultraviolet B-induced cyclooxygenases-2 expression through inhibition of MAPKK4 and PI-3 kinase. Carcinogenesis 30(11):1932–1940. doi:10.1093/carcin/bgp216
Kyrgidis A, Vahtsevanos K, Tzellos TG, Xirou P, Kitikidou K, Antoniades K, Zouboulis CC, Triaridis S (2010) Clinical, histological and demographic predictors for recurrence and second primary tumours of head and neck basal cell carcinoma. A 1062 patient-cohort study from a tertiary cancer referral hospital. Eur J Dermatol: EJD 20(3):276–282. doi:10.1684/ejd.2010.0903
Laferriere J, Houle F, Huot J (2002) Regulation of the metastatic process by E-selectin and stress-activated protein kinase-2/p38. Ann NY Acad Sci 973:562–572
Langowski JL, Zhang X, Wu L, Mattson JD, Chen T, Smith K, Basham B, McClanahan T, Kastelein RA, Oft M (2006) IL-23 promotes tumour incidence and growth. Nature 442(7101):461–465. doi:10.1038/nature04808
Lederle W, Depner S, Schnur S, Obermueller E, Catone N, Just A, Fusenig NE, Mueller MM (2011) IL-6 promotes malignant growth of skin SCCs by regulating a network of autocrine and paracrine cytokines. Int J Cancer J Int du Cancer 128(12):2803–2814. doi:10.1002/ijc.25621
Lee WY, Lockniskar MF, Fischer SM (1994) Interleukin-1 alpha mediates phorbol ester-induced inflammation and epidermal hyperplasia. FASEB Journal: Official Publ Fed Am Soc Exp Biol 8(13):1081–1087
Li AG, Lu SL, Zhang MX, Deng C, Wang XJ (2004) Smad3 knockout mice exhibit a resistance to skin chemical carcinogenesis. Cancer Res 64(21):7836–7845. doi:10.1158/0008-5472.CAN-04-1331
Liang L, Hu D, Liu W, Williams JP, Okunieff P, Ding I (2003) Celecoxib reduces skin damage after radiation: selective reduction of chemokine and receptor mRNA expression in irradiated skin but not in irradiated mammary tumor. Am J Clin Oncol 26(4):S114–S121. doi:10.1097/01.COC.0000074149.95710.40
Loeb LA, Harris CC (2008) Advances in chemical carcinogenesis: a historical review and prospective. Cancer Res 68(17):6863–6872. doi:10.1158/0008-5472.CAN-08-2852
Lu H, Ouyang W, Huang C (2006) Inflammation, a key event in cancer development. Molecular Cancer Res: MCR 4(4):221–233. doi:10.1158/1541-7786.MCR-05-0261
Madan V, Lear JT, Szeimies RM (2010) Non-melanoma skin cancer. Lancet 375(9715):673–685. doi:10.1016/S0140-6736(09)61196-X
Magcwebeba T, Riedel S, Swanevelder S, Bouic P, Swart P, Gelderblom W (2012) Interleukin-1alpha induction in human keratinocytes (HaCaT): an in vitro model for chemoprevention in skin. J Skin Cancer 2012:393681. doi:10.1155/2012/393681
Mallikarjuna G, Dhanalakshmi S, Singh RP, Agarwal C, Agarwal R (2004) Silibinin protects against photocarcinogenesis via modulation of cell cycle regulators, mitogen-activated protein kinases, and Akt signaling. Cancer Res 64(17):6349–6356. doi:10.1158/0008-5472.CAN-04-1632
Mantovani A, Allavena P, Sica A, Balkwill F (2008) Cancer-related inflammation. Nature 454(7203):436–444. doi:10.1038/nature07205
Marsik C, Kazemi-Shirazi L, Schickbauer T, Winkler S, Joukhadar C, Wagner OF, Endler G (2008) C-reactive protein and all-cause mortality in a large hospital-based cohort. Clin Chem 54(2):343–349. doi:10.1373/clinchem.2007.091959
Martin AG, San-Antonio B, Fresno M (2001) Regulation of nuclear factor kappa B transactivation. Implication of phosphatidylinositol 3-kinase and protein kinase C zeta in c-Rel activation by tumor necrosis factor alpha. J Biol Chem 276(19):15840–15849. doi:10.1074/jbc.M011313200
Massoumi R, Chmielarska K, Hennecke K, Pfeifer A, Fassler R (2006) Cyld inhibits tumor cell proliferation by blocking Bcl-3-dependent NF-kappaB signaling. Cell 125(4):665–677. doi:10.1016/j.cell.2006.03.041
Meeran SM, Akhtar S, Katiyar SK (2009) Inhibition of UVB-induced skin tumor development by drinking green tea polyphenols is mediated through DNA repair and subsequent inhibition of inflammation. J Invest Dermatol 129(5):1258–1270. doi:10.1038/jid.2008.354
Meeran SM, Katiyar S, Elmets CA, Katiyar SK (2007) Interleukin-12 deficiency is permissive for angiogenesis in UV radiation-induced skin tumors. Cancer Res 67(8):3785–3793. doi:10.1158/0008-5472.CAN-06-3134
Mikirova N, Casciari J, Rogers A, Taylor P (2012) Effect of high-dose intravenous vitamin C on inflammation in cancer patients. J Transl Med 10:189. doi:10.1186/1479-5876-10-189
Millan O, Rico D, Peinado H, Zarich N, Stamatakis K, Perez-Sala D, Rojas JM, Cano A, Bosca L (2006) Potentiation of tumor formation by topical administration of 15-deoxy-delta12,14-prostaglandin J2 in a model of skin carcinogenesis. Carcinogenesis 27(2):328–336. doi:10.1093/carcin/bgi213
Mishra PK, Raghuram GV, Bhargava A, Ahirwar A, Samarth R, Upadhyaya R, Jain SK, Pathak N (2011) In vitro and in vivo evaluation of the anticarcinogenic and cancer chemopreventive potential of a flavonoid-rich fraction from a traditional Indian herb Selaginella bryopteris. Br J Nutr 106(8):1154–1168. doi:10.1017/S0007114511001498
Mueller MM (2006) Inflammation in epithelial skin tumours: old stories and new ideas. Eur J Cancer 42(6):735–744. doi:10.1016/j.ejca.2006.01.014
Muhleisen B, Petrov I, Gachter T, Kurrer M, Scharer L, Dummer R, French LE, Hofbauer GF (2009) Progression of cutaneous squamous cell carcinoma in immunosuppressed patients is associated with reduced CD123+ and FOXP3+ cells in the perineoplastic inflammatory infiltrate. Histopathology 55(1):67–76. doi:10.1111/j.1365-2559.2009.03324.x
Muller-Decker K, Neufang G, Berger I, Neumann M, Marks F, Furstenberger G (2002) Transgenic cyclooxygenase-2 overexpression sensitizes mouse skin for carcinogenesis. Proc Natl Acad Sci USA 99(19):12483–12488. doi:10.1073/pnas.192323799
Nickoloff BJ, Ben-Neriah Y, Pikarsky E (2005) Inflammation and cancer: is the link as simple as we think? J Invest Dermatol 124(6):x–xiv. doi:10.1111/j.0022-202X.2005.23724.x
Oberyszyn TM, Sabourin CL, Bijur GN, Oberyszyn AS, Boros LG, Robertson FM (1993) Interleukin-1 alpha gene expression and localization of interleukin-1 alpha protein during tumor promotion. Mol Carcinog 7(4):238–248
Osakabe N, Yasuda A, Natsume M, Yoshikawa T (2004) Rosmarinic acid inhibits epidermal inflammatory responses: anticarcinogenic effect of Perilla frutescens extract in the murine two-stage skin model. Carcinogenesis 25(4):549–557. doi:10.1093/carcin/bgh034
Paavonen K, Ekman N, Wirzenius M, Rajantie I, Poutanen M, Alitalo K (2004) Bmx tyrosine kinase transgene induces skin hyperplasia, inflammatory angiogenesis, and accelerated wound healing. Mol Biol Cell 15(9):4226–4233. doi:10.1091/mbc.E04-03-0241
Pahl HL (1999) Activators and target genes of Rel/NF-kappaB transcription factors. Oncogene 18(49):6853–6866. doi:10.1038/sj.onc.1203239
Parkin DM (2006) The global health burden of infection-associated cancers in the year 2002. Int J Cancer J Int du Cancer 118(12):3030–3044. doi:10.1002/ijc.21731
Passos GF, Medeiros R, Marcon R, Nascimento AF, Calixto JB, Pianowski LF (2013) The role of PKC/ERK1/2 signaling in the anti-inflammatory effect of tetracyclic triterpene euphol on TPA-induced skin inflammation in mice. Eur J Pharmacol 698(1–3):413–420. doi:10.1016/j.ejphar.2012.10.019
Patel R, Garg R, Erande S, BM G (2007) Chemopreventive herbal anti-oxidants: current status and future perspectives. J Clin Biochem Nutr 40(2):82–91. doi:10.3164/jcbn.40.82
Patel R, Krishnan R, Ramchandani A, Maru G (2008) Polymeric black tea polyphenols inhibit mouse skin chemical carcinogenesis by decreasing cell proliferation. Cell Prolif 41(3):532–553. doi:10.1111/j.1365-2184.2008.00528.x
Patil AS, Puri YS, Gedham MC, Naik AV, Joshi RK (2005) Saree cancer. Bombay Hosp J 47(3):302–303
Perez-Lorenzo R, Markell LM, Hogan KA, Yuspa SH, Glick AB (2010) Transforming growth factor beta1 enhances tumor promotion in mouse skin carcinogenesis. Carcinogenesis 31(6):1116–1123. doi:10.1093/carcin/bgq041
Perez-Moreno M, Song W, Pasolli HA, Williams SE, Fuchs E (2008) Loss of p120 catenin and links to mitotic alterations, inflammation, and skin cancer. Proc Natl Acad Sci USA 105(40):15399–15404. doi:10.1073/pnas.0807301105
Petit-Frere C, Clingen PH, Grewe M, Krutmann J, Roza L, Arlett CF, Green MH (1998) Induction of interleukin-6 production by ultraviolet radiation in normal human epidermal keratinocytes and in a human keratinocyte cell line is mediated by DNA damage. J Invest Dermatol 111(3):354–359. doi:10.1038/sj.jid.5602962
Prasad S, Ravindran J, Aggarwal BB (2010) NF-κB and cancer: how intimate is this relationship. Mol Cell Biochem 336(1–2):25–37. doi:10.1007/s11010-009-0267-2
Proksch E, Brandner JM, Jensen JM (2008) The skin: an indispensable barrier. Exp Dermatol 17(12):1063–1072
Pytliak M, Vargova V, Mechirova V (2012) Matrix metalloproteinases and their role in oncogenesis: a review. Onkologie 35(1–2):49–53. doi:10.1159/000336304
Ramos MC, Steinbrenner H, Stuhlmann D, Sies H, Brenneisen P (2004) Induction of MMP-10 and MMP-1 in a squamous cell carcinoma cell line by ultraviolet radiation. Biol Chem 385(1):75–86. doi:10.1515/BC.2004.010
Ravi R, Piva TJ (2013) The role of furin in the development of skin cancer. In: Vereecken DP (ed.) Highlights in skin cancer. InTech, UK. doi:10.5772/55569
Reuter S, Gupta SC, Chaturvedi MM, Aggarwal BB (2010) Oxidative stress, inflammation, and cancer: how are they linked? Free Radical Biol Med 49(11):1603–1616. doi:10.1016/j.freeradbiomed.2010.09.006
Rogers HW, Weinstock MA, Harris AR, Hinckley MR, Feldman SR, Fleischer AB, Coldiron BM (2010) Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol 146(3):283–287. doi:10.1001/archdermatol.2010.19
Rundhaug JE, Fischer SM (2010) Molecular mechanisms of mouse skin tumor promotion. Cancers 2(2):436–482. doi:10.3390/cancers2020436
Saladi RN, Persaud AN (2005) The causes of skin cancer: a comprehensive review. Drugs Today (Barc) 41(1):37–53. doi:10.1358/dot.2005.41.1.875777
Schadendorf D, Heidel J, Gawlik C, Suter L, Czarnetzki BM (1995) Association with clinical outcome of expression of VLA-4 in primary cutaneous malignant melanoma as well as P-selectin and E-selectin on intratumoral vessels. J Natl Cancer Inst 87(5):366–371
Schwarz T, Luger TA (1989) Effect of UV irradiation on epidermal cell cytokine production. J Photochem Photobiol B 4(1):1–13
Scott KA, Arnott CH, Robinson SC, Moore RJ, Thompson RG, Marshall JF, Balkwill FR (2004) TNF-α regulates epithelial expression of MMP-9 and integrin αvβ6 during tumour promotion. A role for TNF-α in keratinocyte migration? Oncogene 23(41):6954–6966. doi:10.1038/sj.onc.1207915
Shanmugam MK, Nguyen AH, Kumar AP, Tan BK, Sethi G (2012) Targeted inhibition of tumor proliferation, survival, and metastasis by pentacyclic triterpenoids: potential role in prevention and therapy of cancer. Cancer Lett 320(2):158–170. doi:10.1016/j.canlet.2012.02.037
Shirley SH, Grimm EA, Kusewitt DF (2012) Ultraviolet radiation and the slug transcription factor induce proinflammatory and immunomodulatory mediator expression in melanocytes. J Skin Cancer 2012:410925. doi:10.1155/2012/410925
Shrotriya S, Kundu JK, Na HK, Surh YJ (2010) Diallyl trisulfide inhibits phorbol ester-induced tumor promotion, activation of AP-1, and expression of COX-2 in mouse skin by blocking JNK and Akt signaling. Cancer Res 70(5):1932–1940. doi:10.1158/0008-5472.CAN-09-3501
Siegfried G, Basak A, Cromlish JA, Benjannet S, Marcinkiewicz J, Chretien M, Seidah NG, Khatib AM (2003) The secretory proprotein convertases furin, PC5, and PC7 activate VEGF-C to induce tumorigenesis. J Clin Investig 111(11):1723–1732. doi:10.1172/JCI17220
Singh T, Katiyar SK (2011) Green tea catechins reduce invasive potential of human melanoma cells by targeting COX-2, PGE2 receptors and epithelial-to-mesenchymal transition. PLoS One 6(10):e25224. doi:10.1371/journal.pone.0025224
Slaga TJ, Viaje A, Bracken W (1977) The effects of anti-inflammatory agents on skin tumor initiation and aryl hydrocarbon hydroxylase. Res Commun Chem Pathol Pharmacol 16(2):337–350
Soehnge H, Ouhtit A, Ananthaswamy ON (1997) Mechanisms of induction of skin cancer by UV radiation. Frontiers Biosci: J Virtual Libr 2:d538–d551
St Sauver JL, Sarma AV, Jacobson DJ, McGree ME, Lieber MM, Girman CJ, Nehra A, Jacobsen SJ (2009) Associations between C-reactive protein and benign prostatic hyperplasia/lower urinary tract symptom outcomes in a population-based cohort. Am J Epidemiol 169(11):1281–1290. doi:10.1093/aje/kwp085
Surh YJ, Chun KS, Cha HH, Han SS, Keum YS, Park KK, Lee SS (2001) Molecular mechanisms underlying chemopreventive activities of anti-inflammatory phytochemicals: down-regulation of COX-2 and iNOS through suppression of NF-κB activation. Mutat Res 480–481:243–268
Tiano HF, Loftin CD, Akunda J, Lee CA, Spalding J, Sessoms A, Dunson DB, Rogan EG, Morham SG, Smart RC, Langenbach R (2002) Deficiency of either cyclooxygenase (COX)-1 or COX-2 alters epidermal differentiation and reduces mouse skin tumorigenesis. Cancer Res 62(12):3395–3401
Tober KL, Wilgus TA, Kusewitt DF, Thomas-Ahner JM, Maruyama T, Oberyszyn TM (2006) Importance of the EP(1) receptor in cutaneous UVB-induced inflammation and tumor development. J Invest Dermatol 126(1):205–211. doi:10.1038/sj.jid.5700014
Trompouki E, Hatzivassiliou E, Tsichritzis T, Farmer H, Ashworth A, Mosialos G (2003) CYLD is a deubiquitinating enzyme that negatively regulates NF-kappaB activation by TNFR family members. Nature 424(6950):793–796. doi:10.1038/nature01803
Ulrich C, Johannsen A, Rowert-Huber J, Ulrich M, Sterry W, Stockfleth E (2010) Results of a randomized, placebo-controlled safety and efficacy study of topical diclofenac 3 % gel in organ transplant patients with multiple actinic keratoses. Eur J Dermatol 20(4):482–488. doi:10.1684/ejd.2010.1010
Urban JL, Shepard HM, Rothstein JL, Sugarman BJ, Schreiber H (1986) Tumor necrosis factor: a potent effector molecule for tumor cell killing by activated macrophages. Proc Natl Acad Sci USA 83(14):5233–5237
Vaid M, Sharma SD, Katiyar SK (2010) Honokiol, a phytochemical from the Magnolia plant, inhibits photocarcinogenesis by targeting UVB-induced inflammatory mediators and cell cycle regulators: development of topical formulation. Carcinogenesis 31(11):2004–2011. doi:10.1093/carcin/bgq186
Vanderveen EE, Grekin RC, Swanson NA, Kragballe K (1986) Arachidonic acid metabolites in cutaneous carcinomas. Evidence suggesting that elevated levels of prostaglandins in basal cell carcinomas are associated with an aggressive growth pattern. Arch Dermatol 122(4):407–412
Vougioukalaki M, Kanellis DC, Gkouskou K, Eliopoulos AG (2011) Tpl2 kinase signal transduction in inflammation and cancer. Cancer Lett 304(2):80–89. doi:10.1016/j.canlet.2011.02.004
Wennogle LP, Liang H, Quintavalla JC, Bowen BR, Wasvary J, Miller DB, Allentoff A, Boyer W, Kelly M, Marshall P (1995) Comparison of recombinant cyclooxygenase-2 to native isoforms: aspirin labeling of the active site. FEBS Lett 371(3):315–320
Wilgus TA, Koki AT, Zweifel BS, Kusewitt DF, Rubal PA, Oberyszyn TM (2003) Inhibition of cutaneous ultraviolet light B-mediated inflammation and tumor formation with topical celecoxib treatment. Mol Carcinog 38(2):49–58. doi:10.1002/mc.10141
Witz IP (2006) Tumor-microenvironment interactions: the selectin-selectin ligand axis in tumor-endothelium cross talk. Cancer Treat Res 130:125–140
Wright TI, Spencer JM, Flowers FP (2006) Chemoprevention of nonmelanoma skin cancer. J Am Acad Dermatol 54(6):933–946; quiz 947–950. doi:10.1016/j.jaad.2005.08.062
Yasukawa K, Akihisa T, Yoshida ZY, Takido M (2000) Inhibitory effect of euphol, a triterpene alcohol from the roots of Euphorbia kansui, on tumour promotion by 12-O-tetradecanoylphorbol-13-acetate in two-stage carcinogenesis in mouse skin. J Pharm Pharmacol 52(1):119–124
Yu H, Kortylewski M, Pardoll D (2007) Crosstalk between cancer and immune cells: role of STAT3 in the tumour microenvironment. Nat Rev Immunol 7(1):41–51. doi:10.1038/nri1995
Zhu JW, Wu XJ, Lu ZF, Luo D, Cai SQ, Zheng M (2013) Role of VEGF receptors in normal and psoriatic human keratinocytes: evidence from irradiation with different UV sources. PLoS One 8(1):e55463. doi:10.1371/journal.pone.0055463
Zhu Z, Zhong S, Shen Z (2011) Targeting the inflammatory pathways to enhance chemotherapy of cancer. Cancer Biol Ther 12(2):95–105
Acknowledgments
We thank Dr. Vikram Gota for useful discussion and Council of Scientific and Industrial Research (CSIR) and ACTREC, Government of India, for awarding fellowship to Mr. Gaurav Kumar.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Basel
About this chapter
Cite this chapter
Maru, G.B., Gandhi, K., Ramchandani, A., Kumar, G. (2014). The Role of Inflammation in Skin Cancer. In: Aggarwal, B., Sung, B., Gupta, S. (eds) Inflammation and Cancer. Advances in Experimental Medicine and Biology, vol 816. Springer, Basel. https://doi.org/10.1007/978-3-0348-0837-8_17
Download citation
DOI: https://doi.org/10.1007/978-3-0348-0837-8_17
Published:
Publisher Name: Springer, Basel
Print ISBN: 978-3-0348-0836-1
Online ISBN: 978-3-0348-0837-8
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)