
Abstract
Pain is a highly subjective and complex phenomenon. Current methods used to measure pain mostly rely on the patient’s description, which may not always be possible. This way, pain recognition systems based on body language and physiological signals have emerged. As the emotional state of a person can also influence the way pain is perceived, in this work, a protocol for pain induction with previous emotional elicitation was conducted. Eletrocardiogram (ECG), Electrodermal Activity (EDA) and Eletromyogram (EMG) signals were collected during the protocol. Besides the physiological responses, perception was also assessed through reported-scores (using a numeric scale) and times for pain tolerance. In this protocol, 3 different emotional elicitation sessions, negative, positive and neutral, were performed through videos of excerpts of terror, comedy and documentary movies, respectively, and pain was induced using the Cold Pressor Task (CPT). A total of 56 participants performed the study (with 54 completing all three sessions). The results showed that during the negative emotional state, pain reported-scores were higher and pain threshold and tolerance times were smaller when compared with positive. As expected, the physiological response to pain remain similar despite the emotional elicitation.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Pain is a subjective phenomenon that depends on the past experiences of each individual and the circumstances of the moment. It’s a survival mechanism that allows us to identify harmful situations and avoid tissue damage [9].
Pain has a big impact on people’s lives and society in general, it’s the principal reason for seeking medical attention and it can also provoke a loss of productivity in companies [9]. Moreover, chronic pain costs society more than cancer and heart diseases [9]. So, it is important to deal with pain as soon as possible, identifying its origin to achieve diagnosis and adequate treatment, preventing harmful consequences.
Currently, there are several methods to measure pain, but all of them depend on the patient’s description. Pain assessment is typically done by a caregiver through self-reports, observing behavioral or physiological pain responses, and using information about the pain cause [9]. The methods used to quantify pain are usually visual or numeric scales [4]. However, patients with limited communication skills cannot report their pain experience, these may include infants and children, adults with cognitive damage or intellectual disability, and unconscious people [9]. Thus, an objective measurement of pain could be beneficial. To achieve this goal, there has been some research devoted to the development of pain recognition systems, which are based on the detection of some characteristics provoked in the human body by pain, such as facial expressions, sounds, gestures, or even some physiological signals.
To evaluate pain sensitivity there are three measurements that are commonly used: pain threshold, which is the minimal stimulus intensity required to elicit pain; pain tolerance, which is the maximal stimulus intensity that an individual can withstand; and pain perception, which refers to what classification an individual gives to a standardized stimulus intensity [10]. Pain is not only a physical experience but is also connected with emotions. As mentioned earlier, pain is a subjective experience that depends on the circumstances in which it occurs. One factor that can influence the pain experience is the emotional state of the individual [4].
This work addresses the influence of emotional states on pain responses. Firstly, the participants are subjected to the elicitation of different kinds of emotions, namely negative, positive, and neutral, through the visualization of different excerpts of terror, comedy and documentary movies, respectively, while pain induction is attained through the Cold Pressor Task (CPT) test in three different emotional sessions. Throughout each entire session, electrocardiogram (ECG), eletromyogram (EMG) from triceps and trapezius, electrodermal activity (EDA) and pain-reported measures are collected.
The aim of this work is to understand if emotion elicitation has an influence in pain perception and response. It is expected that emotional elicitation will not have an influence on the physiological response to pain, while it is supposed that perception depends on the elicited emotional state. Negative emotions (in this case, fear) should exacerbated pain, increasing the perception and lowering the tolerance to pain. On the other hand, positive emotions (happiness) should attenuate the perception of pain. This way, this work proposes a new protocol to assess pain perception related to the emotional state of a person and establishes a relationship among pain and positive and negative emotions.
This document is structured as follows: Sect. 2 presents some related studies that assess emotional modulation in pain perception; Sect. 3 describes the materials and the methods used to develop this work; Sect. 4 exposes the obtained results; Sect. 5 presents its discussion and Sect. 6 highlights the main conclusions achieved and a perspective for future research.
2 Related Works
There have been several studies developing pain recognition systems with different approaches. The works below support that emotions can have a crucial role in pain perception, driving the motivation for the present work in studying the influence of emotions on pain perception.
Zhang et. al [10] investigated the differences in pain perception between men and women and how that is related to negative emotions. To quantify pain sensitivity, they used a cold pressure test (CPT), and to assess negative emotions they used several questionnaires and MRI data. The hypothesis was that females experience more negative emotions and that is related to a higher pain sensitivity. So, first, the subjects responded to emotion-related questionnaires and then they were submitted to a CPT. The questionnaires included were the Chinese version of the Fear of Pain Questionnaire (FPQ), the Pain Anxiety Symptoms Scale-20 (PASS), the trait version of State-Trait Anxiety Inventory (STAI) and the Beck Depression Inventory. The pain was induced by putting the individual’s left hand into cold water at a temperature of 2\(^\circ \)C. Pain threshold was determined as the duration of immersion from the time that the hand was kept in the water to the time the subject began to feel pain and pain tolerance as the total time from immersing the hand in the water to the time the participants remove it. Several statistical analyses were performed, such as the non-parametric Mann-Whitney U-tests and Spearman rank correlation analyses (with the skewed distributed variables) and the parametric independent samples t-tests and Pearson correlation analyses (with normally distributed variables). They found statistically significant gender differences in pain threshold and tolerance, and two questionnaires: the males presented higher pain threshold and tolerance and lower scores in the FPQ and PASS questionnaires. Further analysis showed that the two questionnaires’ scores were negatively correlated with pain threshold and tolerance, showing that differences in pain sensitivity were mediated by pain-related negative emotions, specifically pain-related fear and anxiety.
Silva and Sebastião [7] studied the ECG signal during pain induction under disctint emotional contexts. The participants were subjected to a CPT, for inducing pain, while watching an emotional inducing video. The protocol consisted of two sessions, one using a fear emotion-inducing video and a second using a neutral one. The data was pre-processed and then was used 8 machine learning algorithms to classify pain. Attempting on a binary classification of pain, training and testing was performed in several strategies using ECG data from both emotional sessions, and classification results were compared across different strategies. In their work, the results supports that ECG response remain similar along both sessions. As for the classifiers, the RF and AdaBoost showed better performance to classify pain and the LDA and LR models were the worst ones.
Srisopa et. al [8] found that emotion regulation strategies produced significant improvements in decreasing pain intensity during labor. In this review, the type of pain studied was the pain caused in the labor and was measured by self-report or the observation of the participant’s behavior. Strategies based on mindfulness intervention and distraction were used to train the subjects to manage pain. The individuals submitted to these techniques showed a significantly reduced pain intensity during the active phase of labor.
Although the studies of Zhang et al. [10] and Srisopa et al. [8] associate emotional state with pain perception, they do not establish a protocol for emotional and pain induction. The protocol proposed by Silva et al. [7] has certain limitations, which will be discussed in Sect. 5.
3 Materials and Methods
This section presents the materials and methods implemented in this work. The data acquisition and approaches used to analyse the data are also exposed.
3.1 Experimental Setup
Pain was induced using the Cold Pressor Task (CPT). The CPT is a test that involves putting a hand or forearm in cold water causing a stimulus that produces a slowly increasing pain of slight to moderate intensity. It has been used in many different types of works, such as studies about pain, autonomic reactivity, and hormonal stress responses [2].
For the signals collection, a 4-Channel BiosignalspluxFootnote 1 was used. Four sensors were connected to this device: two EMG sensors, one EDA sensor, and one ECG.
In Fig. 1 the equipment’s setup and its placement in the room are shown.

Experimental Setup.
For the CPT test, a stainless-steel tank of 45 liters was used. The tank has an immersion thermostat, that includes a circulation pump that can be used to improve the homogeneity within the bath and to perform a closed liquid circulation circuit. The water was initially cooled with ice and the control panel allows the control and adjustment of temperature. Also, two notebooks were used: one for the acquisition of the sensors’ reading and the respective monitorization (through the software OpenSignals from Biosignalsplux) and the other for displaying the videos with an external monitor (used with headphones for audio). This notebook was also used for completing the questionnaires. The experimental procedure was implemented at the Institute of Electronics and Informatics Engineering of Aveiro, University of Aveiro, in a room prepared specifically for this purpose.
3.2 Protocol
Before the procedure, informed consent with all the information about the process was given to the participants. In the case of a positive response, the first questionnaire, the trait version of State-Trait Inventory for Cognitive and Somatic Anxiety (STICSA-trait) was also given to the participant to be replied before the procedure.
The protocol begins with the participant answering the following questionnaires: the state version of STICSA (STICSA-state), the Perceived Stress Scale (PSS), the Eysenck Personality Inventory (EPI) and the Visual Analog Scale (VAS), in this order. The purpose of these questionnaires is to assess some psychological traits of the participant, as well as the emotional state. The VAS questionnaire measures the participant’s arousal and valence state.
After the questionnaires, the electrodes connected to the Biosignalsplux sensors are placed on the participant according to Fig. 2.

Scheme of the electrodes placement: A) EMG electrodes on the trapezius and triceps muscles; B) ECG electrodes plus reference electrode of the EMG and C) EDA electrodes.
The positive electrodes are represented with a red circle and the negative ones with a black circle. The white electrodes are the reference electrodes for the ECG and EMG signals and must be placed above the pelvic bone for ECG above on the collarbone for EMG. The EMG electrodes were placed in the trapezius and triceps muscles of the non-dominant arm. The ECG electrodes were placed on the rib cage (the positive one on the right side and the negative one on the left side of the body). The EDA was collected on the dominant hand: the positive electrode was placed in the upper part of the palm and the negative in the lower part of the palm.
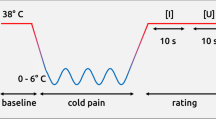
Accounting for the inter-participant variability regarding the physiological responses, the data collection begins with a rest time (Baseline 1), corresponding to five minutes, where the person will be just sat in a comfortable position without any stimuli. After this time, while still in a comfortable position without any pain stimuli, the participant will watch an emotional-inducing video for around ten minutes, in the frontal screen. The video can be one of three kind: an neutral emotional inducing video, which is composed of excerpts of documentaries, a negative emotional inducing video (Fear), which is composed of excerpts of terror movies or a positive emotional inducing video (Happiness), which is composed by excerpts of comedy movies.
When the video ends, the subject will be asked to respond to a last questionnaire, the VAS-pos, and then another rest time begins (Baseline 2) also with a duration of five minutes. At the end of this resting time, the participant is asked to report the pain level, in his non-dominant hand, using a numerical pain scale (NPS) ranging from 0 to 10. Afterwards, the pain stimulus is applied. The individual will be requested to put his non-dominant hand in the cold-water tank with a temperature of approximately 7\(^\circ \)C± 1\(^\circ \)C, beginning the CPT test. To register the participant’s pain threshold, they are asked to report the pain level using the NPS as soon as they feel any pain. The participants are informed to hold the hand immersed as long as they can, with a time limit of 2 min. If they reach the point where they can no longer tolerate the pain, they are instructed to report to the researchers that they will remove the hand from the tank. Before doing so, they are asked to report the pain level (pain tolerance). If they can keep the hand immersed in the tank for the complete duration, the maximum pain experience will be reported at the limited time defined (2 min). Finally, the last rest period begins. After three minutes the level of pain is reported again. At the end of the rest period, the procedure ends.
Each participant repeats this protocol three times, with an interval of approximately 1 week, where each session differs from the type of emotion-induced through the video. The order of the videos is randomized. In the second and third sessions, the participants will only respond to the questionnaires STICSA-state, VAS-pre, and VAS-pos.
The protocol for data collection is schematized in Fig. 3.

Scheme of the protocol applied.
This study was approved by the Ethics and Deontological Council of the University of Aveiro (CED-UA-12-CED/2023).
3.3 Physiological Data Preparation
After the acquisition, the physiological data was filtered and divided into epochs according to the triggers given and processed.
The epochs used in this work correspond to Baseline 1 and CPT epochs only, since the aim is to evaluate if the emotion elicitation had some influence on physiological response to pain and in pain perception.
The signals were pre-processed using Neurokit2Footnote 2 in Python. The ECG was filtered using a 5th-order high-pass Butterworth filter with cut off frequency of 0.5 Hz, followed by powerline filtering (50 Hz). The EDA was filtered using a 4th-order low-pass Butterworth filter with cut off frequency of 5 Hz followed by smoothing of the signal. Lastly, the EMG was filtered using a 4th-order 10 Hz highpass Butterworth filter followed by a notch filter at 50 Hz and a constant detrending. After the filtering, Neurokit2 functions were used to extract some important features of the signals.
Table 1 summarizes all the features extracted from the physiological signals. The choice of the features was based on previous studies where CPT was used [6, 7] and other features were considered for analyses.
Regarding the Heart Rate Variability (HRV), only ultra-short metrics were extracted since the CPT lasted 2 min or less. The works of Salahuddin et. al [5] and Boonnithi et. al [3] prove that the HRV features present in Table 1 are suitable to be calculated through signals lasting only 30 s or less. This way, only the sessions where the participant endured at least 30 s with the hand on the cold water tank were tacked into account to this work.
In order to minimize inter-participant variability, the features were normalized by the ratio between those features extracted from CPT and those extracted from Baseline 1, for each participant.
As HRV_pNN50 had some zero values in the Baseline 1 epoch, this feature was removed from the dataset, since the ratio would lead to NaN values. The HRV_LF, HRV_LFn and HRV_LFHF features were also removed since they had several NaN values.
3.4 Statistical Analysis
In order to investigate if the extracted features differed significantly regarding the emotion elicitation, statistical tests were performed.
First, the normality of all the features was tested using the Shapiro-Wilk test, which tests the null hypothesis that the data was drawn from a normal distribution. Therefore, if the p-value is below a chosen significance level (in this case, \(\alpha \)=0.05), the null hypothesis should be rejected and therefore the feature is not likely to follow a normal distribution [1].
The features that fail the Shapiro-Wilk test (the data does not meet the assumption of normality) were submitted to a non-parametric Friedman test. Those who passed the Shapiro-Wilk test (the data is likely to follow a normal distribution) were submitted to the parametric repeated measures ANOVA test. Both Friedman and ANOVA tests were used to evaluate if the features could differentiate between sessions with different emotion elicitation (F: Fear, H: Happiness, N: Neutral). Afterwards, the Nemenyi post-hoc test was performed to evaluate, for those features, which pair of emotional states differed.
4 Results
A total of 56 volunteers (28 females) with ages between 18 and 30 y.o. (mean of 22.46 and standard deviation of 2.04 y.o.) participate in the study. Only 2 participants did not undergo the last session due to personal reasons. Therefore, a total of 166 sessions were performed.
4.1 Pain Perception
Among all the sessions the mean time of the CPT was about 91.70 ± 39.64 s (mean±standard deviation). Within the 166 sessions, there were 9 sessions where the participant kept the hand in the cold-water tank for less than 30 s. On the opposite, there were 96 sessions where the participants endured the maximum times (2 min) with the hand immersed.
With regard to the pain scores reported, none of the participants felt pain before the CPT. At the time the participants felt pain (pain threshold) they reported a score of 4.78 ± 2.08 in the NPS. At the end of the 2 min or at the moment the participant took the hand off the tank (tolerance) the pain reported was of 7.84±1.71 in the NPS. After 3 min of the removal of the hand from the cold water, the pain reported decreased to 0.72 ± 1.09 in the NPS. There were 96 sessions where participants did not feel any pain at this time.
Taking into account the emotional elicitation, only data from 54 participants were analysed, since 2 did not perform the three sessions and therefore, they were missing an elicitation.
Considering the negative state, the scores reported at pain tolerance and at the 3 min after taking the hand off the water, were greater than those reported when in neutral and positive states. With respect to the scores reported at pain threshold, the values are similar across emotional sessions, specially for negative and positive inducing sessions (4.70 ± 2.20 and 4.71 ± 2.05, respectively). However, with regard to time, both pain threshold and tolerance were lower for the negative state (15.76 ± 9.29 and 92.11 ± 39.76, respectively) when compared with the positive induced condition (19.74 ± 21.94 and 93.23 ± 38.71, respectively).
Figure 4 presents the violinplots for the reported pain scores (top) and for the times (in seconds) of pain threshold and tolerance (bottom). Regarding the scores, when comparing the violins for each emotion, it can be noted that they are very similar to each other. Only smaller differences, regarding gender, can be found, as females tend to report highest scores than males.

Violinplots of the NPS scores reported by participants (top) and of the pain threshold and tolerance, expressed in seconds (bottom). The
 stands for the mean of the scores and times within each emotion. (Color figure online)
stands for the mean of the scores and times within each emotion. (Color figure online)
With respect to tolerance’s time, the violins are quite similar. However, it is interesting that the three plots seem to have two clusters. It shows that the distribution of the time that participants can stand with the hand immersed in the water is not uniform, indicating that are mainly two groups of participants: those who can tolerate the 2 min and those who can barely reach the 1 min. However, it is evident that more participants can reach the two minutes than the opposite. Regarding gender, no differences stand out, since the violins look quite symmetric.
Concerning pain threshold’s time, the violins are also very similar but the values are more dispersed for Positive and Neutral states than for Negative, and, in general, females tend to report pain sooner than males.
These results seem to support the hypothesis that emotion elicitation influences pain perception since, despite the similar scores, when in the negative induced session the pain scores were higher and the threshold and tolerance times where lower, which indicates less resilience to pain and greater exacerbation.
4.2 Physiological Data
As mentioned above, in this work only the sessions where the participant lasted at least 30 s with the hand immersed in the cold water were considered for physiological data analysis. Therefore, the 9 sessions where participants did not endure the CPT for at least 30 s were removed. Two cases where the acquisition of physiological data failed were also removed, leaving signals of 155 sessions for analysis. For statistical analyses, only the participants who had the features computed for the three emotions were considered, leaving a total of 46 participants and therefore 138 samples per feature.
Only two features could differentiate statistically between emotional states, namely R_OnOffDist and SCR_Height.
Figure 5 presents the boxplots of R_OnOffDist and SCR_Height and the p-values between the different emotional states.

Boxplots of the features R_OnOffDist and SCR_Height (top) and the respective p-values between different emotions (bottom). The \(\blacklozenge \) stands for outliers and the
 stands for the mean of the features within each emotion. (Color figure online)
stands for the mean of the features within each emotion. (Color figure online)
The boxplots of the ECG feature for Positive and Neutral states are quite similar, with the Neutral one presenting slight higher values. However, the boxplot for Negative indicates that the values obtained with this state were lower. In fact, all the quartiles, and even the mean, are lower in this case. This feature shows a significant statistically difference between the Negative and Neutral states with a p-value lower than 0.05. With regard to SCR_Height (obtained through EDA), this feature differentiated between Fear and Happy emotions. In fact, despite the minimum and median values of the three boxes being very closer, the boxplot of the Happy elicitation presents higher values compared to the other boxplots, while the Fear elicitation presents the lowest values. The means of the three states are highly influenced by the outliers. Furthermore, the two features, specially SCR_Height, have a considerable number of outliers which can explain the unexpected statistical differences.
Figure 6 presents the boxplots of several features obtained from the ECG signal. None of these features differentiates between any emotion elicitation. Despite some slight differences, the boxplots and the means of these features are very similar across the different emotional states.

Boxplots of several features of the ECG signal. The \(\blacklozenge \) stands for outliers and the
 stands for the mean of the features within each emotion. (Color figure online)
stands for the mean of the features within each emotion. (Color figure online)
Fig. 7 presents boxplots from features extracted from the EDA signal, and none presents statistical significant differences regarding emotion elicitation. Although some outliers, the means computed for each emotion are close to each other and distributions are similar.

Boxplots of several features of the EDA signal. The \(\blacklozenge \) stands for outliers and the
 stands for the mean of the features within each emotion. (Color figure online)
stands for the mean of the features within each emotion. (Color figure online)
Figure 8 shows the boxplots of features computed from the EMG signals from both the trapezius and triceps muscles, presenting a great number of outliers. For the same feature, the values obtained from triceps muscle are lower than those obtained from trapezius, which indicates that trapezius was more activated. Regarding the features from the triceps muscle, despite, consistently, presenting lowest values for Neutral state, the Friedman test did not find any statistical difference between emotional conditions. For the features obtained through the EMG from trapezius, the values and the boxplots are similar for the three emotional elicitation, and Friedman test did not report significant differences between emotional states for any feature.

Boxplots of several features of the EMG signal of both triceps and trapezius muscles. The \(\blacklozenge \) stands for outliers and the
 stands for the mean of the features within each emotion.
stands for the mean of the features within each emotion.
The obtained results for the four physiological signals analyzed support the hypothesis that the physiological response to pain is not influenced by emotional elicitation.
5 Discussion
The aim of this work was to show that emotional elicitation influences the way pain is perceived, but it has no influence on physiological response to pain.
The related works presented supports the idea that emotion has a correlation with pain perception, namely the works of Zhang et. al [10] and Srisopa et. al [8]. Both articles studied the influence of the emotional state on pain perceived (with different pain origins) and the results lead to the conclusion that negative emotions affect the way pain is perceived [10] and emotion modulation can help to manage pain [8].
In the work of Silva and Sebastião [7] the emotion elicitation was performed during the CPT task. The authors found that this strategy was not adequate since many of the participants did not pay enough attention to the video due to the pain felt at the same time. The current protocol was implemented considering the strategy of watching the video before the CPT, anticipated that this adjustment would elicit emotions. However, although differences regarding scores and times for pain tolerance and threshold, the discrepancy in pain perception was not highlighted.
Also, despite the protocol being thoroughly explained to the participants and all the doubts being addressed, some participants did not understand that they were required to report the time they first perceived pain. Consequently, they only reported pain when specifically asked to do so. This may lead to increased values of pain perception in some cases. By re-evaluating the violinplots of pain perception (Fig. 4), this observation is evident from the long tails of the violins. Additionally, some participants reported being confused when evaluating the pain felt using the NPS, struggling to choose the appropriate number.
Another factor that may have hindered emotional elicitation is the fact that some participants had already watched the movies from which the excerpts were taken. Consequently, in this case, the video was unable to elicit emotion, especially fear.
With regard to gender, the distribution of the violinplots for scores and pain threshold seems to be in line with the conclusions of Zhang et. al [10] that males present higher pain threshold and tolerance.
Concerning the second hypothesis, there were only two features among the 52 studied that could distinguish between elicited emotions. This supports the hypothesis that the emotion elicited does not influence on the physiological response to pain. The physiological system shows the same response to pain regardless the emotional state.
6 Conclusions and Further Research
In this work, a protocol for pain induction with previous emotional elicitation was conducted.
The state of the art shows that the emotional state of a person influences the way pain is perceived but has no influence on physiological pain response.
The results showed that emotion elicitation was not clearly achieved, since the pain perception was slightly modified despite the emotional video visualized, which may be due to the time elapsed between the emotional elicitation and the pain induction.
On other hand, as expected, the results showed emotional states pose no influence on the physiological response to pain.
Regarding the encouraging results, further research should be concerned with the design of a protocol to specifically attain the emotional elicitation in order to ensure that emotional states still elicited during pain induction.
With respect to the physiological response to pain, the collected data should be deeper analyzed in order to find relevant patterns and to extract important information for pain prediction. It would also be worthwhile to obtain feature validation from clinical experts and conduct a selection process based on these inputs. Moreover, participant-independent strategies for training and testing the models should be considered, as well as attaining the development of personalized models fitted only with data from the same participant.
As this work emerges within the scope of the EMPA project, the database, fully anonymized, will become available to the scientific community once data collection is complete.
Notes
- 1.
https://www.pluxbiosignals.com/apps/builder/biosignalsplux-kit-builder (accessed 20 July 2023).
- 2.
https://neuropsychology.github.io/NeuroKit/ (Accessed 9 July 2023).
References
Scipy.stats.shapiro - Scipy v1.11.1 manual. https://docs.scipy.org/doc/scipy/reference/ generated/scipy.stats.shapiro.html, Accessed 10 Jul 2023
von Baeyer, C.L., Piira, T., Chambers, C.T., Trapanotto, M., Zeltzer, L.K.: Guidelines for the cold pressor task as an experimental pain stimulus for use with children. J. Pain 6(4), 218–227 (2005)
Boonnithi, S., Phongsuphap, S.: Comparison of heart rate variability measures for mental stress detection. In: 2011 Computing in Cardiology, vol. 38, pp. 85–88 (2011)
Lumley, M.A., et al.: Pain and emotion: a biopsychosocial review of recent research. J. Clin. Psychol. 67(9), 942–968 (2011)
Salahuddin, L., Cho, J., Jeong, M.G., Kim, D.: Ultra short term analysis of heart rate variability for monitoring mental stress in mobile settings. In: 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, IEEE, August 2007. https://doi.org/10.1109/iembs.2007.4353378
Sebastião, R., Bento, A., Brás, S.: Analysis of physiological responses during pain induction. Sensors 22(23) (2022). https://doi.org/10.3390/s22239276
Silva, P., Sebastião, R.: Using the electrocardiogram for pain classification under emotional contexts. Sensors 23(3) (2023). https://doi.org/10.3390/s23031443
Srisopa, P., Cong, X., Russell, B., Lucas, R.: The role of emotion regulation in pain management among women from labor to three months postpartum: an integrative review. Pain Manag. Nurs. 22(6), 783–790 (2021)
Werner, P., Lopez-Martinez, D., Walter, S., Al-Hamadi, A., Gruss, S., Picard, R.W.: Automatic recognition methods supporting pain assessment: A survey. IEEE Trans. Affect. Comput. 13(1), 530–552 (2022)
Zhang, H., Bi, Y., Hou, X., Lu, X., Tu, Y., Hu, L.: The role of negative emotions in sex differences in pain sensitivity. Neuroimage 245(118685), 118685 (2021)
Acknowledgements
This work was funded by national funds through FCT - Fundação para a Ciência e a Tecnologia, I.P., under the grant UI/BI62/10827/2023 (B.A.), and the Scientific Employment Stimulus CEECIND/03986/2018 (R.S.) and CEECINST/00013/2021 (R.S.). This work is also supported by the FCT through national funds, within the R &D unit IEETA/UA (UIDB/00127/2020) and under the project EMPA (2022.05005.PTDC). We extend our sincere appreciation to all the volunteers who participated in the study, as well as to Ana Carolina Almeida and Daniela Pais for their collaboration in data collection and pilot tests.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2024 Springer Nature Switzerland AG
About this paper

Cite this paper
Alves, B., Silva, C., Sebastião, R. (2024). Do Emotional States Influence Physiological Pain Responses?. In: Vasconcelos, V., Domingues, I., Paredes, S. (eds) Progress in Pattern Recognition, Image Analysis, Computer Vision, and Applications. CIARP 2023. Lecture Notes in Computer Science, vol 14470. Springer, Cham. https://doi.org/10.1007/978-3-031-49249-5_9
Download citation
DOI: https://doi.org/10.1007/978-3-031-49249-5_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-49248-8
Online ISBN: 978-3-031-49249-5
eBook Packages: Computer ScienceComputer Science (R0)
