
Abstract
In this chapter, we describe a study assessing the emotional response of terminally ill cancer patients to a music therapy (MT) intervention in a randomized controlled trial. Instantaneous emotional indicators in the form of a coordinate in the arousal–valence plane were extracted from the patients’ brain activity data. The emotional indicators were analysed in order to quantify the overall emotional effect of MT on the patients compared to controls, as well as the relative effect of the different MT techniques applied during the MT intervention. The intervention produced a significant increase in positivity and arousal, while no significant changes were found in controls. These results can be interpreted as a positive emotional effect of MT in palliative care patients. Grounded on the results of this study, we propose a music-based intervention protocol for improving the emotional state of patients in palliative care.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others
Keywords
- Palliative care
- Cancer
- Anxiety
- MT
- Statistically significant
- Alpha activity
- Beta activity
- Correlation
- Emotions
- Edmonton symptom assessment system
- ESAS
6.1 Palliative Care
In 2008, the World Health Organization defined palliative care as “an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.” It is an interdisciplinary approach to specialized medical and nursing care for individuals with life-limiting illnesses. It focuses on providing relief from the symptoms, pain, and psychological stress of a serious illness, regardless of diagnosis. The goal is to improve the quality of life for both the patient and the family. Historically, palliative care emerged as a response to the needs of the terminally ill, primarily cancer patients. Dame Cicely Saunders, often considered the founder of the modern hospice movement, established the first hospice centre, St. Christopher’s Hospice, in the United Kingdom in 1967. The movement sought to address the unmet needs of patients facing the end of life, emphasizing comfort, dignity, and quality of remaining life.
Palliative care, as a holistic approach, underscores the importance of treating the person rather than just the disease. With its patient and family-centred focus, it bridges the often-existing gap between medical interventions and quality, compassionate care. As medical advancements increase the life span and change the nature of life-limiting diseases, the role of palliative care becomes even more critical. Ensuring its understanding, accessibility, and integration into the broader healthcare system is imperative for the modern era.
6.2 Music and Palliative Care
Helping patients in palliative care and their families to cope effectively with the pain, worries, and emotional impact inherent in the diagnosis of terminal illnesses is a recurrent challenge for doctors and nurses in palliative units. In this context, music therapy may be considered a candidate for helping to cope and provide emotional and physical comfort to patients and their families. Active music therapy (for instance, interactive live music performances) delivered by trained music therapists using singing voice and musical instruments can engage patients in ways that receptive music therapy (e.g. pre-recorded music) cannot (Standley 1986; Standley and Hanser 1995). Studies have found that live music is more effective than pre-recorded music with adult cancer patients, i.e. patients over 17 years old (MacGill 1983). Live MT allows for personalized interactions which may be particularly important for patients who relate best to music which is relevant to their special current situation (Stecher et al. 1972). In clinical palliative care, where the patient’s medical condition is not likely to be improved, the objective of MT is often to improve the patient’s quality of life, e.g. the improvement of pain, stress, and help to regulate negative emotions, e.g. depression, anxiety, anger (Planas et al. 2015), as well as to enhance communication (Warth et al. 2014). MT has been associated with a reduction of anxiety (Nguyen 2003; Horne-Thompson and Grocke 2008) and pain (Krout 2001; Lee 2005; Curtis 2011; Gutgsell et al. 2013), in addition to enhancing communication (Brown 2006) and spiritual well-being (Wlodarczyk 2007). Hilliard (2003) reported a significant improvement in quality of life in terminally ill patients using MT compared to standard medical care only. Nakayama et al. (2009) reported a decrease in salivary cortisol levels after nine participants received a receptive MT session. Furthermore, MT has been found not only useful for end-of-life patients but also for family and caregivers (O’Callaghan 2009). However, current reviews consistently state that there is a lack of rigorous studies providing quantitative grounds for recommending or not the use of MT in the context of palliative care (Korczak et al. 2013; Bradt and Dileo 2014). The 2010 Cochrane Review on MT clinical interventions in palliative care reported that only five trials had implemented (quasi-) randomized controlled designs (Bradt and Dileo 2014).
Recently, the neural correlates of music-evoked emotion have been investigated by the neuroscientific community using both functional magnetic resonance imaging and electroencephalography (EEG) techniques. In particular, EEG brain activity information has been used to detect emotional states in humans (Choppin 2000; Takahashi 2004; Bos 2007; Lin et al. 2010; Ramirez and Vamvakousis 2012). Patterns of EEG activity have been found to distinguish emotions induced by stimuli with different valence and arousal levels. Asymmetry patterns in frontal EEG activity have been found to distinguish between positive and negative valence, and patterns of overall frontal EEG activity have been found to identify high and low arousal levels (Schmidt and Trainor 2001; Ramirez and Vamvakousis 2012). Ramirez et al. (2015) have described an approach to computing in real-time continuous arousal and valence values from EEG activity: Based on the EEG signal of a person, the arousal level was determined by computing the ratio of the beta (12–28 Hz) and alpha (8–12 Hz) brainwaves in the prefrontal cortex, while valence values were computed by comparing the alpha power activation levels of the left and right cortical hemispheres.
In this chapter, we describe a study which contributes to the understanding of the emotional effect (estimated by EEG information) of MT in the context of palliative care. More precisely, the study aims to evaluate the effectiveness of a particular MT intervention (a 30-min session including active and receptive MT techniques) for improving the emotional state (e.g. stress, anxiety, anger, and depression) of palliative care patients by analysing their EEG activity. The patients’ emotional states were estimated before, during, and after MT sessions in order to evaluate the general emotional effect of the MT session and to assess the emotional effect of particular (active and receptive) MT techniques. With this aim, 40 patients were randomized and assigned to two groups: the first group, the experimental group (EG), participated in an MT session, while the second (control) group was provided with company. The EEG-based estimated emotional state effects of MT on participants in the EG were compared with the effects of the company on participants in the control group (CG). This study represents the first clinical randomized controlled trial to examine the emotional effects of MT in palliative care using brain activity information.
6.3 Research: Emotions and Music Therapy in Palliative Care – An EEG Study
6.3.1 Participants
The research reported in this chapter is the result of a collaboration between the palliative care unit (PCU), Oncology Service, Parc de Salut Mar in Barcelona, and the Universitat Pompeu Fabra, Barcelona, Spain. Recruitment, interventions, and data collection were carried out at the PCU. Data processing and analysis were carried out at the Universitat Pompeu Fabra. All patients were assessed for eligibility according to predefined inclusion and exclusion criteria shown in Table 6.1. Forty adults (13 females and 27 males, mean = 69 years old, SD = 15) with normal hearing participated in the study of which 20 were randomly selected to participate in an MT intervention consisting of both active and receptive techniques, and the other 20 participants were provided with company by the music therapists, but no music was involved in their sessions. Patients were randomly assigned to the MT group or to the company group by using the method of randomly permuted blocks. Participants granted their written consent, and the study procedures were positively evaluated by the Clinical Research Ethical Committee of the Parc de Salut Mar (CEIC-Parc de Salut Mar), Barcelona, Spain. All participants were patients admitted to the PCU.
6.3.2 Materials
Music Material
Prior to the MT session, participants in the EG were interviewed about their music preferences in order to identify particular pieces to be included in their MT session. Music included both instrumental and vocal pieces in a variety of music genres (both classical and popular music), e.g. Canon de Pachelbel, La Bella Lola, Rien de rien, Hey Jude, and Color Esperanza.
Data Acquisition and Processing
Brain activity data were acquired in the same manner as described in Chap. 3: The Emotiv EPOC EEG system (Emotiv 2014; Badcock et al. 2013) was used for the acquisition of EEG data.
6.3.3 Methods
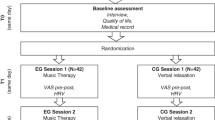
Patients eligible for inclusion in the study were contacted at the palliative care unit (PCU), Oncology Service, and informed about the procedures and objectives of the study. Patients received no information about which of the two interventions was the actual experimental condition. If patients agreed to participate, they were asked to sign the informed consent form. Participants were treated individually. Participants in the EG received an MT session of approximately 30 min. The sessions were conducted by three professional music therapists with extensive experience in palliative care. Each MT session consisted of a receptive song, an active song, and a relaxation/imaginative receptive intervention. EEG data was recorded before the MT session, during the session, and at the end of the session. Participants in the CG were accompanied by the same music therapists for approximately 30 min in which they conversed freely about music and their music preferences. All participants received similar levels of medication at the moment of the study. Figure 6.1 shows a flow diagram of the study design.

Flow diagram of the study design
Similarly to the data analysis in Chap. 3, the patients’ EEG data were transformed into a coordinate in Thayer’s arousal–valence emotion plane (Thayer 1989), following the approach by Ramirez and Vamvakousis (2012). Artefact detection/elimination was performed by visual inspection of the signal. EEG data were normalized to avoid inter-participant variability. Using the EEG signal of a participant, the arousal level was computed as the ratio of the beta (12–28 Hz) and alpha (8–12 Hz) brainwaves (see Eq. 3.1 in Chap. 3) recorded in four locations in the prefrontal cortex: AF3, AF4, F3, and F4 (see Fig. 3.1 in Chap. 3). Valence values were obtained by computing the difference of alpha power in channels F4 and F3 (see Eq. 3.2 in Chap. 3).
6.3.4 Results
Among the symptoms assessed with Edmonton Symptom Assessment System (ESAS), tiredness (p = 0.002), anxiety (p = 0.002), breathing difficulty (p = 0.042), and well-being (p = 0.036) showed statistically significant improvement between pre- and post-values in the EG. No statistically significant differences were found in the pre- and post-values of these indicators in the CG.
Using the EEG data obtained during both the MT sessions and the company sessions, average valence and arousal values were computed at the beginning and at the end of the sessions (see Table 6.2). Average valence values in Table 6.2 correspond to the average degree of relative alpha activity in the left frontal lobe, thus larger values are associated with more positive emotional states. Average arousal values on the other hand correspond to either more beta activity or less alpha activity (or both) in the frontal lobe, and thus larger values represent higher arousal states. For the EG, the average arousal scores at the start and end of the session were −0.3 (0.25) and −0.19 (0.18), respectively. Meanwhile, the average valence scores for the start and end of the session were −0.23 (0.16) and 0.08 (0.17), respectively. For the CG, the average arousal scores at the beginning and conclusion of the session were −0.35 (0.25) and −0.24 (0.24), respectively. The valence scores, on the other hand, were −0.16 (0.38) at the start and −0.11 (0.33) at the end of the session.
In the EG, both the difference between arousal values (p = 0.003) and the difference between valence values (p = 0.0004) at the beginning and the end of the MT sessions were statistically significant. No significant differences were found in the CG.
Figure 6.2 shows the correlation within a session between time and the computed average arousal (orange line) and valence (blue line) values, for the EG. Periods in time correspond to each of the session sections: beginning, receptive song, active song, receptive imaginative intervention, and end of session. For arousal, the obtained correlation was r = 0.63 (p = 0.25), while for valence it was r = 0.89 (p = 0.04).

The experimental group averaged arousal (orange) and valence (blue) levels over time. 1 = beginning, 2 = receptive song, 3 = active song, 4 = receptive imaginative intervention, and 5 = end of session
Figure 6.3 shows the plot in the arousal/valence plane for the averaged estimated emotional state of participants in the EG during the music therapy session: (1) initial state, (2) receptive song, (3) active song, (4) receptive imaginative intervention, and (5) final state.

Plot in the arousal/valence plane for the averaged estimated emotional state of participants in the EG during one session: (1) initial state, (2) receptive song, (3) active song, (4) receptive imaginative intervention, and (5) final state
Discussion
Analysis of the qualitative self-reported data showed that 12 out of the 20 participants in the EG reported feeling less weak after the MT session compared with the beginning of the session (while none of the other participants in the group reported increased weakness), confirming the reported statistically significant difference (p = 0.002) between pre- and post-weakness self-reported values. On the other hand, 6 out of the 20 participants in the CG reported feeling weaker after the company session (while only two reported feeling less weak). Similarly, 11 out of the 20 participants in the EG reported feeling less anxious, and 12 were in a better mood after the MT session compared to their self-reported values at the beginning of the session. This is in line with the statistically significant decrease in anxiety (p = 0.002) and increase in mood (p = 0.036).
Electroencephalography data obtained showed that the overall valence level of the participants in the EG was significantly higher at the end of the MT session compared to the starting level (p = 0.0004). This was not the case in the CG where no significant difference in valence levels was found. This result should be interpreted as a decrease of relative alpha activity in the left frontal lobe in the EG participants, which may be interpreted as an improvement of mood or a lessening of depressive mood (Henriques and Davidson 1991; Gotlib et al. 1999; Ramirez et al. 2015). This reinforces the significant improvement results in self-assessment mood reported by the participants in the EG. Similarly, arousal values at the beginning and at the end of the MT session showed a smaller but nevertheless significant difference (p = 0.003) in the EG, while no difference in arousal values was found in the CG. The lower p-value for arousal may be due to the fact that while most of the patients with terminal cancer are naturally in a low arousal state (e.g. low mood or depressed), there may be some patients who feel anxious, i.e. are already in a high arousal state. EEG data also showed a significant improvement in valence in participants in the EG, reflecting a positive change in their initial emotional state. It is worth noting that while there was a continuous improvement in the participants’ valence throughout the whole MT session, the first MT intervention (i.e. the receptive song) alone produced a significant improvement in valence (p = 0.0019) when compared to the EG participants’ initial state.
Regarding the relative effects of the different MT techniques applied during the session (i.e. passive listening, active listening, and relaxation), relaxation produced significantly lower arousal levels than active listening in participants in the EG (p = 0.025). This result was expected since the relaxation technique is normally used for managing both psychologically and physiologically agitated states. Surprisingly, no similar significant differences were found between relaxation and passive listening. No relatively significant differences in valence were found between passive listening, active listening, and relaxation.
In the EG, no significant correlation between arousal values and time was found. This may be because of differences between the participants’ states of arousal, as previously mentioned, to the different MT techniques used in the sessions, or the differences between participants’ sensitivity to music. Interestingly, the correlation between computed valence levels and time within the MT session was found significant (p = 0.038), which represents a gradual and constant improvement in the EG participants’ valence emotional state. It has to be noted that the time and type of MT intervention are confounded, thus this result has to be investigated further in order to establish if it is due to the natural progression of the MT session or to the particular sequence of interventions.
Considering the observed improvements in valence levels in one MT session and the limited duration of each session (i.e. approximately 30 min), it seems possible that further improvement in valence levels may have been obtained if sessions had been longer and/or if treatment had consisted of more sessions. Unfortunately, due to the very short lifespan (2 weeks on average) of the participants in the study, it was impossible to program more than one MT session per participant. In the past, only a few studies in the literature have investigated the long-term effect of MT. In the current study, no follow-up of the participants in order to examine the long-term effect of MT was possible. We plan to investigate this issue further, perhaps considering a different group of patients.
In summary, the results obtained in this study seem to indicate that MT techniques (both active and receptive) can be useful tools for modulating the emotional state of end-of-life patients. Helping such patients to modulate their emotions may improve their quality of life by helping them cope with the emotional effects inherent in their condition. Although this study is limited in scope due to the use of only one MT session per participant, it provides an evidence-based rationale for MT in palliative care based on methods involving brain activity (EEG) data. Furthermore, the results obtained open the possibility for personalized MT interventions based on patients’ emotional states before MT is applied.
6.4 Protocol: Music Therapy Intervention for Palliative Care Patients
The purpose of this protocol is to apply music therapy (MT) and evaluate its effectiveness in improving the emotional state and physiological symptoms of palliative care patients. The protocol is grounded on the results of the study described earlier in this chapter at the palliative care unit (PCU), Oncology Service, Parc de Salut Mar.
-
Inclusion criteria: Patients who are receiving palliative care and who are able to provide informed consent are eligible to participate in the study.
-
Exclusion criteria: Patients in the agony phase, with cognitive impairment, with deafness, or who are restless or agitated.
Methodology
-
Participants will be informed about the procedures and objectives of the intervention and will sign the informed consent form.
-
Before the intervention, participants will complete the Edmonton Symptom Assessment System (ESAS). In addition to the nine symptoms considered in ESAS which are pain, tiredness, nausea, depression, anxiety, drowsiness, appetite, well-being, and shortness of breath, patients will give a self-report of their arousal and valence states. The degree of severity of each symptom/state is rated on a 0–10 numerical scale.
-
Participants will receive a 30-min MT session conducted by one or more professional music therapists with experience in palliative care. The MT session may consist of a receptive song, an active song, and a relaxation/imaginative receptive intervention. Depending on the initial emotional state of the patient, the music therapist may focus more on a particular technique as follows:
-
For patients with low arousal states, for instance, depression states: focus on active song and receptive song interventions.
-
For patients with high arousal states, for instance, anxious states: focus on relaxation/imaginative receptive intervention and receptive song.
-
-
After the intervention, participants will complete the Edmonton Symptom Assessment System (ESAS), as well as their self-reported arousal and valence levels.
-
Obtained (pre- and post-) ESAS data and self-reported arousal and valence levels will be analysed to determine statistical significance.
Outcome Measures
The primary outcome measure will be the difference between pre- and post-ESAS scores and arousal and valence levels. Secondary outcome measures will include music therapist observations and subjective reports of symptom relief.
This clinical protocol aims to improve the emotional state and physiological symptoms of palliative care patients and provide evidence for the effectiveness of MT as a palliative care intervention. The intervention will contribute to the understanding of how MT can improve the emotional state and the subjective and physiological symptoms of palliative care patients.
6.5 Chapter Summary
This chapter explores the benefits of music therapy to improve the emotional state and physiological symptoms of palliative care patients. We present the findings of a randomized controlled trial aimed at evaluating the impact of music therapy (MT) on terminally ill cancer patients’ emotional responses. EEG-based emotion detection techniques were employed to extract instantaneous emotional indicators from the patients’ brain activity data. These indicators, in the form of a coordinate in the arousal–valence plane, were analysed to quantify the overall emotional effect of MT on the patients, as well as the relative effect of different MT techniques used during the intervention. Our results showed a significant increase in positivity and arousal among the intervention group, while no significant changes were observed in the control group. These findings suggest a positive emotional effect of MT in palliative care patients. Building upon these results, we propose a music-based intervention protocol to improve the well-being of patients in palliative care.
References
Badcock NA, Mousikou P, Mahajan Y, de Lissa P, Johnson T, McArthur G (2013) Validation of the emotiv EPOC® EEG gaming system for measuring research quality auditory ERPs. PeerJ 1:e38. https://doi.org/10.7717/peerj.38
Bos DO (2007) EEG-based emotion recognition: the influence of visual and auditory stimuli. Emotion 57:1798–1806
Bradt J, Dileo C (2014) Music therapy for end-of-life care. Cochrane Database Syst Rev 1:CD007169. https://doi.org/10.1002/14651858.CD007169.pub3
Brown J (2006) Comparison of the effects of music and conversation on hospice patient’s predisposition to communicate and communication behaviors. Master’s thesis, Florida State University, Tallahassee
Choppin A (2000) EEG-based human interface for disabled individuals: emotion expression with neural networks. Master’s thesis, Tokyo Institute of Technology, Yokohama
Curtis SL (2011) Music therapy and the symphony: a university-community collaborative project in palliative care. Music Med 3:20–26. https://doi.org/10.1177/1943862110389618
Emotiv Systems Inc (2014) Researchers. Available at: http://www.emotiv.com
Gotlib IH, Ranganath C, Rosenfeld JP (1999) EEG alpha asymmetry, depression, and cognitive functioning. Cogn. Emot. 12:449–478. https://doi.org/10.1080/026999398379673
Gutgsell KJ, Schluchter M, Margevicius S, DeGolia PA, McLaughlin B, Harris M et al (2013) Music therapy reduces pain in palliative care patients: a randomized controlled trial. J Pain Symptom Manag 45:822–831. https://doi.org/10.1016/j.jpainsymman.2012.05.008
Henriques JB, Davidson RJ (1991) Left frontal hypoactivation in depression. J Abnorm Psychol 100:535–545. https://doi.org/10.1037/0021-843X.100.4.535
Hilliard RE (2003) The effects of music therapy on the quality and length of life of people diagnosed with terminal cancer. J Music Ther 40:113–137. https://doi.org/10.1093/jmt/40.2.113
Horne-Thompson A, Grocke D (2008) The effect of music therapy on anxiety in patients who are terminally ill. J Palliat Med 11:582–590. https://doi.org/10.1089/jpm.2007.0193
Korczak D, Wastian M, Schneider M (2013) Music therapy in palliative setting. GMS Health Technol 9:Doc07. https://doi.org/10.3205/hta000113
Krout RE (2001) The effects of single-session music therapy interventions on the observed and self-reported levels of pain control, physical comfort, and relaxation of hospice patients. Am J Hosp Palliat Care 18:383–390. https://doi.org/10.1177/104990910101800607
Lee H (2005) The effect of live music via the ISO-priniciple on pain management in palliative care as measured by self-report using a graphic rating scale (GRS) and pulse rate. Master’s thesis, Florida State University, Tallahassee
Lin Y-P, Wang C-H, Jung T-P, Wu T-L, Jeng S-K, Duann J-R et al (2010) EEG-based emotion recognition in music listening. IEEE Trans Biomed Eng 57:1798–1806. https://doi.org/10.1109/TBME.2010.2048568
MacGill BL (1983) The effects of live music versus tape recorded music on hospitalized cancer patients. Music Ther 3:17–28. https://doi.org/10.1093/mt/3.1.17
Nakayama H, Kikuta F, Takeda H (2009) A pilot study on effectiveness of music therapy in hospice in Japan. J Music Ther 46:160–172. https://doi.org/10.1093/jmt/46.2.160
Nguyen J (2003) The effect of music therapy on end-of-life patients’ quality of life, emotional state, and family satisfaction as measured by self-report. Master’s thesis, Florida State University, Tallahassee
O’Callaghan C (2009) Objectivist and constructivist music therapy research in oncology and palliative care: an overview and reflection. Music Med. 1:41–60. https://doi.org/10.1177/1943862109337135
Planas J, Escudé N, Farriols C, Villar H, Mercadé J, Ruiz AI (2015) Effectiveness of music therapy in advanced cancer patients admitted to a palliative care unit: a non-randomized controlled. Clin Trial Music Med 7:23–31
Ramirez R, Vamvakousis Z (2012) Detecting emotion from EEG signals using the emotive Epoc device. In: Proceedings of the 2012 International conference on brain informatics, LNCS 7670. Springer, Macau, pp 175–184. https://doi.org/10.1007/978-3-642-35139-6_17
Ramirez R, Palencia-Lefler M, Giraldo S, Vamvakousis Z (2015) Musical neurofeedback for treating depression in elderly people. Front Neurosci 9:354. https://doi.org/10.3389/fnins.2015.00354
Schmidt LA, Trainor LJ (2001) Frontal brain electrical activity (EEG) distinguishes valence and intensity of musical emotions. Cogn Emot 15:487–500. https://doi.org/10.1080/02699930126048
Standley JM (1986) Music research in medical/dental treatment: meta-analysis and clinical implications. J Music Ther 23:56–122. https://doi.org/10.1093/jmt/23.2.56
Standley JM, Hanser SB (1995) Music therapy research and applications in pediatric oncology treatment. J Pediatr Oncol Nurs 12:3–8. https://doi.org/10.1177/104345429501200103
Stecher MB, McElheny H, Greenwood M (1972) Music and movement improvisations (threshold early learning library), vol 4. Macmillan, New York
Takahashi K (2004) Remarks on emotion recognition from bio-potential signals. In: 2nd International conference on autonomous robots and agents, Palmerston North, pp 186–191
Thayer RE (1989) The biopsychology of mood and arousal. Oxford University Press, New York
Warth M, Koenig J, Keßler J, Wormit AF, Hillecke TK, Bardenheuer HJ (2014) Musiktherapie in der palliativmedizinischen versorgung: gegenwärtiger stand und aktuelle entwicklungen. Musikther Umsch 35:331–343. https://doi.org/10.13109/muum.2014.35.4.261
Wlodarczyk N (2007) The effect of music therapy on the spirituality of persons in an in-patient hospice unit as measured by self-report. J Music Ther 44:113–122
Author information
Authors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Ramirez-Melendez, R. (2023). Emotions and Music in Palliative Care. In: Neurocognitive Music Therapy. Springer, Cham. https://doi.org/10.1007/978-3-031-48635-7_6
Download citation
DOI: https://doi.org/10.1007/978-3-031-48635-7_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-48634-0
Online ISBN: 978-3-031-48635-7
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)