
Abstract
The role of prophylactic central neck dissection (pCND) in patients with low risk, clinically node negative (cN0) papillary thyroid cancer (PTC) is controversial. In this chapter, the best available evidence regarding the management of lymph nodes in the central compartment of the neck is analyzed. Rates of recurrence and complications were reviewed for patients with cN0 PTC treated with or without pCND. The important findings are that there is a potential for a small reduction in recurrence following pCND, but with higher rates of temporary and permanent hypoparathyroidism. In the absence of a clear oncologic benefit for pCND, the higher rate of complications outweigh the potential small reduction in recurrence for patients with low risk, cN0 PTC. As a result, pCND does not appear to be justified for treatment of low risk PTC.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Central neck dissection
- Prophylactic central neck dissection
- Lymph node metastases
- Papillary thyroid cancer
- Low risk papillary thyroid cancer
- Clinically node negative papillary thyroid cancer
Case Presentation
A 48-year-old woman was found to have a 3-cm thyroid nodule on a routine physical examination. She had no compressive symptoms, no prior history of head or neck irradiation, and had no family history of thyroid cancer or other endocrinopathies.
On physical examination, she had a 3-cm firm nodule palpable in the right lobe of the thyroid gland. She had no palpable nodules in the isthmus or the left lobe of the thyroid gland. Her trachea was midline. She had no palpable cervical or supraclavicular lymphadenopathy.
Her serum TSH level was 2.107 uIU/ml (0.450–5.330 uIU/ml). A comprehensive ultrasound examination of the neck revealed a 3.0 × 1.6 × 2.9 cm solid, hypoechoic nodule with irregular margins and punctate calcifications in the right lobe of the thyroid gland, classified as TI-RADS 5 (highly suspicious for cancer). There was a 1.3 × 0.8 × 1.2 cm solid, isoechoic nodule in the posterior, superior aspect of left lobe of the thyroid gland, classified as TI-RADS 3. There were no enlarged or abnormal lymph nodes in the central or lateral compartments of the neck.
A fine needle aspiration biopsy (FNAB) of the 3.0-cm nodule in the right lobe of the thyroid gland revealed papillary cancer. After extensive discussion with the patient, she elected for total thyroidectomy. The patient and her endocrinologist ask whether a central neck dissection will be performed during the total thyroidectomy.
Background
Lymph node (LN) metastases are common in patients with papillary thyroid cancer (PTC). LN metastases from PTC most commonly occur in the central compartment of the neck and spread sequentially via the lymphatics to the lateral neck and the superior mediastinum. Risk factors for LN metastases and recurrence include increased tumor size, extrathyroidal extension (ETE), multifocal disease, and extremes of age. In contrast to other malignancies, clinically apparent LN metastases in patients with PTC have no effect on survival in younger patients and likely have only a small effect on disease-specific survival in patients 45 years or older [1, 2]. LN metastases, however, are associated with increased rates of recurrence [3].
Clinically apparent macroscopic LN metastases (cN1) occur in 20–31% of patients with PTC [4] and are associated with increased regional recurrence. LN metastases have been associated with reduced survival in older patients [1, 2]. Total thyroidectomy and therapeutic central compartment neck dissection (CND) are the recommended surgical treatment for cN1 disease in order to reduce recurrence and improve survival [5, 6].
The role of prophylactic central neck dissection (pCND) for patients with no evidence of LN metastases on physical examination, preoperative imaging, or intraoperative evaluation remains controversial. This is due to the significant limitations of retrospective studies and the fact that only two small randomized controlled trials (RCTs) have been published to date [7, 8]. Studies differ in their definitions of recurrence, extent of thyroidectomy (hemithyroidectomy versus total thyroidectomy), extent of pCND (unilateral or bilateral), administration and dosing of radioiodine, and length of follow-up. Most of the published studies have significant selection bias.
Approximately 40–50% of patients with PTC have occult micrometastases in central neck LNs [4, 9]. Micrometastases are defined by sizes less than <2 mm [6]. Despite the high incidence of occult micrometastases, the rate of recurrence in the central neck has been reported to be only 2% whether or not a pCND is performed [10]. This relatively low recurrence rate, combined with the overall excellent prognosis for patients with PTC and central neck micrometastases suggests that micrometastases rarely progress to clinically significant disease. As a result, the benefit of pCND for clinically node-negative disease (cN0) is questionable.
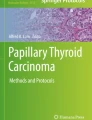
The anatomic boundaries of the central compartment of the neck (Fig. 11.1) are the hyoid bone superiorly, the innominate artery inferiorly, the common carotid arteries laterally, the prevertebral fascia posteriorly, and the superficial layer of the deep cervical fascia anteriorly [11]. The LNs in the central compartment of the neck are categorized as level VI and level VII LNs. Level VI LNs include the prelaryngeal (Delphian) LNs, which are superior to the isthmus in the midline of the neck; the pretracheal LNs, which are inferior to the isthmus along the anterior surface of the trachea; and the right and left paratracheal lymph nodes, which are present along the course of the RLNs between the common carotid arteries and the trachea. Level VII lymph nodes are the superior mediastinal LNs associated with the innominate artery and veins.

Fig. 11.1 Anatomic boundaries for the central compartment of the neck and the lymph nodes that are removed in a central compartment neck dissection. (C common carotid artery, H hyoid bone, I innominate artery, LIV left innominate vein, RLN recurrent laryngeal nerve)
A CND involves removal of all lymph nodes and fibrofatty tissue from the central compartment of the neck. A unilateral CND includes removal of the prelaryngeal, pretracheal, superior mediastinal, and paratracheal LNs on the side of cancer. A bilateral CND includes removal of the prelaryngeal, pretracheal, superior mediastinal, and the right and left paratracheal LNs. A CND is classified as therapeutic when performed for the treatment of cN1 disease and as prophylactic when performed in patients with cN0 disease.
Prophylactic CND has been advocated by some surgeons because of its potential benefits, which include improved accuracy of staging and better selection of patients for I-131 administration, reduced postoperative thyroglobulin levels, reduced recurrence rates, and reduced need for reoperation in the central neck with its potential morbidity. However, pCND has been associated with higher risk of complications compared to thyroidectomy alone [7, 9, 12, 13]. Because of the potentially higher risk of complications following pCND, a unilateral CND has been recommended as an alternative for patients with cN0 disease to reduce potential injury to contralateral RLN and parathyroid glands. Alternatively, some surgeons have recommended that pCND not be performed at all because of lack of significant effect on locoregional recurrence, higher postoperative complication rates, and the potential for overuse of RAI without significant benefit. In our opinion, deciding whether to perform a pCND comes down to weighing the risks of permanent hypoparathyroidism and RLN injury versus the benefit of preventing recurrence and reoperation in the central compartment of the neck.
It has been estimated that a prospective RCT to study the effectiveness of pCND would require 5840 patients at a cost exceeding 15 million dollars [14]. This would be impractical and logistically challenging. As a result, review of data from high-quality observational studies and small prospective randomized controlled studies is required to determine the value, if any, of pCND in patients with cN0 PTC.
In this chapter, we will make recommendations and summarize the best available evidence regarding optimal pre- and intraoperative evaluation and management of central neck nodes for a patient with low risk, cN0 PTC. To determine whether or not pCND is of value in a patient with low risk, cN0 PTC, three questions will need to be addressed: (1) Is the rate of recurrence in the central compartment of the neck lower following pCND? (2) Is the rate of complications higher with pCND? and (3) Does the balance of potential risks and benefits justify performing pCND?
Preoperative Evaluation
Physical exam and comprehensive ultrasound (US) of the central and lateral neck are essential components of the preoperative evaluation of patients with PTC. Physical examination should include palpation of the thyroid gland, with attention to tumor size, location, consistency, mobility, additional nodules, tracheal deviation, and substernal extension. Palpation of the neck to evaluate for clinically apparent LN metastases should include the anterior and posterior cervical, supraclavicular, prelaryngeal, pretracheal, and paratracheal lymph node basins. Palpable cervical lymphadenopathy in a patient with PTC is suggestive of metastatic disease and requires further evaluation with ultrasound and fine needle aspiration biopsy (FNAB) of any abnormal nodes.
The positive predictive value of physical exam in detecting metastatic lateral neck disease in patients with PTC approaches 100%. However, the sensitivity of physical examination in detecting low-volume metastatic lymphadenopathy is only 19% [15]. High-resolution US is a much more sensitive method for detecting metastatic lateral neck disease [15, 16]. Preoperative neck US to evaluate for central and lateral neck compartment LNs is recommended in all patients with biopsy-proven PTC [5, 6].
In patients with a normal physical exam and known PTC, the US was able to identify metastatic disease in LNs of the lateral neck in 14–34% of patients and in the central compartment of the neck in 2–6% of patients [15, 17, 18]. Preoperative US identified suspicious cervical adenopathy in 20–31% of cases, altering the surgical approach in approximately 20% of patients [6, 15, 19]. Additional cross-sectional imaging, most commonly computed tomography with intravenous contrast, may augment ultrasound assessment in patients with a bulky primary, extensive nodal disease, nodes that extend inferiorly that cannot be fully evaluated by ultrasound, or if significant central neck nodal disease is suspected [20].
Preoperative neck ultrasound should be performed or interpreted by a clinician trained in thyroid pathology, using a high-resolution ultrasound scanner with a 7–14 mHz linear array transducer with real-time grayscale and color Doppler imaging [15, 18]. The central compartment (level VI) and the lateral compartments (levels II–V) of the neck should be examined. Sonographic features suggestive of a metastatic LN include size ≥10 mm, loss of a normal fatty hilum, rounded shape, hypoechogenicity, cystic change, microcalcifications, and peripheral vascularity [6, 15, 17, 18]. Confirmation of malignancy in LNs with suspicious US characteristics or enlarged physical exam is achieved by FNAB or intraoperative frozen section exam.
Preoperative FNAB of suspicious lymph nodes should be performed if it will change surgical management [5, 6]. If abnormal nodes are present in the lateral neck compartment, FNAB is performed to confirm metastatic disease to the lateral neck prior to performing a lateral neck dissection. Measurement of thyroglobulin from the needle washout of a FNAB may be helpful to diagnose metastasis in LNs that are cystic or specimens with inadequate cellularity for cytological evaluation [21, 22].
In the central neck, US evaluation of abnormal LNs is limited by the presence of the thyroid gland, and only half of abnormal central neck lymph nodes are detected preoperatively [23]. In addition, patients who have a history of Hashimoto thyroiditis commonly have benign reactive LNs in the central neck that may mimic metastatic disease. FNAB of suspicious central neck LNs can be avoided if intraoperative evaluation with a frozen section is planned or if therapeutic CND is planned based on US findings.
Intraoperative Evaluation
A systematic search and evaluation for abnormal LNs in the central compartment of the neck are routinely performed in patients with nodular thyroid disease and a FNAB that is malignant (Bethesda VI), indeterminate (Bethesda III, IV, and V), or nondiagnostic (Bethesda I). Abnormal LNs are enlarged, firm or rubbery, darker in color, or more rounded in shape.
A preliminary evaluation of the prelaryngeal and pretracheal regions for abnormal LNs occurs during the separation of the sternohyoid muscles in the midline of the neck to expose the thyroid gland. The search for abnormal prelaryngeal LNs is completed during the evaluation for a pyramidal lobe of the thyroid gland and exposure and resection of the pyramidal lobe. The area from the thyroid isthmus inferiorly to the hyoid bone superiorly is carefully examined.
The paratracheal areas, from the common carotid artery laterally to the trachea medially, are examined during the exposure and dissection of the RLNs. Special attention should be paid to the area dorsal to the RLN where abnormal LNs may be present, especially inferiorly on the right. Exposure of the paratracheal areas is optimized by retraction of the trachea medially.
The pretracheal area is further examined during the ligation of the inferior pole vessels and mobilization of the thyroid lobe and isthmus to the contralateral side of the trachea. The area from the inferior margin of the isthmus to the innominate artery is inspected. Inspection of the inferior aspect of the pretracheal area may be best accomplished after the exploration of the right paratracheal area and exposure of the innominate artery. Final evaluation of the pretracheal area is completed during the division of the ligament of Berry and removal of the contralateral lobe of the thyroid gland.
Discovery of an Abnormal LN
When abnormal LNs are discovered intraoperatively in the central neck of patients with PTC, there should be high suspicion of metastatic disease. In patients with concomitant Hashimoto thyroiditis and PTC, intraoperative nodal assessment is more challenging due to the frequent presence of inflammatory lymphadenopathy [20, 24]. A frozen section may be useful for evaluation of suspicious nodes. If positive for metastatic disease, therapeutic CND should be performed.
In patients with cN1 disease, a therapeutic bilateral CND is indicated. The operative report should specify that this is a therapeutic node dissection, and should specify the extent of dissection [11]. The goals of resection of clinically evident nodal metastasis are to decrease recurrence and improve survival [20].
If enlarged nodes are seen on both sides, bilateral CND should be performed [24]. In contrast, if only enlarged ipsilateral nodes are present, the surgeon has the option to perform a unilateral therapeutic node dissection alone, in order to minimize the risk of injury to the contralateral recurrent laryngeal nerve and parathyroid glands [20].
Several studies have shown that bilateral CND may be associated with higher morbidity, primarily RLN injury, and transient hypoparathyroidism, with no reduction in recurrence [12, 20, 25,26,27]. Extent of therapeutic CND should be adjusted based on surgeon judgement, but “berry picking” or removing only the obviously enlarged lymph nodes should be avoided [5, 6, 11, 20]. The number of nodes in the paratracheal regions ranges from 3 to 30 [20]. Nodal yield from a CND has an average of 8 nodes on pathologic exams [12].
Management of Patients with cN0 Disease
For patients with a 1–4 cm low-risk PTC, without evidence of LN metastasis on preoperative and intraoperative evaluation, surgical options include thyroid lobectomy (TL) or total thyroidectomy (TT) with or without pCND. The decision to perform a TL or TT for unilateral PTC must take into account patient and tumor characteristics, risk of loco-regional recurrence, and rate of operative complications. Previous guidelines have recommended TT for all differentiated thyroid cancers >1 cm based on data showing improved survival and decreased recurrence rates [6, 28]. Additional benefits of TT include optimization of the use of serum thyroglobulin for detection of recurrent disease and the use of RAI for imaging and treatment of metastatic disease.
More recent data has demonstrated, that in select patients with unilateral differentiated thyroid cancer <4 cm in size, without ETE, LN metastasis, history of neck radiation exposure or familial thyroid cancer, survival outcomes are similar in patients undergoing TL or TT [29,30,31]. Although some studies have demonstrated a lower risk of locoregional recurrence following TT compared to TL, the overall risk of recurrence after TL in low-risk cN0 PTC is between 1 and 4% [32,33,34]. With proper long-term follow-up, recurrence can be readily detected and treated without impact on overall survival [33,34,35].
Multiple studies comparing TT alone to TT with pCND for cN0 PTC have reported variable rates of recurrence and complications with different conclusions (Table 11.1). The majority of studies are single-institution retrospective cohort studies [4, 9, 13, 36,37,38,39,40,41,42,43,44]. There has been one multicenter retrospective study [45], two prospective RCTs [7, 8] and one prospective non-randomized study [46]. Most studies have not found a significant difference in the overall rate of recurrence and the rate of recurrence in the central neck for patients who underwent TT alone versus patients who underwent TT with pCND.
The first published RCT by Viola et al. included 93 patients randomized to TT with pCND and 88 patients treated with TT alone [7]. The primary endpoints of the study were successful radioiodine ablation with a stimulated thyroglobulin level < 1 ng/ml and recurrence; both were similar in the two groups after 5 years of follow-up. Ninety-nine percent of patients in the study received RAI ablation, however, a higher percentage of the TT group were treated with more than one dose of RAI to achieve successful ablation. Permanent hypoparathyroidism was higher with TT and pCND than with TT alone (19% vs. 8%, p = 0.2). The authors concluded that there was no significant benefit to pCND, with an increased risk of permanent hypoparathyroidism for patients with cN0 PTC.
A recent RCT by Sippel et al. also showed no clear benefit to pCND in patients with cN0 PTC [8]. This trial randomized 30 patients to TT with pCND and 30 patients to TT alone. There was no difference in recurrence and postoperative complication rates were similar between the two groups. However, the duration of follow-up was only 1 year.
A prospective study by Raffaelli et al. evaluated TT alone vs. TT with ipsilateral pCND vs. TT with bilateral pCND in patients with cN0 PTC [46]. A total of 186 patients were assigned to one of the three groups based on surgeon preference and the need to have three equal groups with similar baseline characteristics. With a short follow-up duration of 2 years, there were no significant differences in recurrence between groups, and complication rates were similar except for higher rate of transient hypocalcemia in the patients who underwent TT with bilateral pCND.
Kim et al. retrospectively evaluated the role of pCND in 11,569 cases from a single institution in South Korea [9]. The study included: 1259 patients with TL, 1575 patients with TT, 2107 patients with TL and ipsilateral pCND, 3377 patients with TT and ipsilateral pCND, and 3251 patients with TT and bilateral pCND. The mean tumor size for the thyroidectomy groups vs. pCND groups was 0.8 and 0.9 cm, respectively. There were significant differences in age, T stage, multifocality, ETE, and BRAF positivity between the thyroidectomy groups and the thyroidectomy with pCND groups, which may have affected results. The study showed no benefit to pCND in preventing recurrence and significantly higher rates of temporary RLN palsy and permanent hypoparathyroidism with pCND.
Four of the 16 studies outlined in Table 11.1 found a significantly lower rate of overall recurrence with TT and pCND compared to TT alone, while three studies found a significantly lower rate of central neck recurrence. One of the studies by Barczynski et al. had the longest duration of follow-up of two cohorts that were historically consecutive to each other: a TT group treated between 1993 and 1997 and a TT with pCND group treated between 1998 and 2002 [36]. Overall recurrence and central neck recurrence were significantly lower in the pCND group. The rate of recurrence for the TT group was 13%, higher than the average recurrence rate of 3–5% observed in most other studies. At 10 years, disease-specific survival was higher in the pCND group (98% vs. 92.5%).
A study by Perrino et al. also demonstrated a reduction in recurrence with TT and pCND compared to TT alone [41]. One limitation of this study, however, was that persistent or recurrent disease was defined based on Tg levels. Of those patients who were considered to have persistent or recurrent disease, 72% had an elevated Tg level without evidence of metastatic disease in US [41]. The definition of persistent and recurrent disease varies among the studies detailed in Table 11.1, resulting in varying rates of recurrence.
Popadich et al. performed a multicenter retrospective cohort study with pooled data from 3 Endocrine Surgery units, one each from Australia, the United States, and England [45]. This study showed a significantly lower rate of stimulated Tg level in the pCND group before initial I131 ablation. The total recurrence rate between the group with and without pCND was not significantly different; however, the rate of reoperation in the central neck compartment was lower in the pCND group (1.5% vs. 6%, p = 0.004). The number needed to treat (NNT) with a pCND to prevent 1 recurrence was 20. Effectiveness of pCND was greater for T3 and T4 tumors, with NNT with a pCND to prevent 1 recurrence being 16 and 5, respectively.
The rates of temporary RLN dysfunction were significantly higher with pCND in four studies, while permanent RLN dysfunction was not significantly different in all but one study (Table 11.1) [44]. The rates of temporary hypoparathyroidism were significantly higher with pCND in ten studies, while permanent hypoparathyroidism was significantly higher with pCND in five studies (Table 11.1).
Many of the retrospective studies summarized in Table 11.1 have similar limitations. For the non-randomized studies, the decision for TT vs. TT with pCND was most commonly based on surgeon preference, which created a significant selection bias. In several studies, tumor size, ETE, or the appearance of LNs at operation were used to decide whether or not to perform pCND. The TT group included patients who did not have a preoperative diagnosis of PTC but were found to have PTC on final pathology, another example of selection bias [4]. Both ipsilateral and bilateral pCND were included, however, some studies did not specify the extent of pCND. This resulted in a large variability in the extent of neck dissection, with varying numbers of LNs removed. Although the goal of pCND is to prevent recurrence and need for reoperation in the central neck, many studies did not specify rates of central neck recurrence.
Six meta-analyses have combined data from a variable number of the studies outlined in Table 11.1 [10, 47,48,49,50,51]. Five of them also included studies that only evaluated a pCND cohort without a comparison TT group [47,48,49,50,51]. Four of the 6 meta-analyses found a significantly lower rate of overall locoregional recurrence with pCND compared to the TT alone. Of the three studies that analyzed the rate of central neck recurrence, two meta-analyses noted this to be significantly lower with pCND [47, 49]. Of the three meta-analyses that analyzed complications, two noted significantly higher rates or permanent hypoparathyroidism with TT and pCND compared to TT alone [48, 49].
The five most recent meta-analyses included the study by Barczynski et al. that has an unusually large difference in recurrence rates between the TT with pCND and TT alone, much higher than reported in most other studies (4% vs. 13% for overall recurrence, 1% vs. 8% for central neck recurrence, Table 11.1). The meta-analysis by Lang et al., which included 14 studies, found that the study by Barczynski et al. had a profound impact on the overall incidence rate ratio of locoregional recurrence rate in the two groups. Because the study by Barczynski et al. was close to but within the margin of the funnel plot, it was not excluded from the meta-analysis. This study may have had a significant effect on the final rates of recurrence in several of the meta-analyses outlined in Table 11.2.
A sub-analysis was performed by Liu et al. to evaluate the difference between ipsilateral pCND and bilateral pCND. When comparing TT with ipsilateral CND vs TT alone, there was no difference in recurrence rates; however, TT with bilateral CND had a significantly lower rate of recurrence than TT alone [47]. In the meta-analysis by Chen et al., when the subgroups were compared, there was no difference in local-regional recurrence or complication rates between ipsilateral and bilateral pCND [48].
In several meta-analyses, patients who underwent pCND received higher doses of RAI, which was another confounding factor that may have had a significant impact on recurrence [48,49,50]. Zhao et al. reported a higher rate of recurrence in the lateral neck versus the central neck (3.3% vs. 1.1%) with TT and pCND, whereas the rate of recurrence with TT occurred with equal frequency in the lateral and central neck (3.4% vs. 3.3%) [49]. Wang et al. found no significant difference in recurrence or long-term complications, but a trend toward lower recurrence with TT with pCND, with a NNT of 31 patients to prevent one recurrence [51].
Limitations of meta-analyses that evaluate the role of pCND in the treatment of cN0 PTC are reflective of the quality of the studies included. Most studies were retrospective, with significant selection bias and differences in patient age, tumor size, ETE, and multifocality. In addition, the studies lacked standardized definitions of recurrence. Many studies did not analyze the dosages of RAI used, which may have an effect on recurrence rates. Overall follow-up was <5 years in the majority of studies included in the six meta-analyses, and very few of them reported overall or disease-free survival. The extent of pCND was also different among the studies.
Summary of Evidence-Based Recommendations for Management of Clinically N0 Disease in a Patient with a 3-cm PTC
The current literature comparing TT with pCND to TT alone for cN0 PTC consists of a predominance of retrospective single-institution studies with only modest follow-up duration and as a result, levels of evidence are weak. Despite this, some conclusions and recommendations can be made based on the available data. Rates of temporary and permanent hypoparathyroidism are higher with TT and pCND compared to TT alone, whereas the rate of RLN dysfunction is similar. When pCND is performed, approximately 50% of patients will have occult microscopic LN metastases [4]. This may result in changes in postoperative management with the potential for overtreatment with radioiodine and an unnecessary increase in the intensity of surveillance. However, the impact of pCND on overall recurrence and survival rates is minimal in contrast to macroscopic metastasis [4, 11]. Most studies do not show a significant reduction in overall recurrence or central neck recurrence with pCND (Table 11.1). Studies have shown that the NNT with a pCND to prevent one recurrence ranges from 20 to 31 patients [45, 51]. Thus, one must weigh the increased risk of complications to prevent one recurrence. In experienced hands, central neck reoperation for recurrent disease can be performed with similar rates of complications compared to CND performed during initial operation [52]. In our view, the potential small decrease in recurrence rate compared to the increased rate of complications after pCND does not justify performing routine pCND for low-risk cN0 PTC.
The patient in the clinical scenario at the beginning of the chapter has a 3-cm PTC in the right lobe of the thyroid gland and a 1.3-cm isoechoic nodule in the left lobe. Preoperative ultrasound and intraoperative assessment do not reveal abnormal lymph nodes. The recommended surgical treatment for this patient is a total thyroidectomy without pCND.
References
Zaydfudim V, Feurer ID, Griffin MR, Phay JE. The impact of lymph node involvement on survival in patients with papillary and follicular thyroid carcinoma. Surgery. 2008;144(6):1070–7. discussion 7-8
Lundgren CI, Hall P, Dickman PW, Zedenius J. Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case-control study. Cancer. 2006;106(3):524–31.
Leboulleux S, Rubino C, Baudin E, Caillou B, Hartl DM, Bidart JM, et al. Prognostic factors for persistent or recurrent disease of papillary thyroid carcinoma with neck lymph node metastases and/or tumor extension beyond the thyroid capsule at initial diagnosis. J Clin Endocrinol Metab. 2005;90(10):5723–9.
Hughes DT, Rosen JE, Evans DB, Grubbs E, Wang TS, Solórzano CC. Prophylactic central compartment neck dissection in papillary thyroid cancer and effect on locoregional recurrence. Ann Surg Oncol. 2018;25(9):2526–34.
Patel KN, Yip L, Lubitz CC, Grubbs EG, Miller BS, Shen W, et al. The American Association of Endocrine Surgeons Guidelines for the definitive surgical management of thyroid disease in adults. Ann Surg. 2020;271(3):e21–93.
Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133.
Viola D, Materazzi G, Valerio L, Molinaro E, Agate L, Faviana P, et al. Prophylactic central compartment lymph node dissection in papillary thyroid carcinoma: clinical implications derived from the first prospective randomized controlled single institution study. J Clin Endocrinol Metab. 2015;100(4):1316–24.
Sippel RS, Robbins SE, Poehls JL, Pitt SC, Chen H, Leverson G, et al. A randomized controlled clinical trial: no clear benefit to prophylactic central neck dissection in patients with clinically node negative papillary thyroid cancer. Ann Surg. 2020;272(3):496–503.
Kim SK, Woo JW, Lee JH, Park I, Choe JH, Kim JH, et al. Prophylactic central neck dissection might not be necessary in papillary thyroid carcinoma: analysis of 11,569 cases from a single institution. J Am Coll Surg. 2016;222(5):853–64.
Zetoune T, Keutgen X, Buitrago D, Aldailami H, Shao H, Mazumdar M, et al. Prophylactic central neck dissection and local recurrence in papillary thyroid cancer: a meta-analysis. Ann Surg Oncol. 2010;17(12):3287–93.
Carty SE, Cooper DS, Doherty GM, Duh QY, Kloos RT, Mandel SJ, et al. Consensus statement on the terminology and classification of central neck dissection for thyroid cancer. Thyroid. 2009;19(11):1153–8.
Pereira JA, Jimeno J, Miquel J, Iglesias M, Munné A, Sancho JJ, et al. Nodal yield, morbidity, and recurrence after central neck dissection for papillary thyroid carcinoma. Surgery. 2005;138(6):1095–100. discussion 100-1
Yazıcı D, Çolakoğlu B, Sağlam B, Sezer H, Kapran Y, Aydın Ö, et al. Effect of prophylactic central neck dissection on the surgical outcomes in papillary thyroid cancer: experience in a single center. Eur Arch Otorhinolaryngol. 2020;277(5):1491–7.
Carling T, Carty SE, Ciarleglio MM, Cooper DS, Doherty GM, Kim LT, et al. American Thyroid Association design and feasibility of a prospective randomized controlled trial of prophylactic central lymph node dissection for papillary thyroid carcinoma. Thyroid. 2012;22(3):237–44.
O'Connell K, Yen TW, Quiroz F, Evans DB, Wang TS. The utility of routine preoperative cervical ultrasonography in patients undergoing thyroidectomy for differentiated thyroid cancer. Surgery. 2013;154(4):697–701. discussion -3
Oltmann SC, Schneider DF, Chen H, Sippel RS. All thyroid ultrasound evaluations are not equal: sonographers specialized in thyroid cancer correctly label clinical N0 disease in well differentiated thyroid cancer. Ann Surg Oncol. 2015;22(2):422–8.
Stulak JM, Grant CS, Farley DR, Thompson GB, van Heerden JA, Hay ID, et al. Value of preoperative ultrasonography in the surgical management of initial and reoperative papillary thyroid cancer. Arch Surg. 2006;141(5):489–94. discussion 94-6
Kouvaraki MA, Shapiro SE, Fornage BD, Edeiken-Monro BS, Sherman SI, Vassilopoulou-Sellin R, et al. Role of preoperative ultrasonography in the surgical management of patients with thyroid cancer. Surgery. 2003;134(6):946–54. discussion 54-5
Network NCC. Thyroid Carcinoma (Version 1.2021) 2021. Available from: https://www.nccn.org/professionals/physician_gls/pdf/thyroid.pdf.
Agrawal N, Evasovich MR, Kandil E, Noureldine SI, Felger EA, Tufano RP, et al. Indications and extent of central neck dissection for papillary thyroid cancer: an American Head and Neck Society Consensus Statement. Head Neck. 2017;39(7):1269–79.
Pak K, Suh S, Hong H, Cheon GJ, Hahn SK, Kang KW, et al. Diagnostic values of thyroglobulin measurement in fine-needle aspiration of lymph nodes in patients with thyroid cancer. Endocrine. 2015;49(1):70–7.
Nixon IJ, Shaha AR. Management of regional nodes in thyroid cancer. Oral Oncol. 2013;49(7):671–5.
Leboulleux S, Girard E, Rose M, Travagli JP, Sabbah N, Caillou B, et al. Ultrasound criteria of malignancy for cervical lymph nodes in patients followed up for differentiated thyroid cancer. J Clin Endocrinol Metab. 2007;92(9):3590–4.
Shaha AR. Controversies about the central compartment in thyroid cancer. Editorial regarding the article "Clinical impact of cervical lymph node involvement and central neck dissection in patients with papillary thyroid carcinoma: a retrospective analysis of 368 cases" by Alexandre Bozec et al. Eur Arch Otorhinolaryngol. 2011;268(8):1097–9.
Lee YS, Kim SW, Kim SK, Kang HS, Lee ES, Chung KW. Extent of routine central lymph node dissection with small papillary thyroid carcinoma. World J Surg. 2007;31(10):1954–9.
Roh JL, Park JY, Park CI. Total thyroidectomy plus neck dissection in differentiated papillary thyroid carcinoma patients: pattern of nodal metastasis, morbidity, recurrence, and postoperative levels of serum parathyroid hormone. Ann Surg. 2007;245(4):604–10.
Cavicchi O, Piccin O, Caliceti U, De Cataldis A, Pasquali R, Ceroni AR. Transient hypoparathyroidism following thyroidectomy: a prospective study and multivariate analysis of 604 consecutive patients. Otolaryngol Head Neck Surg. 2007;137(4):654–8.
Cooper DS, Doherty GM, Haugen BR, Hauger BR, Kloos RT, Lee SL, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167–214.
Barney BM, Hitchcock YJ, Sharma P, Shrieve DC, Tward JD. Overall and cause-specific survival for patients undergoing lobectomy, near-total, or total thyroidectomy for differentiated thyroid cancer. Head Neck. 2011;33(5):645–9.
Mendelsohn AH, Elashoff DA, Abemayor E, St John MA. Surgery for papillary thyroid carcinoma: is lobectomy enough? Arch Otolaryngol Head Neck Surg. 2010;136(11):1055–61.
Haigh PI, Urbach DR, Rotstein LE. Extent of thyroidectomy is not a major determinant of survival in low- or high-risk papillary thyroid cancer. Ann Surg Oncol. 2005;12(1):81–9.
Matsuzu K, Sugino K, Masudo K, Nagahama M, Kitagawa W, Shibuya H, et al. Thyroid lobectomy for papillary thyroid cancer: long-term follow-up study of 1,088 cases. World J Surg. 2014;38(1):68–79.
Nixon IJ, Ganly I, Patel SG, Palmer FL, Whitcher MM, Tuttle RM, et al. Thyroid lobectomy for treatment of well differentiated intrathyroid malignancy. Surgery. 2012;151(4):571–9.
Vaisman F, Shaha A, Fish S, Michael TR. Initial therapy with either thyroid lobectomy or total thyroidectomy without radioactive iodine remnant ablation is associated with very low rates of structural disease recurrence in properly selected patients with differentiated thyroid cancer. Clin Endocrinol. 2011;75(1):112–9.
Adam MA, Pura J, Gu L, Dinan MA, Tyler DS, Reed SD, et al. Extent of surgery for papillary thyroid cancer is not associated with survival: an analysis of 61,775 patients. Ann Surg. 2014;260(4):601–5. discussion 5-7
Barczyński M, Konturek A, Stopa M, Nowak W. Prophylactic central neck dissection for papillary thyroid cancer. Br J Surg. 2013;100(3):410–8.
Calò PG, Pisano G, Medas F, Marcialis J, Gordini L, Erdas E, et al. Total thyroidectomy without prophylactic central neck dissection in clinically node-negative papillary thyroid cancer: is it an adequate treatment? World J Surg Oncol. 2014;12:152.
Conzo G, Calò PG, Sinisi AA, De Bellis A, Pasquali D, Iorio S, et al. Impact of prophylactic central compartment neck dissection on locoregional recurrence of differentiated thyroid cancer in clinically node-negative patients: a retrospective study of a large clinical series. Surgery. 2014;155(6):998–1005.
Dobrinja C, Troian M, Cipolat Mis T, Rebez G, Bernardi S, Fabris B, et al. Rationality in prophylactic central neck dissection in clinically node-negative (cN0) papillary thyroid carcinoma: is there anything more to say? A decade experience in a single-center. Int J Surg. 2017;41(Suppl 1):S40–S7.
Lang BH, Wong KP, Wan KY, Lo CY. Impact of routine unilateral central neck dissection on preablative and postablative stimulated thyroglobulin levels after total thyroidectomy in papillary thyroid carcinoma. Ann Surg Oncol. 2012;19(1):60–7.
Perrino M, Vannucchi G, Vicentini L, Cantoni G, Dazzi D, Colombo C, et al. Outcome predictors and impact of central node dissection and radiometabolic treatments in papillary thyroid cancers < or =2 cm. Endocr Relat Cancer. 2009;16(1):201–10.
Sadowski BM, Snyder SK, Lairmore TC. Routine bilateral central lymph node clearance for papillary thyroid cancer. Surgery. 2009;146(4):696–703. discussion -5
Sywak M, Cornford L, Roach P, Stalberg P, Sidhu S, Delbridge L. Routine ipsilateral level VI lymphadenectomy reduces postoperative thyroglobulin levels in papillary thyroid cancer. Surgery. 2006;140(6):1000–5. discussion 5-7
Ywata de Carvalho A, Chulam TC, Kowalski LP. Long-term results of observation vs prophylactic selective level VI neck dissection for papillary thyroid carcinoma at a cancer Center. JAMA Otolaryngol Head Neck Surg. 2015;141(7):599–606.
Popadich A, Levin O, Lee JC, Smooke-Praw S, Ro K, Fazel M, et al. A multicenter cohort study of total thyroidectomy and routine central lymph node dissection for cN0 papillary thyroid cancer. Surgery. 2011;150(6):1048–57.
Raffaelli M, De Crea C, Sessa L, Giustacchini P, Revelli L, Bellantone C, et al. Prospective evaluation of total thyroidectomy versus ipsilateral versus bilateral central neck dissection in patients with clinically node-negative papillary thyroid carcinoma. Surgery. 2012;152(6):957–64.
Liu H, Li Y, Mao Y. Local lymph node recurrence after central neck dissection in papillary thyroid cancers: a meta analysis. Eur Ann Otorhinolaryngol Head Neck Dis. 2019;136(6):481–7.
Chen L, Wu YH, Lee CH, Chen HA, Loh EW, Tam KW. Prophylactic central neck dissection for papillary thyroid carcinoma with clinically uninvolved central neck lymph nodes: a systematic review and meta-analysis. World J Surg. 2018;42(9):2846–57.
Zhao W, You L, Hou X, Chen S, Ren X, Chen G, et al. The effect of prophylactic central neck dissection on locoregional recurrence in papillary thyroid cancer after Total thyroidectomy: a systematic review and meta-analysis : pCND for the locoregional recurrence of papillary thyroid cancer. Ann Surg Oncol. 2017;24(8):2189–98.
Lang BH, Ng SH, Lau LL, Cowling BJ, Wong KP, Wan KY. A systematic review and meta-analysis of prophylactic central neck dissection on short-term locoregional recurrence in papillary thyroid carcinoma after total thyroidectomy. Thyroid. 2013;23(9):1087–98.
Wang TS, Cheung K, Farrokhyar F, Roman SA, Sosa JA. A meta-analysis of the effect of prophylactic central compartment neck dissection on locoregional recurrence rates in patients with papillary thyroid cancer. Ann Surg Oncol. 2013;20(11):3477–83.
Shen WT, Ogawa L, Ruan D, Suh I, Kebebew E, Duh QY, et al. Central neck lymph node dissection for papillary thyroid cancer: comparison of complication and recurrence rates in 295 initial dissections and reoperations. Arch Surg. 2010;145(3):272–5.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Bobanga, I., McHenry, C.R. (2023). Management of Central Neck Nodes in Papillary Thyroid Cancer. In: Roman, S.A., Shen, W.T., Sosa, J.A. (eds) Controversies in Thyroid Nodules and Differentiated Thyroid Cancer. Springer, Cham. https://doi.org/10.1007/978-3-031-37135-6_11
Download citation
DOI: https://doi.org/10.1007/978-3-031-37135-6_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-37134-9
Online ISBN: 978-3-031-37135-6
eBook Packages: MedicineMedicine (R0)