
Abstract
The article concerns the occurrence of body posture defects in children aged 5–6 years. Risk factors for body posture defects are also described here. Recommendations for the prevention of posture defects are given. The consequences of untreated posture defects in children in their adult life were also explained. The study group consisted of 281 children aged 5–6 years. 119 (42.35%) children were 5 years old and 162 (57.65%) were 6 years old. The majority of the study group were boys 144 (51.25%). Assessment of the subjects’ posture was carried out using the viewing method according to the table of postural defects based on modified criteria of Wiktor Dega. The results are as follows no postural defect was found in 186 (66.19%) of the children studied. A slight defect was found in 92 (32.74%) children, and a severe defect was found in 3 (1.07%) subjects. The most common postural defects in the study group were asymmetry and forward tilt of the shoulders in 30 (10.68%) children, flat feet in 16 (5.69%) subjects, lower limb shortening in 11 (3.91%), and scoliosis in 14 (4.98%). Statistical analyses conducted indicate differences between the prevalence of postural defects and gender (p = 0.00), while no such relationship was shown for age (p = 0.30). The majority of girls were characterized by normal posture, while boys were more likely to have postural defects, the differences were statistically significant (p ≤ 0.05). The conducted analyses show that normal posture was present in 186 (66.19%), and postural defects were found in 95 (33.81%) of the children studied. The most common postural defects were asymmetry and anteflexion of the shoulder girdle, scoliosis, flat feet, and lower limb shortening. Postural defects were more common in boys, while normal posture was more common in girls. The age of the children studied did not affect the prevalence of postural defects. Preventive screening of posture in children and adolescents should become a routine procedure of prediction and for assessing a child’s health, at each stage of development in order to act early enough to prevent later defects negatively influencing health status of the child.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The prevalence of postural defects in children and adolescents has been of concern to those concerned with the development of the younger generation for years [1]. Posture is called the way an individual hold themselves in a free-standing position, and the external manifestation of this is the mutual spatial arrangement of the various parts of the body and the silhouette of a person. Posture is similar but not identical in all people—it is an individual trait [2]. Posture according to Kasperczyk’s definition, is the arrangement of individual body parts, not affected by pathological changes, providing optimal stability of the body requiring minimal muscular effort and “creates conditions for optimal positioning of internal organs” [3]. By abnormal posture we mean one in which, due to the occurrence of a defect, deformities have occurred in the formation of the spine, chest, pelvis, lower limbs or feet [4]. The greatest risk of developing abnormal posture is during the period of rapid growth, i.e., between the ages of 5 and 7, and adolescence, i.e., between the ages of 12 and 16 [5]. However, it should be noted that some deviations from normal posture are physiological for a certain age. Until about age 6, lumbar hyperlordosis is present, and the formation of spinal curvatures occurs at age 7. The ontogeny of the development of the lower extremities is distinguished by greater variability. Up to the age of 3 years, the characteristic feature is the scoliosis of the knees. At the age of 4–6 years, physiological valgus of the knees occurs [6]. Schildt showed that the changes that occur in the musculoskeletal system at the age of 5–7 are genetically determined, while external factors (including the influence of physical activity) have a significant impact along with the improvement of the function of the musculoskeletal system [4]. According to Prof. Wiktor Dega, a postural defect is a set of postural errors defined as a small single deviation from normal posture that can be corrected with appropriate passive and active exercises [6].
Data from the Center for Health Information Systems shows that spinal deformities were diagnosed in 17.14% of children and adolescents aged 0–18 and in 9.7% of those aged 2–9. Changes in skeletal elements directly related to the spine (thorax, pelvis) and disorders of the upper and lower extremities account for 45–55% of all postural defects [2, 6].
Factors that contribute to postural defects include: poorly chosen learning positions, inappropriate positions during rest, genetic diseases, bad dietary habits leading to overweight and obesity, overtiredness, vision and hearing defects, and low levels of physical activity [6, 7]. Overweight parameters are as follows: for females, body mass index (BMI) 25–30 and for males, BMI 26–30. Obesity parameters are as follows: class I—BMI 30–35; class II—BMI 35–40; class III—BMI > 40. According to the World Health Organization (WHO), in 2016, 50 million girls and 74 million boys around the globe were registered as being obese [8]. In Germany approx. 1.9 million children and adolescents are overweight, and among these 800,000 are obese. In the USA the number increased from around 5% in the 60 s/70 s to 17% in 2003/04. In Europe approx. Five percent of the children aged 5–17 year are concerned [9]. Pubertal gender dichotomy of girls accumulating fat vs. boys losing fat and growing muscles and height illustrates an obesity-related aspect of gender differential adaptation to scarcity and women’s advantage [10]. Posture can also be affected by age, gender, race, somatic structure of joints, bones and muscles, mental state, including stress, and sports practiced [11, 12]. Nowadays, the increasing prevalence of postural defects seems to be most influenced by low levels of physical activity and the rising rates of overweight and obesity observed in the population of preschool and school-aged children. This is primarily due to a sedentary lifestyle associated with low physical activity and a tendency to spend leisure time in front of the computer or television. Undoubtedly, the occurrence of postural defects is related to the lifestyle. Lifestyle is a term to describe the way individuals, family circles, and societies live and which behavior they manifest in coping with their physical, psychological, social, and economic environments on a day-to-day basis. Lifestyle is expressed by daily work and leisure profiles, including activities, attitudes, interests, opinions, values, and allocation of income. From a psychological point of view lifestyle derives from people’s self-image or self-concept (the way they see themselves and believe they are seen by the others), including self-esteem and self-efficacy [13]. Overall results reported in 2008 by the National Institute of Public Health indicate that physical activity in Poles is too low, and activity in children and adolescents is declining in older age groups [14]. Table 1 illustrates the characteristics of normal posture and faulty posture. Abnormal posture in childhood carries consequences in adulthood, such as reduced cardiorespiratory and lung capacity, pain in the spine and related structures, and displacement of internal organs [15].
Postural defects are any deviation from normal posture. They are fixed changes in the skeletal apparatus that cause various types of dysfunction. Tadeusz Kasperczyk says that postural defects are deviations from the generally accepted characteristics of normal posture, appropriate for a given age group, gender or physique. Postural defects are various types of deformities in the organs of locomotion, such as chest defects, back defects or defects of the lower extremities [7]. The most common posture defects in children and adolescents are as follows:
-
Round back is characterized by excessive backward curvature of the spine. This defect is located in the thoracic region, it is known as hyperkyphosis or deepened thoracic kyphosis. In the round back, the muscles of the back are weakened and stretched: rhomboid, trapezius, neck muscles and extensors of the back, the dysfunction of which causes the torso to tilt forward, spread the shoulder blades, and put the shoulders forward. The muscles that are strained and excessively contracted are: the muscles of the thorax, the serratus and intercostal muscles.
-
Concave back is characterized by a deepening of the lumbar lordosis, an increase in the anterior tilt of the pelvis, a protruding abdomen and a protrusion of the buttocks. In the concave back, the muscles that are excessively stretched and contracted are the straight thigh muscle, the iliac-lumbar muscle, the quadratus lumborum muscle, and the lumbar extensor muscle of the back. Excessively stretched muscles are: gluteal muscles, ischiofemoral muscles, abdominal muscles.
-
Concave-round back is a postural defect in which both round and concave back symptoms are present. The characteristic features of this defect are increased lumbar lordosis and deepened thoracic kyphosis. In a child with a concave back, the head is forward, not projecting onto the sternum, the chest is flattened, the shoulders are protruded, the shoulder blades are outstretched and protruding from the chest, the abdomen is flabby, the buttocks are accentuated.
-
Flat back is a postural defect characterized by a flattening of both physiological curvatures of the spine. The reduction of physiological curvatures reduces the strength of the spine, whose normal shape—with retained curvatures—has 17 times greater strength. Untreated flat back can lead to scoliosis and inversion of the physiological curvatures.
-
Scoliosis, known as lateral curvature of the spine, is a postural defect involving a multiplanar deviation of the spinal line from normal. This deviation occurs in the planes:
-
Frontal—the spine bends to the side, right or left,
-
Sagittal—lordotic and kyphotic bending deepens,
-
Transverse—there is rotation of the vertebrae, which leads to the formation of a hump.
-
-
Funnel chest is characterized by a collapse of the sternum in the region of the xiphoid process. Here the chest is flat and flattened, the abdominal and back muscles are weakened, causing the shoulders to protrude.
-
Pigeon chest is characterized by the fact that the sternum along with the adjacent parts of the ribs protrude significantly forward, while the distal parts of the ribs are collapsed at the sides. This defect is caused by disorders of the ossification processes.
-
Cross-knees, this defect is characterized by an X-shaped medial alignment of the knees. The axis of the lower leg forms an outward open angle with the axis of the thigh. The peripheral segment, which is the shank, is located in abduction. We speak of cross-knees when the distance between the medial ankles exceeds 4–5 cm when the knees are compact and straightened.
-
Bow-legs, are characterized by an inward twisting of the limb. Bow knees are diagnosed when the distance between the knees is greater than 4–5 cm (the legs take the shape of the letter “O”) with the feet together. The most common cause of this defect is rickets caused by vitamin D3 deficiency, overweight children, and adolescents and prolonged sitting in a cross-legged position [7].
In Fig. 1 the relationship between risk factors, assessment of body posture, and the consequences of untreated disorders is shown.

Risk factors, assessment of body posture, and consequences in adulthood
Being aware of the above-mentioned problems and the predictive and preventive potential of the PPPM attitude toward the health of children, the aim of this study was to assess posture in boys and girls aged 5–6 years attending kindergartens in the city of Jawor, Poland as an example of the potential mentioned.
2 Study Group and Research Methods
The tests were conducted as part of the preventive posture testing program implemented by the Jawor District Clinic. The tests were aimed at children aged 5–6 who attend kindergarten in the Jawor municipality. Children from four public kindergartens and one non-public kindergarten were assessed. The study lasted from October 2018 to January 2019. Written consent from a parent or legal guardian was obtained for each child’s participation in the study. Each parent or guardian of a child participating in the study received an examination card describing the child’s posture and recommendations for further management, in case of the presence of a postural defect.
2.1 Study Group
The study group consisted of 281 children aged 5–6 years. 119 (42.35%) children were 5 years old and 162 (57.65%) were 6 years old. The majority of the study group were boys 144 (51.25%). The characteristics of the study group are given in Table 2.
2.2 Study Methods
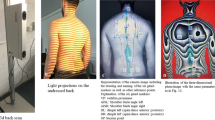
Assessment of the subjects’ posture was carried out using the viewing method according to the table of postural defects based on modified criteria of Wiktor Dega (see Table 3) [16, 17]. In each child, in a lateral position, the following were observed: the position of the head and neck, shoulders and shoulder blades, the formation of the curvatures of the spine—the course of lordosis and kyphosis, the shape of the abdomen and legs. When examining the posture from the front and back, attention was paid to the alignment of the head and neck, shoulders and shoulder blades, the vaulting of the rib cage, the course of the line of the spinous processes of the spine, the triangle of the waist, the anterior superior iliac spines, the knees (crossed, bowed), the structure of the foot (foot: flat, valgus, inflexed). During the examination of the course of the spinal line, the child—standing with his or her back to the examiner—was instructed to perform a loose forward bend of the trunk (feet slightly apart, head and upper limbs loose). The examiner, by running the index and middle finger along the spinous processes of the spine, was able to determine (after the child returned to an upright position) whether the child had a scoliotic posture or not. List of postural defects based on Wiktor Dega’s criteria:
-
Head.
-
Shoulders.
-
Pigeon chest.
-
Funnel chest.
-
Hyperkiphosis.
-
Scoliotic posture.
-
Scoliosis.
-
Hyperlordosis.
-
Pelvis.
-
Abdomen.
-
Flat back.
-
Cross-knee.
-
Bow-legs.
-
Flat foot.
-
Valgus foot.
-
Contractures:
In addition, the children examined were classified into one of the three groups based on the severity of the postural defect. These groups included children without a defect, children with a mild defect that is subject to correction with corrective gymnastics and other physiotherapeutic measures, and subjects with a severe postural defect in whom surgical intervention to correct the defect should be considered.
2.3 Statistical Analysis
The obtained results of the study were subjected to statistical analysis using Statistical version 13.1 software. Normality of distribution of the studied variables was assessed using the Shapiro-Wilk test (p = 0.50), and homogeneity of variance was assessed using the Levene’s test (p = 0.00). The Student’s t-test for independent variables was used to evaluate differences in the incidence of postural defects by age and gender. Spearman’s rank order correlation was used to evaluate the relationship between the incidence of postural defects and age and gender. The p-values were considered statistically significant for p ≤ 0.05.
3 Results
No postural defect was found in 186 (66.19%) of the children studied. A slight defect was found in 92 (32.74%) children, and a severe defect was found in 3 (1.07%) subjects (see Table 3). The most common postural defects in the study group were asymmetry and forward tilt of the shoulders in 30 (10.68%) children, flat feet in 16 (5.69%) subjects, lower limb shortening in 11 (3.91%), and scoliosis in 14 (4.98%). It should be noted that the above-mentioned postural errors were often observed simultaneously in a single child, further increasing the prevalence. Lower limb shortening and shoulder girdle asymmetry co-occurred in 2 (0.71%) subjects, scoliosis and shoulder girdle asymmetry were observed in 13 (4.63%) children, and flat feet and shoulder girdle asymmetry were observed in 4 (1.42%) subjects (see Table 4). Statistical analyses conducted indicate differences between the prevalence of postural defects and gender (p = 0.00), while no such relationship was shown for age (p = 0.30). The majority of girls were characterized by normal posture, while boys were more likely to have postural defects, the differences were statistically significant (p ≤ 0.05).
4 Discussion
4.1 The Occurrence of Postural Defects and Correct Posture in Children
The growing number of postural defects is a significant social problem [18]. However, in the study presented here, the majority of the study population had normal posture. It should be borne in mind that the preschool age is characterized by a large inter-individual variation. This is not only due to the different rates of the development of basic somatic characteristics, but also to the variation in body structure and posture [16]. Similar results were obtained by Wilczyński [14], in whose study there was also a preponderance of children with normal posture, with 71.0% of the subjects, 15.0% of the subjects had concave backs, and 13.0% had flat backs. Also in the study by Drzał-Grabiec et al. [9] children with normal posture predominated, a small percentage of faulty postures (7%) was found, and no poor postures were found. Different results were observed in a pilot study conducted by Janiszewska et al. [4] where the presence of postural defects was found in as many as 93.2% of the children studied. Specific postural abnormalities of the studied population of children occur with similar frequency in both girls and boys. The most common postural abnormalities include: foot defects (78.4%), thoracic and lumbar scoliosis—combined (73.9%) and malaligned shoulder blades (59.5%).
4.2 Type and Frequency of Posture Defects
In the present study, the most common postural defects were asymmetry and anteflexion of the shoulder girdle, scoliosis, flat feet, and lower limb shortness. A similar study was conducted by Andrzejewska and Grabarczyk [19], whose goal was to demonstrate postural abnormalities in children from Wroclaw.
The authors obtained the following results: Among the analyzed postural abnormalities of children, trace scoliosis occurred in boys in an average of 36%, typical scoliosis in 3% at the age of 7–15 years. In girls, trace scoliosis and typical scoliosis were revealed in a similar percentage as in boys—37% and 3%, respectively. Shoulder asymmetry was the most common of all the postural defects analyzed, averaging 55% in boys, with more than 70% in subjects aged 8 and 15. In girls, the asymmetry averaged 56%, with the highest number of subjects with shoulder asymmetry (about 70%) registered among 7- and 14-year-old children. Among abnormalities in knee alignment, cross-knees were observed primarily among both boys and girls. In the evaluation of foot arches, flattening of the feet was found to be the most common defect. More than 35% of boys aged 9 and 11 and girls aged 8 and 10 had this defect. Flat feet were found less frequently, with the exception of 7-year-old boys (40%). There were also defects in the arches of only one of the feet. In a study by Macialczyk-Paprocki et al. [16] the most common abnormalities in the table of errors according to W. Dega concerned the foot (48.2%) and shoulders (37.2%).
The most common abnormalities were flat feet and plano valgus, as well as shoulder malalignment, which occurred significantly more often in boys, compared to girls. Cross-knees were more common in boys than in girls; the differences were not statistically significant. Bow-knees were observed in only about 3% of boys; this defect did not occur in girls. Scoliotic posture was detected in 24.7% of boys and in 20.8% of girls.
4.3 Relationship Between Posture Defects and Overweight and Obesity
The purpose of the study by Wilczynski et al. [20] was to evaluate the relationship between the anteroposterior shape of spinal curvatures and body composition in school-aged children. The study included 257 children aged 11–12 years. Normal spinal curvatures were present in 106 (41.08%) subjects. The other types of abnormalities were: decreased kyphosis and normal lordosis—40 subjects (15.50%), normal kyphosis and decreased lordosis—24 subjects (9.30%), increased kyphosis and normal lordosis, 17 subjects (6.59%), normal kyphosis and increased lordosis, 22 people (8.53%), decreased kyphosis and decreased lordosis, 32 patients (12.40%), decreased kyphosis and increased lordosis, 4 people (1.55%), increased kyphosis and increased lordosis, 13 participants (5.04%).
Another study by Maciałczyk-Paprocki et al. in 2017 [21] assessed the epidemiological prevalence of abnormal posture in overweight and obese children and adolescents residing in Poznań (Poland). The study population consisted of a representative group of children and adolescents aged 3–18 years randomly selected from dozens of kindergartens (3–6 years), elementary schools (7–12 years), and middle and high schools (13–18) in Poznań. The duration of the study was 2 years. In the entire study population (2732 subjects), postural defects were found in 67.9% of the subjects (918 boys and 938 girls). In obese children, the prevalence of postural defects was significantly higher than among normal-weight children (p = 0.001) and overweight children (p = 0.0046). Among girls and boys with excessive body weight (overweight and obese), the percentage of postural defects was highest in the group of children 7–12 years old. Despite the fact that girls with excessive body weight aged 7–12 as well as 13–18 had a higher number of postural defects than boys, the difference was not statistically significant (p > 0.05). The prevalence of abnormal posture in all obese boys was found to be 1.5 times higher than among normal-weight boys, but the difference was not statistically significant. In obese girls, the prevalence rate of postural abnormalities was twice that of the normal-weight group, and this difference was found to be significant (p = 0.004). In children aged 3–6 years, obesity and overweight do not increase the likelihood of postural defects In the group of students aged 7–12 years, the likelihood of postural defects was significantly higher in obese than in normal-weight students, both in boys (p = 0.042) and in girls (p = 0.007). Only overweight boys aged 13–18 had a significantly lower number of foot defects than their normal-weight peers (p = 0.021).
4.4 Foot Defects in Children
Foot defects are a common phenomenon especially in children and are a serious medical and social problem. Feet, more than other parts of the musculoskeletal system, are exposed to adverse effects of the external environment. The most important moment of foot formation is the preschool period [22]. In the present study, flat feet were present in 16 (5.69%) of the children studied, but more often in boys, i.e., in 11 cases (3.91%). The study conducted by Klimczak et al. [18] shows that among the children studied, 48% had normal feet, 25% had flat feet, and 28% had hollow feet in relation to the plantocontourogram with patterned foot types. Rykała et al. [23] observed that in loading the feet with their own body weight, as the children grew older they were characterized by worse transverse arches, while better longitudinal arches of the feet. In a study by Skowron et al. [24], 30% of children had a properly arched foot, 30% had a flattened foot, and 40% had a flat foot.
It should be emphasized that in recent years most studies on the assessment of body posture in children have been conducted by senders from Poland. This situation is evident in the research results cited above.
5 Conclusion and Recommendations
On the basis of our study we conclude and recommend for the practical application of PPPM principles the following:
-
1.
Normal posture was present in 186 (66.19%), and postural defects were found in 95 (33.81%) of the children studied.
-
2.
The most common postural defects were asymmetry and anteflexion of the shoulder girdle, scoliosis, flat feet, and lower limb shortening.
-
3.
Postural defects were more common in boys, while normal posture was more common in girls.
-
4.
The age of the children studied did not affect the prevalence of postural defects.
-
5.
Preventive screening of posture in children and adolescents should become a routine procedure for assessing a child’s health, at each stage of development, which will help to avoid serious health consequences in the future.
-
6.
The use of visual assessment of children’s posture is a simple and effective method of capturing postural abnormalities and referring the child for further diagnosis and treatment.
-
7.
The criteria for correct posture cannot be constant and unambiguous for everyone; on the contrary, they should undergo changes depending on the child’s developmental period. In this assessment, factors such as constitutional type, sports disciplines, and forms of recreation cannot be ignored.
Abbreviations
- BMI:
-
Body Mass Index
- N:
-
Number of children tested
- p:
-
P value
- PPPM:
-
Predictive, preventive, and personalized medicine
- WHO:
-
World Health Organization
References
Pokrywka J, Fugiel J, Posłuszny P (2011) Prevelance of postural disorders in children from copper basin in Poland. Fizjoterapia 19(4):3–10. https://doi.org/10.2478/v10109-011-0025-3
Górecki A, Kiwerski J, Kowalski IM, Marczyński W, Nowotny J, Rybicka M et al (2099) Profilaktyka wad postawy u dzieci i młodzieży w środowisku nauczania i wychowania—rekomendacje ekspertów. Pol Ann Med 16(1):168–177
Zmyślna A, Żurawski AŁ, Śliwiński G, Śliwiński ZW, Kiebzak WP (2021) Assessment of body posture of children with chest pain. Front Pediatr 9:704087. https://doi.org/10.3389/fped.2021.704087
Janiszewska R, Tuzinek S, Nowak S, Ratyńska A, Biniaszewski T (2009) Nieprawidłowości postawy ciała u dzieci 6-12 letnich—uczniów szkół podstawowych z Radomia—badania pilotażowe. Problemy Higieny i Epidemiologii 90(3):342–346
Ziętek M, Machniak M, Wójtowicz D, Chwałczyńska A (2022) The incidence of body posture abnormalities in relation to the segmental body composition in early school-aged children. Int J Environ Res Public Health 19(17):10815
Wawrzyniak A, Tomaszewski M, Mews J, Jung A, Kalicki B (2017) Wady postawy u dzieci i młodzieży jako jeden z głównych problemów w rozwoju psychosomatycznym. Pediatria i Medycyna Rodzinna 13(1):72–78. https://doi.org/10.15557/PiMR.2017.0007
Rosa K, Muszkieta R, Zukow W, Napierała M, Cieślicka M (2013) The incidence of defects posture in children from classes I to III elementary school. J Health Sci 3(12):107–136
Golubnitschaja O, Liskova A, Koklesova L, Samec M, Biringer K, Dietrich Büsselberg D et al (2021) Caution, “normal” BMI: health risks associated with potentially masked individual underweight—EPMA position paper 2021. EPMA J 12:243–264. https://doi.org/10.1007/s13167-021-00251-4
Graf C (2011) Preventing and treating obesity in pediatrics through physical activity. EPMA J 2:261–270. https://doi.org/10.1007/s13167-011-0091-0
Shapira N (2013) Women’s higher health risks in the obesogenic environment: a gender nutrition approach to metabolic dimorphism with predictive, preventive, and personalised medicine. EPMA J 4:1; http://www.epmajournal.com/content/4/1/1
Wyszyńska J, Podgórska-Bednarz J, Drzał-Grabiec J, Rachwał M, Baran J, Czenczek-Lewandowska E et al (2016) Analysis of relationship between the body mass composition and physical activity with body posture in children. Biomed Res Int 2016:1. https://doi.org/10.1155/2016/1851670
Drzał-Grabiec J, Snela S (2012) The infuence of rural environment on body posture. Ann Agric Environ Med 19(4):846–850
Trovato GM (2012) Behavior, nutrition and lifestyle in a comprehensive health and disease paradigm: skills and knowledge for a predictive, preventive and personalized medicine. EPMA J 3:8; http://www.epmajournal.com/content/3/1/8
Permoda-Białozorczyk A, Olszewska-Karaban M, Permoda A, Zajt J, Wiecheć M, Żurawski A (2022) Evaluation of the functional status of the posture control system in children with detected disorders in body posture. Int J Environ Res Public Health 19(21):14529. https://doi.org/10.3390/ijerph192114529
Rusek W, Baran J, Leszczak J, Adamczyk M, Baran R, Weres A et al (2021) Changes in children’s body composition and posture during puberty growth. Child 8(4):288. https://doi.org/10.3390/children8040288
Maciałczyk-Paprocka K, Krzyżaniak A, Kotwicki T, Kałużny Ł, Przybylski J (2011) Postawa ciała dzieci w wieku przedszkolnym. Problemy Higieny i Epidemiologii 92(2):286–290
Maciałczyk-Paprocka K, Krzyżaniak A, Kotwicki T, Sowińska A, Stawińska-Witoszyńska B, Krzywińska-Wiewiorowska M et al (2012) Występowanie błędów w postawie ciała u uczniów poznańskich szkół podstawowych. Problemy Higieny i Epidemiologii 93(2):309–314
Wilczyński J (2006) Najczęściej występujące wady postawy u chłopców w wieku 13–16 lat badanych komputerową metodą Moiré. Med Pr 57(4):347–352
Andrzejewska J, Grabarczyk M (2005) Charakterystyka postawy ciała dzieci wrocławskich. Słupskie Prace Biologiczne 1:7–10
Wilczyński J, Lipińska-Stańczak M, Wilczyński I (2020) Body posture defects and body composition in school-age children. Child 7(11):204. https://doi.org/10.3390/children7110204
Maciałczyk-Paprocka K, Stawińska-Witoszyńska B, Kotwicki T, Sowińska A, Krzyżaniak A, Walkowiak J et al (2017) Prevalence of incorrect body posture in children and adolescents with overweight and obesity. Eur J Pediatr 176(5):563–572. https://doi.org/10.1007/s00431-017-2873-4
Klimczak K, Kochański B, Kałużny K, Plaskiewicz A, Smuczyński W, Ratuszek-Sadowska D et al (2014) Analiza występowania wad stóp u dzieci w wieku 6-10 lat. J Health Sci 4(2):29–38
Rykała J, Snela S, Drzał-Grabiec J, Podgórska J, Nowicka J, Kosiba W (2013) Ocena wysklepienia podłużnego i poprzecznego stóp w warunkach odciążenia i obciążenia masą własną u dzieci w wieku 7–10 lat. Przegląd Medyczny Uniwersytetu Rzeszowskiego i Narodowego Instytutu Leków w Warszawie 2:183–193
Skowron N, Malak R, Mojs E, Samborski W (2015) Foot arch condition in comparison with the muscular balance of lower limbs in children at school age of 6–14 years. J Med Sci 2(84):85–89. https://doi.org/10.20883/medical.e21
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Cieślik, B. (2023). Prevention and Prediction of Body Posture Defects in Children Aged 5–6 Years. In: Podbielska, H., Kapalla, M. (eds) Predictive, Preventive, and Personalised Medicine: From Bench to Bedside. Advances in Predictive, Preventive and Personalised Medicine, vol 17. Springer, Cham. https://doi.org/10.1007/978-3-031-34884-6_6
Download citation
DOI: https://doi.org/10.1007/978-3-031-34884-6_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-34883-9
Online ISBN: 978-3-031-34884-6
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)