
Abstract
The world has capitalized on the unique potential of nurses for centuries. This chapter focuses on the regulation of advanced nursing practice in support of the Future of Nursing 2020–2030 Recommendation 4 (The Future of Nursing 2020–2030: Charting a Path to Achieve Health Equity. The National Academies Press, 2021). Although advanced practice registered nurses (APRNs) vary from country to country, the approaches to achieving health equity with restrictive practice policies are similar. The implementation of APRN practice to increase access to care in two states is evaluated. Japan, a country with emerging APN roles to address its growing aging population, is also discussed.
Future of Nursing 2020–2030: Recommendation 4
All organizations, including state and federal entities and employing organizations, should enable nurses to practice to the full extent of their education and training by removing barriers that prevent them from more fully addressing social needs and social determinants of health and improving health care access, quality, and value. These barriers include regulatory and public and private payment limitations; restrictive policies and practices; and other legal, professional, and commercial impediments.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Access to care
- Health equity
- Advanced practice registered nurse
- Full practice authority
- Policy
- Pandemic
- Global
1 Introduction and Overview
People’s direct access to advanced practice registered nurses (APRNs) has been an evolutionary process, with rapid growth in the last decade. APRN practice in the United States started in the nineteenth century with nurses providing anesthesia services during the Civil War. By the end of the nineteenth century and into the early twentieth century, nursing midwifery grew out of the historical midwifery practice [1, 2]. As nursing midwifery grew into a profession, so did clinical nurse specialists, who started as psychiatric nurses [3, 4]. The nurse practitioner field also had its early roots in the early twentieth century and was firmly established in the 1960s [5]. Subsequently, state regulations governing their profession developed as each advanced nursing specialty gained traction.
The National Academy of Medicine (NAM), in its 2021 Future of Nursing 2020–2030: Charting a Path to Health Equity, called for the federal government, state governments, health systems, and insurers to recognize nurses’ full potential [6]. The NAM reiterated and expanded upon the initial 2010 Future of Nursing report’s recommendation for state and federal governments to modernize their laws pertaining to nursing practice [7]. The 2021 report emphasized the need for nurses and other stakeholders to focus on health equity, diversity of nursing, social determinants of health (SDOH), and laws and institutional policies pertaining to APRNs’ and registered nurses’ scope of practice.
Before exploring the scope of practice-related public and institutional policies, here is a brief explanation of the four APRN roles. As noted earlier, all four APRNs have important roles in providing high-quality clinical care to patients and support for families (see Table 1).
2 Primary Care and Nurse Practitioners: A Decade of Change
In 2007, AARP Foundation, AARP, and the Robert Wood Johnson Foundation created a joint initiative, the Center to Champion Nursing in America (CCNA) [9]. Its mission is to ensure that all Americans have access to highly skilled nurses when and where we need them. CCNA, working closely with AARP government affairs and policy staff and leaders, decided to support and advocate for APRNs’ full practice authority. Full practice authority (FPA) is defined as “the authorization of nurse practitioners (NPs) to evaluate patients, diagnose, order and interpret diagnostic tests, and initiate and manage treatments—including prescribing medications—under the exclusive licensure authority of the state board of nursing” [10]. By doing so, these policies would increase patients’ access to care and support for family caregivers. AARP tracks this public policy win annually in its dashboard measure. Henceforth, AARP and CCNA worked on this policy through the lens of the consumer and eventually helped frame this issue from other perspectives, including free enterprise and most recently health equity.
In 2010, AARP Foundation, AARP, and the Robert Wood Johnson Foundation announced a second joint initiative, Future of Nursing: Campaign for Action. Administered through CCNA, the Campaign was responsible for building a national movement to implement the 2010 Institute of Medicine (IOM), now known as the National Academy of Medicine, Future of Nursing recommendations. As noted earlier, the IOM included FPA for APRNs, and therefore, the Campaign would prioritize this recommendation. Through the Campaign, CCNA provided technical assistance to AARP state offices and nursing coalitions to advocate for FPA. CCNA helps with coalition building and messaging training to help broaden the network of supporters—both grassroots and policymakers.
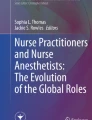
This strategy reflects Kingdon’s (1984) policy stream model [11]. Kingdon’s model starts with the problem stream and underscores the importance of framing the problem. His model then moves into the policy stream, which demonstrates that multiple stakeholders often share an interest in an issue from various perspectives. The model wraps up with the political stream, which is when the decision-makers agree with the problem and policy streams and make a change. Kingdon underscored that stakeholders do not achieve these political wins randomly [12]. Instead, it takes entities and coalitions many attempts at the problem, policy, and political streams, before succeeding. For CCNA, by building the consumer strategy (framing the problem) and helping nursing broaden its reach (policy stream), the Campaign and CCNA have helped nurse practitioners (politics stream) in 14 states achieve FPA since 2011 [10,11,13]. Figure 1 illustrates the progress of the states with access to care. Later are two examples of states that have made advancements as well as a case study that describes the potential for institutional-level advancements.

State progress in improving access to care
3 Case Studies
Case Study A: West Virginia and the Business Case
In 2016, West Virginia achieved an important win. Although it fell just short of recognizing NPs’ FPA, it is close. The state still requires NPs to have a written protocol with a physician to prescribe some controlled substances [14]. The reason it is important to highlight West Virginia relates to their coalition and their messaging.
In the early part of the decade, a prominent change among state legislatures occurred. A majority became conservative, favoring smaller government, less bureaucracy, and consumer choice. In 2015, Nebraska achieved FPA, and a new prominent conservative grassroots organization, Americans for Prosperity, supported it.
Then, in West Virginia in 2016, this issue made headway in the state legislature when the Senate appointed a new Health Committee Chair. The prior one, a physician, held the seat for numerous years and suppressed the scope of practice bill for a vote. With the new Chair, numerous stakeholders, including AARP WV, saw this change in leadership as an opportunity to advance the legislation. Recognizing Americans for Prosperity’s role in Nebraska the year before, AARP invited the conservative organization’s WV chapter to work with each other and with the nursing organizations on NPs’ FPA.
The messaging that the coalition used emphasized removing red tape from health care, consumer choice, and a rural economic case. The coalition argued that NPs would likely open small businesses in rural areas and would hire local people as registered nurses, administrative employees, and medical technicians. These small businesses would help improve the health and well-being, as well as the financial security, of the communities they served.
The law was passed in 2016. In 2018, The Future of Nursing of West Virginia, a nonprofit nursing organization, secured a Campaign for Action $25,000 Nursing Innovations Fund. They raised matching funds from the Greater Kanawha Valley Foundation. Their goal was to teach NPs how to open and run small health-related businesses. The Future of Nursing of West Virginia leveraged this funding to apply for federal funds. In 2021, the Appalachian Regional Commission, which supports sustainable community and economic development, awarded the coalition $630,000 to establish the West Virginia Center for Nurse Entrepreneurship. The coalition has, so far, raised $1.3 million after the original $25,000 from the 2018 Nursing Innovations Fund. Their project partners include the West Virginia Small Business Development Center and the West Virginia Chamber of Commerce. The U.S. Economic Development Administration and the Claude Worthington Benedum Foundation also provided funding [15].
Four years following West Virginia’s passage of its law, a global pandemic, in the form of COVID-19, created a public health emergency. To improve people’s access to care, several states granted waivers for APRNs’ temporary FPA.
Seven states administered these waivers in 2020. Kansas, Louisiana, Massachusetts, New Jersey, New York, Virginia, and Wisconsin [16]. Of the seven, three states passed laws recognizing APRNs’ FPA. They are Kansas (2022), Massachusetts (2020), and New York (2022). Louisiana, Tennessee, and Wisconsin all let their emergency laws expire. New Jersey retired most of its COVID-19 pandemic emergency laws, but the governor, as of this writing (August 2022), has maintained some executive orders—including APRNs’ temporary FPA.
Case Study B: Kansas Makes Permanent Their Temporary Law
The following is a summary of a presentation that Kansas coalition leaders, Michelle Knowles and Amy Siple, provided during AARP’s Access to Care Learning Collaborative, on May 2, 2022. Ms. Siple is the president of the Kansas Association of Nurse Practitioners. Ms. Knowles is a member of the Kansas Advanced Practice Nurse Strategy Team.
Kansas achieved FPA in April 2022, making them the 26th state to fully modernize its APRN laws. The Kansas law recognized the FPA of nurse practitioners, clinical nurse specialists, and certified nurse midwives. The fourth APRN group, certified registered nurse anesthesiologists, had prior recognition from Kansas policymakers. Kansas’s statute also allows APRNs, who have their respective and legal degrees, licenses, and certifications, to immediately practice without unnecessary contracts with physicians.
The Kansas coalition leaders underscored several important tactics they incorporated into their overall strategy. They are:
-
1.
Changing the debate from doctors vs. nurses turf battle to one about access to care was key as was building a broad coalition including AARP, Chamber of Commerce, and Americans for Prosperity.
-
2.
Building trust with legislators, as one APRN group, was the first step to strategizing for FPA. The broad coalition also kept patients as the focus.
-
3.
Nurse leaders familiarized themselves with the “gatekeepers” and how they functioned by studying the hearing processes. Gatekeeper was a term used interchangeably to describe Kansas’ stakeholders and key politicians.
The two leaders also shared the following lessons.
-
(a)
Focus on the patient. The current governor has physicians in her family, so there was concern she would veto the bill. However, the governor understood the needs of Kansans (the patients) and signed the bill.
-
(b)
Learn the key decision-makers. The Speaker of the House assigns who the Chair will be for the health and human committees.
-
(c)
Use smaller and simpler bills. Past bills that were presented to the legislators were complex.
-
(d)
Study opposing stakeholders and figure out what they are doing and where their interests lie.
Regulations Promulgation. Within 2 months of the governor signing the law, the Kansas Board of Nursing started drafting regulations. Organizations that opposed the legislation challenged the draft regulations. In July 2022, the Board of Nursing’s regulations was temporarily implemented for 120 days, and in September, they permanently implemented regulations reflecting the intent of the legislation. Now, all APRNs in Kansas have full practice authority.
Future goal(s): After finalizing the regulatory negotiations in 2022, the Kansas coalition leaders hope to work on legislation in the next year or so to work on global signature authority. This would ensure that APRNs can sign forms such as death certificates and license plate applications for people with disabilities. This type of law is very important for family caregivers. If families are unable to obtain signatures from qualified clinicians on death certificates, they could be forced to wait to have funeral services for their departed loved ones. The next step they will seek is updating the state’s global signature authority law [17].
Case Study C: Health Equity—Midwest-Based Nurse Practitioner Serving a Homeless Shelter
In a call for stories, a nurse practitioner in a Midwestern state described in an email how the law amplifies barriers to care for people who are homeless and other vulnerable populations [18]. The state’s law requires APRNs to contract with physicians to provide clinical care—including APRNs who volunteer at homeless shelters.
If we look at this issue from the perspective of those who experience homelessness, we can look at their experience from a more holistic perspective. Their care is almost always delayed for multiple reasons.
-
The primary issue is people who are homeless rarely have health insurance, and it is almost impossible to find a clinician to care for them.
-
The person’s care is potentially more at risk when a volunteer NP’s contracted physician stops practicing. The NP then needs to seek out another one to contract with. This could take a long time—and in her case, it took 6 months—which delays the care the vulnerable population receives.
-
Then, if the person needs to see a specialist, such as an oncologist, the volunteer NP needs to help the person find a physician or medical team who would care for someone without coverage or the ability to provide co-payments.
-
Another barrier to care this population often experiences is the lack of available affordable transportation.
-
The person lacks access to consistent healthy daily meals and experiences food insecurity, which could lead to malnutrition, which causes poor healing.
-
Of course, underlying all of this is the person’s unstable housing situation magnifies all other barriers to their care and well-being.
Such barriers that vulnerable people, like those who are homeless, experience will discourage them from following through on care. This further diminishes their quality of life—and results in putting an enormous strain on the health care system once they finally access a medical team. Because of a lack of transportation, unstably housed people may not be able to make it to appointments, such as chemotherapy for breast cancer. Their health issues are exacerbated, which leads to hospitalizations for their primary needs until they are stabilized. Keeping in mind that this person is likely uninsured, the system (the state and taxpayers) then absorbs the costs of all care for this person.
Now, assume this person is stabilized and starts to receive the chemotherapy she needs. She continues to access specialty services and the volunteer NP regularly tracks her needs to ensure that the person receives her care as needed. But, what happens if the volunteer NP’s physician no longer practices and their contract ends? As this was the case with the NP in the Midwestern state? The NP cannot attend to any of the people in the shelter, including the woman with breast cancer. It took the NP 6 months before she secured another contract with a physician. Luckily, over those 6 months, the health system that was treating the woman with breast cancer was able to find her nearby stable housing.
Clinical bias is another barrier that many patients, including the unstably housed, experience. In other words, clinicians who are motivated by biases and assumptions often treat assuming such patients are not compliant or will follow through with care. In turn, unstably housed patients mistrust clinicians. It is important for clinicians to understand the social determinants of health impacting vulnerable individuals and treat them through that lens, rather than their own assumptions. That would help achieve health equity.
Case Study D: Institutional Policy and Maximizing APRN and RN Care at Mt Sinai Cancer Center
The senior director of nursing for oncology and clinical quality at Mount Sinai’s Cancer Center in New York City, Toby Bressler, RN, PhD, FAAN, had identified potential efficiencies for improved care in her department over a multiyear period. These efficiencies involved optimizing the skills of both APRNs and RNs. When the COVID-19 pandemic hit New York City in 2020, Dr. Bressler, like all healthcare delivery leaders, recognized that all healthcare workers needed to be deployed in new and different ways than their current systems allowed. If the department’s entire workforce was fully deployed to provide the level of care they were each prepared for, all of their patients would receive better and more equitable care. The clinical team would be able to provide patient-centered care—in other words, the patients would be equitably served. She worked with Mt. Sinai’s leadership and implemented a new set of processes. Rather than the APRNs reporting to physicians, they reported to the nursing director—her. And the RNs reported to the APRNs. In other words, Mt. Sinai Cancer Center implemented a nursing system based entirely on nursing leadership.
All people associated with this new system have reported high satisfaction. The physicians are grateful to focus on patient care and research, and no longer being encumbered by managerial duties. The APRNs and RNs are happy that the care system has less bureaucracy and are especially happy about how patient care has improved. The patients who transition from cancer treatment to post-treatment care are now able to see an advanced clinician within 1 week of discharge—rather than needing to wait months before seeing a physician [19].
4 Capitalizing the Potential of APNs Globally: An Emerging Change
This section discusses the emerging role of international advanced practice registered nurses (APRNs) and explores the standardization of practice to improve global health outcomes. While most states use the term “advanced practice registered nurse” or “APRN,” the International Council of Nursing (ICN) uses the term “advanced practice nurse” or “APN.” Over the past half-century, numerous countries have introduced APNs to increase access to care and reduce poor health outcomes in individuals and families [14, 20, 21]. In addition, APNs demonstrated their potential in securing global health during the COVID-19 pandemic by delivering high-quality care in remote and underserved communities [21, 22]. The world began to understand the social determinants of health (SDOH), its variation in countries, and its role in health outcomes. Systemic barriers that prevented APNs’ from addressing SDOH were also brought to light, and global conversations to achieve health equity were initiated.
The implementation of APNs across the globe relies on the support of ICN. It is the first international healthcare organization and has led nursing practice since 1899. ICN’s priorities include focusing on the central role of nurses in primary care and advocacy for global health through policy [22, 23]. ICN also shares an interest with the World Health Organization (WHO) and the American Association of Nurse Practitioners (AANP) in supporting the development of the nursing workforce to improve world health.
In 2020, ICN released its first Guidelines on Advanced Nursing Practice as a resource for countries to address barriers to APN practice. CNSs and NPs were identified as the most common APNs in developing countries and the only APNs highlighted in the guidelines [4, 24]. There are over ten countries with CNSs who serve as clinical leaders to improve healthcare systems. Many countries with CNSs still face challenges with recognition, regulation, and licensure [3, 25]. For example, CNSs in the United Kingdom face barriers to title protection, educational requirements, and safe patient workload [24, 26].
ICN’s Nurse Practitioner and Advanced Practice Network (NP/APN) was established for ANPs to share best practices that could produce optimal outcomes and educate other interest groups to support their role [20, 25]. NPs can bridge health and social determinants by promoting health practices that prevent the international spread of infections in communities. Although the NP role is defined in many countries, there is a growing need for them to assist with the shortage of providers in Africa and South Asia. In 2011, Nigeria attempted to integrate NPs into its healthcare system but was unable to progress due to the lack of funding and policy [27].
The nurse anesthetist’s education, title, and responsibilities vary from country to country. The International Federation of Nurse Anesthetists (IFNA) leads the world in nurse anesthesia [28]. There are 40 countries with nurse anesthetists with differences in education, training, and anesthesia-related tasks and responsibilities [29].
The International Confederation of Midwives (ICM) oversees education, licensure, regulation, and practice for midwives throughout 119 countries. However, there are variations of certified midwives who improve maternal and infant outcomes. According to the State of the World’s Midwifery Report, midwives could prevent 2 million neonatal deaths and save the global economy 4.3 million dollars per year by 2035. Norway and Iceland have the greatest maternal-infant outcomes with midwives per 1000 births. Africa and South Asia also have the least number of midwives contributing to their high infant and maternal mortality [30].
The future of improved global health outcomes entails the integration of APNs in health care systems. Health outcomes have greatly improved in countries where APNs have been successfully utilized and have greater practice authority [31, 32]. Improving health equity across the globe would take standardization in practice, advocacy, research, and leadership [33]. Nations could consider studying the efficacy of utilizing APNs to achieve health equity. The areas of study would include what Rosa et al. recommend, the standardization of practice, and the potential for APNs in leadership roles [34]. An important leadership role for APNs is having policy knowledge and expertise and how to advocate. Another important leadership role is for APNs to develop research skills and to create a body of evidence demonstrating their efficacy to achieve health equity. To help explain the deployment of APNs globally, later is a case study.
Case Study E: Japanese Model for Aging Societies
The need for APNs in Japan coincides with the growth of the aging population and the shortage of physicians [20, 35, 36]. The three APN groups that practice in Japan are midwives, clinical nurse specialists, and nurse practitioners (see Table 2). The first Japanese APN group was midwives and was established in 1948 to provide perinatal care to women and newborns [29]. Although the term “certified nurse midwives” is commonly used in the U.S., “midwife” is the preferred term in Japan to describe the traditional role of service to the community [36]. In 2006, the Japanese government revised its law to lift some barriers that prevent midwives from practicing to their full extent of education and training. There are over 40,000 midwives who practice in clinics, hospitals, or midwifery homes. Today, there are fewer employment opportunities for midwives because of Japan’s low birth rates.
CNSs were established in 1996 [27]. CNS’ roles in Japan seem to be similar to their original intent in the U.S. As described by Kondo [37], CNSs provide high-quality nursing care for complex cases that requires consultation, coordination, and research. They serve as a liaison between the nurse and physicians. This is an important role when they look holistically at the care being provided to patients.
NPs are the newest APNs that Japan introduced into its health care system in 2015. The nation now has more than 450 certified NPs [35, 38, 39]. The Japanese NP (JNP) model is similar to that in the U.S. In 2005, 12 Japanese faculty members observed the NP education system in the United States. The first post-graduate NP program was established at Oita University of Nursing and Health Sciences (OUNHS) in 2008. In 2010, 17 students graduated from the first NP program at OUNHS. Today Japan has 11 nurse practitioner programs [40].
In Japan, multiple professional nursing and governmental organizations regulate APNs. The Japanese Association of Nursing Programs in Universities (JANPU) accredits CNS programs. JANPU also adopted the American NP practice competencies for all their APNs [37]. The Japan Nursing Association is the professional organization that is responsible for the certification of JNPs [39]. The Ministry of Health, Labor, and Welfare is responsible for the certification and regulation of midwives and public health nurses [28, 32].
In Japan, APNs have what the U.S. described as a restricted practice environment. JNPs are required to be supervised by physicians and have a protocol on file to provide patient care [27, 39]. Current regulations prevent APNs from expanding their scope of practice to meet other provider shortages such as anesthesia. In the interim, Japan continues to educate and train nurses to provide anesthesia care until the nurse anesthesia role is developed and introduced [20]. The implementation of APNs in Japan was created as a model to ensure care for their aging society. Over time it would be important to learn how Japan accomplishes that goal and encourages other nations to adopt its model.
5 Conclusion and Next Steps
In the United States, to ensure that all people have access to care when and where they need it, it is important for all 50 states, districts, territories, and institutions to recognize FPA as the full potential of APRNs and RNs. FPA for APRNs should include their ability to prescribe all medications in which they are trained, including selected opioids (hydrocodone and morphine are examples), buprenorphine, and naltrexone. The latter two drugs are life-saving antidotes for people who are opioid dependent. Some patients require access to opioid analgesics for severe pain [14, 41]. APRNs who are trained in pain management should not be limited in prescribing them. In some states, patients do not have access to benzodiazepines, a controlled medication used for anxiety, through their APRNs. And therefore, APRNs who provide psychiatric and mental health services should be able to prescribe them when necessary.
Also, as noted earlier, it is important for families to have closure when a loved one dies. Any clinician who is trained in and competent to sign death certificates should be able to do so. When Florida still required NPs to have approval from their contracted physician to sign off on death certificates, one NP’s family, for example, had to wait 30 days for a death certificate after their older adult father passed away. The family could not afford the cost of a private medical examiner to declare death. In many states, NPs are not authorized to certify a death [42].
The NAM Future of Nursing report underscored to achieve health equity, it is imperative that all public and institutional policies fully modernize the roles of APRNs, RNs, and LPNs. This should also be done with regulations pertaining to unlicensed staff like certified nurse aides, home health aides, and others [43]. In addition, nurses are encouraged to get involved in their state and national organizations.
The COVID-19 pandemic laid bare our nation’s health disparities among underserved communities. With FPA in each state and in every healthcare system, we can help improve health equity. However, modernizing workforce scope of practice policies is only one set of strategies that are necessary to achieve health equity. Another very critical component to achieving health equity is to have a nursing workforce that reflects the nation’s population. This includes having nurses of color at all levels of care, including in leadership positions in care delivery, academia, research, and on boards.
Globally, capitalizing on APNs’ potential would help countries care for those most in need of care, in addition to containing costs. Countries without associations are encouraged to join international organizations for steps to achieve and sustain health equity.
Study Guide Questions
-
1.
How does increasing access to care for nurses help achieve health equity?
-
2.
How would you frame the access to APRN care issue with policymakers from the conservative and the liberal perspectives?
-
3.
Describe the importance of coalitions when seeking policy changes.
-
4.
How are barriers to care more challenging for people who are experiencing homelessness versus those in the general population?
-
5.
The youngest baby boomer in the United States will be 65 years of age in 2030. What can we learn from Japan’s story in preparation for 2030?
References
Brodsky PL. Where have all the midwives gone? J Perinat Educ. 2008;17(4):48–51. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2582410/. https://doi.org/10.1624/105812408X324912.
Nadelson C. Woman and psychiatry. In: Smelser NJ, Baltes PB, editors. International encyclopedia of social and behavioral sciences. Oxford: Elsevier Science Ltd; 2001. [cited 2022 Aug 16] Chapter 1. https://www.sciencedirect.com/topics/nursing-and-health-professions/nurse-midwife.
Buerhaus PI, Auderbach DI. Market for professional nurses in the U.S. In: Encyclopedia of health economics. New York: Springer; 2014. p. 199–209. https://www.sciencedirect.com/topics/nursing-and-health-professions/clinical-nurse-specialist.
Cannaby AM, Carter V, Rolland P, Finn A, Owen J. The scope and variance of clinical nurse specialist job descriptions. Br J Nurs. 2020;29(11):606–11. https://pubmed.ncbi.nlm.nih.gov/32516038/. https://doi.org/10.12968/bjon.2020.29.11.606.
Lusk B, Cockerham AZ, Keeling AW. In: Tracy MF, O’Grady ET, editors. Hamric and Hanson’s Advanced practice nursing: an integrative approach. 6th ed. Amsterdam: Elsevier; 2018.
The future of nursing 2020-2030: Charting a path to achieve health equity. National Academies of Sciences, Engineering, and Medicine. The National Academies Press, 2021. https://doi.org/10.17226/25982.
The future of nursing: Leading change, advancing health. Institute of Medicine (US) Committee on the Robert Wood Johnson Foundation Initiative on the Future of Nursing, at the Institute of Medicine. Washington, DC: National Academies Press; 2011 [cited 2022 Aug 11]. https://doi.org/10.17226/12956.
Four types of APRNs. Campaign for Action. [cited 2022 Dec 2022]. https://campaignforaction.org/resource/types-advanced-practice-registered-nurses/.
Our story and timeline. Campaign for Action (2022). [cited 2022 Nov 22]. https://campaignforaction.org/about/our-story/.
State Practice Environment. American Association of Nurse Practitioners. [updated 2022 10; cited 2022 Nov 20]. https://www.aanp.org/advocacy/state/state-practice-environment.
Kingdon JW, Stano E. Agendas, alternatives, and public policies. Boston: Little Brown and Company; 1984.
Lovell A. Agendas, alternatives and public policies. 2010 [cited 2022 Aug 16]. https://pdfs.semanticscholar.org/b601/985c67970ba87d79fabf6160ca91b1933003.pdf.
Kelley J. Improving consumers’ access to practice and care: state progress in improving access to care by nurse practitioners. Campaign for Action, [cited 2022 April 18]. https://campaignforaction.org/wp-content/uploads/2022/04/Dashboard-Map-Removing-Barriers-to-Practice-and-Care-4-18-2022-scaled.jpg.
Denis AM. Managing opioid use disorder: the nurse practitioner addressing the challenge CNE series. 2019 Sep [cited 2022 Aug 22];28(5):281–316. https://www.proquest.com/openview/cf2411ca358ad0f0ac91d0b4f984bbac/1.pdf?pq-origsite=gscholar&cbl=30764.
Singer A, Mertz L. The future of nursing West Virginia: creating jobs, improving health. Campaign for Action; 2021 Sep [cited 2022 Aug 18]. https://campaignforaction.org/the-future-of-nursing-west-virginia-creating-jobs-improving-health/, https://campaignforaction.org/the-future-of-nursing-west-virginia-creating-jobs-improving-health/.
Young HM, Quinn W, Brassard A, Gualtieri C, Reinhard S. COVID-19 pandemic spurs policy changes benefiting older adults. J Gerontol Nurs. 2020;46(6):19–23. https://doi.org/10.3928/00989134-20200515-01.
Knowles M, Siple A. Legislative update on Kansas [Meeting] Center to champion nursing in America Access to Care Learning Collaborative; 2022.
Allen J. Collecting stories of APRN barriers [email] message to: Quinn W. 2021 May 14 [cited 2022 Dec 9].
Consumers benefited when a hospital removed barriers to nursing care during the pandemic; Join a webinar to learn how nurse leaders at Mt. Sinai Health System accomplished it. 2022 Campaign for Action, [cited 2022 Aug 16]. https://campaignforaction.org/hospital-removed-barriers-to-nurse-care/.
Hideyo T, Broome ME, Mai T. Advancing nurses’ role to address issues facing Japanese anesthesia practice. AANA J. 2020;88(6):453–8. https://pubmed.ncbi.nlm.nih.gov/33218380/.
Montemuro MA. The evolution of the clinical nurse specialist: response to the challenge of professional nursing practice. Clin Nurse Spec. 1987;1(3):106–10. https://pubmed.ncbi.nlm.nih.gov/3651963/.
Henni SH, Kirkevold M, Antypas K, Foss C. Perceptions of the scope of practice of nurse practitioners caring for older adults: level of agreement among different healthcare providers. Scand J Caring Sci. 2021;35(2):492–501. https://pubmed.ncbi.nlm.nih.gov/31348141/.
Global Health. Healthy people [updated 2022 Feb 6; cited 2022 Aug 22]. https://www.healthypeople.gov/2020/topics-objectives/topic/global-health.
Guidelines on advanced practice nursing. International Council of Nursing 2020 [cited 2022 Aug 15]. https://www.icn.ch/system/files/documents/2020-04/ICN_APN%20Report_EN_WEB.pdf.
Fritz S, Chaitow L, Hymel GM. Clinical massage in the healthcare setting medical and health-related professionals (Chapter 3). Maryland Heights: Mosby; 2008. p. 54–85. https://www.sciencedirect.com/topics/medicine-and-dentistry/nurse-anesthetist.
Fulton J. Clinical nurse specialists international. Clin Nurse Spec. 2018;32(6):288–9. https://doi.org/10.1097/NUR.0000000000000412.
International Nurse Practitioner Resources: the NP role continues to emerge around the world. American Association of Nurse Practitioners. [cited 2022 Aug 16]. https://www.aanp.org/about/all-about-nps/international.
Midwifery in Japan. Japanese Nurses Association. 2018. https://www.nurse.or.jp/jna/english/midwifery/index.html.
Meeusen V, Ouellette S, Horton B, INF Board Officers 2016. Trends Anaesth Crit Care. 2016 Feb [cited 2022 Aug 11];6:20–25 . https://doi.org/10.1016/j.tacc.2016.03.001.
Nursing and midwifery. World Health Organization [updated 2022 Mar 18; cited 2022 Aug 11]. https://www.who.int/news-room/fact-sheets/detail/nursing-and-midwifery.
Fukuda H, Miyauchi S, Tonai M, Ono M, Magilvy JK, Murashima S. The first nurse practitioner graduate programme in Japan. Int Nurs Rev. 2014;61(4):487–90. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4277332/.
Kondo A. Advanced practice nurses in Japan: education and related issues. J Nurse Care. 2013;s5:004. https://doi.org/10.4172/2167-1168.S5-004.
Kooienga SA, Carryer JB. Globalization and advancing primary health care nurse practitioner practice. J Nurse Pract. 2015;11(8):804–11. https://doi.org/10.1016/j.nurpra.2015.06.012.
Rosa WE, Fitzgerald M, Davis S, Farley JE, Khanyola J, Kwong J, et al. Leveraging nurse practitioner capacities to achieve global health for all: COVID-19 and beyond. Int Nurs Rev. 2020;67(4):554–9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7537537/.
Eklund W. Japan and its healthcare challenges and potential contribution of neonatal nurse practitioners. J Perinat Neonatal Nurs. 2010;24(2):155–166. https://journals.lww.com/jpnnjournal/Abstract/2010/04000/Japan_and_Its_Healthcare_Challenges_and_Potential.11.aspx.
Itoh T, Mori H, Maehara M, Izumi Y. Nurse practitioners’ interdisciplinary practice competencies in Japan: a qualitative research. J Nurse Pract. 2021;17(6):727–31. https://www.sciencedirect.com/science/article/pii/S155541552100060X.
Kansas Board of Nursing. Important update on APRN changes [updated 2022 July 19; cited 2022 Aug 16]. https://ksbn.kansas.gov/wp-content/uploads/2022/07/KSBN-Update-7-19-22.pdf.
Ono M, Miyauchi S, Edzuki Y, Saiki K, Fukuda H, Tonai M, et al. Japanese nurse practitioner practice and outcomes in a nursing home. Int Nurs Rev. 2015;62(2):275–9. https://onlinelibrary.wiley.com/doi/full/10.1111/inr.12158.
Sugiyama S, Asakura K, Takada N. Japanese nurse practitioners’ legal liability ambiguity regarding their medical practice: a qualitative study. BMC Nurs. 2020;19(1):1–6. https://bmcnurs.biomedcentral.com/articles/10.1186/s12912-020-00458-2/.
Moore-Nadler M, Clanton C, Roussel L. Storytelling to capture the health care perspective of people who are homeless. Qual Health Res. 2020;30(2):182–95. https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,shib&db=rzh&AN=140353812&site=ehost-live&scope=site.
McCarty D, Priest KC, Korthuis PT. Treatment and prevention of opioid use disorder: challenges and opportunities. Annu Rev Public Health. 2018;39:525–41.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5880741/. https://doi.org/10.1146/annurev-publhealth-040617-013526.
Ruiz L, Posey BM, Neuilly M, Stohr MK, Hemmens C. Certifying death in the United States. J Forensic Sci. 2018;63(4):1138–45. https://doi.org/10.1111/1556-4029.13689. https://pubmed.ncbi.nlm.nih.gov/29143322/.
Lifting nurse practice barriers to achieve health equity. National Academy of Medicine. The future of nursing 2020-2030: charting a path to health equity. 2021. Report Brief. https://nap.nationalacademies.org/resource/25982/FON%20One%20Pagers%20Lifting%20Barriers.pdf.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

{kind=link}
Cite this chapter
Quinn, W.V., Reinhard, S.C., Little, P.F. (2023). Capitalizing on Nurses’ Potential to Improve Consumers’ Access to Care. In: Hassmiller, S., Darcy Mahoney, A., Beard, K. (eds) The Future of Nursing 2020-2030: Global Applications to Advance Health Equity. Springer, Cham. https://doi.org/10.1007/978-3-031-29746-5_7
Download citation
DOI: https://doi.org/10.1007/978-3-031-29746-5_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-29745-8
Online ISBN: 978-3-031-29746-5
eBook Packages: MedicineMedicine (R0)