
Abstract
In underdeveloped countries (UDCs), the burden of skin disease is disproportionately high while the number of dermatology-trained health professionals is relatively low. As a result, many patients in UDCs suffer from under-diagnosed yet treatable skin conditions. To help alleviate the barriers to dermatologic care, healthcare teams have implemented teledermatology (TD) programs around the world with the goal of improving access, reducing costs, and improving diagnostic accuracy. In this chapter, we describe the various social media platforms, cloud storage services, electronic medical record (EMR) systems, and independent websites that have been deployed in UDCs for TD. We also outline key characteristics and challenges to sustainable TD in UDCs and highlight a few examples of successful TD programs. We conclude by detailing a few quantitative variables that may impact a TD program’s overall success and describe future technological improvements that may continue to aid in the expansion of TD in UDCs.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Global teledermatology
- Underdeveloped countries
- Developing countries
- Low-income countries
- Emerging markets
- Social media
- Cloud-based storage
- EMR systems
Introduction
In 2022, the World Population Review identified 78 underdeveloped countries (UDCs), with 44 (56%) countries in Africa and 22 (28%) in Asia (see Fig. 23.1) [1]. Alternative names for UDCs include “low-income countries” used by the World Bank, “developing countries” or “least-developed countries” used by the United Nations, and “emerging markets” used by other international organizations [2, 3]. Although UDC is an unofficial classification, it is based on seven characteristics: (1) low-income per capita; (2) lack of public and private capital for government projects; (3) population explosion defined as birth rate far exceeding death rate; (4) excessive unemployment caused by slow-growing job markets; (5) predominance of agriculture contributing to national income; (6) small and unproductive investments; and (7) diminished productivity with laborers who are malnourished and have limited classroom education. “UDC” refers to the financial, economic, and age-related demographic aspects of a country and does not assess the people and culture of these countries.

In UDCs, dermatologic care is a crucial component of healthcare needs. Approximately 24% of all medical visits in sub-Saharan Africa involve skin-related conditions [4, 5]. Access to dermatologic care is limited, with many patients not receiving the care they need, resulting in poor health outcomes [6, 7]. In comparison to higher resourced countries, a majority of UDCs have a significantly greater number of disability-adjusted life years (DALYs) due to skin conditions, indicating a higher skin disease burden and lower quality of life. For example, the umbrella category “dermatitis” has the highest DALY rate in sub-Saharan Africa, where many UDCs are located [8]. Due to underdiagnosis and suboptimal management, skin infections account for a significant number of morbidities and mortalities (i.e., 23% misdiagnosis rate for Kaposi’s sarcoma in Uganda) [9]. Cutaneous tuberculosis, leprosy, leishmaniasis, scabies, cutaneous larva migrans, Buruli ulcer, mycetoma, and lymphatic filariasis are also prevalent in UDCs with humid climates and overcrowded regions. These infections and infestations are curable with prompt diagnosis and treatment, signaling a pivotal role of early access to dermatologic care in improving health outcomes [10].
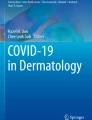
Despite the significant burden of skin diseases, UDCs have a disproportionate unmet need for dermatologic care due to a lack of dermatologists and dermatology training. Of the 55 countries in Africa, there is no opportunity for dermatology specialization in 30 (55%) of the countries [11]. In 2012, the dermatologist-population ratio in Africa was estimated to be 1 dermatologist per 500,000 to 1 million people [12]. In 2021, there were two trained dermatologists in Malawi, a country of almost 20 million people [13]. In stark contrast, the United Kingdom (UK) has 10 dermatologists per million people, the United States of America (USA) has 36 dermatologists per million, and Germany has 65 dermatologists per million (see Fig. 23.2) [14]. Furthermore, similar to those in the USA, many trained dermatologists in UDCs reside in urban areas, leaving suburban and rural populations with limited access to dermatologic care [4, 5, 10]. To address the need for dermatologic care in UDCs, teledermatology has become an expanding, sustainable patient care and dermatology education model.

Bar graph showing the number of dermatologists per million people in select countries, illustrating the scarcity of dermatologists in a majority of UDCs (colored in green) compared to non-UDCs (colored in blue). Most UDCs except Egypt fall below the ideal dermatologist-population ratio of 33.33 dermatologists per million people [11, 13, 14, 72,73,74]
Historically, challenges to teledermatology (TD) in UDCs have been attributed to lack of Internet accessibility, poor connection quality, and cost of implementation [12, 15]. As a measure of TD utilization, we performed a systematic search of each UDC on PubMed using the keywords “teledermatology” and “[UDC name].” As of May 2022, 47 (60%) of the 78 UDCs have no documented TD study or pilot program on PubMed (see Fig. 23.1).
With increasing globalization and technological advancements, barriers to teledermatology are beginning to be addressed. Higher quality mobile phones have become more affordable and accessible, with 83% of people in UDCs having a mobile phone as of 2018 [16]. Humanitarian efforts have spearheaded new projects to connect resources from developed countries with people living in UDCs. Furthermore, the COVID-19 pandemic has accelerated the adoption of TD globally, with new infrastructure in developed countries benefiting UDCs as well [17].
This chapter reviews the numerous platforms that global UDCs have used to implement teledermatology, along with some of their strengths and limitations. We explore the defining characteristics of successful TD programs and derive lessons on how some programs have built sustainable infrastructure with fewer resources. We conclude with a look toward the future with an emphasis on shared resources and technology to expand effective, accessible, and sustainable TD in UDCs.
TD Platforms and Methodologies in UDCs
In UDCs, many TD platforms have been used to transmit and store patient history and clinical media. These TD platforms include mobile phone-based social media, cloud-based platforms, and open-source electronic medical record (EMR) systems (see Table 23.1). The healthcare team operating TD programs varies widely, with a mixture of local general practitioners (GPs), nurses, dermatology officers/physician assistants, domestic teledermatologists, international teledermatologists, medical students, and community healthcare workers (HCWs) working together. The members of the TD healthcare team may be within the UDC or include several international countries.
Social Media
As global access to the Internet has improved [18], social media platforms have become a popular method of daily communication. These platforms have become critical in increasing TD efficiency, usability, and sustainability within UDCs [19]. Many new forms of TD were implemented during the COVID-19 pandemic out of necessity to continue dermatology care in a safer manner compared to face-to-face visits [20].
WhatsApp®, created in the USA, is a free mobile application with many qualities suitable for TD in UDCs. It is used worldwide for everyday communication and has a low barrier to adoption [21]. This platform supports messaging via texts, audio recordings, videos, and images, allowing for synchronous, asynchronous, and hybrid forms of TD. In particular, the ability to send audio recordings in the user’s native language has been shown to increase satisfaction and diagnostic accuracy [22]. WhatsApp is outfitted with end-to-end encryption between users, ensuring communication is safe and secure [23]. Some limitations reported with WhatsApp include decreased image resolution of media, and limited storage and transmission issues [24].
The ease of use of WhatsApp has made it the most popular platform for TD within UDCs like Pakistan, Nepal, Djibouti, Egypt, and India [20, 25,26,27]. Anecdotally, WhatsApp has been successfully used for life-saving TD for a Djiboutian patient with emergent toxic epidermal necrolysis [28] and for a Nepalese patient diagnosed with autosomal recessive congenital ichthyosis [29].
Facebook® is another social media mobile application created in the USA that is now used worldwide. Facebook’s user-friendly interface and ability for active discussions in near real-time greatly increase its long-term sustainability in UDCs. The main concerns with Facebook as a TD tool are patient health information (PHI) breach risks and image quality; however, a survey of Nepalese social media users reports that most people would still be comfortable with sending clinical photos of their skin via Facebook. In fact, hybrid TD with mobile phones was preferred over any other methodology in this study [18].
During the COVID-19 pandemic, Nepalese dermatologists reported that Facebook, along with other social media platforms, such as Viber®, created in Israel, and WhatsApp, have been widely used. Such platforms are adequate in supporting the discussion and diagnosis of common skin disorders like fungal infections, alopecia, and eczema [20]. In the Philippines, health care teams used Facebook Messenger as a component of hybrid TD in which teledermatologists receive clinical images via Facebook Messenger® while speaking to patients via phone calls. This combined approach circumvents the often unstable Internet connection in the Philippines while maintaining personal communication with patients [30]. A TD program in Mexico has uniquely implemented an educational discussion platform using the Facebook website. GPs post clinical photos of skin conditions and include pertinent clinical history as a comment associated with those images. Teledermatologists from a local general hospital would then post comments asking follow-up questions, providing diagnoses, and detailing treatment plans. They mitigate PHI risks by limiting which users have access to the images and information [31].
Zoom® is a live video teleconferencing application developed by Zoom Video Communications in the USA equipped with end-to-end encryption; it has been used to provide synchronous TD during the COVID-19 pandemic in UDCs [32]. Zoom has also been a useful tool for building local dermatology capacity through live instruction. Potential limitations of Zoom utilization in UDCs include the need for a stable Internet connection and minimum recommended bandwidth [33]. In an Egyptian TD study, healthcare teams utilized both Zoom and WhatsApp for synchronous and asynchronous forms of TD, respectively harnessing the advantages of each platform to make the TD experience more efficacious. Of the 62 patients that completed a post-TD telehealth usability questionnaire, 57 of them were satisfied with this dual model of teledermatology and valued TD as effective as a face-to-face visit. A majority of the follow-up appointments after the initial TD consults were also carried out using TD, increasing the availability of in-person dermatology appointments for more urgent cases [25]. Another TD program is using Zoom to host live discussions about clinical indications, recommended diagnoses, and suggested care plans with local HCWs [4].
Social media platforms carry many advantages in facilitating sustainable TD systems within UDCs. Most are free to use, familiar to patients and healthcare teams, and can be used with a mobile phone. The main limitations of using social media have been lack of EMR integration, poor continuity of care, PHI concerns, and lower image quality. As EMR compatibility, phone camera quality, and cybersecurity improve over time, these will become less of a hindrance toward developing sustainable TD infrastructure using social media.
Cloud-Based Storage Platforms
Many TD programs in UDCs have also utilized free or low-cost cloud storage platforms for secure and efficient asynchronous TD. Clinical photos taken with either a camera or a smartphone are uploaded directly to a protected cloud storage, where the teledermatologist can review the photos [34]. A TD study in Haiti is using Google Apps™ to create an encrypted HIPAA-compliant platform that only costs $5 USD per month, providing a financially sustainable method to securely transmit sensitive patient information [35]. Another TD program uses Dropbox®, a widely used cloud storage platform created in the USA, for TD care due to its large storage capacity, rapid dissemination capabilities, user-friendliness, and security. It requires no initial training or technical expertise and allows the referring person to send clinical photos and patient history to an entire healthcare team simultaneously [36].
Telemedicine EMR Systems
While social media and cloud storage platforms are more user-friendly, EMR systems built specifically for telemedicine offer higher layers of security and a more organized structure. Many are low-cost or open-source, allowing for UDCs to employ such platforms in providing TD.
Collegium Telemedicus (CT) is a telemedicine system developed in the UK by Collegium Telemedicus Ltd. that is free for all humanitarian efforts in low-resource settings. It offers secure messaging, central storage of patient information, and ready-made templates designed for TD. This platform allows for TD to be trialed and expanded with low financial risk and provides a foundation for UDCs to create an organized system [15, 37]. Médecins Sans Frontières, also known as Doctors Without Borders, has successfully used the CT network to provide sustainable TD to ten UDCs, with most use cases coming from South Sudan, Ethiopia, and the Democratic Republic of Congo. Some dermatology examples of diagnoses made through CT’s teledemedicine system include leprosy, a mycobacterial infection, and neurofibromatosis [38].
A TD pilot program in Mali has been using Bogou, an inexpensive encrypted, multilingual tele-expertise platform created in Mali that allows file compression so that clinical information can be sent in areas with poor Internet connection [12]. Bogou is available in many UDCs’ official languages, including English, Spanish, French, and Portuguese, streamlining communication for both patients and TD teams. Because of its password protection, encryption, and moderated teams for each patient case, Bogou proves to be a stable and secure method for TD [39].
ClickMedix is a HIPAA-compliant telemedicine platform created by Carnegie Mellon University (Pittsburgh, PA, USA) and the Massachusetts Institute of Technology (MIT, Boston, MA, USA) that offers seamless smartphone-to-website transfer of clinical images, templates for taking patient history and physical exam, and email notifications upon new consults [40]. This platform also allows unlimited images and cases to be uploaded to the encrypted website. While the cost for ClickMedix is more than previous platforms at $200 USD/month, a TD program providing care for patients in Uganda and Guatemala reported that the financial burden decreases as more patients receive appropriate care [41].
iPath is a Switzerland-based telemedicine server that integrates the simplicity of email with the centrality of a website to make an organized, user-friendly EMR system. The referral workflow involves emailing a patient’s clinical information to an iPath server. This information is converted into its own page on the server, which is then sent to the teledermatologist with an email notification. Because iPath’s code is completely free and open-source, this allows TD programs to create further applications to cater to their specific needs while incurring no additional financial burden. iPath has been employed successfully by two TD projects in Ethiopia and South Africa after they initially encountered problems with more inefficient methods for sending patient information, including basic email, HTML pages, and their own telemedicine software [42, 43].
Sana is a free smartphone-based media and clinical information capture tool developed by MIT that integrates with EMR systems like OpenMRS. This allows HCWs to collect and upload patient information from their phones directly to OpenMRS for teledermatologists to examine. Sana works in areas with poor Internet connection: it can temporarily store files on the phone until the connection is adequate, parse large files into smaller pieces, and has several ways to transfer information [44]. One TD project has used OpenMRS in conjunction with Sana to provide low-cost, effective TD for rural regions of Mongolia [45].
Favorable characteristics making telemedicine-adept EMR systems suitable for TD in UDCs include their low costs, PHI security, and greater layers of organization for each clinical encounter. In addition, the aforementioned EMR systems have a simple design that can adequately function in areas with poor Internet infrastructure.
TD-Site-Specific Websites
TD programs in UDCs can also create their own websites to customize the layout and functionality to suit specific needs. One example is the African Teledermatology Project (ATP), created and funded as a joint effort by three dermatology departments in Austria, Philadelphia, and Australia. This program has provided TD to at least 13 countries (11 of them UDCs) since its inception in 2007. ATP incorporates into its website (africa.telederm.org) educational opportunities for referring HCWs and teledermatologists: monthly clinical case conferences, discussion forums, and a formal dermatology curriculum [40, 46]. ATP also creates more targeted educational programs regarding each of its locations’ most prevalent skin conditions. The website’s simplicity helps ensure lower latency in areas with poor connectivity [47]. Other UDCs such as Tanzania, Malawi, and Iran have also used their own websites for TD. However, it has proven difficult for some UDCs to develop their own websites, as it requires initial and recurring financial costs to build and maintain a website [13, 48, 49].
Characteristics for Sustainable TD in UDCs
Many TD programs in UDCs have attributed their success and long-term sustainability to the following: creating long-lasting educational impact, standardizing the patient history and physical examination (H&P), and improving image quality.
One of global TD’s primary goals is to lessen the dependence of UDCs on higher resourced countries for dermatology consults. The educational impact that TD can provide is of great importance for under-resourced areas. Studies have found that diagnostic concordance increases between referring teams and teledermatologists as local HCWs gain more dermatology exposure over time. One study reports an increased diagnostic concordance from 13% to 50% after just nine TD cases [50] while another shows an increase from 44% to 68% after several cases of TD [51]. By expanding upon the reasoning behind a diagnosis and treatment recommendation, teledermatologists can improve local HCWs’ long-term ability to manage similar cases in the future. One TD program in Afghanistan sends pertinent supplementary information about skin conditions through email along with a lengthy explanation of the diagnoses to referring HCWs [52]. Another Afghan TD program incorporates a virtual grand rounds curriculum at Emory University (Atlanta, GA, USA) featuring prior international cases. This gives both US dermatology residents and faculty more international learning opportunities while also improving dermatology care in Afghanistan [53]. Synchronous TD, while usually more time-consuming and costly than asynchronous TD, allows for the teledermatologist to explain to both the referring team and patient the rationale for diagnostic treatment and answer any questions in real-time [54]. Lastly, providing local healthcare teams with point-of-care dermatology tools and information readily accessible on mobile devices is fundamental to increasing long-term educational impact. A Botswana TD program was able to increase self-learning of dermatology, with five out of six residents seeking out supplementary materials even when not in the hospital [55]. Effective dermatology education should be a central component in any TD program seeking to provide sustainable care.
Standardization of patient H&P collection is also critical within TD infrastructure, as insufficient histories can result in an inability to diagnose or adequately treat patients [36, 46, 47, 56]. Multiple TD programs describe a dermatology-specific history form with the acronym SCALDA for the referring HCWs to better understand what information to collect: “Size, shape, surface; Color; Arrangement; Lesion type; Distribution; Always check hair, nail, mucous, intertriginous areas” [35, 38]. While using referral templates can increase the overall time spent per patient, higher quality patient information provided from these templates can improve teledermatologists’ ability to provide a diagnostic recommendation [7, 50].
Since TD is highly dependent on images, many TD quality improvement efforts have focused on image resolution optimization. Poor image quality is often the sole reason why some TD cases (3–8%) result in no diagnosis [12, 41, 46, 52]. To enhance overall image quality, recommended image guidelines involve the following: initial training on using the media capture device [45, 57], obtaining proper lighting beforehand [58], using a uniform background [59], taking at least two pictures of the skin lesion from different angles [38] along with taking pictures of other parts of the body that could provide clues [25], and using optimal image formatting [7, 35] and image compression [51, 60]. Adhering to such measures allow teledermatologists to adequately examine the skin condition in the images and provide the best possible diagnosis.
Barriers to Sustainable TD in UDCs
The most significant limitations for building sustainable TD programs in UDCs include lack of technology infrastructure, cost, inadequate local workforce, and resistance to TD adoption [61].
Poor infrastructure in UDCs can hinder the integration of TD care. Power outages without a backup electricity source, bug infestations leading to mangled electrical wiring, and unreliable Wifi speeds can all disrupt TD workflow [12, 35, 48]. Many UDCs also lack established diagnostic capabilities, including dermatopathology testing [62], skin cultures, and immunohistochemical staining [34, 52, 63]. This lack of comprehensive confirmatory testing can lead to uncertain or inaccurate diagnoses. Moving forward, grants such as the International League of Dermatological Societies’ DermLink Grant of up to $5000 can help bridge the financial gap in creating the infrastructure necessary for sustainable TD [64].
An insufficient local workforce is also a common hindrance in low-resourced regions. Understaffed clinics may be hesitant to add on a TD service, as it would create extra work for already overworked employees [46, 65]. A way to sustainably alleviate physician workload is to train other HCWs or students to carry out the necessary steps for TD referrals [41, 43]. Another successful but limited avenue is through the American Academy of Dermatology Resident International Grant, which sends a dozen US and Canadian dermatology residents to multiple UDCs each year to help establish a stronger dermatology foundation in the area and learn more about global dermatology [66, 67]. The traveling residents can help launch TD services along with training local HCWs to maintain TD functionality.
Local resistance to TD often stems from cultural or religious beliefs, concerns about TD’s patient privacy, or opposition to seeking foreign help [5, 46]. The ATP has also noted that some HCWs do not like asking for help via TD [12]. One program has remedied this by having medical students serve as on-site proxies within clinics in UDCs. The medical students develop longitudinal relationships with local HCWs, gaining their trust and ultimately increasing the utilization of TD [41].
Quantitative Variables to Measure TD Program Success
Certain objective variables can help measure the overall success of TD programs in UDCs: (1) patient case volume [7, 35, 54]; (2) diagnostic concordance between teledermatologists and local health teams or in-person dermatologists [47, 51, 59]; (3) response time [12, 21, 38]; (4) cost of TD per patient [20, 41, 45, 52]; and (5) overall patient/TD team satisfaction [22, 36, 53]. These five variables are measurable and may be tracked over time to guide management of a TD program’s effectiveness and sustainability in UDCs.
Future Improvements of TD in UDCs
Many TD programs in UDCs currently operate as isolated, distinct entities with fewer resources compared to programs like the ATP, a collaborative TD network of dozens of countries. Increased partnerships and shared resources among programs can further strengthen TD’s long-term sustainability in UDCs. Future technological advancements will also improve TD in UDCs through increased democratization of information, growing access to Internet and mobile phones, improved image quality, and new innovative applications. One such advancement is Starlink, which seeks to provide a reliable Internet connection to any part of the world via thousands of satellites, potentially serving as a dependable foundation of communication for TD in UDCs [68].
Conclusion
This chapter outlines several ways to lower the barriers to starting and maintaining TD services in UDCs. Cost is a significant concern to mitigate when measuring the long-term sustainability of TD in low-resourced settings. Free social media applications as well as open-source telemedicine and EMR systems may help alleviate these financial burdens. Low-cost cloud storage systems have also proven satisfactory in providing a blend of greater organization than social media platforms and greater simplicity than EMR systems or site-specific websites. Beyond choosing the right vehicle for transferring clinical information, programs can also optimize the impact and quality of TD by including educational components, standardizing information given within referrals, ensuring adequate staffing, and gaining the trust of local patients and HCWs. While there are many obstacles to implementing TD, employing the aforementioned strategies can greatly increase the long-term success of dermatology care in UDCs.
References
World Population Review: Underdeveloped countries 2022. 2022. https://www.worldpopulationreview.com/country-rankings/underdeveloped-countries. Accessed 19 Apr 2022.
United Nations Department of Economic and Social Affairs Economic Analysis: Least developed countries (LDCs). 2022. https://www.un.org/development/desa/dpad/least-developed-country-category.html. Accessed 8 June 2022.
The World Bank: World Bank country and lending groups. 2022. https://www.datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups . Accessed 8 June 2022.
Lewis H, Becevic M, Myers D, Helming D, Mutrux R, Fleming D, et al. Dermatology ECHO—an innovative solution to address limited access to dermatology expertise. Rural Remote Health. 2018:10.22605/RRH4415.
Coates SJ, Kvedar J, Granstein RD. Teledermatology: from historical perspective to emerging techniques of the modern era. J Am Acad Dermatol. 2015;72(4):563–74. https://doi.org/10.1016/j.jaad.2014.07.061.
Nelson CA, Takeshita J, Wanat KA, Bream KD, Holmes JH, Koenig HC, et al. Impact of store-and-forward (SAF) teledermatology on outpatient dermatologic care: a prospective study in an underserved urban primary care setting. J Am Acad Dermatol. 2016;74(3):484–90.e1. https://doi.org/10.1016/j.jaad.2015.09.058.
Kaliyadan F, Venkitakrishnan S. Teledermatology: clinical case profiles and practical issues. Indian J Dermatol Venereol Leprol. 2009;75(1):32–5. https://doi.org/10.4103/0378-6323.45217.
Karimkhani C, Dellavalle RP, Coffeng LE, Flohr C, Hay RJ, Langan SM, et al. Global skin disease morbidity and mortality. JAMA Dermatol. 2017;153(5):406–12. https://doi.org/10.1001/jamadermatol.2016.5538.
Seth D, Cheldize K, Brown D, Freeman EF. Global burden of skin disease: inequities and innovations. Curr Dermatol Rep. 2017;6(3):204–10. https://doi.org/10.1007/s13671-017-0192-7.
Afsar FS. Skin infections in developing countries. Curr Opin Pediatr. 2010;22(4):459–66. https://doi.org/10.1097/mop.0b013e32833bc468.
Mosam A, Todd G. Dermatology training in Africa: successes and challenges. Dermatol Clin. 2021;39(1):57–71. https://doi.org/10.1016/j.det.2020.08.006.
Faye O, Bagayoko C, Dicko A, Cissé L, Berthé S, Traoré B, et al. A teledermatology pilot programme for the management of skin diseases in primary health care centres: experiences from a resource-limited country (Mali, West Africa). Trop Med Infect Dis. 2018; https://doi.org/10.3390/tropicalmed3030088.
Galván-Casas C, Mitjá O, Esteban S, Kafulafula J, Phiri T, Navarro-Fernández Í, et al. A facility and community-based assessment of scabies in rural Malawi. PLoS Negl Trop Dis. 2021; https://doi.org/10.1371/journal.pntd.0009386.
Tiwari R, Amien A, Visser WI, Chikte U. Counting dermatologists in South Africa: number, distribution and requirement. Br J Dermatol. 2022; https://doi.org/10.1111/bjd.21036.
Wootton R, Bonnardot L. Experience of supporting telemedicine networks with the collegium system: first 6 years. Front Public Health. 2019; https://doi.org/10.3389/fpubh.2019.00226.
Brookings: Mobile phones are key to economic development. Are women missing out? 2019. https://www.brookings.edu/blog/future-development/2019/04/10/mobile-phones-are-key-to-economic-development-are-women-missing-out/#:~:text=Fresh%20Gallup%20World%20Poll%20data,Yet%20digital%20divides%20persist. Accessed 10 Jun 2022.
Farr MA, Duvic M, Joshi TP. Teledermatology during COVID-19: an updated review. Am J Clin Dermatol. 2021;22(4):467–75. https://doi.org/10.1007/s40257-021-00601-y.
Pokharel S, Poudel S, Agrawal S, Marahatta S. Awareness, acceptability, and satisfaction of teledermatology consultation among social-media users in Nepal. J Cosmet Dermatol. 2021;00:1–7. https://doi.org/10.1111/jocd.14557.
Jha SM, Dangol AKS, Suwal B, Yadav J. Fungal infections among teledermatology consultations in dermatology department of a tertiary care hospital: a descriptive cross-sectional study. J Nepal Med Assoc. 2021;59(243):1094–7. https://doi.org/10.31729/jnma.5900.
Paudel V. Patterns and barriers of teledermatology in resource-limited settings in COVID-19 pandemic: a descriptive cross-sectional survey of Nepalese dermatologists. JAAD Int. 2022;7:62–6. https://doi.org/10.1016/j.jdin.2022.02.011.
Handa S, Mehta H, Bishnoi A, Vinay K, Mahajan R, Tk N, et al. Teledermatology during the COVID-19 pandemic: experience at a tertiary care Centre in North India. Dermatol Ther. 2021; https://doi.org/10.1111/dth.15022.
Khalid T, Tariq R, Alia S, Ather R. Teledermatology using WhatsApp messenger during COVID 19 pan-demic; our experience of a cost-effective solution to reach out patients in limited resource settings. In: Journal of Health Informatics in Developing Countries 2021. https://www.jhidc.org/index.php/jhidc/article/view/288. Accessed 11 Mar 2022.
WhatsApp: WhatsApp security. 2022. https://www.whatsapp.com/security/#:~:text=WhatsApp’s%20end%2Dto%2Dend%20encryption,in%20between%2C%20not%20even%20WhatsApp. Accessed 10 June 2022.
Singhal RR, Talati KN, Gandhi BP, Shinde MK, Nair PA, Phatak AG. Prevalence and pattern of skin diseases in tribal villages of Gujarat: a teledermatology approach. Indian J Community Med. 2020;45(2):199–203. https://doi.org/10.4103/ijcm.IJCM_76_19.
Mostafa PIN, Hegazy AA. Dermatological consultations in the COVID-19 era: is teledermatology the key to social distancing? An Egyptian experience. J Dermatolog Treat. 2020;33(2):910–5. https://doi.org/10.1080/09546634.2020.1789046.
Yadav D, Bhatia S, Ramam M, Singh V, Khanna N, Khandpur S, et al. Patient perception and satisfaction with a smartphone-based teledermatology service initiated during the COVID-19 pandemic at a tertiary care hospital in North India. Indian J Dermatol Venereol Leprol. 2022:10.25259/IJDVL_608_2021.
Sharma A, Jindal V, Singla P, Goldust M, Mhatre M. Will teledermatology be the silver lining during and after COVID-19? Dermatol Ther. 2020; https://doi.org/10.1111/dth.13643.
Paudel V, Chudal D. Carbamazepine-induced toxic epidermal necrolysis managed by mobile teledermatology in COVID-19 pandemic in rural Nepal. Case Rep Dermatol Med. 2020; https://doi.org/10.1155/2020/8845759.
Pickard-Gabriel CJ, Rudinsky S. Difficult diagnoses in an austere environment: a clinical vignette? The presentation, diagnosis, and management of ichthyosis. J Spec Oper Med. 2013;13(1):61–5.
Tinio PA, Melendres JM, Chavez CP, Agon MK, Merilleno AS, Balagat R, et al. Clinical profile and response to treatment of patients with psoriasis seen via teledermatology during the COVID-19 pandemic in The Philippines. JAAD Int. 2022;7:35–7. https://doi.org/10.1016/j.jdin.2022.02.001.
Garcia-Romero M, Prado F, Dominguez-Cherit J, Hojyo-Tomomka M, Arenas R. Teledermatology via a social networking web site: a pilot study between a general hospital and a rural clinic. Telemed J E Health. 2011;17(8):652–5. https://doi.org/10.1089/tmj.2011.0038.
Zoom Support: End-to-end (E2EE) encryption for meetings. 2022. https://support.zoom.us/hc/en-us/articles/360048660871-End-to-end-E2EE-encryption-for-meetings. Accessed 14 June 2022.
Zoom Support: Zoom system requirements: windows, macOS, Linux. 2022. https://support.zoom.us/hc/en-us/articles/201362023-Zoom-system-requirements-Windows-macOS-Linux#:~:text=Bandwidth%20requirements,-The%20bandwidth%20used&text=For%201%3A1%20video%20calling,3.0Mbps%20(up%2Fdown. Accessed 14 June 2022.
Bobbs M, Bayer M, Frazer T, Humphrey S, Wilson B, Olasz E, et al. Building a global teledermatology collaboration. Int J Dermatol. 2016;55(4):446–9. https://doi.org/10.1111/ijd.13223.
Cutler L, Ross K, Withers M, Chiu M, Cutler D. Teledermatology: meeting the need for specialized care in rural Haiti. J Health Care Poor Underserved. 2019;30(4):1394–406. https://doi.org/10.1353/hpu.2019.0097.
Saleh N, Hay RA, Hegazy R, Hussein M, Gomaa D. Can teledermatology be a useful diagnostic tool in dermatology practice in remote areas? An Egyptian experience with 600 patients. J Telemed Telecare. 2016;23(2):233–8. https://doi.org/10.1177/1357633X16633944.
Wootton R, Wu W, Bonnardot L. Nucleating the development of telemedicine to support healthcare workers in resource-limited settings: a new approach. J Telemed Telecare. 2013;19(7):411–7. https://doi.org/10.1177/1357633X13506511.
Delaigue S, Morand J, Olson D, Wootton R, Bonnardot L. Teledermatology in low-resource settings: the MSF experience with a multilingual tele-expertise platform. Front Public Health. 2014; https://doi.org/10.3389/fpubh.2014.00233.
Fondation Pierre Fabre: Bogou. https://www.odess.io/initiative-detail/bogou.html. Accessed 18 May 2022.
Osei-tutu A, Shih T, Rosen A, Amanquah N, Chowdhury M, Nijhawan RI, et al. Mobile teledermatology in Ghana: sending and answering consults via mobile platform. J Am Acad Dermatol. 2013;69(2):e90–1. https://doi.org/10.1016/j.jaad.2012.08.008.
Greisman L, Nguyen T, Mann R, Baganizi M, Jacobson M, Paccione G, et al. Feasibility and cost of a medical student proxy-based mobile teledermatology consult service with Kisoro, Uganda, and Lake Atitlán, Guatemala. Int J Dermatol. 2014;54(6):685–92. https://doi.org/10.1111/ijd.12708.
Brauchli K, O’Mahony D, Banach L, Oberholzer M. iPath—a telemedicine platform to support health providers in low resource settings. Stud Health Technol Inform. 2005;114:11–7.
Shiferaw F, Zolfo M. The role of information communication technology (ICT) towards universal health coverage: the first steps of a telemedicine project in Ethiopia. Glob Health Action. 2012; https://doi.org/10.3402/gha.v5i0.15638.
Sana: The Sana technology overview. http://www.kidk.net/sanamobile/tech.html. Accessed 20 May 2022.
Byamba K, Syed-Abdul S, García-Romero M, Huang C, Nergyi S, Nyamdorj A, et al. Mobile teledermatology for a prompter and more efficient dermatological care in rural Mongolia. Br J Dermatol. 2015;173(1):265–7. https://doi.org/10.1111/bjd.13607.
Kaddu S, Soyer H, Gabler G, Kovarik C. The Africa Teledermatology project: preliminary experience with a sub-Saharan teledermatology and e-learning program. J Am Acad Dermatol. 2009;61(1):155–7. https://doi.org/10.1016/j.jaad.2008.12.007.
Lipoff J, Cobos G, Kaddu S, Kovarik C. The Africa Teledermatology project: a retrospective case review of 1229 consultations from sub-Saharan Africa. J Am Acad Dermatol. 2015;72(6):1084–5. https://doi.org/10.1016/j.jaad.2015.02.1119.
Schmid-Grendelmeier P, Doe P, Pakenham-Walsh N. Teledermatology in sub-Saharan Africa. Curr Probl Dermatol. 2003;32:233–46. https://doi.org/10.1159/000067349.
Mahdieh M, Kambiz B, Shahram T. Design and implementation a web base teledermatology system to reduce provincial travelling in Kerman Medical University. Health Inf Manag. 2015;11(6):681–8.
Colven R, Shim MM, Brock D, Todd G. Dermatological diagnostic acumen improves with use of a simple telemedicine system for underserved areas of South Africa. Telemed J E Health. 2011;17(5):363–9. https://doi.org/10.1089/tmj.2010.0163.
Caumes E, Le Bris V, Couzigou C, Menard A, Janier M, Flahault A. Dermatoses associated with travel to Burkina Faso and diagnosed by means of teledermatology. Br J Dermatol. 2004;150(2):312–6. https://doi.org/10.1111/j.1365-2133.2004.05745.x.
Ismail A, Stoff B, McMichael J. Store-and-forward teledermatology service for primary care providers in Afghanistan. Int J Dermatol. 2018;57(11):e145–7. https://doi.org/10.1111/ijd.14165.
Yeung H, Sargen MR, Luk KM, Berry EG, Gurnee EA, Heuring E, et al. Teledermatology and teledermatopathology as educational tools for international dermatology: a virtual grand rounds pilot curriculum. Int J Dermatol. 2018;57(11):1358–62. https://doi.org/10.1111/ijd.14014.
Rajagopal R, Sood A, Arora S. Teledermatology in air force: our experience. Med J Armed Forces India. 2009;65(4):342–6. https://doi.org/10.1016/S0377-1237(09)80096-8.
Chang AY, Ghose S, Littman-Quinn R, Anolik RB, Kyer A, Mazhani L, et al. Use of mobile learning by resident physicians in Botswana. Telemed J E Health. 2012;18(1):11–3. https://doi.org/10.1089/tmj.2011.0050.
Tran K, Ayad M, Weinberg J, Cherng A, Chowdhury M, Monir S, et al. Mobile teledermatology in the developing world: implications of a feasibility study on 30 Egyptian patients with common skin diseases. J Am Acad Dermatol. 2011;64(2):302–9. https://doi.org/10.1016/j.jaad.2010.01.010.
Lasierra N, Alesanco A, Gilaberte Y, Magallón R, García J. Lessons learned after a three-year store and forward teledermatology experience using internet: strengths and limitations. Int J Med Inform. 2012;81(5):332–43. https://doi.org/10.1016/j.ijmedinf.2012.02.008.
Lee M, Stavert R. Factors contributing to diagnostic discordance between store-and-forward teledermatology consultations and in-person visits: case series. JMIR Dermatol. 2021; https://doi.org/10.2196/24820.
Patro BK, Tripathy JP, De D, Sinha S, Singh A, Kanwar AJ. Diagnostic agreement between a primary care physician and a teledermatologist for common dermatological conditions in North India. Indian Dermatol Online J. 2015;6(1):21–6. https://doi.org/10.4103/2229-5178.148927.
Bakhshali MA, Gholizadeh M, Layegh P, Nahidi Y, Memarzadeh Z, Meybodi NT, et al. Evaluation of high-efficiency image coding algorithm for dermatology images in teledermatology. Skin Res Technol. 2021;27(6):1162–8. https://doi.org/10.1111/srt.13081.
Desai B, McKoy K, Kovarik C. Overview of international teledermatology. Pan Afr Med J. 2010;6:3.
Tsang MW, Kovarik CL. Global access to dermatopathology services: physician survey of availability and needs in sub-Saharan Africa. J Am Acad Dermatol. 2010;63(2):346–8. https://doi.org/10.1016/j.jaad.2009.09.038.
Ismail A, McMichael JR, Stoff BK. Utility of international store-and-forward teledermatopathology among a cohort of mostly female patients at a tertiary referral center in Afghanistan. Int J Womens Dermatol. 2018;4(2):83–6. https://doi.org/10.1016/j.ijwd.2017.10.011.
ILDS: 2021 DermLink Grant recipients announced 2021. https://ilds.org/news/2021-dermlink-grant-recipients-announced/. Accessed 17 Apr 2022.
Mars M. Health capacity development through telemedicine in Africa. Yearb Med Inform. 2010:87–93.
Introcaso CE, Kovarik CL. Dermatology in Botswana: the American Academy of Dermatology’s Resident International Grant. Dermatol Clin. 2011;29(1):63–7. https://doi.org/10.1016/j.det.2010.09.001.
American Academy of Dermatology Association: Resident International Grant. 2022. https://www.aad.org/member/career/awards/resident-international. Accessed 17 Apr 2022.
Mann A, Pultarova T, Howell E. SpaceX Starlink internet: costs, collision risks and how it works. In: Spacecom. 2022. https://www.space.com/spacex-starlink-satellites.html. Accessed 27 May 2022.
MapChart: World map: simple. 2022. https://www.mapchart.net/world.html. Accessed 5 Jun 2022.
Kravets K, Vasylenko O, Dranyk Z, Bogomolets O. Store-and-forward teledermatology for the most common skin neoplasms in Ukraine. Acta Dermatovenerol Alp Pannonica Adriat. 2018;27(2):79–83. https://doi.org/10.15570/actaapa.2018.18.
Rashid E, Ishtiaq O, Gilani S, Zafar A. Comparison of store and forward method of teledermatology with face-to-face consultation. J Ayub Med Coll Abbottabad. 2003;15(2):34–6.
Marahatta S, Marahatta SB. Challenges of COVID-19 pandemic: dermatologist’s perspective from Nepal. Int J Dermatol. 2020;59(12):1537–8. https://doi.org/10.1111/ijd.15236.
Global Psoriasis Atlas: Global Psoriasis Atlas annual report year 2: April 2018-March 2019. 2019. https://www.globalpsoriasisatlas.org/uploads/attachments/ckia5zj61013d54jnh1fdsj29-global-psoriasis-atlas-annual-report-april-2018-march-2019.pdf. Accessed 15 Jun 2022.
Coustasse A, Sarkar R, Abodunde B, Metzger BJ, Slater CM. Use of teledermatology to improve dermatological access in rural areas. Telemed J E Health. 2019;25(11):1022–32. https://doi.org/10.1089/tmj.2018.0130.
Daman R, Tripathi MM. Encryption tools for secured health data in public cloud. Int J Innov Sci Technol. 2015;2(11):843–8.
Dropbox: Social Impact. 2022. https://www.dropbox.com/social-impact. Accessed 18 Jun 2022.
Dropbox: Get a Dropbox free account. https://www.dropbox.com/basic. Accessed 18 Jun 2022.
Collegium Telemedicus: Frequently asked questions. https://www.collegiumtelemedicus.org/ct/faqs.php. Accessed 18 Jun 2022.
McGoey AT, Oakley A, Rademaker M. Waikato teledermatology: a pilot project for improving access in New Zealand. J Telemed Telecare. 2015;21(7):414–9. https://doi.org/10.1177/1357633X15583216.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Ethics declarations
The authors have no sources of funding to disclose.
Conflict of Interest
The authors declare that they do not have conflict of interest to disclose.
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Hwang, J.C., Tung, J.K., James, A.J. (2023). Global Teledermatology in Underdeveloped Countries. In: English III, J.C. (eds) Teledermatology. Updates in Clinical Dermatology. Springer, Cham. https://doi.org/10.1007/978-3-031-27276-9_23
Download citation
DOI: https://doi.org/10.1007/978-3-031-27276-9_23
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-27275-2
Online ISBN: 978-3-031-27276-9
eBook Packages: MedicineMedicine (R0)