
Abstract
Endoscopy plays a crucial role in the diagnosis and management of inflammatory bowel diseases. Endoscopy has been shown to be fundamental during follow-up through monitoring of response to therapy and assessment of mucosal healing, which has been associated with improved long-term outcomes. Despite advances in medical and surgical treatments, many patients with IBD still go on to develop disease complications such as strictures, penetrating disease, or malignancy, highlighting the need for additional treatment options. In recent years, the role of endoscopy has expanded to add a variety of non-invasive techniques to our therapeutic armamentarium in IBD. In this review article, we discuss the different techniques used in the management of strictures, the importance of endoscopy in the monitoring and management of dysplasia and will provide a glimpse into novel and future therapeutic endoscopic options in IBD.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Crohn’s disease
- Inflammatory bowel disease
- Ulcerative colitis
- Stricture
- Endoscopic balloon dilation
- Stricturotomy
- Dysplasia
- Chromoendoscopy
- Sinusotomy
- J-pouch
Introduction
Inflammatory bowel diseases (IBD), comprised of ulcerative colitis (UC) and Crohn’s disease (CD), are chronic immune-mediated inflammatory diseases of the gastrointestinal tract leading to significant morbidity in affected patients. More than two million North Americans are estimated to have IBD, with worldwide incidence rates increasing significantly over the last few years [1]. Endoscopy plays a crucial role in the diagnosis and management of inflammatory bowel diseases [2]. In addition to its well-established role in the diagnosis of IBD, endoscopy has been shown to be fundamental during follow-up through monitoring of response to therapy and assessment of mucosal healing, which has been associated with improved long-term outcomes [3]. However, despite advances in medical and surgical treatments, many patients with IBD go on to develop disease complications such as strictures, penetrating disease or malignancy, highlighting the need for additional therapeutic options. In recent years, the role of endoscopy has therefore expanded to add a variety of non-invasive techniques to our therapeutic armamentarium in IBD. In the following chapter we will discuss the different types of endoscopic techniques used in the treatment of IBD, with a focus on the management of stricturing complications and dysplasia.
Endoscopic Management of Strictures
About 20% of patients with Crohn’s disease have a stricture at the time of diagnosis, and up to half of patients may develop strictures over the course of their disease [4]. Strictures most commonly occur in the small bowel, but can be found anywhere throughout the gastrointestinal tract, including the colon [5]. In patients with UC, colonic strictures are usually managed surgically given the risk of underlying malignancy. In Crohn’s disease, strictures in the colon are associated with an increased risk of malignancy and surgery is therefore considered earlier in the management algorithm, particularly in the setting of medically refractory disease [6, 7].
Several modalities are available for the management of small bowel CD strictures, including medical therapy, endoscopic techniques, and surgery. A multidisciplinary team approach to discussing these patients is therefore important in order to help decision-making and optimize outcomes [8].
Endoscopic Balloon Dilation
Although multiple endoscopic modalities have been described in the treatment of strictures, endoscopic balloon dilation (EBD) remains the cornerstone of endoscopic stricture management [5]. In a large meta-analysis including individual patient level data, EBD was found to have a clinical efficacy rate of 80.8% with an immediate technical success rate of up to 89.1% [9]. EBD can be used in both naïve and anastomotic strictures and is an option for straight and short (<5 cm) strictures that can be reached endoscopically. There should not be an associated abscess, internal fistula, or suspected malignancy [5].
Stricture biopsies are recommended prior to dilation in order to rule out cancer, although this is rare in the small bowel [10]. EBD is performed with the use of a through-the-scope balloon and can be done in the setting of both standard endoscopy and balloon-assisted enteroscopy [11]. Complications associated with EBD can occur in up to 4% of patients and include infection, perforation, bleeding, or/and hospitalization [9].
Stricturotomy
Stricturotomy using a needle-knife has been described in the management of anal and small bowel strictures [2]. In a cohort of 85 patients, needle-knife stricturotomy led to passage of the scope in all patients immediately after treatment [12]. However, 60.6% of patients required additional endoscopic stricture therapy (dilation or stricturotomy) during follow-up. Although stricturotomy appears promising, additional efficacy and safety data are needed to better understand long-term outcomes.
Stent Placement
Stents have been used in the management of CD-associated strictures [2, 13]. However, stent placement can be complicated by perforation or stent migration and is consequently not recommended in the routine treatment of strictures, pending further data on its efficacy and safety in this setting. Emerging data on removable temporary or biodegradable stents are promising [2].
Intralesional Injection
Injection of corticosteroids or infliximab into a stricture has been described but has shown controversial data. In a recent systematic review, intralesional injection was not found to be beneficial and is therefore not recommended [14].
Dysplasia Diagnosis and Management
Endoscopy plays a crucial role in the evaluation and management of IBD-associated dysplasia.
The incidence of colorectal neoplasia in patients with IBD is estimated to be 60% higher than in the general population and increases over the disease course [15]. The risk of colorectal cancer (CRC) is estimated at 2%, 8%, and 18% at 10, 20, and 30 years of disease, respectively [16].
In addition to disease duration, several other factors are associated with an increased risk of IBD-associated neoplasia [17] and are listed in Fig. 13.1.

Risk factors for IBD-associated neoplasia [17]; CD Crohn’s disease, PSC primary sclerosing cholangitis, UC ulcerative colitis
Society guidelines recommend initiating colorectal neoplasia surveillance 8 years after diagnosis in patients with UC with extent greater than the rectum and in CD patients with at least 30% of colon involvement [18, 19]. Surveillance in patients with concurrent primary sclerosing cholangitis (PSC) should be performed at the time of PSC diagnosis and annually thereafter [18].
Diagnosing IBD-Associated Dysplasia
Different modalities and techniques are available for CRC surveillance and are summarized in Table 13.1. In order to optimize dysplasia detection, a good bowel preparation and minimal mucosal inflammation on endoscopy are important, regardless of the modality used for surveillance [20].
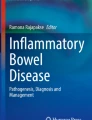
Dye spray chromoendoscopy (DCE) involves the application of dye (generally methylene blue or indigo carmine) during colonoscopy to enhance visualization of the mucosa and improve dysplasia detection [21]. On the other hand, virtual chromoendoscopy (VCE) uses image-enhancement technology to improve mucosal visualization Fig. 13.2. White light endoscopy is used as well, supplemented with 4-quadrant biopsies every 10 cm in order to sample for possible invisible dysplasia particularly in the setting of standard-definition endoscopy [22].

Virtual chromoendoscopy in a patient with Crohn’s disease undergoing colon cancer surveillance. (a), colon mucosa visualized using high-definition white light; (b), colon mucosa visualized using narrow-band imaging; (c), polyp visualized using high-definition white light; (d), polyp visualized using narrow-band imaging. Courtesy Dr. Ammar Kheir
Although both high-definition white light endoscopy (HDWLE) and chromoendoscopy have been shown to be superior to standard-definition white light endoscopy (SDWLE) in the diagnosis of dysplasia [20], it is still unclear how HDWLE compares to chromoendoscopy. Although the SCENIC consensus statements recommended dye spray chromoendoscopy over white light endoscopy (particularly if only standard-definition endoscopy is available) in 2015 [22], several practice-changing studies have been published since. Meta-analyses of prior observational studies indeed show a superiority of chromoendoscopy in the detection of dysplasia over SDWLE and HDWLE, but this does not hold true for HDWLE in randomized controlled trials (RCTs) [23]. In two recent RCTs, VCE [24] and HDWLE [24, 25] were not inferior to dye spray chromoendoscopy.
Current ACG guidelines recommend dye spray chromoendoscopy, particularly if standard-definition endoscopy is used. In the setting of high-definition endoscopy, either DCE or VCE with narrow-band imaging (NBI) can be used.
Our approach to dysplasia screening is however likely to evolve over the next few years as we gather additional data on the current techniques and as more modalities possibly become available, such as artificial intelligence-based detection methods [26].
Endoscopic Management of IBD-Associated Dysplasia
The first step in managing IBD-associated dysplasia is determining whether it is resectable endoscopically. According to the SCENIC consensus statements, an endoscopically resectable lesion should have the following features: (1) distinct margins (2) complete removal on visual inspection after resection (3) complete removal on histology (4) dysplasia-free biopsies from the adjacent mucosa [22]. There should not be concurrent multifocal or high-grade dysplasia. Resection of these lesions should be undertaken by endoscopists skilled to perform such techniques.
Several techniques can be used and are summarized in Table 13.1. Endoscopic mucosal resection (EMR) is the most common method and generally involves the use of lifting the lesion. However, for lesions larger than 2 cm, piecemeal resection is required. Lifting can also be challenging in the setting of submucosal fibrosis. Endoscopic submucosal dissection can allow the lesion to be resected en bloc and circumvents the need for lifting. However, ESD is not easily accessible and many centers may lack the adequate expertise [21]. Hybrid ESD has also been described, in which a lesion is resected using a snare after limited submucosal dissection [21].
Tattooing the lesion after resection is recommended in addition to sampling the mucosa adjacent to the resected lesion for dysplasia [22].
However, it is important to emphasize that patients with IBD-associated dysplasia should ideally be discussed in a multidisciplinary team approach to discuss endoscopic or surgical options in order to determine the optimal management [27].
Other Therapeutic Endoscopic Procedures
In addition to its important role in strictures and dysplasia management, endoscopy has also been used in the treatment of fistulas, post-operative complications or in the management of complex pouch disorders.
Management of IBD Post-Operative Complications
Endoscopic treatment of various post-operative acute and chronic complications such as anastomotic strictures, leaks, or sinuses has been described [2]. Several techniques have been reported in the endoscopic management of anastomotic leaks, including clips, suturing, or stent placement [2]. In addition, several endoscopic modalities have been used in the management of J-pouch complications, such as closure of “tip of the J” leaks using over-the-scope clips in a case series of 12 patients [28]. In addition, endoscopic management of chronic presacral sinuses using needle-knife sinusotomy has been described [29, 30].
Fistulas
Endoscopy has been used in the treatment of fistulas. In a case series of 29 patients with fistulas in a variety of locations (including perianal, pouch-pouch, and entero-enteric fistulas), successful endoscopic fistulotomy using a needle-knife was reported in 89.6% of patients [31]. Endoscopic closure of fistulas has also been described using over-the-scope clips [32]. Although promising, further safety and long-term efficacy data are needed before these techniques can be used in routine clinical practice.
Conclusion
In recent years, the role of endoscopy has expanded to include a variety of non-invasive techniques to address gaps in IBD care. In addition to its important function in the management of strictures and dysplasia, recent advances in endoscopy have allowed alternative options in the management of disease or surgical complications such as fistulas, leaks, and sinuses. As endoscopic technologies continue to develop, such as through additional and artificial intelligence-based detection methods, IBD care is likely to evolve, with endoscopy gradually filling important gaps in IBD management.
Abbreviations
- CRC:
-
Colorectal cancer
- CD:
-
Crohn’s disease
- DCE:
-
Dye spray chromoendoscopy
- EBD:
-
Endoscopic balloon dilation
- HDWLE:
-
High-definition white light endoscopy
- IBD:
-
Inflammatory bowel disease
- PSC:
-
Primary sclerosing cholangitis
- RCT:
-
Randomized controlled trial
- SDWLE:
-
Standard-definition white light endoscopy
- UC:
-
Ulcerative colitis
- VCE:
-
Virtual chromoendoscopy
References
Windsor JW, Kaplan GG. Evolving epidemiology of IBD. Curr Gastroenterol Rep. 2019;21(8):40.
Shen B, Kochhar G, Navaneethan U, Liu X, Farraye FA, Gonzalez-Lama Y, et al. Role of interventional inflammatory bowel disease in the era of biologic therapy: a position statement from the global interventional IBD group. Gastrointest Endosc. 2019;89(2):215–37.
Pineton de Chambrun G, Peyrin-Biroulet L, Lémann M, Colombel J-F. Clinical implications of mucosal healing for the management of IBD. Nature reviews. Gastroenterol Hepatol. 2010;7(1):15–29.
Sleiman J, El Ouali S, Qazi T, Cohen B, Steele SR, Baker ME, et al. Prevention and treatment of Stricturing Crohn’s disease—perspectives and challenges. Expert Rev Gastroenterol Hepatol. 2021;15(4):401–11.
Rieder F, Fiocchi C, Rogler G. Mechanisms, management, and treatment of fibrosis in patients with inflammatory bowel diseases. Gastroenterology. 2017;152(2):340–50 e6.
Fumery M, Pineton de Chambrun G, Stefanescu C, Buisson A, Bressenot A, Beaugerie L, et al. Detection of dysplasia or cancer in 3.5% of patients with inflammatory bowel disease and colonic strictures. Clin Gastroenterol Hepatol. 2015;13(10):1770–5.
Lovasz BD, Lakatos L, Golovics PA, David G, Pandur T, Erdelyi Z, et al. Risk of colorectal cancer in Crohn’s disease patients with colonic involvement and stenosing disease in a population-based cohort from Hungary. J Gastrointestin Liver Dis. 2013;22(3):265–8.
El Ouali S, Click B, Holubar SD, Rieder F. Natural history, diagnosis and treatment approach to fibrostenosing Crohn’s disease. United European Gastroenterol J. 2020;8(3):263–70.
Bettenworth D, Gustavsson A, Atreja A, Lopez R, Tysk C, van Assche G, et al. A pooled analysis of efficacy, safety, and Long-term outcome of endoscopic balloon dilation therapy for patients with Stricturing Crohn’s disease. Inflamm Bowel Dis. 2017;23(1):133–42.
Rieder F, Latella G, Magro F, Yuksel ES, Higgins PD, Di Sabatino A, et al. European Crohn’s and colitis organisation topical review on prediction, diagnosis and management of fibrostenosing Crohn’s disease. J Crohns Colitis. 2016;10(8):873–85.
Bettenworth D, Bokemeyer A, Kou L, Lopez R, Bena JF, El Ouali S, et al. Systematic review with meta-analysis: efficacy of balloon-assisted enteroscopy for dilation of small bowel Crohn’s disease strictures. Aliment Pharmacol Ther. 2020;52(7):1104–16.
Lan N, Shen B. Endoscopic Stricturotomy with needle knife in the treatment of strictures from inflammatory bowel disease. Inflamm Bowel Dis. 2017;23(4):502–13.
El Ouali S, Kessler H, Shen B. Self-expandable metal stent in the treatment of refractory long pouch inlet stricture. Inflamm Bowel Dis. 2019;25(3):e13–e4.
Lu C, Baraty B, Lee Robertson H, Filyk A, Shen H, Fung T, et al. Systematic review: medical therapy for fibrostenosing Crohn’s disease. Aliment Pharmacol Ther. 2020;51(12):1233–46.
Herrinton LJ, Liu L, Levin TR, Allison JE, Lewis JD, Velayos F. Incidence and mortality of colorectal adenocarcinoma in persons with inflammatory bowel disease from 1998 to 2010. Gastroenterology. 2012;143(2):382–9.
Eaden JA, Abrams KR, Mayberry JF. The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut. 2001;48(4):526–35.
Wijnands AM, de Jong ME, Lutgens MWMD, Hoentjen F, Elias SG, Oldenburg B. Prognostic factors for advanced colorectal neoplasia in inflammatory bowel disease: systematic review and meta-analysis. Gastroenterology. 2021;160(5):1584–98.
Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD. ACG clinical guideline: ulcerative colitis in adults. Am J Gastroenterol |ACG. 2019;114(3):384–413.
Lichtenstein GR, Loftus EV, Isaacs KL, Regueiro MD, Gerson LB, Sands BE. ACG clinical guideline: management of Crohn’s disease in adults. Am. J. Gastroenterol.|ACG. 2018;113(4):481–517.
Núñez P, Cleveland NK, Quera R, Rubin DT. Evolving role of endoscopy in inflammatory bowel disease: going beyond diagnosis. World J Gastroenterol. 2021;27(20):2521.
Soetikno R, East J, Suzuki N, Uedo N, Matsumoto T, Watanabe K, et al. Endoscopic submucosal dissection for nonpolypoid colorectal dysplasia in patients with inflammatory bowel disease: in medias res. Gastrointest Endosc. 2018;87(4):1085–94.
Laine L, Kaltenbach T, Barkun A, McQuaid KR, Subramanian V, Soetikno R. SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease. Gastroenterology. 2015;148(3):639–51.e28.
Feuerstein JD, Rakowsky S, Sattler L, Yadav A, Foromera J, Grossberg L, et al. Meta-analysis of dye-based chromoendoscopy compared with standard- and high-definition white light endoscopy in patients with inflammatory bowel disease at increased risk of colon cancer. Gastrointest Endosc. 2019;90(2):186–95.e1.
Yang DH, Park SJ, Kim HS, Park YS, Park DI, Lee KM, et al. High-definition chromoendoscopy versus high-definition white light colonoscopy for neoplasia surveillance in ulcerative colitis: a randomized controlled trial. Am J Gastroenterol. 2019;114(10):1642–8.
Iacucci M, Kaplan GG, Panaccione R, Akinola O, Lethebe BC, Lowerison M, et al. A randomized trial comparing high definition colonoscopy alone with high definition dye spraying and electronic virtual chromoendoscopy for detection of colonic neoplastic lesions during IBD surveillance colonoscopy. Am J Gastroenterol | ACG. 2018;113(2):225–34.
Maeda Y, Kudo S-E, Ogata N, Misawa M, Mori Y, Mori K, et al. Can artificial intelligence help to detect dysplasia in patients with ulcerative colitis? Endoscopy. 2020;53(07):E273–4.
Axelrad JE, Shah SC. Diagnosis and management of inflammatory bowel disease-associated neoplasia: considerations in the modern era. Ther Adv Gastroenterol. 2020;13:1756284820920779.
Kochhar GS, Shen B. Endoscopic treatment of leak at the tip of the “J” ileal pouch. Endosc Int Open. 2017;5(1):E64–e6.
El Ouali S, Veniero JC, Shen B. Computed tomography-guided endoscopic sinusotomy for an ileal pouch presacral sinus. Endoscopy. 2018;50(7):730–1.
Lan N, Hull TL, Shen B. Endoscopic sinusotomy versus redo surgery for the treatment of chronic pouch anastomotic sinus in ulcerative colitis patients. Gastrointest Endosc. 2019;89(1):144–56.
Kochhar G, Shen B. Endoscopic fistulotomy in inflammatory bowel disease (with video). Gastrointest Endosc. 2018;88(1):87–94.
Haito-Chavez Y, Law JK, Kratt T, Arezzo A, Verra M, Morino M, et al. International multicenter experience with an over-the-scope clipping device for endoscopic management of GI defects (with video). Gastrointest Endosc. 2014;80(4):610–22.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Ethics declarations
FR is a consultant to or on the advisory board of Adnovate, Agomab, Allergan, AbbVie, Arena, Boehringer-Ingelheim, Celgene/BMS, CDISC, Cowen, Galmed, Genentech, Gilead, Gossamer, Guidepoint, Helmsley, Index Pharma, Jannsen, Koutif, Mestag, Metacrine, Morphic, Organovo, Origo, Pfizer, Pliant, Prometheus Biosciences, Receptos, RedX, Roche, Samsung, Surmodics, Surrozen, Takeda, Techlab, Theravance, Thetis, UCB, Ysios, 89Bio.
Rights and permissions
Copyright information
© 2023 SAGES
About this chapter

Cite this chapter
El Ouali, S., Rieder, F. (2023). Interventional Procedures for Inflammatory Bowel Disease. In: Kroh, M., Docimo Jr., S., El Djouzi, S., Shada, A., Reavis, K.M. (eds) The SAGES Manual Operating Through the Endoscope. Springer, Cham. https://doi.org/10.1007/978-3-031-21044-0_13
Download citation
DOI: https://doi.org/10.1007/978-3-031-21044-0_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-21043-3
Online ISBN: 978-3-031-21044-0
eBook Packages: MedicineMedicine (R0)