
Abstract
Third mobile window syndrome (TMWS) (also known as third window syndrome [TWS] or otic capsule dehiscence syndrome [OCDS]) is a vestibular-cochlear disorder in humans in which a third mobile window of the inner ear creates changes to the flow of sound pressure level energy through the perilymph/endolymph. Sound transmission to the inner ear is normally through the oval and round window. Acoustic pressure enters through the oval window, is transmitted through the cochlea, and exits into the middle ear cavity via the round window [1]. The fluid in the cochlea through which sound is transmitted is functionally incompressible due to the surrounding osseous structures [2]. Movement of the cochlear fluid is thereby dependent on the mobility of the round and oval window membranes. Inward displacement of the oval window membrane via the stapes by ossicular vibration is matched by outward round window membrane displacement [2]. However, if a third mobile window is present, some of the acoustic pressure is shunted away from the cochlea and delivered to the vestibular receptors. Normally, sound pressure transduction by the stapes results in only cochlear hair cell transduction due to the round window, which dissipates cochlear vibration by impedance matching. Normally, because the vestibular labyrinth does not have a membrane or release valve to dissipate the introduced sound pressure, their pressure remains constant and the vestibular end-organs are not stimulated. However, if there is an additional fenestration, the energy typically confined to the vestibule and cochlea escapes along a path of least resistance toward the defect or “third window” and during this the vestibular end-organs can be abnormally stimulated. The nature and location of this third mobile window can occur at many different sites (or multiple sites), which will be discussed later. The primary physiological symptoms include sound-induced and pressure-induced gravitational receptor dysfunction type of vertigo, migraine headaches (and variants), pseudoconductive hearing loss, autophony while speaking, and visual problems (nystagmus, oscillopsia). At the same time, individuals experience measurable deficits in basic decision-making, short-term memory, concentration, spatial cognition, and anxiety. In this chapter, the history of TMWS will be reviewed, but first a description of the clinical phenotype is essential to understand the spectrum of problems these patients experience.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Autophony
- Cognitive dysfunction
- Dizziness
- Depression
- Otic capsule dehiscence
- Perilymph fistula
- Superior semicircular canal dehiscence
- Third window syndrome
- Vestibular
Third mobile window syndrome (TMWS) (also known as third window syndrome [TWS] or otic capsule dehiscence syndrome [OCDS]) is a vestibular-cochlear disorder in humans in which a third mobile window of the inner ear creates changes to the flow of sound pressure level energy through the perilymph/endolymph. Sound transmission to the inner ear is normally through the oval and round window. Acoustic pressure enters through the oval window, is transmitted through the cochlea, and exits into the middle ear cavity via the round window [1]. The fluid in the cochlea through which sound is transmitted is functionally incompressible due to the surrounding osseous structures [2]. Movement of the cochlear fluid is thereby dependent on the mobility of the round and oval window membranes. Inward displacement of the oval window membrane via the stapes by ossicular vibration is matched by outward round window membrane displacement [2]. However, if a third mobile window is present, some of the acoustic pressure is shunted away from the cochlea and delivered to the vestibular receptors. Normally, sound pressure transduction by the stapes results in only cochlear hair cell transduction due to the round window, which dissipates cochlear vibration by impedance matching. Normally, because the vestibular labyrinth does not have a membrane or release valve to dissipate the introduced sound pressure, their pressure remains constant and the vestibular end-organs are not stimulated. However, if there is an additional fenestration, the energy typically confined to the vestibule and cochlea escapes along a path of least resistance toward the defect or “third window” and during this the vestibular end-organs can be abnormally stimulated. The nature and location of this third mobile window can occur at many different sites (or multiple sites), which will be discussed later. The primary physiological symptoms include sound-induced and pressure-induced gravitational receptor dysfunction type of vertigo, migraine headaches (and variants), pseudoconductive hearing loss, autophony while speaking, and visual problems (nystagmus, oscillopsia). At the same time, individuals experience measurable deficits in basic decision-making, short-term memory, concentration, spatial cognition, and anxiety. In this chapter, the history of TMWS will be reviewed, but first a description of the clinical phenotype is essential to understand the spectrum of problems these patients experience.
Clinical Phenotype
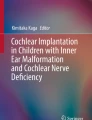
The literature has been conflicted about the frequency of symptoms and diagnostic test findings in patients with TMWS. One illustrative summary that highlights the spectrum of the most common complaints from patients with perilymph fistula was published nearly a quarter century ago [3]. No doubt many of these patients had TMWS due to bony sites of dehiscence not yet discovered. Figure 1.1 shows the percentage of these patients reporting each of the 13 most common complaints. The three most frequent complaints were disequilibrium, headache, and dizziness. Other important clinical symptoms included cognitive dysfunction, nausea, visual disturbance, and objective as well as subjective hearing loss. Review of Fig. 1.1 also demonstrates that these are extraordinarily similar to the spectrum of symptoms experienced by patients with SSCD, other TMWS sites of dehiscence and vestibular migraine. Table 1.1 outlines the contemporary spectrum of symptoms, signs or exacerbating factors seen in TMWS. It is important to understand that every patient with TMWS does not have all of the observed symptoms and that TMWS should be viewed as a spectrum of symptoms. Table 1.2 combines synonymous symptoms into common terms so that the reader can see a simplified framework illustrating these symptoms. As shown in Table 1.3 there are currently 15 known sites of dehiscence that can be seen using high-resolution temporal bone CT and in addition there are sites of dehiscence that cannot yet be seen with contemporary high-resolution temporal bone CT scans (CT– TMWS).

Clinical phenotype of perilymph fistula (PLF). Percentage of 58 PLF patients reporting each of the most common complaints (created from the dataset of Black et al. [3]) Copyright © P.A. Wackym, used with permission
The more general term of TMWS is more appropriate than SSCD syndrome because the same spectrum of symptoms, signs on physical examination, and audiological diagnostic findings are encountered with superior semicircular canal dehiscence (SSCD), posterior semicircular canal dehiscence, posterior semicircular canal-jugular bulb dehiscence, posterior semicircular canal-endolymphatic sac/vestibular aqueduct dehiscence, lateral semicircular canal dehiscence, lateral semicircular canal-facial nerve dehiscence, cochlea-facial nerve dehiscence (CFD), cochlea-internal carotid artery dehiscence, cochlea-internal auditory canal dehiscence, cochlear otosclerosis with internal auditory canal involvement, wide vestibular aqueduct, endolymphatic sac-jugular bulb dehiscence, posttraumatic hypermobile stapes footplate, vestibule-middle ear dehiscence, modiolus (X-linked stapes gusher), and CT– TWS (see review [4]). A common structural finding in all of these conditions is an otic capsule defect that creates a “third window.” In the light of our recognition that there are multiple sites where third windows occur in the otic capsule, it is interesting to note that Kohut’s definition of a PLF, from over a quarter century ago, still applies to all currently known sites producing a TWS [6]; “A perilymph fistula may be defined as an abnormal opening between the inner ear and the external surface of the labyrinth capsule….” Hence, a fistula of the otic capsule (Kohut’s definition) can occur in any location that is in communication with perilymph, whether a SSCD, CFD, or any of the well-established sites that can result in a TMWS.
Peripheral Vestibular Physiology and the Need for a Precise Lexicon
A central problem with understanding peripheral vestibular disorders or communicating associated symptoms is our use of poor, or at least imprecise, terminology. The terms vertigo, dizziness, and disequilibrium are frequently used; however, what do they mean? To best answer this question a brief review of peripheral vestibular function is necessary.
The role of the ten vestibular receptors is to transduce the forces associated with head acceleration and gravity into a biologic signal. Central nervous system integration of these data results in the subjective awareness of head position relative to the environment. Motor reflexes to maintain gaze and posture are generated in response to afferent vestibular input. Propulsion and orientation of the body in space depend on the vestibular system, on vision, and on the proprioceptive system. Most persons can manage with only two of these systems, but not with one. Accordingly, patients with vestibular dysfunction may have additional difficulty in maintaining equilibrium when vision or proprioception is impaired.
The vestibular system, through its signal transduction by the peripheral end-organs and their afferent neurotransmission, constantly signals the position of the head in space and effects a continuous adjustment of the musculature of the body. More specifically, it signals acceleration and deceleration of motion. The otolith organs are capable of signaling only linear acceleration or deceleration, whereas the cristae within the semicircular ducts are able to signal angular acceleration or deceleration. Constant motion/acceleration cannot be detected by the vestibular system.
The peripheral vestibular system represents a unique neurosensory system. At rest, the type I and type II vestibular hair cells and their primary afferent neurons have a relatively constant and symmetrical resting discharge rate of approximately 80 spikes/s. This discharge rate increases if the stereocilia are deflected toward the kinocilium of each type I or type II vestibular hair cell, and it decreases if they are deflected away from the kinocilium. Transduction of accelerated motion is brought about by movement of the endolymph, which is coupled to the stereocilia and kinocilia of the neuroepithelium. All the kinocilia are oriented in the same direction relative to the long axis of each crista, and flow of endolymph in one direction results in the same discharge characteristics for all the hair cells in each individual end-organ. A further level of redundancy exists in the push–pull organization between both sets of vestibular apparatus. For example, with rotation to the right in the horizontal plane, there is relative flow of endolymph to the left. The resting discharge rate from the right horizontal crista ampullaris is greatly increased as the cupula is deflected toward the vestibule (i.e., ampullipetal displacement), whereas the discharge rate from the left side decreases an equal amount as the cupula of the left horizontal crista ampullaris is deflected away from the vestibule (i.e., ampullifugal displacement). Normally, this bilateral system is constantly at work, receiving signals and passing them on to regulate posture and movement of the body, limbs, and eyes. Each of the five vestibular receptors on the left are paired with a specific receptor on the right. Under normal circumstances, the vestibular signals produced by each side are equal and opposite in magnitude bilaterally. The paired otolithic organs function by similar mechanisms, except that type I and type II vestibular hair cells are coupled to gravitational force through the otolithic membrane, and their overlying otoconia and the kinocilia are polarized relative to a region called the striola. Consequently, conscious perception of this normal vestibular activity does not occur. However, if there is an imbalance in the relative increase and decrease in afferent firing between paired vestibular receptors on both sides, patients experience vertigo.
Vertigo is an illusion of movement in any plane or direction. Patients are deceived so that they feel themselves move or see abnormal movement of their surroundings. For rotational receptor asymmetries, patients experience a true rotational or spinning movement. For gravitational receptor asymmetries, patients have a gravitational receptor dysfunction type of vertigo. They will often describe a “rocky, wavy, tilting” perception. Other descriptors include a sensation as “being on a moving boat, the floor falling out from under them or flipping.” The terms dizziness, giddiness or disequilibrium do not accurately capture these experiences, yet they are often used, which leads to a poor understanding of TMWS otic capsule defect (e.g., SSCD) symptoms by most physicians. Patients with TMWS sites can experience true rotational vertigo; however, the dominant complaint is usually sound-induced gravitational receptor dysfunction type of vertigo. This clinical observation can be blurred by vestibular migraine with true rotational vertigo being superimposed on SSCD, CFD or other TMWS site of dehiscence. This will be discussed in greater detail in Chap. 25, “Migraine, Headache and Third Mobile Window Syndrome.”
Autonomic Dysfunction
Autonomic dysfunction occurs to varying degrees with TMWS and/or vestibular migraine; however, it is extremely common. Autonomic dysfunction also occurs with rotational receptor asymmetries. These symptoms include nausea, “cold-clammy skin,” decreased heart rate and vomiting. There have been many investigators who have studied the underlying mechanisms and pathways subserving this dysfunction [21,22,23].
Cognitive Dysfunction
Cognitive dysfunction is nearly universal in patients with TMWS due to the otolithic asymmetry. This is uncommon in rotational receptor dysfunction type of vertigo as seen with benign positional vertigo, vestibular neuronitis or other disorders producing true rotational vertigo. Patients with TMWS often use the following descriptors when describing their cognitive function: “fuzzy, foggy, spacey, out-of-it; memory and concentration are poor; difficulty reading—as if the words are floating on the page; trouble finding the right words; and forgetting what I wanted to say.” This will be discussed in greater detail in Chap. 6, “The Cognitive/Psychological Effects of Third Mobile Window Syndrome.”
Altered Spatial Orientation
Patients with TMWS and/or vestibular migraine often use the following descriptors when describing their altered spatial orientation: “trouble judging distances; feeling detached and separated or not connected, almost like watching a play when around other people; and even an out-of-body experience (in more severe gravitational receptor asymmetries).” Several groups have begun studying this phenomenon. Clinically, this spatial disorientation reverses after surgery; however, Baek and colleagues reported that spatial memory deficits following bilateral vestibular loss may be permanent [24]. There is also evidence that simulation of the vestibular system is necessary to maintain normal spatial memory [25]. Deroualle and Lopez have explored the visual-vestibular interaction and in their 2014 review of the topic conclude that vestibular signals may be involved in the sensory bases of self-other distinction and mirroring, emotion perception and perspective taking [26]. Clinically, patients with TMWS recognize changes in their personality. Smith and Darlington argue that these changes in cognitive and emotional occur because of the role the ascending vestibular pathways to the limbic system and neocortex play in the sense of spatial orientation [27]. They further suggest that this change in the sense of self is responsible for the depersonalization and derealization symptoms such as feeling “spaced out,” “body feeling strange,” and “not feeling in control of self.”
Anxiety
Vestibular disorders can produce anxiety; however, the classic sense of impending doom only occurs with the most severe gravitational receptor asymmetries. It is none-the-less quite unnerving to patients because it is a unique type of anxiety and characteristically patients have no insight why they feel that way or what is making them feel that way. Much work has been completed to understand the underlying mechanisms and pathways subserving this dysfunction [18,19,20,21,22,23, 28, 29].
Sound-Induced Gravitational Receptor Dysfunction Type of Vertigo
In Minor’s review of 65 patients with SSCD, 54 (83%) had vestibular symptoms elicited by loud sounds, and 44 (67%) had pressure-induced (sneezing, coughing, and straining) symptoms [30]. This is also characteristic of TMWS patients with other sites of dehiscence (Tables 1.1 and 1.2) [8,9,10,11,12,13,14,15,16,17].
Autophony
In TMWS one of the most disturbing auditory symptoms is autophony, an unpleasant subjective discomfort of one’s own voice during phonation. Often patients describe their voice as “echo-like” or “resonant.” This is also very common in TMWS. Just as in the case with SSCD [31], some patients with other sites of dehiscence can also hear their eyes move or blink [8,9,10]. There appears to be decreased hearing thresholds for bone-conducted sounds. Bhutta has postulated that patients who hear their eyes move do so via transdural transmission of extraocular muscle contraction [32]. If this is the case, further credence to the hypothesis that some cases of CT– TMWS represent an otic capsule defect in an area such as the modiolus creating a third window, just as is the case with SSCD and CFD [4, 18, 19].
Migraine and Gravitational Receptor Dysfunction Type of Vertigo
Migraine headache is nearly always present in patients with gravitational receptor dysfunction type of vertigo caused by a TMWS, but infrequently with rotational receptor dysfunction type of true rotational vertigo [4, 19,20,21]. This is an important concept as TMWS can induce or exacerbate migraine and the three variants of migraine—ocular migraine, hemiplegic migraine, and vestibular migraine in affected patients. This is why patients with TMWS, who normally only have gravitational receptor dysfunction type of vertigo (disequilibrium) can have episodes of vestibular migraine and infrequent true rotational vertigo attacks. Surgical management, based upon the procedure specific to the site of dehiscence typically resolves the migraine; however, sometimes there is a marked decrease of the frequency and intensity of the migraines, as migraine has a high incidence overall [4, 8,9,10,11,12,13,14,15,16,17,18,19,20]. This will be discussed in greater detail in Chap. 25, “Migraine, Headache and Third Mobile Window Syndrome.”
The Experiments of Pietro Tullio
Pietro Tullio (1881–1941) was the director of the Laboratory of Experimental Physiology in Bologna during the early twentieth century. While other scientists of his time studying the nervous system preferred removing or lesioning a structure to deducing the singular function from the singular deficiency, Tullio preferred the direct stimulation of these parts to deduce function. He undertook most of his experiments on live pigeons. Pigeons had already been established as the classical test animal for labyrinth physiology because of their favorable semicircular canal anatomy. It was also well documented that head nystagmus was more prominent than ocular nystagmus in the pigeon, making observations of responses easier [33].
In 1929, Tullio presented “Some Experiments and Considerations on Experimental Otology and Phonetics” at the meeting of the Società dei Cultori delle Scienze Mediche e Naturali in 1929 [34]. These experiments described the eponymous Tullio phenomenon of sound-induced vertigo and/or eye movements. This work was nominated for the Nobel Prize in Physiology or Medicine in both 1930 and 1932; however, he was never awarded the prize. The body of this work was focused on surgically creating a third window in the semicircular canals of pigeons [35, 36]. Tullio hypothesized that the sound pressure reaching the ear affects all three canals at the same time, not just the opened canal. The difference in intensity in which the currents are distributed in the canals produces the head movement. By making an opening in a canal, its current of sound pressure would be dominant over the other canals, leading to visible movement in the plane of this canal. Tullio subsequently analyzed the movement made by pigeons on opening each canal. After the opening of the superior canal, the pigeon lifted its head and beak in the plane of the canal. With a single sound, the lifting and tilting of the head was about 45°; the extension of the movement attained 90° when the sound was prolonged. What he did not address was the otolithic function which is no doubt responsible for the head tilt visible in the figures that he published. When cocaine crystals were introduced into the osseous opening near the ampulla, so that the anesthetic reached the perilymph, the pigeon lifted its beak at every sound to successively decreasing heights, until it finally lowered. This phenomenon is due to the cocaine paralyzing the primary afferent dendrites of the ampulla in the superior semicircular canal, and likely the vestibule, so that the pigeon could no longer respond to this acoustic stimulation. The pigeon was still responsive to the currents in the lateral and posterior canals. This had a cumulative effect wherein the pigeon lowered its head in an intermediate plane to those canals. In a clever experimental design, Tullio attached a lever and marker to the pigeon’s beak to provide a graphical plot of the reflexes made in response to the sound pressure stimulus. It was decades later that these basic experiments in pigeons were recognized to represent a clinical entity now known as TMWS. According to Cawthorne [37], the Tullio phenomenon only occurred in humans when more than one mobile window opened into the inner ear on the vestibular side of the inner ear.
Semicircular Canal Fenestration Operations for Otosclerosis
Antonio Maria Valsalva first described stapes ankylosis as a cause of hearing loss in 1704. Adam Politzer described the pathology as due to “new bone, overgrowing the oval window and stapes” in 1893. This corresponded with the first era of stapes surgery, which consisted of stapes mobilization, trephination, or removal. As these procedures became more common in Europe, complications of meningitis and death were recognized and led to the abandonment of the procedures around 1900 [37]. Following this, otologists continued to investigate alternative, safer methods of surgically correcting the conductive hearing loss from otosclerosis. Beginning in 1897, when Passow first postulated that perhaps it would be better to detour around the obstruction in the oval window rather than to mobilize or extract the stapes. Balance, Floderus, Bárány, Holmgren, Jenkins and Sourdille all contributed to refinement of multistage fenestration operations to create a new mobile window in the lateral semicircular canal. In 1938, Julius Lempert described a breakthrough single-stage technique creating a new mobile window that he termed “nov-ovalis” in the lateral semicircular canal fenestration via an endaural approach. About 50% of patients who had this procedure had improvement of their conductive hearing loss to a 20–25 dB air-bone gap with lasting results. This marked the rise of the fenestration era of otosclerosis surgery [38,39,40]. Shambaugh reviewed the postoperative problems that these fenestration patients experienced: wet fenestrated ear; meatal atresia; ballooning of the fenestra; closure of the fenestra; sensorineural hearing loss after fenestration; and progressive sensorineural hearing loss due to otospongiosis [39]. Interestingly, these patients, although susceptible to temperature-induced dizziness typically did not experience sound-induced dizziness. This is likely due to the fenestration operation recreating a second mobile window, as the oval window was not mobile. Cawthorne described the Tullio phenomenon in patients who had undergone fenestration procedures for otosclerosis in which the stapes was not fixed, creating a “third window” in the inner ear, which underscores this point [41].
Cholesteatoma
Labyrinthine fistulas creating a TMW constitute around 4–12% of complications due to cholesteatoma. In a large meta-analysis, the affected site of the labyrinthine fistula was lateral semicircular canal dehiscence in 87% of cases, promontory dehiscence in 8% of cases, SSCD in 6% of cases, and posterior semicircular canal dehiscence in 2% of cases [42]. Historically, management has been to leave the cholesteatoma matrix intact over the fistula; however, this results in frequent temperature and pressure related stimulation of inhibition of the affected side. More recently, removal of the entire cholesteatoma matrix from the fistula with immediate covering by autogenous material or after removal plugging the canal with autologous tissue [43]. Other authors have advocated the use of hydrodissection of the cholesteatoma matrix in the presence of labyrinthine fistula as a means of hearing preservation [44].
Early Stapedectomy Lessons Learned
Iatrogenic post-stapedectomy perilymph fistulas were first described a half-century ago. Steffen et al. [45] reported findings of gross perilymph flow at the oval window in post-stapedectomy patients with hearing loss, tinnitus, and vertigo. Fee [46] reported three patients who presented with vertigo, fluctuating hearing loss, and tinnitus, who also had known or suspected recent head trauma. Intraoperative findings showed perilymph leak at the oval window. Repair of the leak resulted in significant improvement in symptoms.
Vestibular Evoked Myogenic Potentials
It was over a century ago that Robert Bárány began using caloric irrigation and his vertical axis rotational chair to assess horizontal canal function, yet it was not until 1994 that Colebatch and colleagues developed the sound-evoked cervical vestibular evoked myogenic potential (cVEMP) to study the gravitational receptors [47]. Sound-induced activation of the saccule leads to an inhibition of the sternocleidomastoid muscle and this inhibitory potential can be recorded as the cVEMP (for review see [48,49,50]). The evoked potentials recorded from a number of other muscles have been studied as well; however, it is the sternocleidomastoid muscle that is most consistently used in research and clinical applications. It has also been shown that both an ipsilateral and contralateral cVEMP can be recorded from the sternocleidomastoid muscle following ipsilateral stimulation [48, 51]. Bone-conducted stimuli have also been used to evoke cVEMP responses (for review see [49, 50]). All of these cVEMP methods depend on voluntary contraction of the sternocleidomastoid muscle so that the evoked inhibitory potential can be measured.
In patients with SSCD and other sites of dehiscence resulting in third window syndrome, cVEMPs are useful diagnostic indicators, with patients exhibiting abnormal responses to auditory clicks or tone bursts used in this test [4, 18,19,20, 52, 53]. The cVEMP amplitudes in the affected labyrinth are increased, and thresholds are reduced as the opening in the superior semicircular canal renders otolithic receptors more susceptible to stimulation by sound and vibration [4, 18,19,20, 30, 54,55,56]. The same cVEMP increased amplitude and decreased threshold has been reported in many other locations creating a TMWS including CT– TMWS and CFD [4, 18,19,20]. After surgical plugging of the SSCD, cVEMP thresholds and amplitudes normalize [56].
The ocular vestibular evoked myogenic potential (oVEMP) testing represents another diagnostic tool that can be important in the diagnosis of patients with TMWS. These potentials are excitatory and are recorded from surface electrodes over the inferior oblique muscles. Many have contributed to understanding the oVEMP response, particularly Ian Curthoys’ group [49]. Both acoustic and bone-conduction stimuli activate the saccular and utricular otolithic receptors; however, the otolithic input to the sternocleidomastoid muscle is predominately from the saccular macula whereas the otolithic input to the inferior oblique muscle is predominately from the utricular macula [48,49,50]. Thus, quantitatively, cVEMP tests saccular function while oVEMP tests utricular function. Another practical extension of these relationships is that the cVEMP reflects inferior vestibular nerve function while the oVEMP reflects the superior vestibular nerve function. Clinically, the oVEMP amplitude is much smaller than the cVEMP amplitude and the response is often absent in older patients. Therefore, oVEMP thresholds are not typically measured but either a single 4 kHz or combination of 500 Hz and 4 kHz oVEMP response is measured [57]. With TMWS, the oVEMP amplitude is typically elevated [57].
Audiometry
Since TMWS patients suffer from auditory symptoms, all should undergo pure tone audiometry measuring both air-conduction and bone-conduction thresholds. If the difference between air- and unmasked bone-conduction thresholds is >10 dB, bone-conduction thresholds should be masked to accurately assess the left and right ear separately. The air-bone gap (ABG) is calculated by subtracting the bone-conduction threshold from the air-conduction threshold. Many, but not all, patients with TMWS, including SSCD, CFD CT– TMWS and many others suffer from low frequency air-bone gaps (ABG) of ≥10 dB, which can be due to low or negative bone-conduction thresholds and/or elevated air-conduction thresholds [4, 18,19,20, 54]. Obviously, ABGs are not unique to TMWS. They are a common finding in other otologic disorders causing conductive hearing loss, especially those with middle ear pathology [58]. Therefore, further evaluation of middle ear function using tympanometry and acoustic reflexes is warranted and aids in differentiating the various causes of the ABG [58, 59]. In contrast to ABG from middle ear pathology that causes abnormalities of tympanometry and/or loss of acoustic reflexes, TMWS cases with an ABG will exhibit normal tympanometry and preservation of acoustic reflexes. Therefore, the term pseudoconductive hearing loss is used in describing this ABG in TMWS patients.
High-Resolution Temporal Bone CT
The development and continued refinement of high-resolution temporal bone CT has been transformative in the identification of bony sites of TMWS. The ability to reformat the acquired data into axial, coronal, Stenvers and Pöschl planes, as well as utilization of gray-scale inversion has allowed the identification of small and unusual sites of a third mobile window resulting in TMWS [4, 60]. This will be discussed in greater detail in Chap. 12, “Imaging.”
Superior Semicircular Canal Dehiscence
While it was nearly a century ago that Tullio described the physiologic outcomes of creating a third mobile window in the semicircular canals of pigeons [33, 35, 36], it is approaching a quarter century ago that Minor et al. first described superior semicircular canal dehiscence (SSCD) in two patients [61]. However, this is not a new clinical entity as SSCD has been observed after CT imaging of Egyptian mummy heads [62].
Over the past 60 years, we have learned much regarding the clinical features, outcomes measured by validated survey instruments and neuropsychology testing as well as objective diagnostic studies in TMWS [54, 58, 59, 63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96]. Poe’s group observed that 94% of patients with SSCD, or symptoms consistent with SSCD, experienced autophony and aural fullness, while 86% were found to have pseudoconductive hearing loss [58, 75]. Interestingly, in their 2007 study, they included four cases of CT– TWS among their series of CT+ SSCD who had also had abnormally low cVEMP thresholds [58]. Because of their diagnostic dilemma, they did not manage these patients with surgical intervention. The University of Michigan group first described abnormal electrocochleography findings, usually associated with endolymphatic hydrops, in SSCD patients [96]. All four patients who were managed surgically had resolution of their abnormal ECoG findings. The Wackym group has used the Dizziness Handicap Inventory, the Headache Impact Test and comprehensive neuropsychology test batteries preoperatively and postoperatively to measure the cognitive dysfunction and migraine headache in TMWS patients to quantify their dysfunction and recovery outcomes [4, 18,19,20]. Crane et al. also reported the reduction of Dizziness Handicap Inventory scores after plugging the superior semicircular canal in patients with SSCD [92].
In addition, the Wackym group has reported a delayed development of CT– TWS after surgical plugging and resurfacing of CT+ SSCD TMWS [18,19,20]. In a series of near-SSCD patients undergoing plugging and resurfacing procedures at the Johns Hopkins Hospital, all patients noted initial improvement in at least one presenting TMWS symptom; however, five subjects (45%) reported the persistence or recurrence of at least one TMWS symptom at greater than one month after surgery [59]. In a larger series of SSCD patients, John Carey’s group reported that among 222 patients who underwent plugging procedures for SSCD, there were 21 patients who underwent 23 revision surgeries for failure to resolve their TMWS symptoms [97]. After revision surgery, TMWS symptoms were completely resolved in eight (35%), partially resolved in seven (30%), and unresolved in seven (30%) [97]. One possible explanation of these findings is that in 14 (61%) of these patients, they also had CT– TMWS. It has been suggested that the modiolus may be one site for a CT– TMWS [4, 18,19,20], and Ilmari Pyykkö’s and Dennis Poe’s demonstration that intratympanic injection of gadolinium subsequently fills the perilymphatic space in mice [98], rats [99] and then exits the inner ear via the modiolus and into the internal auditory canal supports this possibility. Manzari and Scagnelli reported a patient with bilateral SSCD and bilateral dehiscent modioli experiencing bilateral TMWS; however, the patient was lost to follow up before surgical intervention [85]. Another possible etiology of “CT– TMWS” is an unrecognized CFD, as we reported recently [4].
Surgical management using plugging techniques via the middle cranial fossa or transmastoid approaches, as well as resurfacing techniques and round window reinforcement, have all been described (for review see [73]) and will be discussed in Chap. 15, “Surgical Intervention, Revision Surgery and Surgical Complications.”
Spectrum of Known Sites Creating a Third Mobile Window
As shown in Table 1.3 there are currently 15 known sites of dehiscence that can be seen using high-resolution temporal bone CT and in addition there are sites of dehiscence that cannot yet be seen with contemporary high-resolution temporal bone CT scans (CT– TMWS). The 15 known visible by imaging sites of dehiscence are: superior semicircular canal dehiscence (SSCD), posterior semicircular canal dehiscence, posterior semicircular canal-jugular bulb dehiscence, posterior semicircular canal-endolymphatic sac/vestibular aqueduct dehiscence, lateral semicircular canal dehiscence, lateral semicircular canal-facial nerve dehiscence, cochlea-facial nerve dehiscence (CFD), cochlea-internal carotid artery dehiscence, cochlea-internal auditory canal dehiscence, cochlear otosclerosis with internal auditory canal involvement, wide vestibular aqueduct, endolymphatic sac-jugular bulb dehiscence, posttraumatic hypermobile stapes footplate, vestibule-middle ear dehiscence, modiolus (X-linked stapes gusher) plus CT– TWS (see review [4]).The prevalence of these TMWS sites in a cohort of 401 patients (802 temporal bones; 502 temporal bones associated with TMWS symptoms) with TMWS symptoms have been reported [4]. Of note, as shown in Table 1.4, there can be more than one site of dehiscence which has important implications for patients with persistent TMWS symptoms after surgical management of the most obvious site of dehiscence.
In general, surgical management involves plugging of the site of dehiscence when doing so introduces low to no morbidity; however, some sites of dehiscence such as a CFD could be plugged, but the resultant deafness and facial paralysis represent an unacceptable morbidity. For these sites, round window reinforcement has been an effective management strategy. Wackym et al. reported a series of CFD dehiscence patients managed with round window reinforcement using layered perichondrium, cartilage and minced perichondrium admixed with tissue glue [4]. Statistically there was no change in hearing postoperatively and a highly significant reduction in Dizziness Handicap Inventory scores (Fig. 1.2) [4].

For the cochlea-facial nerve dehiscence cohort who had round window reinforcement procedures performed, the preoperative mean Dizziness Handicap Inventory score was 54.25 (SE 4.9, range 30–74). The postoperative mean Dizziness Handicap Inventory score was 5.5 (SE 4.2, range 0–34). This improvement was highly statistically significant (paired t-test, p < 0.0001). These data are plotted as a single black line. Individual patients are plotted as separate lines (red). Copyright © P.A. Wackym, used with permission
This topic is covered in more detail in Chap. 7, “Other Sites of Dehiscence” and in Chap. 15, “Surgical Intervention, Revision Surgery and Surgical Complications.”
Frontiers
The development of an experimental model for various TMWS sites, but especially SSCD, is essential for us to begin understanding the mechanisms responsible for the cognitive dysfunction, spatial disorientation, anxiety and migraine experienced by patients with TMWS. With this knowledge, better insight into the role peripheral vestibular dysfunction plays in disrupting central nervous system processing will emerge and thereby will open new avenues in clinical intervention in resolving these problems or accelerating recovery in these patients. It is also anticipated that advances will be made in refining surgical techniques (e.g., biological 3-D printed caps to cover SSCD defects) and improved diagnostic methods.
References
Merchant SN, Rosowski JJ. Conductive hearing loss caused by third-window lesions of the inner ear. Otol Neurotol. 2008;29:282–9. https://doi.org/10.1097/mao.0b013e318161ab24.
Stenfelt S, Goode RL. Bone-conducted sound: physiological and clinical aspects. Otol Neurotol. 2005;26:1245–6. https://doi.org/10.1097/01.mao.0000187236.10842.d5.
Black FO, Pesznecker S, Norton T, et al. Surgical management of perilymphatic fistulas: a Portland experience. Am J Otol. 1992;13:254–62.
Wackym PA, Balaban CD, Zhang P, Siker DA, Hundal JS. Third window syndrome: surgical management of cochlea-facial dehiscence. Front Neurol. 2019;10:1281. https://doi.org/10.3389/fneur.2019.01281.
Naert L, Van de Berg R, Van de Heyning P, et al. Aggregating the symptoms of superior semicircular canal dehiscence syndrome. Laryngoscope. 2018;128(8):1932–8. https://doi.org/10.1002/lary.27062.
Kohut RI, Perilymph fistulas. Clinical criteria. Arch Otolaryngol Head Neck Surg. 1992;118(7):687–92. https://doi.org/10.1001/archotol.1992.01880070017003.
Wackym PA. Vestibular migraine. Patient video describing symptoms before and after treatment with Topamax. https://www.youtube.com/watch?v=Zy7YjCDnLYM. https://doi.org/10.13140/RG.2.1.3096.2647. Published April 12, 2012. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA. Right perilymph fistula not superior canal dehiscence. Patient video describing symptoms before and after surgical repair. https://www.youtube.com/watch?v=bDph0B0uLbg. https://doi.org/10.13140/RG.2.1.3097.8000. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA. Right cochlea-facial nerve dehiscence: 16 year old thought to have conversion disorder. https://youtu.be/fTjsnnUALBw. https://doi.org/10.13140/RG.2.2.27418.90564. Published April 14, 2019. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA. Perilymph fistula. https://www.youtube.com/watch?v=jSAM6h-7Mwc. https://doi.org/10.13140/RG.2.1.1000.6488. Published April 15, 2012. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA. Right superior semicircular canal dehiscence repair: Symptoms and recovery. https://youtu.be/er4k8NZrG2I. https://doi.org/10.13140/RG.2.2.32032.79361. Published January 9, 2017. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA. Recurrent third window syndrome co-morbidity: Functional neurological symptom disorder. https://youtu.be/AgUy07QxTxo. https://doi.org/10.13140/RG.2.2.15255.57763. Published January 9, 2017. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA. Otic capsule dehiscence syndrome in one ear after a car accident. https://www.youtube.com/watch?v=1Nl9T6etxqM. https://doi.org/10.13140/RG.2.1.3359.9440. Published April 5, 2015. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA. Cochlea-facial nerve dehiscence: traumatic third window syndrome after a snowboarding accident. https://youtu.be/NCDMD5FGf-w. https://doi.org/10.13140/RG.2.2.17283.76327. Published April 9, 2019. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA. Surgery for cochlea-facial nerve dehiscence: Symptoms and tuning fork testing. https://youtu.be/lFR-zdYlIsY. https://doi.org/10.13140/RG.2.2.34129.79209. Published April 14, 2019. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA. Tuning fork testing in otic capsule dehiscence syndrome. https://www.youtube.com/watch?v=Szp_kO8oVos. https://doi.org/10.13140/RG.2.1.4408.5204. Published April 21, 2015. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA. Tuning fork testing before and after repair of two types of otic capsule dehiscence. https://www.youtube.com/watch?v=NIauJPbvSpA. https://doi.org/10.13140/RG.2.1.4365.7048. Published December 13, 2015. Accessed August 15, 2022. Copyright © P.A. Wackym, MD, used with permission.
Wackym PA, Wood SJ, Siker DA, Carter DM. Otic capsule dehiscence syndrome: Superior canal dehiscence syndrome with no radiographically visible dehiscence. Ear Nose Throat J. 2015;94(7):8–24. https://doi.org/10.1177/014556131509400802.
Wackym PA, Balaban CD, Mackay HT, et al. Longitudinal cognitive and neurobehavioral functional outcomes after repairing otic capsule dehiscence. Otol Neurotol. 2016;37(1):70–82. https://doi.org/10.1097/MAO.0000000000000928.
Wackym PA, Mackay-Promitas HT, Demirel S, et al. Comorbidities confounding the outcomes of surgery for third window syndrome: outlier analysis. Laryngosc Invest Otolaryngol. 2017;2(5):225–53. https://doi.org/10.1002/lio2.89.
Wackym PA, Balaban CD. Molecules, motion, and man. Otolaryngol Head Neck Surg. 1998;118:15–23.
Balaban CD, Thayer JF. Neurological bases for balance-anxiety links. J Anxiety Disord. 2001;15(1-2):53–79. https://doi.org/10.1016/s0887-6185(00)00042-6.
Balaban CD, McGee DM, Zhou J, Scudder CA. Responses of primate caudal parabrachial nucleus and Kölliker-fuse nucleus neurons to whole body rotation. J Neurophysiol. 2002;88:3175–93. https://doi.org/10.1152/jn.00499.2002.
Baek JH, Zheng Y, Darlington CL, Smith PF. Evidence that spatial memory deficits following bilateral vestibular deafferentation in rats are probably permanent. Neurobiol Learn Mem. 2010;94(3):402–13. https://doi.org/10.1016/j.nlm.2010.08.007.
Smith PF, Darlington CL, Zheng Y. Move it or lose it–is stimulation of the vestibular system necessary for normal spatial memory? Hippocampus. 2010;20(1):36–43. https://doi.org/10.1002/hipo.20588.
Deroualle D, Lopez C. Toward a vestibular contribution to social cognition. Front Integr Neurosci. 2014;8:16. https://doi.org/10.3389/fnint.2014.00016.
Smith PF, Darlington CL. Personality changes in patients with vestibular dysfunction. Front Hum Neurosci. 2013;7:678. https://doi.org/10.3389/fnhum.2013.00678.
Balaban CD. Projections from the parabrachial nucleus to the vestibular nuclei: potential substrates for autonomic and limbic influences on vestibular responses. Brain Res. 2004;996(1):126–37. https://doi.org/10.1016/j.brainres.2003.10.026.
Darlington CL, Goddard M, Zheng Y, Smith PF. Anxiety-related behavior and biogenic amine pathways in the rat following bilateral vestibular lesions. Ann N Y Acad Sci. 2009;1164:134–9. https://doi.org/10.1111/j.1749-6632.2008.03725.x.
Minor LB. Clinical manifestations of superior semicircular canal dehiscence. Laryngoscope. 2005;115:1717–27.
Crane BT, Lin FR, Minor LB, Carey JP. Improvement in autophony symptoms after superior canal dehiscence repair. Otol Neurotol. 2010;31(1):140–6.
Bhutta MF. Eye movement autophony in superior semicircular canal dehiscence syndrome may be caused by trans-dural transmission of extraocular muscle contraction. Int J Audiol. 2015;54(1):61–2.
Huizinga E. The physiological and clinical importance of experimental work on the pigeon’s labyrinth. J Laryngol Otol. 1955;69:260–8. https://doi.org/10.1017/s0022215100050635.
Tullio P. Some experiments and considerations on experimental otology and phonetics: a lecture delivered at the meeting of the “Società dei cultori delle scienze e naturali” of Cagliari on 1st, July 1929: L. Cappelli 1929 ASIN: B0008B2T6Y
Tullio P. Das Ohr und die Entstehung der Sprache und Schrift. Berlin: Urban & Schwarzenberg; 1929. p. 1–455.
Addams-Williams J, Wu K, Ray J. The experiments behind the Tullio phenomenon. J Laryngol Otol. 2014;128(3):223–7. https://doi.org/10.1017/S0022215114000280.
Cawthorne T. Contributions of surgery to problems of neurootology. Br Med Bull. 1956;12:143–5.
Shea JJ Jr. A personal history of stapedectomy. Am J Otol. 1998;19(5):S2–12.
Shambaugh GE Jr. Julius Lempert and the fenestration operation. Am J Otol. 1995;16(2):247–52.
Lempert J. Lempert fenestra nov-ovalis for the restoration of practical unaided hearing in clinical otosclerosis; its present status. Proc R Soc Med. 1948;41(9):617–30.
Cawthorne T. Otosclerosis. J Laryngol Otol. 1955;69:437–56. https://doi.org/10.1017/S0022215100050933.
Copeland BJ, Buchman CA. Management of labyrinthine fistulae in chronic ear surgery. Am J Otolaryngol. 2003;24(1):51–60. https://doi.org/10.1053/ajot.2003.10.
Meyer A, Bouchetemblé P, Costentin B, Dehesdin D, Lerosey Y, Marie JP. Lateral semicircular canal fistula in cholesteatoma: diagnosis and management. Eur Arch Otorhinolaryngol. 2016;273(8):2055–63. https://doi.org/10.1007/s00405-015-3775-6.
Schmerber S, Baguant A, Fabre C, Quatre R. Surgical treatment of cholesteatomatous labyrinthine fistula by hydrodissection. Eur Ann Otorhinolaryngol Head Neck Dis. 2021;138(4):279–82. https://doi.org/10.1016/j.anorl.2020.11.004.
Steffen TN, Sheehy JL, House HP. The slipped strut problem. Ann Otol Rhinol Laryngol. 1963;72:191–205.
Fee GA. Traumatic perilymphatic fistulas. Arch Otolaryngol. 1968;88:477–80.
Colebatch JG, Halmagyi GM, Skuse NF. Myogenic potentials generated by click-evoked vestibulocollic reflex. J Neurol Neurosurg Psychiatry. 1994;57:190–7.
Welgampola MS, Colebatch JG. Characteristics and clinical applications of vestibular-evoked myogenic potentials. Neurology. 2005;64:1682–8.
Curthoys IS. A critical review of the neurophysiological evidence underlying clinical vestibular testing using sound, vibration and galvanic stimuli. Clin Neurophysiol. 2010;121(2):132–44.
Wackym PA, Ratigan JA, Birck JD, et al. Rapid cVEMP and oVEMP responses elicited by a novel head striker and recording device. Otol Neurotol. 2012;33(8):1392–400. https://doi.org/10.1097/MAO.0b013e318268d234.
McNerney KM, Burkard RF. The vestibular evoked myogenic potential (VEMP): air- versus bone-conducted stimuli. Ear Hear. 2011;32(6):e6–e15.
Hunter JB, Patel NS, O’Connell BP, et al. Cervical and ocular VEMP testing in diagnosing superior semicircular canal dehiscence. Otolaryngol Head Neck Surg. 2017;156:917–23. https://doi.org/10.1177/0194599817690720.
Brantberg K, Bergenius J, Tribukait A. Vestibular-evoked myogenic potentials in patients with dehiscence of the superior semicircular canal. Acta Otolaryngol. 1999;119:633–40. https://doi.org/10.1080/00016489950180559.
Pfammatter A, Darrouzet V, Gärtner M, et al. A superior semicircular canal dehiscence syndrome multicenter study: is there an association between size and symptoms? Otol Neurotol. 2010;31(3):447–54. https://doi.org/10.1097/MAO.0b013e3181d27740.
Streubel SO, Cremer PD, Carey JP, Weg N, Minor LB. Vestibular-evoked myogenic potentials in the diagnosis of superior canal dehiscence syndrome. Acta Otolaryngol Suppl. 2001;545:41–9. https://doi.org/10.1080/000164801750388090.
Welgampola MS, Myrie OA, Minor LB, Carey JP. Vestibular-evoked myogenic potential thresholds normalize on plugging superior canal dehiscence. Neurology. 2008;70:464–72. https://doi.org/10.1212/01.wnl.0000299084.76250.4a.
Tran ED, Swanson A, Sharon JD, et al. Ocular vestibular-evoked myogenic potential amplitudes elicited at 4 kHz optimize detection of superior semicircular canal dehiscence. Front Neurol. 2020;11:879. https://doi.org/10.3389/fneur.2020.00879.
Zhou G, Gopen Q, Poe DS. Clinical and diagnostic characterization of canal dehiscence syndrome: a great otologic mimicker. Otol Neurotol. 2007;28(7):920–6.
Ward BK, Wenzel A, Ritzl EK, et al. Near-dehiscence: clinical findings in patients with thin bone over the superior semicircular canal. Otol Neurotol. 2013;34:1421–8. https://doi.org/10.1097/MAO.0b013e318287efe6.
Schwartz T, Lindemann TL, Mongelluzzo G, Wackym PA, Gadre AK. Gray-scale inversion on HRCT: an adjunct to visualize fine structures of the temporal bone. Ann Otol Rhinol Laryngol. 2021;130(10):1125–31. https://doi.org/10.1177/0003489421996844.
Minor LB, Solomon D, Zinreich JS, Zee DS. Sound- and/or pressure-induced vertigo due to bone dehiscence of the superior semicircular canal. Arch Otolaryngol Head Neck Surg. 1998;124(3):249–58. https://doi.org/10.1001/archotol.124.3.249.
Dalchow CV, Schmidt C, Harbort J, Knecht R, Grzyska U, Muenscher A. Imaging of ancient Egyptian mummies’ temporal bones with digital volume tomography. Eur Arch Otorhinolaryngol. 2012;269(10):2277–84. https://doi.org/10.1007/s00405-012-2011-x.
Wackym PA, Balaban CD, Ikezono T, Agrawal Y. Third window syndrome. Lausanne: Frontiers Media SA. 2021. https://doi.org/10.3389/978-2-88971-190-1. https://www.frontiersin.org/research-topics/12065/third-window-syndrome
Wackym PA, Agrawal Y, Ikezono T, Balaban CD. Editorial: Third window syndrome. Front Neurol. 2021;12:704095. https://doi.org/10.3389/fneur.2021.704095. PMID: 34220698; PMCID: 8250852.
Wackym PA. Round window reinforcement surgery for cochlea-facial nerve dehiscence: symptoms and testing. https://youtu.be/2z1RJEKZQ1A. Published April 15, 2019. https://doi.org/10.13140/RG.2.2.30617.06247. Accessed August 15, 2022.
Smullen JL, Andrist EC, Gianoli GJ. Superior semicircular canal dehiscence: a new cause of vertigo. J La State Med Soc. 1999;151(8):397–400.
Grieser BJ, Kleiser L, Obrist D. Identifying mechanisms behind the Tullio phenomenon: a computational study based on first principles. J Assoc Res Otolaryngol. 2016;17(2):103–18. https://doi.org/10.1007/s10162-016-0553-0.
Fox EJ, Balkany TJ, Arenberg IK. The Tullio phenomenon and perilymph fistula. Otolaryngol Head Neck Surg. 1988;98(1):88–9.
Pyykkö I, Ishizaki H, Aalto H, Starck J. Relevance of the Tullio phenomenon in assessing perilymphatic leak in vertiginous patients. Am J Otol. 1992;13(4):339–42.
Colebatch JG, Rothwell JC, Bronstein A, Ludman H. Click-evoked vestibular activation in the Tullio phenomenon. J Neurol Neurosurg Psychiatry. 1994;57:1538–40. https://doi.org/10.1136/jnnp.57.12.1538.
Ostrowski VB, Hain TC, Wiet RJ. Pressure-induced ocular torsion. Arch Otolaryngol Head Neck Surg. 1997;123(6):646–9.
Weinreich HM, Carey JP. Perilymphatic fistulas and superior semi-circular canal dehiscence syndrome. Adv Otorhinolaryngol. 2019;82:93–100. https://doi.org/10.1159/000490276.
Ward BK, Carey JP, Minor LB. Superior canal dehiscence syndrome: lessons from the first 20 years. Front Neurol. 2017;8:177. https://doi.org/10.3389/fneur.2017.00177.
Wackym PA. Cochlea-facial nerve dehiscence: third window syndrome after a car accident. https://youtu.be/eJX2RA3okKc. Published April 7, 2019. https://doi.org/10.13140/RG.2.2.12447.20646. Accessed August 15, 2022.
Mikulec AA, Poe DS, McKenna MJ. Operative management of superior semicircular canal dehiscence. Laryngoscope. 2005;115(3):501–7.
Young L, Isaacson B. Cochlear and petrous carotid canal erosion secondary to cholesteatoma. Otol Neurotol. 2010;31:697–8.
Meiklejohn DA, Corrales CE, Boldt BM, et al. Pediatric semicircular canal dehiscence: radiographic and histologic prevalence, with clinical correlations. Otol Neurotol. 2015;36(8):1383–9.
Park JJ, Shen A, Loberg C, Westhofen M. The relationship between jugular bulb position and jugular bulb related inner ear dehiscence: a retrospective analysis. Am J Otolaryngol. 2015;36(3):347–51.
Gopen Q, Zhou G, Poe D, Kenna M, Jones D. Posterior semicircular canal dehiscence: first reported case series. Otol Neurotol. 2010;31(2):339–44.
Bear ZW, McEvoy TP, Mikulec AA. Quantification of hearing loss in patients with posterior semicircular canal dehiscence. Acta Otolaryngol. 2015;135(10):974–7.
Elmali M, Poltat AV, Kucuk H, Atmaca S, Aksoy A. Semicircular canal dehiscence: frequency and distribution on temporal bone CT and its relationship with the clinical outcomes. Eur J Radiol. 2013;82(10):e606–9.
Blake DM, Tomovic S, Vazquez A, Lee HJ, Jyung RW. Cochlear-facial dehiscence–a newly described entity. Laryngoscope. 2014;124(1):283–9.
Fujita T, Kobayashi T, Saito K, Seo T, Ikezono T, Doi K. Vestibule-middle ear dehiscence tested with perilymph-specific protein cochlin-tomoprotein (CTP) detection test. Front Neurol. 2019;10:47.
Manzari L. Multiple dehiscences of bony labyrinthine capsule. A rare case report and review of the literature. Acta Otorhinolaryngol Ital. 2010;30(6):317–20.
Manzari L, Scagnelli P. Large bilateral internal auditory meatus associated with bilateral superior semicircular canal dehiscence. Ear Nose Throat J. 2013;92(1):25–33.
Fang CH, Chung SY, Blake DM, et al. Prevalence of cochlear-facial dehiscence in a study of 1,020 temporal bone specimens. Otol Neurotol. 2016;37(7):967–72.
Ho ML, Moonis G, Halpin CF, Curtin HD. Spectrum of third window abnormalities: semicircular canal dehiscence and beyond. AJNR Am J Neuroradiol. 2017;38(1):2–9. https://doi.org/10.3174/ajnr.A4922.
Koo JW, Hong SK, Kim DK, Kim JS. Superior semicircular canal dehiscence syndrome by the superior petrosal sinus. J Neurol Neurosurg Psychiatry. 2010;81:465–7. https://doi.org/10.1136/jnnp.2008.155564.
Ionescu EC, Al Tamami N, Neagu A, et al. Superior semicircular canal ampullae dehiscence as part of the spectrum of the third window abnormalities: a case study. Front Neurol. 2017;8:683. https://doi.org/10.3389/fneur.2017.00683.
Dasgupta S, Ratnayake SAB. Functional and objective audiovestibular evaluation of children with apparent semicircular canal dehiscence - a case series in a pediatric vestibular center. Front Neurol. 2019;10:306. https://doi.org/10.3389/fneur.2019.00306.
Hornibrook J. The balance abnormality of chronic perilymph fistula. https://www.youtube.com/watch?v=2DXgQMnlgbw. Published Nov 26, 2015. Accessed August 15, 2022.
Crane BT, Minor LB, Carey JP. Superior canal dehiscence plugging reduces dizziness handicap. Laryngoscope. 2008;118:1809–13. https://doi.org/10.1097/MLG.0b013e31817f18fa.
Gadre AK, Edwards IR, Baker VM, Roof CR. Membranous or hypermobile stapes footplate: a new anatomic site resulting in third window syndrome. Front Neurol. 2020;11:871. https://doi.org/10.3389/fneur.2020.00871.
Matsuda H, Tanzawa Y, Sekine T, et al. Congenital membranous stapes footplate producing episodic pressure-induced perilymphatic fistula symptoms. Front Neurol. 2020;11:585747. https://doi.org/10.3389/fneur.2020.585747.
Lin K, Lahey R, Beckley R, et al. Validating the utility of high frequency ocular vestibular evoked myogenic potential testing in the diagnosis of superior semicircular canal dehiscence. Otol Neurotol. 2019;40(10):1353–8. https://doi.org/10.1097/MAO.0000000000002388.
Arts HA, Adams ME, Telian SA, El-Kashlan H, Kileny PR. Reversible electrocochleographic abnormalities in superior canal dehiscence. Otol Neurotol. 2009;30(1):79–86.
Sharon JD, Pross SE, Ward BK, Carey JP. Revision surgery for superior canal dehiscence syndrome. Otol Neurotol. 2016;37(8):1096–103.
Zou J, Zhang W, Poe D, Zhang Y, Ramadan UA, Pyykkö I. Differential passage of gadolinium through the mouse inner ear barriers evaluated with 4.7T MRI. Hear Res. 2010;259(1-2):36–43.
Zou J, Poe D, Ramadan UA, Pyykkö I. Oval window transport of Gd-dOTA from rat middle ear to vestibulum and scala vestibuli visualized by in vivo magnetic resonance imaging. Ann Otol Rhinol Laryngol. 2012;121(2):119–28.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Wackym, P.A., Balaban, C.D., Mowery, T.M. (2022). History and Overview of Third Mobile Window Syndrome. In: Gianoli, G.J., Thomson, P. (eds) Third Mobile Window Syndrome of the Inner Ear. Springer, Cham. https://doi.org/10.1007/978-3-031-16586-3_1
Download citation
DOI: https://doi.org/10.1007/978-3-031-16586-3_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-16585-6
Online ISBN: 978-3-031-16586-3
eBook Packages: MedicineMedicine (R0)