
Abstract
Tardive dyskinesia (TD), frequently expressed as excessive perioral activity, represents an adverse outcome of prolonged antipsychotic treatments, occurring in 5% of patients per treatment year. Although neuronal mechanisms underlying TD are largely unknown, recent experiments in animal models of TD provide insight into neuronal mechanisms associated with TD and implicate newer treatment approaches. It is evident that a predominance in the ratio of dopamine (DA) D1:D2 receptor (R) activation accounts for induction of perioral movements in rodent models of TD, also in nonhuman primate models of TD, and in humans with TD. Experimentally, TD is produced in animal models in a manner analogous to that by which TD is produced in humans – by continuous prolonged DA D2 R antagonist treatment (i.e., an antipsychotic drug). Also, in rodent models of TD, lesioning of dopaminergic – mainly nigroneostriatal – neurons hastens the time to onset of TD, while increasing its severity and resultant permanence, even after discontinuing D2 R antagonist treatment. Induction of perioral activity is related to DAR supersensitivity but unrelated to numbers of D1 R and D2 R in the neostriatum, a brain region associated with perioral activity. More apropos, serotoninergic systems apparently have a greater role in effecting perioral activity, as a 5-HT2C R antagonist most effectively abates perioral activity in the rodent TD model. These analyses guide towards a newer understanding of mechanisms underlying TD and provide insight into novel approaches towards treatment of human TD. It is proposed that there be refocus towards 5-HT2C-R antagonists as effective antidyskinetic agents.
Access provided by Autonomous University of Puebla. Download reference work entry PDF
Similar content being viewed by others


Keywords
- 5-HT2 receptor
- 5-Hydroxytryptamine
- 6-Hydroxydopamine
- D2 receptor
- Dopamine
- Haloperidol
- Perioral movements
- Receptor supersensitivity
- Serotonin
- Tardive dyskinesia
- Vacuous chewing
1 Introduction
On the website of the National Institute of Neurological Disorders and Stroke (NINDS) (https://www.ninds.nih.gov/Disorders/All-Disorders/Tardive-Dyskinesia-Information-Page), tardive dyskinesia (TD) is classified as an extrapyramidal syndrome arising from long-term use of neuroleptic agents (i.e., antipsychotics). TD is characterized by repetitive involuntary purposeless movements of specific muscle groups, which may include fingers, arms, legs, and trunk but generally presents as oral dyskinesia (typically, vacuous chewing movements, VCMs) which may include lip smacking and tongue protrusion. A person with TD may appear to be chewing gum.
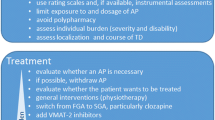
TD arises in humans, nonhuman primates (Blanchet et al., 2012), and rodents by chronic (exclusive) treatment with a dopamine (DA) D2 receptor (R) antagonist (Saifee & Edwards, 2011) – the class of agents oft used for treating schizophrenia. The incidence rate of TD is approximately 5% per treatment year with a “classical” (first-generation) antipsychotic drug (e.g., haloperidol) (Kane et al., 1985) and two to threefold less so when atypical antipsychotic agents (e.g., clozapine or quetiapine) are used (Tarsy et al., 2011). TD tends to be long lived, sometimes lifelong, and is usually refractory to treatment. TD remains a serious problem today. First-line “treatment” of TD is withdrawal of the antipsychotic, if possible. Vesicular monoamine transport inhibitors such as deutetrabenazine and valbenazine are viable treatment options (Bhidayasiri et al., 2018; Keepers et al., 2020; Ricciardi et al., 2019), although a variety of other drugs is often attempted.
2 Multineuronal Associations with Tardive Dyskinesia
Although TD arises from prolonged administration of a DA D2 R antagonist, it is recognized that many different neuronal phenotypes may have a role in the development or persistence of TD (Casey, 1987; Egan et al., 1995; Gong et al., 1992; Gunne & Häggström, 1983; Jeste & Caligiuri, 1993; Knable et al., 1994; Kostrzewa, 1995; Waddington, 1990). Cholinergic (Kostrzewa & Neely, 1993; Rupniak et al., 1983, 1985; Salamone et al., 1990), GABA-ergic [GABA, gamma-aminobutyric acid] (Gunne et al., 1982; Lloyd et al., 1985; Mithani et al., 1987; Tamminga et al., 1979), and serotoninergic (Gong et al., 1992; Gong & Kostrzewa, 1992) involvements have been implicated in TD. Nevertheless, the focus of this chapter will remain on dopaminergic systems and the uncovered important role of serotoninergic systems in TD.
3 Oral Dyskinesia Arising in Rodents from Acute Dopamine Receptor Agonist or Antagonist Treatments
Acute administration of a DA D2 R antagonist to rats or mice results in the onset of oral dyskinesias, which are prominent over the following hour or more. The short-lived effect of the D2 R antagonist is dose-related. Similarly, acute administration of a DA D1 R agonist is associated with a short-lived and dose-related induction of oral dyskinesia. These correlated findings give credence to the possibility that oral dyskinesia may be related to an imbalance in D1 R/D2 R activation by the endogenous neurotransmitter, DA (Rosengarten et al., 1983). Moreover, when a D2 R antagonist is administered chronically, as per animal modeling of TD, or when psychiatric patients are treated long term with an antipsychotic drug, one must consider the long-term effect of such treatment on the overall balance of D1 R/D2 R activation – and the effect this might have on the origin of TD.
3.1 Experimental Induction of Oral Dyskinesia in Rodents by Acute Dopamine D1 R Agonist Treatment or D2 R Antagonist Treatment
Antipsychotics and D2 R antagonists in general induce the occurrence of spontaneous oral activity – the so-called oral dyskinesias in humans and the so-called VCMs in rodents (Clow et al., 1979; Iversen et al., 1980; Waddington & Gamble, 1980). Similarly, DA D1 R agonists induce oral activity (Arnt et al., 1987; Koshikawa et al., 1987; Levin et al., 1989; Molloy & Waddington, 1988; Murray & Waddington, 1989; Rosengarten et al., 1983; Rosengarten, Schweitzer, Egawa, & Friedhoff, 1986a; Rosengarten, Schweitzer, & Friedhoff, 1986b; Rupniak et al., 1985), and it is the presumed balance in D1R/D2R activation that is considered to be important for this behavioral response (Rosengarten et al., 1983). For example, in rodents, there is an increase in oral activity when there is an increase in D1R/D2R activation, as occurs with D2R antagonists, also after D1R agonist treatment (Johansson et al., 1987; Molloy & Waddington, 1987, 1988; Rosengarten et al., 1983), and in rat strains with reduced numbers of D2R (Rosengarten et al. 1986a, b).
3.2 Effect of Neonatal Dopaminergic Denervation on Induction of Oral Dyskinesia in Rodents by Dopamine D1R Agonists or D2R Antagonists
When rats are lesioned perinatally with the neurotoxin 6-hydroxydopamine (6-OHDA; desipramine pretreatment), repeated D1 R agonist treatments “prime” DA D1 R. Initial D1 R agonist treatments have no marked effect, but repeated D1 R agonist treatments permanently sensitize D1 R, so that exaggerated behavioral responses are observed following acute D1 R agonist treatment. This process is known as homologous priming of D1 R, and the resulting D1 R supersensitization is lifelong (Breese et al. (1985, 1987). Also, repeated D2 R agonist treatments of 6-OHDA-lesioned rats can induce the D1 R supersensitization, a process known as heterologous priming of D1 R (Criswell et al., 1989).
When rats so-lesioned perinatally with 6-OHDA were challenged with a single dose of a D2 R antagonist, there was an increase in perioral movements when compared to the effect in nonlesioned control rats (Kostrzewa & Hamdi, 1991). In an analogous manner for rats that were perinatally 6-OHDA lesioned, the first adulthood challenge dose of a D1 R agonist surprisingly produced an increased number of perioral movements in comparison to nonlesioned control rats (Kostrzewa & Gong, 1991). Thus, in contrast to the latent D1 R supersensitivity for locomotory and stereotyped activities that required unmasking by repeated D1 R agonist treatments (Breese et al., 1985, 1987), there was overt supersensitization of D1 R for D1 R agonist induction of perioral activity. Moreover, in rats that were perinatally 6-OHDA-lesioned, perioral activity was induced in adulthood by a D1 R agonist dose that was 100–1,000 times lower than was needed for induction of perioral activity in intact control rats (Kostrzewa & Gong, 1991). The D1 R supersensitivity for this effect developed if the nigroneostriatal dopaminergic fiber lesioning by 6-OHDA occurred within the first week postbirth (Kostrzewa et al., 1993) and if neostriatal DA depletion was 98.5 % or more (Gong et al., 1993). This D1 R supersensitization was also lifelong. Moreover, the effect was unaccompanied by an increase in the Bmax for D1 R (i.e., relative number of D1 R) or change in the Kd (i.e., relative affinity of the receptor for an agonist) (Gong et al., 1994).
Perinatal 6-OHDA treatment which produces near total destruction of nigroneostriatal dopaminergic neurons (Doucet et al., 1986) leaves the ventral tegmental nucleus largely intact and able to provide dopaminergic innervation to limbic regions (Fernandes Xavier et al., 1994; Snyder et al., 1986). Thus, the important element of the above studies is that a lesion of dopaminergic innervation to the neostriatum resulted in overt D1 R supersensitization for the induction of oral activity (Kostrzewa, 1995; Kostrzewa et al., 1998, 2003, 2008).
4 Oral Dyskinesia Arising in Rodents from Acute Serotonin Agonist Treatment
When perinatally 6-OHDA-lesioned rats were challenged in adulthood with the serotonin (5-hydroxytryptamine, 5-HT) 5-HT2 R agonist m-chlorophenylpiperazine (mCPP), the initial mCPP dose produced an enhanced increase in the number of perioral movements in comparison to that of intact control rats (Gong & Kostrzewa, 1992). This finding and others indicate that 5-HT2 R is supersensitized by 6-OHDA lesioning (El Mansari et al., 1994). The effect was not replicated by 5-HT1A R agonist 8-OH-DPAT [(±)8-hydroxydipropylaminotetralin] or 5-HT1B R agonist CGS-12066B (7-trifluoromethyl-4(4-methyl-1-piperazinyl)-pyrrolo[1,2-alquinoxaline]); nor was the effect attenuated by 5-HT1A/1B R antagonist pindolol, nor by the predominate 5-HT2A R antagonist ketanserin, nor by 5-HT3 R antagonist MDL 72222 (3-tropanyl-3,4-dichlorobenzoate) (Gong et al., 1993). However, the selective 5-HT2 R antagonist mianserin blocked the effect of mCPP, indicating that 5-HT2 R, perhaps 5-HT2C R specifically, represents the subtype that is overtly supersensitized by perinatal 6-OHDA lesioning. It is thus considered that supersensitized 5-HT2C R accounts for enhanced perioral movements following an adulthood 5-HT-agonist challenge dose in the group of rats perinatally 6-OHDA-lesioned rats (Gong et al., 1993).
In fact, the number of perioral movements after mCPP treatment was greater than that following D1 R agonist treatment (Gong et al., 1992). Mianserin pretreatment, in addition to blocking the effect of the 5-HT2 R agonist mCPP, blocked the effect of a D1 R agonist on perioral activity (Gong et al., 1992), and the dorsal striatum was one site for this interaction (Plech et al., 1995; Salamone et al., 1990). By contrast, a D1 R antagonist did not block the effect of mCPP (Gong et al., 1992). These findings indicate that DAR supersensitivity for perioral activity is mediated via a serotoninergic system and notably at the 5-HT2 R (Gong et al., 1993).
5-HT fiber hyperinnervation of neostriatum and the forebrain is prominent in rats lesioned perinatally with 6-OHDA (Berger et al., 1985; Snyder et al., 1986; Mrini et al., 1995; see Kostrzewa et al., 1998), and this is accompanied by an approximate 30–60% increase in the number of 5-HT1A R, 5-HT1B R, 5-HT1nonAB R, 5-HT2A R, and 5-HT2C R (Radja et al., 1993). Therefore, to further explore the effect of 5-HT innervation on perioral activity, the neurotoxin 5,7-dihydroxytryptamine (5,7-DHT) was co-administered with 6-OHDA to perinatal rats which were then studied as adults. In rats co-lesioned with 6-OHDA and 5,7-DHT, the supersensitized perioral response to a D1 R agonist was eliminated, indicating that 5-HT fibers indeed mediate the D1 R agonist effect on perioral movements (Brus et al., 1994).
5 Abatement of Oral Dyskinesia in a Rodent Model of Tardive Dyskinesia
Although acute effects of D1 R agonists on perioral activity are attenuated by acute D1 R antagonist treatment, a 5-HT2 R antagonist is equally effective (Gong et al., 1994). In the rodent model of TD, produced by chronic administration (approximating one year) of a D2 R antagonist, acute treatment during the haloperidol-withdrawal phase with a D1 R antagonist does not reduce the incidence of perioral movements (Kostrzewa et al., 2007); nor does a D2 R antagonist (spiperone), muscarinic receptor antagonist (scopolamine), histamine H1 R antagonist (cyproheptadine), opioid mu receptor agonist (morphine) or mu receptor antagonist (naloxone), adenosine A2A R antagonist (theophylline), alpha-adrenoceptor antagonist (phentolamine, phenoxybenzamine), beta-adrenoceptor antagonist (propranolol); neither a 5-HT1A R agonist (pindolol) nor 5-HT2A R antagonist (ketanserin). However, agents with 5-HT2C R antagonist activity were all effective in acutely reducing the number of perioral movements in the rodent haloperidol-withdrawn model of TD. Thus, mianserin, mesulergine, ritanserin, and clozapine each acutely reduced spontaneous oral activity during 8 months of the haloperidol-withdrawn phase in the rodent model of TD (Kostrzewa et al., 2007).
Despite the neural reorganization that occurs consequent to months-long continuous administration of a D2 R antagonist, it appears that it is an action mediated by serotoninergic 5-HT2 R that is most consequential in reducing spontaneous perioral movements (Gong et al., 1992). This is somewhat surprising, because 5-HT innervation in the brain is considered to be an afferent input, not an efferent output system. 5-HT innervation in the brain arises from the brainstem in the dorsal and medial raphe nuclei (see Kostrzewa et al., 1998). Also, from studies in rodents, it is recognized that perinatal 6-OHDA destruction of dopaminergic nerves results in supersensitization of DA D1 R as well as 5-HT2 R (Brus et al., 1994; Gong et al., 1992). Therefore, in TD it may be that supersensitized 5-HT2 R has the major influence on the induction of spontaneous perioral movements.
6 Tardive Dyskinesia Arising in Rodents from Chronic Dopamine Receptor Antagonist Treatment
Waddington and colleagues (Waddington et al., 1983; Waddington & Gamble, 1980) produced the first rodent model of TD by administering haloperidol in drinking water to rats for 6 consecutive months. An increase in spontaneous perioral movements developed only at 4 months, thus fulfilling the characteristic “tardive” element of TD (i.e., tardive signifies an onset of symptoms after chronic drug treatment). The increase in spontaneous oral activity persisted for as long as haloperidol continued to be administered. When haloperidol was withdrawn, spontaneous perioral movements waned and reverted to normal over a period of a month (see also Waddington, 1990). Ultimately, Ellison and See (1989) showed that the form and periodicity of oral dyskinesias in haloperidol-treated rats was similar in form to those of humans with TD. A disadvantage to this model of TD was that the high level of oral activity in rats dissipated over a period of 1 month, back to control level, after haloperidol was withdrawn. This was unlike the persistence of perioral activity in people with TD.
Gunne et al. (1982) and Glassman and Glassman (1980) had observed that there is an increase in neuroleptic-evoked perioral activity in rats following damage to the brain. In the interest of developing a somewhat more novel model and possibly permanent model of TD, it occurred that DA denervation, as occurs with 6-OHDA lesioning, may be an important element in both the prominence and persistence of oral dyskinesia in rodents. Accordingly, rats with 6-OHDA were perinatally lesioned, then haloperidol was added to the drinking water when these rats were 2 months of age. In these largely DA-denervated rats, an increase in spontaneous oral activity occurred at 3 months, one full month earlier than in intact rats receiving haloperidol via drinking water. Also, the number of perioral movements induced in 6-OHDA-lesioned rats by chronic haloperidol was twice the level for chronic haloperidol-exposed intact rats. At 1 year the neostriatal Bmax for the D2 R antagonist [3H]raclopride was increased ∼25 % in 6-OHDA-lesioned rats and ∼65 % in haloperidol-treated rats were either nonlesioned or additionally 6-OHDA-lesioned. Notably, when 6-OHDA-lesioned rats were withdrawn from haloperidol at 1 year, increased perioral activity did not revert to control levels. The high level of perioral activity observed during the haloperidol phase continued to persist in the group during the withdrawal phase until the study was terminated 8 months later. Further, it is notable that there was no increase in the neostriatal D2 R (i.e., Bmax for [3H]raclopride binding to striatal homogenates) during the haloperidol-withdrawal phase in which there was a persistent high level of perioral activity (Huang et al., 1997). Andersson et al. (1990) have shown that humans with TD do not have an increase in D2 R in the brain.
7 Neural Mechanisms Attending Animal Modeling of Tardive Dyskinesia: Relevance to Human Tardive Dyskinesia
The multiple animal modeling studies relating to TD indicate the following neural mechanism relating to TD. The balance of DA D1 R/D2 R activation appears to be of critical importance. Both D1 R agonists and D2 R antagonists promote oral activity. However, acute effects do not represent a modeling of TD.
TD is, by definition, a “tardive” effect, one that develops over a period of months during prolonged or chronic treatments, specifically with a D2 R antagonist. TD appears to be induced by prolonged imbalance of D1 R/D2 R activation, consequent to a tip in the balance towards D1 R overactivation, and possibly in neostriatum or other regions of the forebrain. The nigroneostriatal dopaminergic tract appears to relate most closely to TD. A remodeling of neural circuitry in the brain, over a period of months, represents an adaptive mechanism to the imbalance of D1 R/D2 R activation, which ultimately results in induction of spontaneous perioral movements. The neural adjustments and reorganization involved in the process are still a mystery.
Nevertheless, prolonged overactivation of DA D1 R appears to be the genesis for TD. Furthermore, it is apparent that damage to brain circuitry can accelerate the appearance of TD and impact on its permanence. From the most recent experimental studies, it is obvious that damage to dopaminergic innervation to neostriatum promotes earlier onset of TD and a fostering of permanence. From studies by Gunne et al. (1988), it is possible that damage to other neural circuits in the brain can have similar influence on TD.
8 Conclusion
Because chronic D2 R antagonist treatment of both humans and rodents produces TD, it is reasonable to assume that similar neural adaptive mechanisms occur in the brain of both rats and humans. Also, because nonspecific injury in the brain (see Gunne & Häggström, 1983) as well as nigroneostriatal dopaminergic damage confer permanence to the TD produced by prolonged DA D2 R antagonist treatment, it is possible that in those patients who develop lifelong TD, there is residual brain damage or dopaminergic fiber degeneration that impacts of the D2 R antagonist treatment. It is speculated that even a mild brain injury could have occurred earlier in life (i.e., head trauma) or perhaps dopaminergic innervation of the brain declines with aging. The latter event is thought to occur and thereby account for the origin of Parkinson’s disease in aged humans (Kish et al., 1992).
Moreover, an increase in the number of nigroneostriatal DA D2 R is not correlated with high levels of perioral movements, as demonstrated by Huang et al. (1997). Studies by Breese et al. (1985) and Gong et al. (1994) established that DA D1 R supersensitivity is not necessarily accompanied by an increase in the number of D1 R. Also, DA D2 R supersensitivity is not correlated with an increase in nigroneostriatal DA D2 R number in rodents (Kostrzewa & Brus, 1991) nor in humans with TD (Andersson et al., 1990). Therefore, the process of receptor supersensitization is not reliant on changes in DA receptor number or affinity. Regardless of underlying factors for development of TD, the animal experimental findings implicate 5-HT2 R antagonists as reasonable agents for the treatment of TD (Kostrzewa et al., 2007). It is proposed that the development of new agents for TD should re-focus on the serotoninergic 5-HT2C receptor.
Abbreviations
- 5,7-DHT:
-
5,7-Dihydroxytryptamine
- 5-HT:
-
5-Hydroxytryptamine, serotonin
- 6-OHDA:
-
6-Hydroxydopamine
- 8-OH-DPAT:
-
(±)8-Hydroxydipropylaminotetralin
- CGS-12066B:
-
7-Trifluoromethyl-4(4-methyl-1-piperazinyl)-pyrrolo[1,2-alquinoxaline]
- DA:
-
Dopamine
- mCPP:
-
m-Chlorophenylpiperazine
- MDL 72222:
-
3-Tropanyl-3,4-dichlorobenzoate
- NINDS:
-
National Institute of Neurological Disorders and Stroke
- R:
-
Receptor
- TD:
-
Tardive dyskinesia
- VCMs:
-
Vacuous chewing movements
References
Andersson, U., Eckernas, S. A., Hartvig, P., Ulin, J., Langstrom, B., & Häggström, J. E. (1990). Striatal binding of 11C-NMSP studied with positron emission tomography in patients with persistent tardive dyskinesia: No evidence for altered dopamine D2 receptor binding. Journal of Neural Transmission General Section, 79, 215–226.
Arnt, J., Hyttel, J., & Perregard, J. (1987). Dopamine D-1 receptor agonists combined with the selective D-2 agonist, quinpirole, facilitate the expression of oral stereotyped behaviour in rats. European Journal of Pharmacology, 133, 137–145.
Berger, T. W., Kaul, S., Stricker, E. M., & Zigmond, M. J. (1985). Hyperinnervation of the striatum by dorsal raphe afferents after dopamine-depleting brain lesions in neonatal rats. Brain Research, 366, 354–358.
Bhidayasiri, R., Jitkritsadakul, O., Friedman, J. H., & Fahn, S. (2018). Updating the recommendations for treatment of tardive syndromes: a systematic review of new evidence and practical treatment algorithm. Journal of Neurological Science, 389, 67–75.
Blanchet, P. F., Parent, M.-T., Rompré, P. H., & Lévesque, D. (2012). Relevance of animal models to human tardive dyskinesia. Behavioral and Brain Functions, 8(12), 1–9.
Breese, G. R., Baumeister, A., Napier, T. C., Frye, G. D., & Mueller, R. A. (1985). Evidence that D1 dopamine receptors contribute to the supersensitive behavioral responses induced by l-dihydroxyphenylalanine in rats treated neonatally with 6-hydroxydopamine. The Journal of Pharmacology and Experimental Therapeutics, 235, 287–295.
Breese, G. R., Duncan, G. E., Napier, T. C., Bondy, S. C., Iorio, L. C., & Mueller, R. A. (1987). 6-Hydroxydopamine treatments enhance behavioral responses to intracerebral microinjection of D1- and D2-dopamine agonists into the nucleus accumbens and striatum without changing dopamine antagonist binding. The Journal of Pharmacology and Experimental Therapeutics, 240, 167–176.
Brus, R., Kostrzewa, R. M., Perry, K. W., & Fuller, R. W. (1994). Supersensitization of the oral response to SKF 38393 in neonatal 6-hydroxydopamine-lesioned rats is eliminated by neonatal 5,7-dihydroxytryptamine treatment. The Journal of Pharmacology and Experimental Therapeutics, 268, 231–237.
Casey, D. E. (1987). Tardive dyskinesia. In H. Y. Meltzer (Ed.), Psychopharmacology: The third generation of progress (pp. 1411–1419). Raven.
Clow, A., Jenner, P., & Marsden, C. D. (1979). Changes in dopamine-mediated behavior during one year’s neuroleptic administration. European Journal of Pharmacology, 57, 365–375.
Criswell, H., Mueller, R. A., & Breese, G. R. (1989). Priming of D1-dopamine receptor responses: Long-lasting behavioral supersensitivity to a D1-dopamine agonist following repeated administration to neonatal 6-OHDA-lesioned rats. The Journal of Neuroscience, 9, 125–133.
Doucet, G., Descarries, L., & Garcia, S. (1986). Quantification of the dopamine innervation in adult rat neostriatum. Neuroscience, 19, 427–445.
Egan, M. F., Hyde, T. M., Kleinman, J. E., & Wyatt, R. J. (1995). Neuroleptic-induced vacuous chewing movements in rodents: Incidence and effects of long-term increases in haloperidol dose. Psychopharmacology, 117, 74–81.
El Mansari, M., Radja, F., Ferron, A., Reader, T. A., Molina-Holgado, E., & Descarries, L. (1994). Hypersensitivity to serotonin and its agonists in serotonin-hyperinnervated neostriatum after neonatal dopamine denervation. European Journal of Pharmacology, 261, 171–178.
Ellison, G. D., & See, R. E. (1989). Rats administered chronic neuroleptics develop oral movements which are similar in form to those in humans with tardive dyskinesia. Psychopharmacology, 98, 564–566.
Fernandes Xavier, F. G., Doucet, G., Geffard, M., & Descarries, L. (1994). Dopamine neoinnervation in the substantia nigra and hyperinnervation in the interpeduncular nucleus of adult rat following neonatal cerebroventricular administration of 6-hydroxydopamine. Neuroscience, 59, 77–87.
Glassman, R. B., & Glassman, H. N. (1980). Oral dyskinesia in brain-damaged rats withdrawn from a neuroleptic: Implications for models of tardive dyskinesia. Psychopharmacology, 69, 19–25.
Gong, L., & Kostrzewa, R. M. (1992). Supersensitized oral response to a serotonin agonist in neonatal 6-OHDA treated rats. Pharmacology, Biochemistry, and Behavior, 41, 621–623.
Gong, L., Kostrzewa, R. M., Fuller, R. W., & Perry, K. W. (1992). Supersensitization of the oral response to SKF 38393 in neonatal 6-OHDA-lesioned rats is mediated through a serotonin system. The Journal of Pharmacology and Experimental Therapeutics, 261, 1000–1007.
Gong, L., Kostrzewa, R. M., Perry, K. W., & Fuller, R. W. (1993). Dose-related effects of a neonatal 6-OHDA lesion on SKF-38393- and m-chlorophenylpiperazine-induced oral activity responses of rats. Developmental Brain Research, 76, 233–238.
Gong, L., Kostrzewa, R. M., & Li, C. (1994). Neonatal 6-hydroxydopamine and adult SKF 38393 treatments alter dopamine D1 receptor mRNA levels: Absence of other neurochemical associations with the enhanced behavioral responses of lesioned rats. Journal of Neurochemistry, 63, 1282–1290.
Gunne, L. M., & Häggström, J. E. (1983). Reduction of nigral glutamic acid decarboxylase in rats with neuroleptic-induced oral dyskinesia. Psychopharmacology, 81, 191–194.
Gunne, L. M., Growdon, J., & Glaeser, B. (1982). Oral dyskinesia in rats following brain lesions and neuroleptic drug administration. Psychopharmacology, 77, 134–139.
Huang, N.-Y., Kostrzewa, R. M., Li, C., Perry, K. W., & Fuller, R. W. (1997). Persistent spontaneous oral dyskinesias in haloperidol-withdrawn rats neonatally lesioned with 6-hydroxydopamine: Absence of an association with the Bmax for [3H]raclopride binding to neostriatal homogenates. The Journal of Pharmacology and Experimental Therapeutics, 280, 268–276. https://www.ninds.nih.gov/Disorders/All-Disorders/Tardive-Dyskinesia-Information-Page (last date of access 2 August 2021)
Iversen, S. D., Howells, R. B., & Hughes, R. P. (1980). Behavioral consequences of long-term treatment with neuroleptic drugs. Advances in Biochemical Psychopharmacology, 24, 305–313.
Jeste, D. V., & Caligiuri, M. P. (1993). Tardive dyskinesia. Schizophrenia Bulletin, 19, 303–315.
Johansson, P., Levin, E., Gunne, L., & Ellison, G. (1987). Opposite effects of a D1 and D2 agonist on oral movements in rats. European Journal of Pharmacology, 134, 83–88.
Kane, J. M., Woerner, M., & Lieberman, J. (1985). Tardive dyskinesia: Prevalence, incidence, and risk factors. Psychopharmacology. Supplementum, 2, 72–78.
Keepers, G. A., Fochtmann, J., Anzia, J. M., Benjamin, S., Lyness, J. M., Mojtabai, R., Servis, M., Walaszek, A., Buckley, P., Lenzenweger, M. F., Young, A. S., Degenhardt, A., & Hong, S. H. (2020). Systematic Review. Americal Journal of Psychiatry, 177(9), 868–872.
Kish, S. J., Shannak, K., Rajput, A., Deck, J. H., & Hornykiewicz, O. (1992). Aging produces a specific pattern of striatal dopamine loss: Implications for the etiology of idiopathic Parkinson’s disease. Journal of Neurochemistry, 58, 642–648.
Knable, M. B., Hyde, T. M., Egan, M. F., Tosayali, M., Wyatt, R. J., & Kleinman, J. E. (1994). Quantitative autoradiography of striatal dopamine D1, D2 and re-uptake sites in rats with vacuous chewing movements. Brain Research, 646, 217–222.
Koshikawa, N., Aoki, S., Tomiyama, M., Maruyama, Y., & Kobayashi, M. (1987). Sulpiride injection into the dorsal striatum increases methamphetamine-induced gnawing in rats. European Journal of Pharmacology, 133, 119–125.
Kostrzewa, R. M. (1995). Dopamine receptor supersensitivity. Neuroscience and Biobehavioral Reviews, 19, 1–17.
Kostrzewa, R. M., & Brus, R. (1991). Ontogenic homologous supersensitization of quinpirole-induced yawning in rats. Pharmacology, Biochemistry, and Behavior, 39, 517–519.
Kostrzewa, R. M., & Gong, L. (1991). Supersensitized D1 receptors mediate enhanced oral activity after neonatal 6-OHDA. Pharmacology, Biochemistry, and Behavior, 39, 677–682.
Kostrzewa, R. M., & Hamdi, A. (1991). Potentiation of spiroperidol induced oral activity in rats after neonatal 6 hydroxydopamine. Pharmacology, Biochemistry, and Behavior, 38, 215–218.
Kostrzewa, R. M., & Neely, D. (1993). Enhanced pilocarpine-induced oral activity responses in neonatal 6-OHDA-treated rats. Pharmacology, Biochemistry, and Behavior, 45, 737–740.
Kostrzewa, R. M., Brus, R., Perry, K. W., & Fuller, R. W. (1993). Age-dependence of a 6-hydroxydopamine lesion on SKF 38393- and m-chlorophenylpiperazine-induced oral activity responses of rats. Developmental Brain Research, 76, 87–93.
Kostrzewa, R. M., Reader, T. A., & Descarries, L. (1998). Serotonin neural adaptations to ontogenetic loss of dopamine neurons in rat brain. Journal of Neurochemistry, 70, 889–898.
Kostrzewa, R. M., Kostrzewa, J. P., & Brus, R. (2003). Dopamine receptor supersensitivity: An outcome and index of neurotoxicity. Neurotoxicity Research, 5, 111–118.
Kostrzewa, R. M., Huang, N.-Y., Kostrzewa, J. P., Nowak, P., & Brus, R. (2007). Modeling tardive dyskinesia: Predictive 5-HT 2C receptor antagonist treatment. Neurotoxicity Research, 11, 41–50.
Kostrzewa, R. M., Kostrzewa, J. P., Brown, R., Nowak, P., & Brus, R. (2008). Dopamine receptor supersensitivity: Development, mechanisms, presentation, and clinical applicability. Neurotoxicity Research, 14, 121–128.
Levin, E. D., See, R. E., & South, D. (1989). Effects of dopamine D1, D2 receptor antagonists on oral activity in rats. Pharmacology, Biochemistry, and Behavior, 34, 43–48.
Lloyd, K. G., Willigens, M. T., & Goldstein, M. (1985). Induction and reversal of dopamine dyskinesia in rat, cat, and monkey. Psychopharmacology. Supplementum, 2, 200–210.
Mithani, S., Atmadja, S., Baimbridge, K. G., & Fibiger, H. C. (1987). Neuroleptic-induced oral dyskinesias: Effects of progabide and lack of correlation with regional changes in glutamic acid decarboxylase and choline acetyltransferase activities. Psychopharmacology, 93, 94–100.
Molloy, A. G., & Waddington, J. L. (1987). Assessment of grooming and other behavioural responses to the D1 dopamine receptor agonist SKF38393 and its R- and S-enantiomers in the intact adult rat. Psychopharmacology (Berlin), 92, 164–168.
Molloy, A. G., & Waddington, J. L. (1988). Behavioural responses to the selective D1-dopamine receptor agonist R-SK&F 38393 and the selective D2-agonist RU 24213 in young compared with aged rat. British Journal of Pharmacology, 95, 335–342.
Mrini, A., Soucy, J.-P., Lafaille, F., Lemoine, P., & Descarries, L. (1995). Quantification of the serotonin hyperinnervation in adult rat neostriatum after neonatal 6-hydroxydopamine lesion of nigral dopamine neurons. Brain Research, 669, 303–308.
Murray, A. M., & Waddington, J. L. (1989). The induction of grooming and vacuous chewing by a series of selective D-1 dopamine receptor agonists: Two directions of D-1:D-2 interaction. European Journal of Pharmacology, 160, 377–387.
Plech, A., Brus, R., Kalbfleisch, J. H., & Kostrzewa, R. M. (1995). Enhanced oral activity responses to intrastriatal SKF 38393 and m-CPP are attenuated by intrastriatal mianserin in neonatal 6-OHDA-lesioned rats. Psychopharmacology, 119, 466–473.
Radja, F., Descarries, L., Dewar, K. M., & Reader, T. A. (1993). Serotonin 5-HT1 and 5-HT2 receptors in adult rat brain after neonatal destruction of nigrostriatal dopamine neurons: A quantitative autoradiographic study. Brain Research, 606, 273–285.
Ricciardi, L., Pringsheim, T., Barnes, T. R. E., Martino, D., Gardner, D., Remington, G., Addington, D., Morgante, F., Poole, N., Carson, A., & Edwards, M. (2019). Treatment Recommendations for Tardive Dyskinesia. Canadian Journal of Psychiatry, 64, 388–399.
Rosengarten, H., Schweitzer, J. W., & Friedhoff, A. J. (1983). Induction of oral dyskinesias in naïve rats by D1 stimulation. Life Sciences, 33, 2479–2482.
Rosengarten, H., Schweitzer, J. W., Egawa, J., & Friedhoff, A. J. (1986a). Diminished D2 dopamine receptor function and the emergence of repetitive jaw movements. Advances in Experimental Medicine and Biology, 235, 159–167.
Rosengarten, H., Schweitzer, J. W., & Friedhoff, A. J. (1986b). Selective dopamine D2 receptor reduction enhances a D1 mediated oral dyskinesia. Life Sciences, 39, 29–35.
Rupniak, N. M., Jenner, P., & Marsden, C. D. (1983). Cholinergic manipulation of perioral behaviour induced by chronic neuroleptic administration to rats. Psychopharmacology, 79(2–3), 226–230.
Rupniak, N. M. J., Jenner, P., & Marsden, C. D. (1985). Pharmacological characterization of spontaneous or drug-associated purposeless chewing movements in rats. Psychopharmacology, 85, 71–79.
Saifee, T. A., & Edwards, M. J. (2011). Tardive movement disorders: A practical approach. Practical Neurology, 11, 341–348.
Salamone, J. D., Johnson, C. J., McCullough, L. D., & Steinpreis, R. E. (1990). Lateral striatal cholinergic mechanisms involved in oral motor activities in the rat. Psychopharmacology, 102, 529–534.
Snyder, A. M., Zigmond, M. J., & Lund, R. D. (1986). Sprouting of serotonergic afferents into striatum after dopamine depleting lesions in infant rats: A retrograde transport and immunocytochemical study. The Journal of Comparative Neurology, 245, 274–281.
Tamminga, C. A., Crayton, J. W., & Chase, T. N. (1979). Improvement in tardive dyskinesia after muscimol therapy. Archives of General Psychiatry, 36, 595–598.
Tarsy, D., Lungu, C., & Baldessarini, R. J. (2011). Epidemiology of tardive dyskinesia before and during the era of modern antipsychotic drugs. Handbook of Clinical Neurology, 100, 601–616.
Waddington, J. L. (1990). Spontaneous orofacial movements induced in rodents by very long-term neuroleptic drug administration: Phenomenology, pathophysiology and putative relationship to tardive dyskinesia. Psychopharmacology (Berlin), 101, 431–447.
Waddington, J. L., & Gamble, S. J. (1980). Neuroleptic treatment for a substantial proportion of adult life: Behavioral sequelae of 9 months haloperidol administration. European Journal of Pharmacology, 67, 363–369.
Waddington, J. L., Cross, A. J., Gamble, S. J., & Bourne, R. C. (1983). Spontaneous orofacial dyskinesia and dopaminergic function in rats after 6 months of neuroleptic treatment. Science, 220, 530–532.
Acknowledgments
This work underlying this chapter was supported by Grant NS 29505 from the National Institute of Neurological Disorders and Stroke.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this entry

Cite this entry
Kostrzewa, R.M., Brus, R., Kostrzewa, J.P. (2022). Tardive Dyskinesia: Outcome of Antipsychotic Treatment and Brain Damage?. In: Kostrzewa, R.M. (eds) Handbook of Neurotoxicity. Springer, Cham. https://doi.org/10.1007/978-3-031-15080-7_163
Download citation
DOI: https://doi.org/10.1007/978-3-031-15080-7_163
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-15079-1
Online ISBN: 978-3-031-15080-7
eBook Packages: Biomedical and Life SciencesReference Module Biomedical and Life Sciences