
Abstract
Construction workers can be exposed to fibres, dust, and other toxic particles that can cause pneumoconiosis from silica, asbestos, and mixed dust. This systematic review aims to analyse how pneumoconiosis caused by exposure to dust contributed to the rise of occupational diseases in construction workers from 2001 to 2021. Sixteen keywords were combined to perform the search in six databases. Were included 26 articles which fulfilled all the defined inclusion criteria. A global analysis of risk disease distribution shows that exposures to mixed dust (41.1%), silica (37.5%) and asbestos (21.4%) were related to pneumoconiosis. In addition, individual analysis revealed that pneumoconiosis caused by exposure to chemical agents (silica, asbestos, and their dust) in the construction industry are predominantly related to the exposure to silica (Silicosis 38.1%), asbestos (asbestosis 33.3%, lung cancer 33.3%), and mixed dust (lung cancer 21.7%). Mixed dust seems to be the source of the highest incidence of pneumoconiosis, silica associated with silicosis is the most frequent disease.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
The construction industry is related to the mining industry, i.e., in extracting sand and stones as aggregates and subjecting workers to exposure to mixed dust (Agioutanti et al. 2020; Sauvé 2015). Several authors mention pneumoconiosis originated from occupational exposure to dust and fibres as one of the work-related diseases in the construction industry (Stocks et al. 2011; Sauvé 2015; Cummings et al. 2019; Bell and Mazurek 2020). These dusts, derived from different minerals such as silica and asbestos, are suspended in the air, resulting in diseases such as silicosis and asbestosis (Stocks et al. 2011; Nelson et al. 2011; Sauvé 2015; Nicol et al. 2015; Walters et al. 2018). Also the mineral nanoparticles are very toxic. They enter the body and can affect several vital mechanisms through blood circulation (Ophir et al. 2019; Bajpayee et al. 2004). In a comparative study on pneumoconiosis between China, Australia, and the United States, it was observed that China lags in studying health concerning safety. This lag is due to companies’ emphasis on eliminating work accidents with visible consequences rather than invisible causes such as pneumoconiosis diseases (Han et al. 2018). Between 2001 and 2016 in the United Kingdom, in the Birmingham region, Occupational Lung Disease Services (OLDS) conducted a study to assess the prevalence of pneumoconiosis from asbestos in various industries. There were 160 cases found, of which 71 (44%) were from the construction industry (Walters et al. 2018). Due to the long incubation period, patients with asbestosis were detected only after working in construction for 25, 30 or 40 years (Philteos et al. 2004). However, exposure to silica, asbestos, and mixed dust, forces companies to have greater attention to mitigating health effects considered incurable and characteristics suggestive of asbestosis disease that can impair worker performance, such as oxidative stress, fibrotic degeneration of lung tissue, complexation iron, apoptosis, and inflammation (Chong et al. 2006; Perret et al. 2017; Schmajuk et al. 2019). Likewise, asbestos, silica, and mixed dust were considered risk factors for pneumoconiosis in a study about Global Burden diseases (GBD 2016) and Risk Factors Collaborators (RFC 2016). The WHO/ILO (World Health Organization/International Labour Organization) in 2018 presented a systematical review protocol that designed quantitative studies on the prevalence of pneumoconiosis attributed to risk factors. This study was about the chemical agents (asbestos, silica, and mixed dust) from 1960 to 2018 among the working-age population and disaggregated by country, sex, age, and industrial sector occupation, including the construction industry (Mandrioli et al. 2018; Hall et al. 2020; Kurth et al. 2020; Dhatrak and Nandi 2020).
To investigate pneumoconiosis, it is necessary to consider confounding factors in the manifestation of the disease, such as age, sex, biomass, smoking, tuberculosis, socioeconomic status, pathological conditions and type of work (Han et al. 2017). In addition, the permissible exposure limit (PEL) for free silica was established to prevent the development of the disease. Several studies noted significant differences (Liu et al. 2017). Some of them were set by OSHA and ACGIH (Linch 2002; Dhatrak and Nandi 2020). For identifying pneumoconiosis, an exposure questionnaire (Ben Saad et al. 2013), spirometry tests (Prasad et al. 2020; Quanjer et al. 2012) and chest X-rays were also suggested to check rounded or irregular opacities, especially in the upper and lower lung fields (Han et al. 2018; Baur 2020; Dhatrak and Nandi 2020). Other authors suggest post-mortem pathophysiological diagnoses of lung tissue (Naidoo et al. 2005; Ndlovu et al. 2016).
This review focuses on pneumoconiosis resulting from exposure to workplace chemical agents such as silica, asbestos, and mixed dust. Some studies which have been visited recognise that silica, asbestos, and mixed dust are risk factors for pneumoconiosis in the construction industry. So, the present systematic literature review (SLR) intends to answer the following questions:
To what extent does the prevalence of pneumoconiosis contribute to illness in civil construction between 2001 and 2021?
Which chemical agent has the greatest weight in the prevalence of pneumoconiosis?
2 Materials and Methods
The research used the PRISMA Statement (Page et al. 2021). The information to compose the research was extracted from six electronic academic databases: Scopus; Ovid Medline with Daily Update; OSH update; Web of Science; EMBASE; and PubMed. Cited references were extracted using keywords related to the topic. A checklist was created to facilitate the analysis of the results, considering the following items: the authors’ surnames and publication year, prevalence of pneumoconiosis, exposure to chemical agents, i.e., exposure to silica, asbestos and/or mixed dust, and the disease(s) derived from chemical agents. After selecting the articles related to the construction industry, the authors included pneumoconiosis papers related to other sectors, such as mining, to compare data and results.
2.1 Search Strategy
The strategy used in data extraction was based on a 20-year time horizon (2001–2021). “Data were extracted from works published between January 2001 and December 2021,” taking into account title contents, abstracts, and keywords of all articles retrieved from the six databases. The following keywords have been considered, using the booleans “OR” and “AND”: [(construction AND asbestos); OR (construction AND silica) OR (asbestos AND mixed dust)]; [(concrete AND asbestos) OR (silica AND mixed dust)]; [(occupational lung disease AND construction)]; [(permissible exposure limit AND silica) OR (construction industry AND mixed dust)]; [(pneumoconiosis AND construction)]; [(abrasive blasting AND silicosis) OR (pneumoconiosis AND asbestosis)]; [(pneumoconiosis AND spirometry)]; [(chest r-x AND pneumoconiosis) OR (asbestos AND mixed dust)]; (construction AND accidents); (pneumoconiosis AND accidents). The asterisk symbol was used to ensure that all possible variations of the terms were considered.
Data were extracted using a standard form developed in Excel to organise and compare information from the articles.
To be included/excluded in this review, studies had to meet the following criteria: experimental random or observational analytical studies focused on pneumoconiosis prevalence caused by silica, asbestos, and mixed dust in the construction industry or related activities with measurements (similar tasks of mining has been included). In addition, the articles need to have available full text and be written in English.
2.2 Data Analyses
The absolute frequencies of diseases in the included studies associated with exposure to at least one of the chemical agents (silica, asbestos and mixed dust) as well as the associated risk factor were sought.
The determination of the absolute and relative frequencies and the verification of the level of prevalence, in percentage, was through the following equation:
where:
-
fi—(absolute frequency) shows how many times the disease appeared for each article reviewed according to its risk factor;
-
N—refers to the total number of diseases associated with a risk factor;
-
fr—(relative frequency) shows the impact number converted into a percentage.
3 Results
3.1 Study Selection and Characteristics
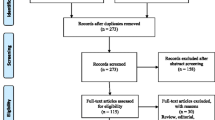
A comprehensive selection of studies was carried out in this systematic review, using the six databases and observing the inclusion/exclusion criteria referred to in the methodology. A total of 1823 records were screened, 1357 of which were removed because they were duplicates, incomplete, not peer-reviewed, not published in scientific journals, or off-topic. Were screened 466 articles having these been removed 440 because they did not correspond to the period under study (2001–2021), had contradictory objectives, or were not written in English. There were found 26 articles considered eligible (Fig. 1). The extracted information is summarised in Table 1.

Study screening diagram (Page et al. 2021)
3.2 Distribution of Diseases According to Exposure Agent
The construction industry involves a wide range of activities, such as stone-breaking, concrete or brick cutting, pipe cutting, abrasive blasting, and tunnelling (Wang and Meng 2018). Exposure to crystalline silica, asbestos and mixed dust (risk factor) develops silicosis and asbestosis. Mixed dust is a blend of minerals, and it has the potential to cause pneumoconiosis (Nelson et al. 2010). A statistical analysis has been performed with the compiled data from items and characteristics described in Table 2. Moreover, diseases associated with different risk factors can be identified. Note that a disease may be associated with more than one risk factor.
The comparison of prevalence was represented by the absolute and relative frequencies of each type of disease caused by the three chemical agents: silica, asbestos and mixed dust.
Regarding the global analysis of the disease distribution in relation to pneumoconiosis, is noted: silica (37.5%), asbestos (21.4%), and mixed dust (41.1%). Obtained through the relative frequencies of the diseases of each agent divided by the total occurrence of the diseases (56%).
Analysing the occurrence of individualised diseases in relation to their risk agent, the following higher frequencies are noted: silica for (Silicosis 38.1%); asbestos for (asbestosis and lung cancer 33.3%), and mix dust for (lung cancer 21.7%) Table 2.
3.3 Permissible Exposure Limit
The literature review shows the need to establish an exposure limit value, given the risk factors for pneumoconiosis in the mining and construction industries (Hall et al. 2020). Despite the effort involving several organisations that deal with workers’ health, there has been no consensus on standardising exposure values.
Whether due to the continuous exposure to risk factors or too high values of the Permissible Exposure Limit (PEL) (Liu et al. 2017), there are differences in standard levels of silica compared to those recommended by Occupational Safety and Health (OSH) and international organisations in several countries, (Linch 2002; Dhatrak and Nandi 2020) (Fig. 3). The two values corresponding to the United States belong to NIOSH (0.05 mg/m3) and MSHA (0.10 mg/m3). China values vary according to the type of ore, from 0.07 to 0.35 mg/m3. There is currently a difference in exposure values in countries such as India, France, and Portugal, contributing to the prevalence of diseases related to pneumoconiosis, Fig. 2.

Permissible exposure limit depending on the country (Linch 2002)
4 Discussion
The prevalence of pneumoconiosis in the construction industry has been studied since the last century (Linch 2002; Higgins et al. 2011; Sauvé 2015; Mandrioli et al. 2018; FCL 2021). In addition, there were studies on asbestos, silica, and mixed dust considered the risk factor for occupational pneumoconiosis, responsible for 100% of this disease (GBD 2016; RFC 2016). Review shows that exposure to chemical agents (silica, asbestos, and mixed dust) are responsible for diseases such as; Silicosis, asbestosis, lung cancer, chronic pulmonary obstructive diseases, moderate to marked emphysema, mixed dust pneumoconiosis, unknown pneumoconiosis, pulmonary tuberculosis, and progressive massive fibrosis (PMF) Tables 1 and 2. These diseases are associated with causes of pneumoconiosis morbidity and mortality in the construction industry due to dust and fibres (Stocks et al. 2011; Agioutanti et al. 2020).
Based on the global review analyse, Table 2, it is noted that mixed dust has a higher frequency of diseases with 41.1%. This can be justified by the presence of two elements together, namely silica and asbestos, forming a compound, joining the diseases of each element (Baur 2020). Then, silica with 37.5% and asbestos with 21.7% caused a long latency fibrotic lung diseases/pneumoconiosis (Stocks et al. 2011; Walters et al. 2018), referenced in Table 2. There is a long latency period for these diseases and a lack of health care for workers in the construction industry. These two factors make employers decline their responsibility (Ndlovu et al. 2016). In pneumoconiosis, workers may have signs of pulmonary dysfunction (pneumoconiosis) 20, 30, 40 or more years after leaving the company. Few studies have shown shorter times (Philteos et al. 2004; Nicol et al. 2015). The individual analysis of the maximum frequencies of diseases related to exposure to the three chemical agents supports the prevalence of pneumoconiosis in the construction industry with the following values: silica (Silicosis 38.1%), asbestos (asbestosis and lung cancer 33.3% both); and mixed dust (lung cancer 21.7%). Although the research shows evidence of pneumoconiosis from silicosis in the mines (Bajpayee et al. 2004; Stocks et al. 2011; Dhatrak and Nandi 2020; Baur 2020), the higher values of silicosis concerning asbestos and mixed dust referred to in Table 2, can support its impact on the construction industry. Knowledge of the risk factors with the most significant impact on the work environment helps identify the causes and, consequently, implement preventive and corrective actions (Bell and Mazurek 2020).
More evidence was seen at the South African Conference on silicosis analysis over 75 years. It was found that silica still affects 19% of construction industry workers (Sauvé 2015). The presence of different levels of exposure in many countries may influence the pneumoconiosis prevalence value (Fig. 2). Exposure Limit Values are not the same in all countries, although there are international organisations that seek to establish a common value for all countries. The existence of different limits influences the value of the prevalence of pneumoconiosis (Linch 2002; Dhatrak and Nandi 2020).
Construction industry workers are subject to the use and handling of products and machines such as explosive pressure vessels, explosives and breakers, machines and loaders, mixed dust, silica and asbestos (Baur 2020; Agioutanti et al. 2020). Proposals to combat pneumoconiosis were suggested, from preventive (work education) and corrective actions, which can be added using diagnosis like exposure questionnaires, spirometry (Prasad et al. 2020), chest X-ray (Dhatrak and Nandi 2020), Computer Tomographic (CT), and Magnetic Tomography Imaging (Ben Saad et al. 2013).
5 Conclusion
After the present literature review, 26 articles were considered eligible. The research shows that the prevalence of pneumoconiosis in the construction industry is due to the raw materials containing chemical elements considered risk factors, namely silica, asbestos and mixed dust. In the global analysis of the risk factors for pneumoconiosis, it was found that mixed dust is responsible for the higher frequency of pneumoconiosis (41.1%), followed by silicosis and asbestosis with 37.5% and 21.7%, respectively. In the individual analysis of the diseases, silicosis is observed more frequently, with 38.1% associated with silica, followed by asbestosis and lung cancer with 33.3% both related to asbestos and mixed dust with lung cancer (21.7%). In conclusion, the three risk factors contribute to diseases that cause pneumoconiosis; mixed dust has the highest number of diseases, while silicosis is the most frequently associated with silica.
References
Agioutanti, E., Keles, C., Sarver, E.: A thermogravimetric analysis application to determine coal, carbonate, and non-carbonate minerals mass fractions in respirable mine dust. J. Occup. Environ. Hyg. 17(2–3), 47–58 (2020). https://doi.org/10.1080/15459624.2019.1695057
Bajpayee, T.S., Rehak, T.R., Mowrey, G.L., Ingram, D.K.: Blasting injuries in surface mining with emphasis on flyrock and blast area security. J. Saf. Res. 35(1), 47–57 (2004). https://doi.org/10.1016/j.jsr.2003.07.003
Baur, X.: Diagnostic challenges of mixed dust silicosis (mixed dust pneumoconiosis)—5 case reports. Pneumologie 74(3), 159–172 (2020). https://doi.org/10.1055/a-1087-7229
Bell, J.L., Mazurek, J.M.: Trends in pneumoconiosis deaths—United States, 1999–2018. MMWR. Morb. Mortal. Wkly. Rep. 69(23), 693–698 (2020). https://doi.org/10.15585/mmwr.mm6923a1
Ben Saad, H., El Attar, M.N., Hadj Mabrouk, K., Ben Abdelaziz, A., Abdelghani, A., Bousarssar, M., Limam, K., Maatoug, C., Bouslah, H., Charrada, A., Rouatbi, S.: The recent multi-ethnic global lung initiative 2012 (GLI2012) reference values don’t reflect contemporary adult’s North African spirometry. Respir. Med. 107(12), 2000–2008 (2013). https://doi.org/10.1016/j.rmed.2013.10.015
Chong, S., Lee, K.S., Chung, M.J., Han, J., Kwon, O.J., Kim, T.S.: Pneumoconiosis: comparison of imaging and pathologic. Radiographics 26(1), 59–77 (2006). https://doi.org/10.1148/rg.261055070
Cummings, K.J., Johns, D.O., Mazurek, J.M., Hearl, F.J., Weissman, D.N.: NIOSH’s respiratory health division: 50 years of science and service. Arch. Environ. Occup. Health 74(1–2), 15–29 (2019). https://doi.org/10.1080/19338244.2018.1532387
Dhatrak, S., Nandi, S.: Assessment of silica dust exposure profile in relation to prevalence of Silicosis among Indian sandstone mine workers: need for review of standards. Am. J. Ind. Med. 63(3), 277–281 (2020). https://doi.org/10.1002/ajim.23077
Fundación Laboral de la Construcción: Trabajos con exposición a SCR: implicaciones asociadas a su consideración como agente cancerígeno en el RD 665/1997, p. 18 (2021). http://www.gotowebinar.com/
GBD 2016 Risk Factors Collaborators: Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 390(10100), 1345–1422 (2017).https://doi.org/10.1016/S0140-6736(17)32366-8
Higgins, J.P.T., Green, S., Collaboration, C.: Cochrane Handbook for Systematic Reviews of Interventions. Wiley Online Library (2008)
Higgins, J.P.T., Green, S., (eds.): Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. 2011 The Cochrane Collaboration (2011). Available from http://handbook.cochrane.org. Updated March 2011
Hall, N.B., Halldin, C.N., Blackley, D.J., Laney, A.S.: Assessment of pneumoconiosis in surface coal miners after implementation of a national radiographic surveillance program, United States, 2014–2019. Am. J. Ind. Med. (2020). https://doi.org/10.1002/ajim.23184
Han, L., Gao, Q., Yang, J., Wu, Q., Zhu, B., Zhang, H., Ding, B., Ni, C.: Survival analysis of coal workers’ pneumoconiosis (CWP) patients in a state-owned mine in the east of China from 1963 to 2014. Int. J. Environ. Res. Public Health 14(5) (2017). https://doi.org/10.3390/ijerph14050489
Han, S., Chen, H., Harvey, M.A., Stemn, E., Cliff, D.: Focusing on coal workers’ lung diseases: a comparative analysis of China, Australia, and the United States. Int. J. Environ. Res. Public Health 15(11) (2018). https://doi.org/10.3390/ijerph15112565
Kurth, L., Laney, A.S., Blackley, D.J., Halldin, C.N.: Prevalence of spirometry-defined airflow obstruction in never-smoking working US coal miners by pneumoconiosis status. Occup. Environ. Med. 77(4), 265–267 (2020). https://doi.org/10.1136/oemed-2019-106213
Leonard, R., Zulfikar, R., Stansbury, R.: Coal mining and lung disease in the 21st century. Curr. Opin. Pulm. Med. 26(2), 135–141 (2020). Lippincott Williams and Wilkins, https://doi.org/10.1097/MCP.0000000000000653
Linch, K.D.: Respirable concrete dust-silicosis hazard in the construction industry. Appl. Occup. Environ. Hyg. 17(3), 209–221 (2002). https://doi.org/10.1080/104732202753438298
Liu, Y., Zhou, Y., Hnizdo, E., Shi, T., Steenland, K., He, X., Chen, W.: Total and cause-specific mortality risk associated with low-level exposure to crystalline silica: a 44-year cohort study from China. Am. J. Epidemiol. 186(4), 481–490 (2017). https://doi.org/10.1093/aje/kwx124
Mandrioli, D., Schlünssen, V., Ádám, B., Cohen, R.A., Colosio, C., Chen, W., Fischer, A., Godderis, L., Göen, T., Ivanov, I.D., Leppink, N., Mandic-Rajcevic, S., Masci, F., Nemery, B., Pega, F., Prüss-Üstün, A., Sgargi, D., Ujita, Y., van der Mierden, S., Scheepers, P.T.J., et al.: WHO/ILO work-related burden of disease and injury: protocol for systematic reviews of occupational exposure to dusts and/or fibres and of the effect of occupational exposure to dusts and/or fibers on pneumoconiosis. Environ. Int. 119, 174–185 (2018). Elsevier Ltd., https://doi.org/10.1016/j.envint.2018.06.005
Miller, M.R., Hankinson, J., Brusasco, V., Burgos, F., Casaburi, R., Coates, A., Crapo, R., Enright, P., van der Grinten, C.P.M., Gustafsson, P., Jensen, R., Johnson, D.C., MacIntrye, N., McKay, R., Navajas, D., Pedersen, O.F., Pellegrino, R., Viegi, G., Wagner, J.: Standardisation of spirometry. Eur. Respir. J. 26(2), 319–338 (2005). https://doi.org/10.1183/09031936.05.00034805
Naidoo, R.N., Robins, T.G., Murray, J.: Respiratory outcomes among South African coal miners at autopsy. Am. J. Ind. Med. 48(3), 217–224 (2005). https://doi.org/10.1002/ajim.20207
Ndlovu, N., Nelson, G., Vorajee, N., Murray, J.: 38 years of autopsy findings in South African mineworkers. Am. J. Ind. Med. 59(4), 307–314 (2016). https://doi.org/10.1002/ajim.22574
Nelson, G., Girdler-Brown, B., Ndlovu, N., Murray, J.: Three decades of Silicosis: disease trends at autopsy in South African gold miners. Environ. Health Perspect. 118(3), 421–426 (2010). https://doi.org/10.1289/ehp.0900918
Nelson, G., Murray, J., Phillips, J.I.: The risk of asbestos exposure in South African diamond mine workers. Ann. Occup. Hyg. 55(6), 569–577 (2011). https://doi.org/10.1093/annhyg/mer028
Nicol, L.M., McFarlane, P.A., Hirani, N., Reid, P.T.: Six cases of Silicosis: implications for health surveillance of stonemasons. Occup. Med. 65(3), 220–225 (2015). https://doi.org/10.1093/occmed/kqu209
Ophir, N., Bar Shai, A., Korenstein, R., Kramer, M.R., Fireman, E.: Functional, inflammatory, and interstitial impairment due to artificial stone dust ultrafine particles exposure. Occup. Environ. Med. 76(12), 875–879 (2019). https://doi.org/10.1136/oemed-2019-105711
Page, M.J., McKenzie, J.E., Bossuyt, P.M., Boutron, I., Hoffmann, T.C,. Mulrow, C.D., et al.: The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71 (2021). https://doi.org/10.1136/bmj.n71
Perret, J.L., Plush, B., Lachapelle, P., Hinks, T.S.C., Walter, C., Clarke, P., Irving, L., Brady, P., Dharmage, S.C., Stewart, A.: Coal mine dust lung disease in the modern era. Respirology 22(4), 662–670 (2017). https://doi.org/10.1111/resp.13034
Prasad, S.K., Singh, S., Bose, A., Prasad, B., Banerjee, O., Bhattacharjee, A., Maji, B.K., Samanta, A., Mukherjee, S.: Association between duration of coal dust exposure and respiratory impairment in coal miners of West Bengal, India. Int. J. Occup. Saf. Ergon. (2020). https://doi.org/10.1080/10803548.2020.1742463
Philteos, G.S.R., Coverett, K., Chibbar, R., Ward, H.A., Cockcroft, D.W.: Asbestosis and probable microscopic polyangiitis. Can. Respir. J. 11(5), 359–362 (2004). https://doi.org/10.1155/2004/341942
Quanjer, P.H., Stanojevic, S., Cole, T.J., Baur, X., Hall, G.L., Culver, B.H., Enright, P.L., Hankinson, J.L., Ip, M.S.M., Zheng, J., Stocks, J., Schindler, C.: Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur. Respir. J. 40(6), 1324–1343 (2012). https://doi.org/10.1183/09031936.00080312
Sauvé, J.F.: Historical and emerging workplaces affected by silica exposure since the 1930 Johannesburg conference on silicosis, with special reference to construction. Am. J. Ind. Med. 58, 67–71 (2015). https://doi.org/10.1002/ajim.22507
Schmajuk, G., Trupin, L., Yelin, E., Blanc, P.D.: Prevalence of arthritis and rheumatoid arthritis in coal mining counties of the United States. Arthritis Care Res. 71(9), 1209–1215 (2019). https://doi.org/10.1002/acr.23874
Stocks, S.J., Turner, S., Mcnamee, R., Carder, M., Hussey, L., Agius, R.M.: Occupation and work-related ill-health in UK construction workers. Occup. Med. 61(6), 407–415 (2011). https://doi.org/10.1093/occmed/kqr075
Walters, G.I., Robertson, A.S., Bhomra, P.S., Burge, P.S.: Brief communication asbestosis is prevalent in a variety of construction industry trades. Primary Care Respir. Med. 28, 11 (2018). https://doi.org/10.1038/s41533-018-0078-6
Wang, X., Meng, F.-B.: Statistical analysis of large accidents in China’s coal mines in 2016. Nat. Hazards 92, 311–325 (2018)
Acknowledgements
This research was funded by the Doctoral Program in Occupational Safety and Health of the University of Porto, grant number demssogaa541344.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Andaque, G.A., de las Nieves González-García, M., Branco, J.C., Nunes, E., Guedes, J.C., Baptista, J.S. (2023). Prevalence of Pneumoconiosis in the Construction Industry: A Systematic Review. In: Arezes, P.M., et al. Occupational and Environmental Safety and Health IV. Studies in Systems, Decision and Control, vol 449. Springer, Cham. https://doi.org/10.1007/978-3-031-12547-8_51
Download citation
DOI: https://doi.org/10.1007/978-3-031-12547-8_51
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-12546-1
Online ISBN: 978-3-031-12547-8
eBook Packages: EngineeringEngineering (R0)