
Abstract
Different machine learning techniques and approaches were implemented to detect the features of COVID-19, from chest X-Ray and CT medical images, as well as to identify them from other similar human-being lungs infection diseases. In this work, Logistic Regression, Neural Networks, Random Forests, Decision Trees, kNN, and CN2 Rule Induction are the machine learning models and classifiers that were utilized to perform such detection and identification. The entire process according to the importance of good parameters selection, and such performance was presented and emphasized at different phases of models analysis and visualization. In our presented method, the achieved classification accuracies were up to 95.5%. Our work was implemented using Orange software, as a visual-based tool, and dedicated for physicians with no experience in machine learning algorithms and programming languages.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
The Coronavirus disease pandemic, a.k.a. COVID-19 by WHO (World Health Organization) [1], is world widely spread affecting many people in different countries. Since this virus does not have a well-known information as well as not match any similar symptoms that occur by other well-documented and knowledge-based viruses, medical concerns and emergency orders were firmly raised in many regions, e.g. schools and businesses closures as well as stay-home orders, to protect lives and eliminate the disease outbreak excessively as well. For that, hourly data collections regarding infected areas, communities, and people are continuously gathered, accumulated, and compiled to form visual representations of COVID-19 morbidness cases and their spreading in different zones.
From the scientific and engineering point of view, the machine learning algorithms and models can play a role in classifying and identifying the COVID-19 cases from other similar human-being lungs infection diseases, such as Bacterial Pneumonia, Viral Pneumonia, Pneumocystis, Streptococcus, and SARS, using chest X-Ray and CT (Computerized Tomography) medical images. Some researchers were able to have fairly classified results from such diagnostic images using different models of ImageNet deep learning classifiers [2, 3], as described in [4,5,6]. Alimadadi et al. stated how governments, research institutes, and technological companies issued an urgent call-to-action for AI (Artificial Intelligence) researchers to develop data mining techniques and build open-source real-time analytical datasets to fight the COVID-19 pandemic and stop its spreading. Such that, the collection of large real-time diagnostic datasets of COVID-19 cases can give a better understanding of the COVID-19 patterns and spreading, as well as improve the speed and accuracy of the medical analyses when such diagnostic datasets are integrated with machine learning algorithms [7]. Pinter et al. mentioned that due to the lack of necessarily diagnostically datasets collection, the epidemiological models were in challenge in the matter of higher accuracy delivery for a long-term prediction. They implemented the ANFIS (Adaptive Neural-Fuzzy Inference System) and MLP-ICA (Multi-Layer Perceptron-Imperialist Competitive Algorithm) as a hybrid machine learning algorithms approach to predict the time-series of the infected individuals and their mortality rates, using MATLAB’s ANFIS toolbox. Moreover, their work can be considered as an initial benchmarking tool for future research regarding the potential of machine learning algorithms in COVID-19 pandemic prediction [8]. In the paper of Elaziz et al., a new machine learning method was presented to classify the COVID-19 and non-COVID-19 cases using chest X-ray images. The features extracted from such images using the method of FrMEMs (Fractional Multichannel Exponent Moments) within a parallel workstation to accelerate the overall computational process. Their work was evaluated using two COVID-19 chest X-ray datasets that achieved accuracy rates of 96.09% and 98.09% for the first and second datasets, respectively [9]. Sujath et al. presented a model to predict the spread of COVID-19 in India, this approach was implemented using different machine learning models, such as Linear Regression, MLP, and Vector Autoregression using the COVID-19 Kaggle repository datasets for the epidemiological COVID-19 cases in India, only. Their work showed that the CI (Confidence Interval), a way of quantifying the uncertainty of estimated results, was 95% for the completely implemented machine learning models [10]. Ardabili et al. presented a comparative analysis of different machine learning models, such as MLP and ANFIS, and soft computing models, such as GA (Genetic Algorithm), PSO (Particle Swarm Optimization), and GWO (Grey Wolf Optimizer), to predict the COVID-19 outbreak and spreading. They demonstrated that the machine learning algorithms were effective tools and have more promising results than the soft computing models in the COVID-19 pandemic prediction [11]. Brinati et al. described the amplification of COVID-19 viral RNA using the rRT–PCR (real-time Reverse Transcription–Polymerase Chain Reaction) is the current gold standard test for COVID-19 infections confirmation. However, due to the rRT-PCR weaknesses, such as false-negative rates of 15–20%, and a potential shortage of reagents, therefore faster, less expensive, and more accessible testing methods, as alternative solutions, should be developed. Two machine learning models were implemented to classify patients as either positive or negative to the COVID-19 infection using the hematochemical values from the routine blood exams. In such two models, the accuracy ranges 82–86% and the sensitivity ranges 92–95% with respect to the gold standard test. Moreover, a Decision Tree model was implemented as straightforward simple decision assistance for the COVID-19 suspected cases [12]. Cheng et al. indicated that approximately 20–30% of COVID-19 infected cases need hospitalization, while 5–12% of them may require critical care in the ICU (Intensive Care Unit). In their work, they developed a machine learning algorithm, as a risk prioritization tool, using Random Forest model to predict the ICU requirements within the 24-h. Time-series information, laboratory data, vital signs, nursing valuations, and ECG (Electrocardiograms) signals were used as input datasets for this model. These datasets were randomly split into 70% of the training dataset and 30% of the test dataset. Then, this model was trained using the tenfold CV (Cross-Validation) technique. The model’s performance and prediction was evaluated on the test dataset, as the following: sensitivity of 72.8% (95% CI: 63.2–81.1%), specificity of 76.3% (95% CI: 74.7–77.9%), accuracy of 76.2% (95% CI: 74.6–77.7%), and Area under ROC of 79.9% (95% CI: 75.2–84.6%). Thus, this machine learning tool could improve the planning and the management of hospital resources in more effective ways regarding the COVID-19 patients’ hospitalization [13]. In the study of Rustam et al., different supervised machine learning models were implemented to forecast the number of patients infected by COVID-19. Four standard models, such as Linear Regression, Exponential Smoothing, LASSO (Least Absolute Shrinkage and Selection Operator), and SVM (Support Vector Machine), were developed to forecast the upcoming patients and results. The number of newly infected patients, the number of recovered patients in the next 10 days, and the number of deaths were the three prediction categories for each model. The Exponential Smoothing model had better forecasting results than the other models, followed by the Linear Regression model, and then the LASSO model performed well in forecasting the newly infected cases, recovery rate, and death rate. While the SVM model performed poorly in the three prediction categories. The three models were performed on the Johns Hopkins University's COVID-19 repository datasets [14].
2 Materials and Methods
A large set of diagnostic medical images of human-being lungs diseases, i.e. datasets, has to be publicly provided to the scientific communities, to achieve the valuable comparable results of identification and classification of COVID-19 cases. For this reason, many medical datasets [15, 16] have been already published to stop the COVID-19 outbreak using vast sets of technologies and applied approaches, e.g. machine learning algorithms. The aim of our work is to identify the best classifiers, within the best CA (Classification Accuracy) scores, that classify the COVID-19 infected cases from other human-being lungs infected cases. As well as to provide a convenient visual-based classification tool to physicians, without their need to understand the deep knowledge of machine learning algorithms, the programming languages, such as Python, the computational libraries, such as NumPy, Pandas, and scikit-learn, and the abstraction platforms, such as PyTorch and TensorFlow. Our work was fully designed, built, and implemented using the open-source machine learning and data visualization tool Orange, from the University of Ljubljana [17].
Orange provides data analysis, data visualization, statistical distributions, and vast sets of plotting tools, as well as its GUI (Graphical User Interface) allows the physicians to focus on data analysis and manipulating, instead of coding, to accelerate the diagnostically identification and classification workflows with ease. Our presented work with Orange was performed using the datasets that were provided by the Kaggle repository [15], and the workflow was categorized into four proposed phases: (1) Datasets Preparation Phase, (2) Training Dataset Operations Phase, (3) Test Dataset Operations Phase, and (4) Prediction and Performance Phase. Furthermore, seven machine learning algorithms were utilized, in this work, to have sufficient comparable decisions regarding the best-chosen model for the best classification accuracy to identify and classify the COVID-19 cases. These models are:
-
Distances that computes the distances between the rows and columns in the datasets, i.e. the cases [18, 19],
-
Logistic Regression that classifies the cases using the non-linear Sigmoid function (σ) [19, 20],
-
CN2 Rule Induction that uses efficient induction of simple and comprehensive rules in the form of (IF condition THEN predict case) to predict the cases [21, 22],
-
Tree that splits the cases into nodes and leaves by labeling purity and forward pruning [23, 24],
-
Random Forest that classifies the cases using an ensemble of decision trees [25, 26],
-
kNN (k-Nearest Neighbors) that searches for the k closest cases based on their features and their averages as classification factors [27, 28], and
-
Neural Network that classifies the cases within the MLP model using the backpropagation method [29].
Note that all the aforementioned algorithms are supervised classifiers, except the Distances, which is an unsupervised classifier.
Note that some of Orange's toolboxes have been renamed in purpose to match their underlying phases as well as their designated operations, for ease of follow and understanding.
2.1 Datasets Preparation Phase
The datasets were gathered from the chest X-Ray (of PA “Posteroanterior”, AP “Anteroposterior”, APS “AP Supine”, and L “Lateral” captures [30]) and CT (of Axial and Coronal scans [31]) medical images of COVID-19, SARS, Pneumocystis, and Streptococcus infection cases. Since the number of these gathered images is relatively small, the data augmentation technique is performed in this phase. The data augmentation was achieved by enlarging the size of each medical image, i.e. sample, in the datasets by increasing their (1) brightness by the factor of 16 and (2) contrast by the factor of 32, to have a sufficient number of samples. A sufficient number of samples yields a good identification and better classification accuracy judgment, as well as fulfills Hoeffding’s Inequality generalization bound [32]. For instance, to demonstrate Hoeffding’s Inequality, for any randomly selected size of N COVID-19 and non-COVID-19 samples, the generalization bound for the probability (\(P\left[\cdot \right]\)) of such an event for any tolerance (\(\epsilon >0\)) is as stated in Eq. (1):
where, \(\mu\) is the probability of the COVID-19 samples in a bin consisting of COVID-19 and non-COVID-19 samples, while \(v\) is the fraction of the selected COVID-19 samples among the non-COVID-19 samples. Note that Hoeffding’s Inequality formula mostly affects by how large N and the chosen \(\epsilon\) are.
The ACDSee® photo editing software was used to implement such data augmentation [33]. Note that other data augmentation methods, such as shape sheering, angles rotation, and flipping/mirroring, were not used in this phase, due to the fact that physicians usually check such diagnostic images in the normal straightway position, as portraits. For fast data processing, the samples were scaled uniformly to the dimensions of 128 × 128 pixels, and the resultant statistics of these samples are summarized in Table 1.
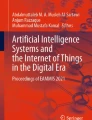
Figure 1 demonstrates the preparation phase of these datasets that consists of the following Orange toolboxes: (1) Import Images that loads the datasets locally, i.e. from the computer, (2) Image Viewer that visually checks the loaded datasets, (3) Adding Labels that generates the cases for each sample. Since these datasets are non-labeled and most of the classifiers are supervised, then a column of labels, i.e. classes, was generated regarding the samples’ filenames. Note that, each filename corresponds to an infected case name, for instance the filename of the “COVID-19-APSupine-Xray-1.jpeg” sample generates the “COVID-19” case as a label. (4) Whole Datasets that lists the whole labeled datasets, (5) Distributions that statistically displays the labeled datasets, and (6) Datasets Sampler that samples the whole labeled datasets into 70% of training dataset and 30% of test dataset, i.e. 209 training samples and 89 test samples.

Datasets preparation phase using orange toolboxes
For more illustration, Fig. 2 illustrates the Image Viewer and Adding Labels toolboxes of Orange.

Orange image viewer (left) and adding labels (right) toolboxes
Note that four labels were generated using Adding Labels toolbox with labels as COVID-19, Pneumocystis, SARS, and Streptococcus. Figure 3 shows the Whole Datasets toolbox of Orange

Orange whole datasets toolbox
Finally, Fig. 4 demonstrates the Distributions and Datasets Sampler toolboxes of Orange.

Orange distributions (left) and datasets sampler (right) toolboxes, the sampling percentage can be changed based on the model design and technical requirements
2.2 Training Dataset Phase
After the 209 samples, i.e. the training dataset, were received from the Datasets Sampler toolbox from the Datasets Preparation Phase, they can be buffered and visually checked along with their generated labels using the Training Dataset toolbox. Since these training samples contain no useful classifiable information, the Inception v3 Model (Training) toolbox is in need to represent this training dataset into its vectorized equivalent representations, a.k.a. features. This toolbox generates 2048 numerical features for each sample that makes the next classification processes more meaningful, and such features can be viewed using the Training Dataset Features toolbox of Orange. Note that the Inception v3 Model (Training) toolbox is based on Google’s Inception v3 CNN (Convolutional Neural Network) architecture [34] that is trained on ImageNet.
Then, these features along with their labels from the Inception v3 Model (Training) toolbox were fed to various machine learning classifiers for further identification and classification of training dataset based on their features (and labels, if they were supervised classifiers), as shown in Fig. 5. Note that, the calculated distances in the Distances classifier were visualized using the Hierarchical Clustering toolbox along with the Hierarchical Clustering Viewer toolbox, the generated rules in the CN2 Rule Induction classifier were viewed through the CN2 Rule Viewer toolbox, the generated tree with nodes and leaves in the Tree classifier were visualized using the Tree Viewer toolbox.

Training Dataset Operations Phase using Orange toolboxes, (left) the training dataset was fed from the first phase then propagated to the Inception v3 Model for features generating, (middle) predictions were calculated from the machine learning classifiers then forwarded to the fourth phase for classification accuracies, (right) and the distances, rules, and trees can be viewed through the viewers
2.3 Test Dataset Phase
After the 89 samples, i.e. the test dataset, were received from the Datasets Sampler toolbox from the Datasets Preparation Phase, they can be buffered and visually checked along with their labels using the Test Dataset toolbox, as shown in Fig. 6. Since these test samples contain no useful classifiable information, the Inception v3 Model (Test) toolbox was applied here, and their features can be viewed within the Test Dataset Features toolbox.

Test Dataset Operations Phase using Orange toolboxes, (left) the test dataset was fed from the first phase, (middle) then propagated to the Inception v3 Model for features generating that fed to the fourth phase for performance measurement, (right) and these features can be visually viewed using test Dataset Features toolbox
2.4 Prediction and Performance Phase
The received signals from the Training Dataset Phase, i.e. the predictions from the machine learning classifiers, as well as from the Test Dataset Phase, i.e. the features from the Inception v3 Model (Test) toolbox were fed to the Predictions toolbox, to measure the performance and score the classification accuracies regarding the best-chosen classifier for COVID-19 cases. The following Orange toolboxes were implemented to compute such measurement and scoring, as illustrated in Fig. 7:

Prediction and Performance Phase using Orange toolboxes, (left) the signals were received from the second and third phases, (right) and then the performance measurement and classification accuracies scoring were achieved through these three toolboxes
-
Confusion Matrix: Shows the numbers of matched and unmatched samples from the test dataset under the predicted and the actual cases that were judged by the Predictions toolbox [35].
-
Sieve Diagram: Visualizes the frequencies of cases based on a pair of classifiers [36].
-
Linear Projection: Plots the linear separation of cases concerning their classifiers [37].
3 Methodology
In our presented work, an appropriate visual-based classification tool is provided that targets the medical domain, especially for the physicians with less experience in the machine learning philosophy and limited programming skills. Different distances, rules, trees, tables, and plots were obtained from the proposed seven machine learning classifiers based on their different selection of parameters. For that, the following configurable parameters for each machine learning classifier were chosen and tuned to have the best human-classifiable results regarding COVID-19 infection cases among other similar human-being lungs infection cases. Note that some parameters have an insignificant effect or no effect at all on the classification results for some classifiers.
3.1 Parameters of Distances Classifier
The Distances toolbox, along with the Hierarchical Clustering and Hierarchical Clustering Viewer toolboxes, performs a good classification on the training dataset with a small number of errors in clustering the cases, as demonstrated in Figs. 8, 9, and 10. Few cases in the clustering process have mismatched results, and the explanations of these outcomes were left to the epidemiology specialists due to their deep knowledge in this field. Our work provides an adequate and easy-to-use tool for them. Note that the Distance Metric parameter is better to be set as Cosine when dealing with images, in general.

Distances and hierarchical clustering results of COVID-19 axial CT scans of 100% accuracy

Distances and hierarchical clustering results of streptococcus L X-Ray images with one mismatched case

Distances and hierarchical clustering results of SARS PA X-Ray images with one mismatched case
3.2 Parameters of CN2 Rule Induction Classifier
The CN2 Rule Induction toolbox produces different rules, in the format of (IF condition THEN predict case), and classification accuracies based on its Evaluation measure parameter. Such that, when this parameter was set to Entropy [38] its classification accuracy was 53.9% and the generated number of rules was 43, as shown in Fig. 11. However, when this parameter was set to Laplace accuracy [38], its classification accuracy changed to 64% and the generated number of rules to 19, as shown in Fig. 12. Therefore, the Laplace accuracy parameter produces more classification accuracy results with fewer easy-to-read induced classifiable rules. Note that, the colored bars in the Distribution column represent the infection case: Blue for COVID-19, Green for SARS, Orange for Streptococcus, and Red for Pneumocystis.

CN2 Rule Induction and Evaluation measure parameter as Entropy, lower classification accuracy and higher induced difficult-to-read rules

CN2 Rule Induction and Evaluation measure parameter as Laplace accuracy, higher classification accuracy and a few induced easy-to-read rules
3.3 Parameters of Random Forest Classifier
The parameter Number of trees does not influence at all on the Random Forest toolbox CA performance and its results. Such that, when this parameter was set to 10, its CA is 70.8%. While, when this parameter was set to 20, its CA still be at 70.8%.
3.4 Parameters of Tree Classifier
The Min. number of instances in leaves parameter has no huge influence on the Tree toolbox’s CA performance and its results. Such that, when this parameter was set to 2, its CA is 58.4% with a tree generating of 35 nodes and 18 leaves. While, when this parameter set to 3, its CA changed to 59.6% with the same tree of 35 nodes and 18 leaves, as illustrated in Fig. 13.

Orange Tree viewer toolbox of 35 nodes and 18 leaves tree at either 2 or 3 of the Min. number of instances in leaves parameter selection
The interpretability rules that generate the unbalanced binary tree, as shown in Fig. 13, will be as follows:
-
The parent node, root, generates the left-side child, node, when (n21 ≤ 0.283447).
-
The root generates the right-side node when (n21 > 0.283447).
-
The left-side and right-side nodes then generate their children in the same fashion, and so on …
According to these interpretability rules, the percentile of cases was calculated based on the nXXXX. Note that the n21, for instance, is one of the 2048 features that were obtained previously from the Inception v3 Model (Training) toolbox on the training dataset.
3.5 Parameters of kNN Classifier
The kNN toolbox produces different CA based on Number of neighbors and Weight parameters. Table 2 presents the generated CA based on these two parameters. Note that, there were insignificant changes in its CA for the 5 or 10 selection of the Number of neighbors parameter as well as for the Uniform or Distance selection of the Weight parameter.
3.6 Parameters of Logistic Regression Classifier
The Logistic Regression toolbox generates different CA depending on the Regularization type parameter. Therefore, when this parameter was set to Ridge (L2) [39], then its CA was 95.5%. While, when this parameter was set to Lasso (L1) [40] then its CA changed be 84.3%. Since the Lasso (L1) parameter shrinks the extreme values of each sample towards its central values, then this could cause the loss of important information during the classification process than the Ridge (L2) parameter. Note that the Strength parameter was set to C = 1.
3.7 Parameters of Neural Network Classifier
The Neural Network toolbox produces different CA based on its Neurons in hidden layers, Activation, and Solver parameters. In our work, this classifier was implemented as an MLP of 2 hidden layers, due to the MLP architecture of more hidden layers had the same generated CA with the same parameters selection. The following activation functions of Logistic, tanh, and ReLU [41] as well as the solver optimizers of SGD [42] and Adam [43] were selected in this work, due to their robustness and non-linearity behaviors. Note that the Regularization parameter was set to 0.9 and the Maximal number of iterations was set to 100. Table 3 states the generated CA based on these three parameters.
The best-chosen CA was 91.0% for the MLP architecture of the (100 × 100 × 4) neurons with ReLU activation and Adam solver parameters selection, as well as of the (500 × 500 × 4) neurons with tanh activation and Adam solver parameters selection. However, the small MLP architecture of (100 × 100 × 4) neurons was chosen due to its fewer number of the utilized neurons that decrease the classification time, rather than the medium MLP architecture of (500 × 500 × 4) neurons.
4 Results and Discussion
In our work, the obtained human-classifiable results were based on the following factors: (1) the number of medical samples in the training and test datasets, (2) the seven proposed machine learning classifiers, (3) the selected and tuned parameters for each classifier, and (4) the predicted probabilities. Moreover, the Predictions toolbox was implemented to visually illustrate the predicted probabilities for the test dataset based on their labels as well as the outcome signals from the classifiers based on the training dataset. These predicted probabilities are CA, AUC (Area under ROC—Receiver Operating Characteristic), Precision, Recall, and F1 (a weighted harmonic mean of Precision and Recall) that used to compute the statistical performance of a machine learning classifier [44], as demonstrated in Fig. 14. Note that, in this Predictions toolbox, the cases can be chosen individually or as a group to show the best-chosen classifier(s) that predicted them, as denoted by the lengths, or strengths, of the blue bars.

Orange Predictions toolbox, (top) the blue bars show the strength of each classifier in predicting the four infected cases individually or as a group, and (bottom) the predicted probabilities (CA, AUC, Precision, Recall, and F1) of computing the statistical performance for each classifier
Moreover, other Orange toolboxes, such as Confusion Matrix, Linear Projection, and Sieve Diagram, were implemented to calculate the correlations and illustrate the projections between the training dataset and the test dataset for each machine learning classifier.
4.1 Results from Confusion Matrix
Figure 15 illustrates the correlation between the actual and the predicted cases on the samples from the test dataset as comparable matrices for each classifier regarding the four infected cases. It was observed that the COVID-19 samples were more classifiable under the Logistic Regression and Neural Network than the other classifiers, and especially for the Logistic Regression classifier since it has only four mismatched COVID-19 cases with Streptococcus cases, then followed by the Neural Network classifier that has eight mismatched COVID-19 cases with Pneumocystis and Streptococcus cases.

Confusion matrices for each classifier, and the Logistic Regression classifier performs well on COVID-19 cases classification
4.2 Results from Linear Projection
As demonstrated in Fig. 16, the COVID-19 samples, as the blue dots, were selected to be linearly projected with the Logistic Regression, Tree, Random Forest, kNN, and Neural Network classifiers to check their accurate classification and performance. It was visually noted that the COVID-19 samples were more classifiable under the Logistic Regression and Neural Network than the other classifiers, and especially for the Logistic Regression classifier due to a large number of blue dots around its axis, then followed by the Neural Network classifier.

Linear projection of COVID-19 samples, as the blue dots, within the five classifiers, and the Logistic Regression classifier performs well on COVID-19 cases classification
4.3 Results from Sieve Diagram
Orange Sieve Diagram toolbox provides the N samples visualization of the test dataset along with a pair of classifiers, as well as shows the Sieve Rank (X2). The darker blue regions are the stronger is the relationship of a given case for a pair of classifiers. This can be influenced on the X2 as well, so that the higher X2 gives a better illustration of the stronger relationship for a given case among a pair of classifiers. Figure 17 shows different Sieve diagrams for different pairs of classifiers, and it was visually observed that the COVID-19 samples were more classifiable under the pair of Logistic Regression and Neural Network classifiers. This observation was based on darker blue regions and higher X2 than for other pairs of classifiers. On the other hand, the COVID-19 samples were less classifiable under the pairs of Logistic Regression and Tree/Random Forest/CN2 Rule Inducer classifiers, which have lighter blue regions and lower X2.

Sieve diagrams for pairs of classifiers, N is the number of test samples and X2 is Sieve rank. (top-left) the pair of Logistic Regression and Neural Network classifiers performs well on COVID-19 cases classification with darker blue regions and higher X2
5 Conclusions
When more medical images regarding the COVID-19 datasets have been clinically provided and publicly available, this will open the chance to do more research in this field as well as increase the number of samples to the classifiers, which yields to get better modeling performance and classification accuracy. Hence, larger datasets of various diseases’ cases will contribute to do more labeling assignments, however less data augmentation would be required. The image scaling of 128 × 128 pixels was chosen, in this work, for the purpose of fast processing time, but this downscaling may also affect the hidden features of these diagnostic images, which gives at the end no better features extraction and detection using the Orange Inception v3 model toolbox. Our work was implemented using Orange software, a visual analytical tool for epidemiology specialists that have little knowledge in machine learning techniques and limited programming skills, to allow them to focus on COVID-19 cases analysis and classification with ease of use and simplicity of understanding and manipulating.
Some of the toolboxes’ parameters do not affect the overall workflow, while others do. Table 4 describes the parameters that have been carefully chosen for better rules, easy visualization, as well as higher performance and CA.
Based on Table 4, the Predictions toolbox demonstrates different CA for different classifiers. The higher CA is, the better classifier does, as categorized by Table 5.
Based on the Confusion Matrix toolbox, as in Fig. 15 shown previously, the Logistic Regression classifier has a better matching between the actual and the predicted cases for the samples from the test dataset, and then followed by the Neural Network classifier. While the Tree classifier has the worst matching pattern. Therefore, this is in agreement with Table 5. Based on the Linear Projection toolbox, as in Fig. 16 shown previously, the Logistic Regression and Neural Network classifiers have the most COVID-19 cases projection along their axes than the other classifiers. Therefore, this is in agreement with Table 5.
Based on the Sieve Diagram toolbox, as in Fig. 17 shown previously, the pair of Logistic Regression and Neural Network classifiers have the most test samples frequencies of COVID-19 cases, due to the darker blue regions and higher X2. Therefore, this is in agreement with Table 5. Based on the careful parameters selection and tuning for each classifier, the Predictions toolbox, the Confusion Matrix toolbox, the Linear Projection toolbox, the Sieve Diagram toolbox, and the CA from Table 5, the Logistic Regression model was the appropriate best-chosen classifier in identifying and classifying the COVID-19 cases among the other similar human-being lungs infected cases (SARS, Pneumocystis, and Streptococcus). The achieved CA for the Logistic Regression classifier was up to 95.5%. Figure 18 demonstrates the completed layout of all connected phases, toolboxes, and signals to achieve the overall Orange workflow for COVID-19 features detection and extraction using machine learning classifiers.

Orange phases, toolboxes, and signals workflow layout
References
World Health Organization. Coronavirus disease (COVID-19) pandemic. WHO.int. https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed 4 May 2021
Marmanis, D., Datcu, M., Esch, T., Stilla, U.: Deep learning earth observation classification using ImageNet pretrained networks. IEEE Geosci. Remote Sens. Lett. 13(1), 105–109 (2015)
Krizhevsky, A., Sutskever, I., Hinton, G.E.: ImageNet classification with deep convolutional neural networks. Adv. Neural. Inf. Process. Syst. 25, 1097–1105 (2012)
Rajpurkar, P., Irvin, J., Zhu, K., Yang, B., Mehta, H., Duan, T., Ding, D., Bagul, A., Langlotz, C., Shpanskaya, K., Lungren, M.P.: CheXNet: Radiologist-level pneumonia detection on chest X-rays with deep learning (2017). arXiv preprint arXiv:1711.05225
Ayan, E., Ünver, H.M.: Diagnosis of pneumonia from chest X-ray images using deep learning. In: 2019 Scientific Meeting on Electrical-Electronics & Biomedical Engineering and Computer Science (EBBT) pp. 1–5
Stephen, O., Sain, M., Maduh, U.J., Jeong, D.U.: An efficient deep learning approach to Pneumonia classification in healthcare. J. Healthc. Eng. (2019). https://doi.org/10.1155/4180949
Alimadadi, A., Aryal, S., Manandhar, I., Munroe, P.B., Joe, B., Cheng, X.: Artificial intelligence and machine learning to fight COVID-19. Physiol. Genomics 52, 200–202 (2020). https://doi.org/10.1152/00029.2020
Pinter, G., Felde, I., Mosavi, A., Ghamisi, P., Gloaguen, R.: COVID-19 pandemic prediction for Hungary; a hybrid machine learning approach. Mathematics 8(6) (2020). https://doi.org/10.3390/math8060890
Elaziz, M.A., Hosny, K.M., Salah, A., Darwish, M.M., Lu, S., Sahlol, A.T.: New machine learning method for image-based diagnosis of COVID-19. PLOS ONE 15(6) (2020). https://doi.org/10.1371/journal.pone.0235187
Sujath, R., Chatterjee, J.M., Hassanien, A.E.: A machine learning forecasting model for COVID-19 pandemic in India. Stoch. Env. Res. Risk Assess. 34, 959–972 (2020). https://doi.org/10.1007/s00477-020-01827-8
Ardabili, S.F., Mosavi, A., Ghamisi, P., Ferdinand, F., Varkonyi-Koczy, A.R., Reuter, U., Rabczuk, T., Atkinson, P.M.: COVID-19 outbreak prediction with machine learning. Algorithms 13(10) (2020). https://doi.org/10.3390/a13100249
Brinati, D., Campagner, A., Ferrari, D., Locatelli, M., Banfi, G., Cabitza, F.: Detection of COVID-19 infection from routine blood exams with machine learning: a feasibility study. J. Med. Syst. 44(135), 1–12 (2020). https://doi.org/10.1007/s10916-020-01597-4
Cheng, F.Y., Joshi, H., Tandon, P., Freeman, R., Reich, D.L., Mazumdar, M., Kohli-Seth, R., Levin, M., Timsina, P., Kia, A.: Using machine learning to predict ICU transfer in hospitalized COVID-19 patients. J. Clin. Med. 9(6) (2020). https://doi.org/10.3390/jcm9061668
Rustam, F., Reshi, A.A., Mehmood, A., Ullah, S., On, B.W., Aslam, W., Choi, G.S.: COVID-19 future forecasting using supervised machine learning models. IEEE Access 8, 101489–101499 (2020). https://doi.org/10.1109/ACCESS.2020.2997311
Kumar, S.R.: Novel Corona Virus 2019 Dataset V151. Distributed by Kaggle Inc. https://www.kaggle.com/sudalairajkumar/novel-corona-virus-2019-dataset
Allen Institute for AI: COVID-19 Open Research Dataset Challenge (CORD-19) V92. Distributed by Kaggle Inc. https://www.kaggle.com/allen-institute-for-ai/CORD-19-research-challenge
Orange: University of Ljubljana (2021). Accessed Apr 2021. https://orangedatamining.com
Gärtner, T., Lloyd, J.W., Flach, P.A.: Kernels and distances for structured data. Mach. Learn. 57(3), 205–232 (2004)
Collins, M., Schapire, R.E., Singer, Y.: Logistic regression, AdaBoost and Bregman distances. Mach. Learn. 48(1), 253–285 (2002)
Dreiseitl, S., Ohno-Machado, L.: Logistic regression and artificial neural network classification models: a methodology review. J. Biomed. Inform. 35, 352–359 (2002)
Clark, P., Boswell, R.: Rule induction with CN2: some recent improvements. In: Machine Learning—Proceedings of the Fifth European Conference (EWSL-91), pp. 151–163 (1991)
Džeroski, S., Grbovic, J., Walley, W.J., Kompare, B.: Using machine learning techniques in the construction of models. II. Data analysis with rule induction. Ecol. Model. 95(1), 95–111 (1997)
Dietterich, T.G., Kong, E.B.: Machine learning bias, statistical bias, and statistical variance of decision tree algorithms pp. 0–13. Technical report, Dept. of Computer Science, Oregon State University, USA (1995)
Olson, R.S., Moore, J.H.: TPOT: A tree-based pipeline optimization tool for automating machine learning. In: Workshop on Automatic Machine Learning (ICML), pp. 66–74 (2016)
Segal M.R.: Machine learning benchmarks and random forest regression. UCSF: Center for Bioinformatics and Molecular Biostatistics (2004). Retrieved from https://escholarship.org/uc/item/35x3v9t4
Rodriguez-Galiano, V., Sanchez-Castillo, M., Chica-Olmo, M., Chica-Rivas, M.: Machine learning predictive models for mineral prospectivity: an evaluation of neural networks, random forest, regression trees and support vector machines. Ore Geol. Rev. 71, 804–818 (2015). https://doi.org/10.1016/j.oregeorev.2015.01.001
Kramer, O.: K-nearest neighbors. In: Dimensionality Reduction with Unsupervised Nearest Neighbors. Intell. Syst. Ref. Libr. 51, 13–23 (2013). https://doi.org/10.1007/978-3-642-38652-7_2
Zhang, Z.: Introduction to machine learning: k-nearest neighbors. Ann. Transl. Med. 4(11) (2016). https://doi.org/10.21037/atm.2016.03.37
Chen, H.: Machine learning for information retrieval: Neural networks, symbolic learning, and genetic algorithms. J. Am. Soc. Inf. Sci. 46(3), 194–216 (1995)
Lampignano, J.P., Kendrick, L.E.: Bontrager’s Handbook of Radiographic Positioning and Techniques, 9th edn. Mosby, USA (2017)
Herring, W.: Learning Radiology: Recognizing the Basics, 4th edn. Elsevier, USA (2019)
Abu-Mostafa, Y.S., Magdon-Ismail, M., Lin, H.T.: Learning From Data: A Short Course. AMLBook, USA (2012)
ACDSee: ACD Systems International Inc. (2020). https://www.acdsee.com
Szegedy, C., Vanhoucke, V., Ioffe, S., Shlens, J., Wojna, Z.: Rethinking the inception architecture for computer vision. In: Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR), 2016, pp. 2818–2826
Deng, X., Liu, Q., Deng, Y., Mahadevan, S.: An improved method to construct basic probability assignment based on the confusion matrix for classification problem. Inf. Sci. 340, 250–261 (2016). https://doi.org/10.1016/j.ins.2016.01.033
Hidayatullah, R.S., Cholifah, W.N., Ambarsari, E.W., Kustian, N., Julaeha, S.: Sieve diagram for data exploration of Instagram usage habit obtained from Indonesia questioner’s sample. J. Phys. 1783(1) (2021). https://doi.org/10.1088/1742-6596/1783/1/012028
Belhumeur, P.N., Hespanha, J.P., Kriegman, D.J.: Eigenfaces vs. fisherfaces: recognition using class specific linear projection. IEEE Trans. Pattern Anal. Mach. Intell. 19(7), 711–720 (1997). https://doi.org/10.1109/34.598228
MacKay, D.: Information Theory, Inference and Learning Algorithms, 1st edn. Cambridge University Press, UK (2003)
Martínez-Martínez, J.M., Escandell-Montero, P., Soria-Olivas, E., Martín-Guerrero, J.D., Magdalena-Benedito, R., GóMez-Sanchis, J.: Regularized extreme learning machine for regression problems. Neurocomputing 74(17), 3716–3721 (2011). https://doi.org/10.1016/j.neucom.2011.06.013
Tibshirani, R.: Regression shrinkage and selection via the lasso. J. Roy. Stat. Soc. 58(1), 267–288 (1996)
Zhang, H., Weng, T.W., Chen, P.Y., Hsieh, C.J., Daniel, L.: Efficient neural network robustness certification with general activation functions (2018). arXiv preprint arXiv:1811.00866
Qian, N.: On the momentum term in gradient descent learning algorithms. Neural Netw. 12(1), 145–151 (1999). https://doi.org/10.1016/S0893-6080(98)00116-6
Kingma, D.P., Ba, J.: Adam: a method for stochastic optimization (2017). arXiv preprint arXiv:1412.6980
Powers, D.M.W.: Evaluation: from precision, recall and F-measure to ROC, informedness, markedness and correlation. 2020, arXiv preprint arXiv:2010.16061
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Al-Bayaty, A., Perkowski, M. (2022). COVID-19 Features Detection Using Machine Learning Models and Classifiers. In: Adibi, S., Rajabifard, A., Shariful Islam, S.M., Ahmadvand, A. (eds) The Science behind the COVID Pandemic and Healthcare Technology Solutions. Springer Series on Bio- and Neurosystems, vol 15. Springer, Cham. https://doi.org/10.1007/978-3-031-10031-4_18
Download citation
DOI: https://doi.org/10.1007/978-3-031-10031-4_18
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-10030-7
Online ISBN: 978-3-031-10031-4
eBook Packages: MedicineMedicine (R0)