
Abstract
Laryngeal surgery in children has advanced in the last 100 years. This has largely been due to developments in paediatric anaesthesia, diagnostic tools, microsurgical instruments and a multidisciplinary approach to the child’s larynx within a specialised paediatric institution.
The spectrum of laryngeal pathologies is different to that seen in adults and varies from neonates to infants to young to older children. Paediatric otolaryngologists manage such conditions as vocal cord nodules, laryngomalacia, subglottic stenosis and cysts, vocal cord paralysis and recurrent respiratory papillomatosis. On the other hand, adult otolaryngologists frequently encounter laryngitis, muscle tension dysphonia, spasmodic dysphonia, vocal cord paralysis, vocal cord polyps, nodules or cysts (non-cancerous lesions) and pre-cancerous and cancerous lesions. Most paediatric laryngeal disorders can be managed surgically with endoscopic minimally invasive techniques. The aim of this chapter is to discuss the advances in the diagnosis and management of the majority of laryngeal disorders encountered by a paediatric otolaryngologist. The laryngeal assessment, anaesthetic considerations and 13 different pathological disorders are presented.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Stridor
- Laryngomalacia
- Vocal cord paralysis
- Subglottic stenosis and cysts
- Recurrent respiratory papillomatosis
- Vocal cord nodules
- Anterior glottic web
- Laryngeal cleft
- Vallecular cyst
- Subglottic haemangioma
-
Laryngeal surgery in children differs from adults in many respects but particularly in relation to the anatomy, the assessment and the distinct pathological disorders.
-
Diagnostic procedures vary with age. The older child can tolerate videostroboscopy and voice analysis, whereas the infant and younger child will often need assessment under general anaesthesia.
-
Modern paediatric anaesthesia is critical in order to provide a safe and tubeless surgical field to work in.
-
A multidisciplinary team approach is essential for the best outcome and includes a paediatric otolaryngologist, anaesthetist, intensivist, radiologist, paediatrician, neonatologist and speech pathologist working in a designated paediatric institution.
-
Most paediatric laryngeal disorders can be managed surgically with an endoscopic minimally invasive technique.
-
Speech therapy is the therapeutic treatment of choice for vocal cord nodules.
-
Only 10% of children with laryngomalacia require a supraglottoplasty.
-
Injection medialisation laryngoplasty is the primary treatment of unilateral vocal cord paralysis.
-
Fifty percent of children with bilateral vocal cord paralysis will have spontaneous resolution in the first 24 months.
-
The most popular endoscopic treatment of subglottic stenosis is balloon dilation after scar division with or without local steroid injection.
-
Endoscopic marsupialisation of subglottic cysts is the most common surgical treatment.
-
Symptomatic type 1, type 2 and some type 3 laryngeal clefts can be repaired endoscopically using an endoscopic suture repair.
-
Beta-blockers are the first-line treatment for subglottic haemangiomas.
-
Endoscopic marsupialisation of vallecular cysts is the first-line treatment for the majority of cases.
-
Laser photoreduction of sarcoidosis of the supraglottis can be useful to avoid a tracheostomy in cases unresponsive to systemic steroids.
-
Granulomatosis with polyangiitis (GPA) with involvement of the subglottis can be surgically managed with the removal of granulation, balloon dilatation and intralesional corticosteroid injection.
-
Subtotal endoscopic excision is the main treatment for neurofibroma of the larynx.
13.1 Introduction
Laryngeal surgery in children is different in many respects to that of adults. The last two centuries have witnessed significant advances in laryngoscopy and bronchoscopy with the development of new instrumentation, fibre optics, light sources, video electronics and advanced anaesthesia techniques.
The anatomy of a child’s airway has unique features that may pose a challenge for airway management. Unique features include a prominent occiput resulting in neck flexion, large tongue, adenotonsillar hypertrophy, superior laryngeal position and lower functional residual capacity with higher oxygen metabolism resulting in more rapid desaturations in the presence of apnoea.
Diagnostic procedures will vary with age. The older child can tolerate investigations such as stroboscopy and voice analysis. However, the infant and younger child will often need assessment under general anaesthesia.
The diagnosis and surgical management of laryngeal disorders in children require a skilled paediatric anaesthetist, the objective being to provide a safe tubeless field for endoscopy and surgical management on the smaller larynx. Endotracheal tubes obstruct the view and limit the surgical access. Modern techniques used are inhalational anaesthesia, total intravenous anaesthesia (TIVA) or a combination with oxygenation provided via a nasopharyngeal tube or high flow oxygen techniques such as AIRVO.
A wide range of paediatric surgical instrumentation are required such as laryngoscopes, endoscopes, bronchoscopes, cold steel microsurgical instruments, lasers, microdebriders and high-pressure balloons.
A spectrum of pathologies are different to those seen in adults and vary from neonates to infants to young and older children. Paediatric otolaryngologists manage such conditions as vocal cord nodules, laryngomalacia, subglottic stenosis and cysts, vocal cord paralysis and recurrent respiratory papillomatosis. On the other hand, adult otolaryngologists frequently encounter laryngitis, muscle tension dysphonia, spasmodic dysphonia, vocal cord paralysis, vocal cord polyps, nodules or cysts (non-cancerous lesions) and pre-cancerous and cancerous lesions.
A multidisciplinary approach is essential and includes paediatric otolaryngologists, anaesthetists and intensivists, radiologists, paediatricians and neonatologists, speech and swallow therapists and specialist nurses in a designated paediatric institution.
It is fair to say that most paediatric laryngeal disorders can be treated endoscopically apart from severe subglottic/glottic stenosis which requires open surgery and will be discussed in detail in Chap. 16.
13.2 Laryngeal Assessment
Neonate, infant and young child
The most common symptom necessitating an ENT referral in a neonate is stridor. History should include onset and diurnal variation of stridor, antenatal and perinatal events, previous intubation or intensive care, underlying genetic conditions, feeding difficulties, failure to thrive, chronic cough and history of apnoea or cyanosis.
Examination should assess for the inspiratory versus expiratory nature of the stridor, tachypnoea, grunting, inward retractions of the chest wall, nasal flaring, central cyanosis and a weak cry.
Other features which should be noted include haemangiomas in the beard distribution, lymphatic malformations, evidence of craniofacial abnormalities or neuromuscular disease, congenital abnormalities, dysmorphic features, micrognathia, patency of the nasal apertures and macroglossia.
Flexible laryngoscopy is now widely used in the assessment of neonatal stridor and involves the use of a small 2.2 mm fiberoptic endoscope. The procedure is well tolerated and gives a good view of the supraglottis and vocal cords and allows dynamic assessment of the airway in an awake child. In addition, during the procedure, the paediatric otolaryngologist will be able to assess for stridor or a weak cry. Flexible laryngoscopy however, does not allow visualisation of the subglottis and trachea. Therefore, most children with stridor other than mild and moderate laryngomalacia still require microlaryngoscopy and bronchoscopy (MLB) under general anaesthesia. MLB is the gold standard for assessing the paediatric airway.
An additional investigation useful when assessing neonates with airway obstruction is polysomnography. Many babies with airway obstruction will suffer with sleep apnoea as the upper airway musculature relaxes during sleep. Polysomnography can therefore be a useful tool when investigating these neonates and deciding upon operative management [1].
Lateral neck X-ray and Cincinnati views show the subglottis, oropharynx and nasopharynx and allow the identification of subglottic stenosis or rare space-occupying lesions.
The main indications for computed tomography or magnetic resonance angiogram are to confirm the presence of external airway compression when suspected following a microlaryngoscopy and bronchoscopy, for example, innominate artery compression, a double aortic arch or a pulmonary artery sling.
Modified barium swallow (MBS) and fiberoptic endoscopic evaluation of swallowing (FEES) can be used to assess the child’s swallow. FEES uses a fiberoptic scope with real-time observation of the hypopharynx and larynx during swallowing. It is advantageous in that it does not expose the child to radiation. However, MBS can also assess the oral and pharyngeal phases of swallowing, and the patient does not need to cooperate like with FEES.
Laryngeal ultrasound is a safe, non-invasive alternative to flexible nasendoscopy to evaluate vocal cord mobility in neonates [2].
Laryngeal EMG can provide prognostic information on patients with unilateral or bilateral vocal cord paralysis. It may also assess the potential for recovery and can be useful prior to considering a reinnervation procedure. It, however, must be performed under general anaesthesia in children, and its reliability is highly dependent on the placement of electrodes by the otolaryngologist and the interpretation of the data by an experienced electroneurophysiologist.
Young child/teenager
Hoarseness is the most common presenting symptom of laryngeal pathology in the older child. Dedicated paediatric voice clinics include an assessment with a paediatric otolaryngologist and a paediatric speech and language therapist. Assessment includes fiberoptic laryngoscopy and stroboscopy in the older child. Speech and language therapists assess voice using a number of parameters as recommended by the European Laryngological Society including perceptual evaluation of voice using a standardised voice evaluation tool, acoustic analysis of voice, evaluation of aerodynamic support for voicing and subjective rating of impact using parent questionnaires [3].
-
Videolaryngostroboscopy is the main clinical tool for the aetiological diagnosis of voice disorders and should be recorded in order to assess the effectiveness of treatment. It can be carried out using a flexible nasendoscopy or a rigid telescope. Transoral examination using a 70-degree reverse angle sinus scope or a 70-degree Hopkins rod allows for excellent visualisation of vocal fold lesions and is surprisingly well tolerated [4].
Basic parameters assessed are glottal closure, mucosal wave and symmetry of the mucosal waves.
-
For perceptual-auditory vocal analysis, the GRB scale has been used worldwide. This scale evaluates the general degree of vocal alteration (G-grade), the irregular vibrations of the glottal cycle (R-roughness) and the turbulent air leakage through an insufficient glottic closure (B-breathiness). For reporting purposes, a 4-point grading scale is convenient (0, normal; 1, slight deviance; 2, moderate deviance; 3, severe deviance), but it is also possible to score on a visual analogue scale.
-
Acoustic analysis provides objective quantitative values to measure vocal function. Currently, acoustic parameters most commonly used include the fundamental frequency (Fo), jitter, shimmer and noise-to-harmonic ratio.
-
The simplest aerodynamic parameter of voicing is the maximum phonation time (MPT) in seconds. Another useful measure is the mean air flow rate which is equal to the vital capacity (mL)/MPT (s). It can also be calculated using a pneumotachograph. This device provides a direct measurement of the mean airflow rate (mL/s) for sustained phonation over a comfortable duration, usually 2–3 s, at the habitual pitch and intensity level and following inspiration of a habitual kind. There is a large overlapping range of values in normal and dysphonic children, and this limits its value for diagnostic purposes [5].
-
The use of quality-of-life protocols for the voice has been greatly valued, since they allow the quantification of the clinical improvement of vocal symptoms in the daily activity of children. One of the most used protocols is the paediatric voice handicap index (pVHI) which includes ten open-ended questions regarding the impact of the child’s voice quality on overall communication, development, education and social and family life [5].


13.4 Paediatric Anaesthetic Considerations
Anaesthesia for paediatric airway surgery requires training, experience and good communication between the anaesthetist and surgeon to determine the most appropriate mode of anaesthesia.
Traditionally, the classic inhalational anaesthesia was the most common anaesthesia technique during airway surgery; however, in recent years, total intravenous anaesthesia (TIVA) has become more and more popular. TIVA has many advantages in paediatric airway procedures which include reduced airway reactivity, reduced episodes of hypoxia, reduced laryngospasm and bronchospasm and there is no reliance on the inhalation route for administration of anaesthesia [6].
Preoperatively, an oral sedative can be useful in the anxious child provided there are no signs of imminent airway obstruction. Monitoring includes pulse oximetry, electrocardiography (ECG), non-invasive blood pressure and capnography (carbon dioxide measurement). A difficult intubation trolley should always be immediately available and stocked with a variety of laryngoscope blades, supraglottic airways, tracheal tube guides, oral and nasal airways and fiberoptic and videolaryngoscopic instruments.
In children, anaesthetic induction can be achieved using inhalation agents, total intravenous anaesthesia (TIVA) or a hybrid technique with a combination of inhalation and TIVA. Sevoflurane is the pharmacologic agent of choice for inhalation induction. Spontaneous ventilation is recommended although occasionally it might be necessary to assist ventilation with gentle mask ventilation. After induction, a cannula should be sited, if it has not been sited prior to induction. Intravenous anaesthetics such as propofol, dexmedetomidine, ketamine and/or remifentanil are used for anaesthesia maintenance as they provide a reliable level of anaesthesia. The correct balance of these agents is essential for effective and safe management in paediatric airway procedures, and this requires a good understanding of their respective and combined pharmacokinetics and pharmacodynamics [6]. When the child is deeply anaesthetised, laryngoscopy should be performed, and the larynx and trachea sprayed with 4% lignocaine (maximum dose 4 mg/kg). The laryngoscope is withdrawn and oxygenation is maintained. Once adequate depth of anaesthesia is achieved, the ENT surgeon re-exposes the larynx, and the child is placed on suspension. Supplemental oxygen is provided through a nasopharyngeal tube with the tip in the oropharynx or via high flow nasal oxygen such as AIRVO [7, 8].
A T-piece circuit can be attached to the sidearm of a ventilating bronchoscope to allow delivery of oxygen and anaesthetic gases during the procedure.
Despite the plan to have the patient spontaneously breathing, a set of appropriately sized endotracheal tubes should be available both for airway sizing and for intermittent intubation if needed.
13.5 Disorders of the Larynx in Children and Their Surgical Management
13.5.1 Laryngomalacia
13.5.1.1 Introduction
Laryngomalacia is the most common cause of stridor in infants and children. Dynamic obstruction of the supraglottic area during inspiration causes stridor, but the pathophysiological mechanism is still debated. The exact aetiology is unknown, but the most popular theory is that laryngomalacia is caused by hypotonia due to abnormal sensorimotor integrative function. This hypotonia allows for prolapse of the supraglottic airway which leads to obstructive airway symptoms. Gastrooesophageal reflux disease plays a role, although it is not fully understood. One theory is that the airway obstruction as a result of laryngomalacia generates negative intrathoracic pressure which promotes gastric acid reflux, which in turn results in supraglottic oedema and further obstruction [9].
13.5.1.2 Clinical Features
Typical symptoms of laryngomalacia include inspiratory stridor that worsens with feeding, crying, supine positioning and agitation. Symptoms typically begin within the first weeks of life, peak at a few months of age and commonly resolve on their own within 12–24 months. Infants with laryngomalacia may have a difficult time coordinating the suck-swallow-breath sequence needed for feeding as a result of their airway obstruction. The increased metabolic demand of coordinating eating and breathing against the obstruction can be so severe that it results in weight loss and failure to thrive. In severe cases, apnoea and cyanosis may occur.
13.5.1.3 Diagnosis
Diagnosis is suspected on clinical history and can be confirmed with flexible nasendoscopy. Once diagnosed, laryngomalacia can be classified as mild, moderate or severe depending on the associated feeding and obstructive symptoms. In mild cases, the baby will have inspiratory stridor without any feeding difficulties or apnoea. In moderate cases, the baby will have stridor with associated feeding difficulties, while in severe cases, which account for 10–20% of cases, there is significant airway obstruction as well as feeding difficulties and failure to thrive (FTT).
13.5.1.4 Management
In 1999, Olney et al. classified laryngomalacia based on the site of the obstruction. Type 1 which is the most common is secondary to prolapse of the mucosa overlying the arytenoid cartilage. Type 2 is secondary to short aryepiglottic folds. Type 3 occurs due to posterior displacement of the epiglottis [10]. Children who present with mild disease are managed conservatively and should be reviewed 6 weeks following diagnosis to ensure symptoms are improving. Those children with moderate laryngomalacia are initially managed in conjunction with the speech and swallow therapists with feeding modification techniques such as thickened formula, bottle pacing and upright position for feeding as well as acid suppression treatment. Babies with severe laryngomalacia should be admitted to hospital and managed within a multidisciplinary team including otolaryngologists, paediatricians, respiratory physicians, speech and swallow therapists and dieticians. Investigations will include a paediatric review to exclude any underlying genetic, neurologic or cardiac abnormalities, a feeding assessment such as a videofluoroscopic swallowing study (VFSS) or fiberoptic endoscopic evaluation of swallowing (FEES) as well as a sleep study [11].
13.5.1.5 Surgery
Approximately 10% of children with laryngomalacia will have severe symptoms which require surgical intervention in the form of a supraglottoplasty.
Supraglottoplasty has a success rate of greater than 90%. The most common type involves debulking of the arytenoids using graspers and microscissors or the microdebrider as well as division of the aryepiglottic (AE) folds with microscissors. This can also be done using laser, but it is thought that cold steel is less painful and causes less damage to the sensory nerves of the supraglottis. It is very important to avoid traumatising the mucosa on the medial surface of the arytenoid in order to prevent interarytenoid scarring and supraglottic stenosis. Most cases are successfully treated by the above procedure. Occasionally, for a type 3 laryngomalacia, a different type of supraglottoplasty (epiglottopexy) is required. This involves resection of mucosa with diathermy, laser or coblation to the lingual surface of the epiglottis and base of the tongue in order to encourage scar/adhesion formation as well as suturing of the epiglottis to tongue base [12].
Following supraglottoplasty, patients are often fed via nasogastric tube for 24–48 h. Children are commenced on proton pump inhibitors for 1 month postoperatively in order to break the cycle of oedema resulting in obstruction, increased negative pressure, worsening reflux and increasing oedema [13] (Fig. 13.3).

Severe laryngomalacia (a) before and (b) after supraglottoplasty
Approximately 10% of children with laryngomalacia will have severe symptoms which require surgical intervention in the form of a supraglottoplasty.
13.5.2 Vocal Cord Paralysis
13.5.2.1 Introduction
Vocal cord paralysis (VCP) is the second most common cause of neonatal stridor after laryngomalacia. It accounts for approximately 10% of congenital laryngeal lesions. Unilateral vocal cord paralysis (UVCP) and bilateral vocal cord paralysis (BVCP) are different entities with varying presenting symptoms, causes and treatment. The most common causes of VCP are neurologic, traumatic, iatrogenic or idiopathic. The Arnold-Chiari (Chiari II) malformation is the most common neurologic finding in BVCP. Intubation and birth trauma related to breach or vertex delivery or the use of forceps can lead to compression or stretching of the recurrent laryngeal nerve in the neck. Cardiothoracic surgery, in particular, patent ductus arteriosus repair, is most often implicated as a cause of iatrogenic UVCP [14].
13.5.2.2 Unilateral Vocal Cord Paralysis
13.5.2.2.1 Clinical Features
Although stridor is the most common presenting symptom, children may also present with an abnormal cry, dysphonia and feeding difficulties.
13.5.2.2.2 Diagnosis
Unilateral vocal cord paralysis (UVCP) can be confirmed on dynamic assessment of the larynx with a flexible fiberoptic endoscopy; however, this does have its challenges. Difficulty in visualising the larynx can occur due to increased respiratory rate, floppy supraglottic structures, secretions and a narrowed epiglottis.
Because of these difficulties, other methods have been proposed to evaluate the neonatal larynx.
Ultrasonography of the larynx is a useful non-invasive and reliable adjunctive examination.
MLB under general anaesthesia is often carried out if the diagnosis is unclear after awake flexible laryngoscopy or if a secondary airway lesion is suspected.
The role of laryngeal electromyography (EMG) in contributing to the diagnosis and prognosis of vocal cord immobility in children has been debated. This test assesses for the presence and morphology of motor unit action potentials (MUAPs) in the denervated muscles. EMG is not routinely used except in a limited number of institutions [15].
13.5.2.2.3 Management
The treatment of unilateral vocal cord paralysis is determined by a patient’s symptoms, and in many instances, there is effective compensation from the contralateral vocal cord, and no surgical intervention is required. All children are assessed by a speech and swallow therapist, with the addition of a swallow study such as VFSS or FEES if necessary.
Multiple treatment options are currently available for unilateral vocal cord paralysis, but the three most common procedures are injection medialisation laryngoplasty (IML), thyroplasty and ansa cervicalis to recurrent laryngeal nerve (RLN) reinnervation procedures.
13.5.2.2.4 Surgery
Injection medialisation laryngoplasty (IML) is the mainstay of treatment for unilateral vocal cord paralysis. Glottic closure is improved by injecting the thyroarytenoid muscle in the paralysed cord. A number of injectable substances are available and are currently categorised as temporary such as carboxymethyl cellulose or long term such as calcium hydroxyapatite. The decision regarding what substance to use is based on the duration of the paralysis as well as the indication for the procedure. Carboxymethyl cellulose is the most commonly used temporary material and is useful in providing temporary results if return of vocal function is possible or while deciding whether to proceed with a more permanent procedure such as injection with calcium hydroxyapatite or reinnervation [16].
In thyroplasty, the paralysed vocal cord is medialised permanently with an implant positioned by an external neck incision. It remains a common intervention in adults; however, in paediatrics, it is generally reserved for adolescents who are able to tolerate the procedure while awake so that intraoperative phonation can be tested for optimal vocal cord positioning.
Nonselective laryngeal reinnervation using the ansa cervicalis to the recurrent laryngeal nerve has gained tremendous popularity in the past decade. The goal of laryngeal reinnervation is to provide bulk and tone to the denervated vocal fold not to restore mobility. Reinnervation is a permanent intervention that does not affect laryngeal development or framework. Reinnervation typically takes 4–6 months for evidence of effect; therefore, clinicians will often perform concomitant IML with a resorbable implant material to temporarily provide bulk and improve closure during the healing process [17].
Preoperatively, laryngeal electromyography (EMG) is a useful tool to better understand and anticipate the prognosis.
A key issue that remains controversial in the management of UVCP is the timing of surgical intervention. This should be guided by symptom severity, knowledge of UVCP natural history and the effect of dysphonia on the child. Children who experience aspiration due to UVCP should be offered at least a temporary surgical intervention. For the first few years after diagnosis of UVCP, conservative measures and/or temporary measures should be offered, whereas thyroplasty and reinnervation are two long-term surgical solutions [18, 19].
Injection medialisation laryngoplasty (IML) is the mainstay of treatment of unilateral vocal cord palsy.
13.5.2.3 Bilateral VCP
13.5.2.3.1 Clinical Features
In patients with BVCP, as opposed to UVCP, their voice is often normal as the vocal cords are usually in a paramedian position with abductor paralysis. Stridor, cyanosis, apnoeic episodes and respiratory distress are more likely to occur in patients with BVCP.
13.5.2.3.2 Diagnosis
BVCP can be confirmed on flexible nasendoscopy. Children should undergo an MRI of the brain to outrule any central nervous system or brainstem cause.
13.5.2.3.3 Management
Management options for BVCP depend primarily on the degree of airway compromise. It varies from watchful waiting, non-invasive positive pressure ventilation (NIPPV), endoscopic surgery such as anterior and posterior cricoid split, cordotomy, suture lateralisation, posterior cricoid split with endoscopic insertion of cartilage grafts or tracheostomy [20, 21].
13.5.2.3.4 Endoscopic Surgery
More than 50% of children with BVCP will have spontaneous resolution in the first 24 months of life; therefore, any procedure to establish a safe airway should have minimal impact on the ability to phonate and swallow for the child and carers. Historically, tracheostomy was performed on the majority of patients with BVCP, and although the majority of children will be decannulated, it is associated with significant morbidity and lengthy hospital stays. As a result, several procedures have been described as an alternative to tracheostomy, but there is no one operation that is clearly superior than others [22].
-
1.
Endoscopic Percutaneous Suture Lateralisation
Suture laterofixation has been a treatment modality for BVCP for several decades in adults. Several different techniques have been described in recent years to modify this technique for use in neonates. Suture lateralisation provides a stable, long-lasting and wide airway that is potentially reversible as the anatomical structures are not significantly disturbed.
Reversal needs to be carefully considered, because reinnervation of the two vocal cords does not necessarily occur simultaneously. This decision will be based on clinical symptoms such as aspiration and dysphonia. Potentially in the future, this decision could be considered if endoscopic and/or laryngeal electromyographic examinations confirm the reinnervations [23].
-
2.
Cordotomy
Endoscopic cordotomy consists of an incision in the posterior third of the true vocal fold. The technique enlarges the posterior part of glottis, while the vocal folds still have a good contact on the anterior commissure. While this technique may have a lesser impact on voice and swallowing, it does require an irreversible alteration of the larynx.
-
3.
Anterior and Posterior Cricoid Split (APCS)
The anterior and posterior cricoid split was first described in 2017. As governed by Poiseuille’s law, a small increase in the radius of the airway will exponentially increase airflow through the larynx. They proposed that by achieving a modest increase in intraluminal diameter without making permanent or potentially destructive changes to the glottic structures, tracheostomy could be avoided in some children. The biggest disadvantage of anterior posterior cricoid split is its irreversible alteration of the laryngeal skeleton, and the long-term sequelae to phonation are unknown. Early results are promising, but the duration of intubation post-procedure is variable and not clearly defined [20].
-
4.
Endoscopic Posterior Cricoid Split with Graft
Endoscopic posterior cricoid split with rib cartilage graft is a relatively new technique used for bilateral VCP. Previously, posterior cricoid grafting with costal cartilage was used for children with subglottic or posterior glottic stenosis, but Inglis has described its success in children with bilateral VCP [24].
The CO2 laser or cold steel is used to perform the posterior cricoid split. Measurements of the width and length of the split are taken and recorded. The rib cartilage graft is harvested from the fourth or fifth rib on the right side with a horizontal incision and shaped to distract the free edges of the cricoid. The graft is snapped into place under direct microscopic visualisation, and no sutures are used to fix the graft in place.
The advantages of endoscopic posterior cricoid split with rib cartilage graft are that it avoids injury to the vocal cords and in theory is reversible in the event of recovery of function [23]. The disadvantage is that it is not suitable for neonates or infants with BVCP.
-
5.
Selective Laryngeal Reinnervation
Selective laryngeal reinnervation aims to restore the physiological function of the vocal cords by reinnervating both the laryngeal abductors and adductors. The main advantage of this procedure is that unlike the above-described static glottic enlargement procedures, reinnervation does not permanently compromise voice quality as patients can regain considerable abduction but also adduction [25]. The technique has been modified and honed by Professor Jean Marie and recently has been described in children. Branches of the phrenic nerve and hypoglossal nerve are most commonly used. Careful patient selection is essential as this procedure is not suitable for small babies or young children or those with severe underlying cardiorespiratory disorders due to the long duration of surgery required [26] (Fig. 13.4).

(a) Post-left cordotomy and (b) post-right suture lateralisation for bilateral vocal cord paralysis
Fifty percent of children with BVCP will have spontaneous resolution in the first 24 months of life; therefore, any procedure to establish a safe airway should have minimal impact on the ability to phonate and swallow long term.
13.5.3 Subglottic Stenosis
13.5.3.1 Introduction
Subglottic stenosis (SGS) can be congenital or acquired, and our focus in this chapter is on the endoscopic management of the less severe grades of acquired SGS. Laryngotracheal stenosis will be discussed in detail in Chap. 16.
The severity of subglottic stenosis is determined as per the Cotton-Myer grading system: Grade I, up to 50% stenosis; Grade II, 51–70% stenosis; Grade III, 71–99% stenosis; and Grade IV, 100% stenosis [27].
Congenital SGS forms as a result of failure of recanalisation of the airway which usually occurs by the tenth week of gestation. Congenital subglottic stenosis varies from mild narrowing to complete laryngeal atresia depending on the severity of incomplete cricoid recanalisation. It is often associated with syndromes, such as trisomy 21, CHARGE and 22q11 deletion.
Acquired SGS is most commonly associated with post-intubation injury in 90% of cases. Leung and Berkowitz described the incidence of severe acquired SGS requiring surgical intervention as 0.005%. While an exact incidence of acquired SGS is difficult to determine, it is clear that a trend towards a decreased incidence is evident, most likely due to advances in neonatal care. The two main advances have been the use of surfactant and the avoidance of intubation due to the increased use of non-invasive ventilation in very premature babies [28]. Other factors that are suspected to play a role include the size and type of the endotracheal tube, duration of intubation, traumatic intubation, number of intubations, presence of an infection while intubated and possibly gastrooesophageal reflux disease [29].
13.5.3.2 Clinical Features and Diagnosis
The presentation of subglottic stenosis depends on the degree of narrowing. Mild SGS may go undiagnosed for years only to manifest as recurrent croup during childhood. Severe SGS may present immediately with inspiratory or biphasic stridor, respiratory distress and difficulty with intubation. Flexible fiberoptic laryngoscopy is important to assess for possible concurrent laryngomalacia and vocal fold immobility. However, a rigid direct laryngoscopy and bronchoscopy under general anaesthesia is required to formally evaluate the airway distal to the level of the vocal cords. The airway should be sized by placing a series of increasing sized endotracheal tubes (ET) through the laryngeal inlet and observing for leak, evidenced by air bubbles around the ET tube at the level of the cords at less than 20 cm of water pressure.
Plain film X-ray may reveal a characteristic narrowed appearance, similar to that seen in croup, known as the steeple sign.
Multidisciplinary paediatric workup is required in particular an assessment of the patients’ swallow function, and if there are any concerns, a functional evaluation of swallowing (FEES) is useful. The cardiac, respiratory, neurological and nutritional status of the child are important factors in deciding what type of surgery is needed.
13.5.3.3 Surgery
Surgical techniques are broadly grouped into either endoscopic or open procedures. Open procedures are not discussed here; see Chap. 16.
13.5.3.4 Endoscopic
Indications for endoscopic techniques include Cotton-Myer Grade II and less severe Grade III, membranous stenosis with adequate cartilaginous support and craniocaudal extension of stenosis no longer than 1 cm.
The mainstay of endoscopic treatment of subglottic stenosis is high-pressure balloon dilatation after scar division with or without steroid injection. In endoscopic balloon dilatation, the balloon is inserted into the airway and gently inflated, applying radial pressure circumferentially to the stricture. Recently, new balloons pioneered by Professor Rutter at Cincinnati Children’s Hospital have been introduced. These are designed so that on initial inflation, two hubs appear distally and proximally on the balloon. This locks the balloon in place over the stricture and prevents it from sliding proximally or distally on inflation. Balloon dilatation is also useful as an adjunct to open surgery either preoperatively or postoperatively. Scar division can be useful for patients with thicker stenosis refractory to dilatation and can be done prior to dilatation. Typically, three radial incisions are carried out in a “Mercedes-Benz” configuration with a Blitzer knife or laser. This creates weak points in the stenosis, allowing dilation to produce controlled tears through the scar tissue.
13.5.3.5 Medical
Adjuvant topical treatments include intralesional steroids and topical mitomycin C. Steroids, such as triamcinolone, are particularly beneficial if an underlying inflammatory disorder is suspected [30]. Mitomycin C is an antibiotic and an antineoplastic agent that inhibits the proliferation of fibroblasts and has been used topically with the aim of preventing restenosis. Its use is controversial as it is a potential carcinogen with a lack of evidence of effectiveness and has therefore fallen out of favour recently [31].
13.5.3.6 Open Surgery
Open surgical techniques are reserved for patients with more severe grades of subglottic stenosis, patients with multilevel disease or those who fail repeated endoscopic balloon dilatations [32, 33] (Fig. 13.5).

(a) Early subglottic stenosis; (b) 1-week post-cricoid split and balloon dilatation
The mainstay of endoscopic treatment of subglottic stenosis is balloon dilatation after scar division +/− local steroid injection.
13.5.4 Subglottic Cysts
13.5.4.1 Introduction
Subglottic cysts are a rare but increasingly recognised cause of respiratory complications in neonates. From all previous reports in the literature, it seems likely that subglottic cysts are usually acquired lesions since all reported infants with subglottic cysts have a prior history of intubation [34].
The pathogenesis of subglottic cysts is likely to involve mucosal damage, fibrosis, obstruction of mucous glands and subsequent mucus retention cyst formation [35].
13.5.4.2 Clinical Presentation and Diagnosis
The most common presenting symptom is biphasic stridor. Other symptoms include apnoea, recurrent croup and feeding difficulties. Children may present with acute airway obstruction or may present a more indolent course as the cyst progressively enlarges.
Direct laryngoscopy and bronchoscopy is the gold standard for diagnosis.
13.5.4.3 Surgery
Management options include observation and endoscopic or open surgical approaches.
Endoscopic treatment of cysts mostly consists of marsupialisation of the cysts using laser, cold steel or the microdebrider.
Patients who have had subglottic cysts treated should have a follow-up assessment as there is a tendency for these cysts to recur (Fig. 13.6).

(a) Subglottic cyst; (b) following excision with microdebrider
Endoscopic treatment of cysts mostly consists of marsupialisation of the cysts using laser, cold steel or the microdebrider.
13.5.5 Recurrent Respiratory Papillomatosis
13.5.5.1 Introduction
Recurrent respiratory papillomatosis (RRP) is discussed in more detail in Chap. 14, and our focus in this chapter is on the management of juvenile-onset RRP in children who present with more severe disease.
Recurrent respiratory papillomatosis (RRP) is the most common benign neoplasm of the larynx in children with an estimated incidence of 4.3 per 100,000 children. The juvenile-onset form of RRP usually develops in early childhood with a mean age of diagnosis between 3 and 4 years. It is caused by human papillomavirus, and subtypes 6 and 11 are thought to be responsible for more than 85% of cases. Transmission of the virus is thought to occur through the birth canal, and there is a 200-fold increased risk for RRP if the mother has active condyloma at the time of delivery. The majority of patients, however, delivered to HPV-positive mothers will not develop RRP, and caesarean section delivery does not completely prevent the disease; hence, much is still unknown about HPV transmission in utero and peripartum [36].
13.5.5.2 Natural History
The natural history varies significantly and is difficult to predict. Some children experience minor symptoms with spontaneous and complete remission at puberty, while others require multiple surgeries throughout childhood. In rare situations, the disease may transform into malignant lesions or, in 1–3% of cases, may spread to the lower respiratory tract, entailing high mortality.
Worldwide with increasing vaccination rates, the incidence of juvenile RRP should theoretically decrease overall [37].
13.5.5.3 Clinical Features
The most common presenting symptoms are progressive hoarseness, stridor and respiratory distress.
13.5.5.4 Diagnosis
RRP is diagnosed on flexible nasendoscopy and confirmed on direct microlaryngoscopy and bronchoscopy. At the time of the diagnostic MLB, a sample should be sent for pathological analysis, while many institutions will also perform DNA analysis by PCR to determine the viral subtype which may help to predict the aggressiveness of the lesions [38].
The most common staging systems are the Derkay score and the modified Wiatrak score which can be used to document severity and facilitate surveillance [39, 40].
13.5.5.5 Surgery
Although multiple treatment options exist, there is no cure, and surgical debulking remains the mainstay of therapy along with a variety of topical, intralesional and systemic adjuvant therapies. Laryngeal microdebrider is the most popular technique, but other options include the CO2 laser, KTP (potassium titanyl phosphate) laser, pulsed dye laser, cold steel and radiofrequency ablation. The aim of surgery is to remove the papillomas while preserving anatomic structures, and care should be taken to avoid opposing raw surfaces which could result in scarring, webbing and/or stenosis [36].
13.5.5.6 Adjuvant Therapy
Several intralesional adjuvant therapies have been described. Cidofovir and bevacizumab are the most widely used although they remain off-label use.
Growing evidence exists in support of vascular endothelial growth factor (VEGF) as an important factor in the development of RRP, and bevacizumab is a recombinant monoclonal antibody designed to bind VEGF and inhibit the VEGF receptor. It has been used in the past systemically to treat metastatic carcinoma and topically to treat hereditary haemorrhagic telangiectasia. Zietells et al. were the first to report its use intralesionally in RRP in adults in 2009. Doses used sublesionally are far lower than those required for systemic treatment with reduced potential for adverse side effects which would include coagulopathy, poor wound healing and gastrointestinal perforation. Bevacizumab has been shown to reduce disease recurrence and disease severity.
Cidofovir is an antiviral that selectively inhibits viral DNA polymerase, which prevents viral replication and transcription. Its use remains off-label and controversial. There are known side effects such as nephrotoxicity; however, the potential carcinogenicity in vitro of cidofovir has caused widespread concern about its use. A Cochrane review in 2012 reported no benefit with its use, and as such, its use has fallen out of favour [41].
Novel adjuvant systemic therapy may be considered in those patients who require more than four procedures per year, have disease present in locations difficult to treat with standard surgical interventions or have rapid regrowth with airway compromise. Bevacizumab is the most promising systemic treatment, but its use remains off-label. Other systemic treatments include the HPV recombinant vaccine, interferon and systemic antivirals [38].
RRP requires ongoing surveillance as there is no known cure and the clinical course can vary from spontaneous regression to rapidly progressive fatal disease.
Complications of surgery in RRP are in general secondary to overaggressive resections resulting in granulation tissue, fibrosis, scarring and stenosis. These complications can end up being more troublesome than the initial disease and often are harder to treat. Special care should be taken at the anterior and posterior commissure to prevent webbing [36] (Fig. 13.7).

Recurrent respiratory papillomas: (a) glottic and (b) supraglottic and glottic
Although multiple treatment options exist, there is no cure, and surgical debulking remains the mainstay of therapy along with a variety of topical, intralesional and systemic adjuvant therapies.
13.5.6 Vocal Cord Nodules
13.5.6.1 Introduction
Vocal fold nodules (VFNs) are benign lesions usually occurring at the junction of the anterior and middle third of the vocal folds. They develop as a result of trauma due to contact between opposing surfaces of the vocal folds, often associated with repeated vocal abuse. Many factors, including gastrooesophageal reflux, allergies, sinusitis, postnasal discharge and chronic cough, can be effective in creating a more favourable environment for VFN formation [42].
13.5.6.2 Clinical Features and Diagnosis
The most common symptom in patients with VFNs is dysphonia. Diagnosis can be achieved with flexible nasendoscopy, direct laryngoscopy and bronchoscopy or laryngeal stroboscopy.
Speech and language therapists will assess a number of parameters such as perceptual evaluation of voice (grade, roughness, breathiness, strain), acoustic analysis and aerodynamics [43].
13.5.6.3 Management
Speech therapy is the therapeutic cornerstone for paediatric vocal fold nodules. Intervention must be tailored not only to the pathology but also to a child’s willingness to engage. Generally, if the child is bothered by their voice, they will be motivated to change it, whereas if the child is not troubled, they are unlikely to comply with voice hygiene or cessation of vocally abusive behaviours.
Indirect therapy or voice hygiene typically includes education about healthy voice care, increased hydration and elimination of abusive habits. Direct voice therapy encompasses a variety of behavioural techniques including progressive relaxation, laryngeal massage, vocal intensity reduction and pitch elevation. Both direct and indirect voice therapy approaches appear to improve voice-related quality of life although there doesn’t appear to be a significant difference between the two forms of therapy [44,45,46].
In addition to speech therapy, any exacerbating factors such as allergic rhinitis or gastrooesophageal reflux should be addressed.
13.5.6.4 Surgery
Laryngeal microsurgery is reserved for cases where significant vocal limitations remain despite optimal behavioural management (Fig. 13.8).

Vocal cord nodules
Speech therapy is the therapeutic treatment of choice for paediatric vocal fold nodules as well as treating any exacerbating factors such as allergic rhinitis or gastrooesophageal reflux.
13.5.7 Anterior Glottic Web
13.5.7.1 Introduction
Glottic webs are characterised by the formation of abnormal, epithelium-covered fibrous tissue between the vocal folds. The anterior glottis is the most common site of involvement. Glottic webs may be congenital or acquired. Acquired anterior glottic webs are more common and typically occur from a traumatic injury to the larynx such as intubation, laryngeal trauma or surgery close to the anterior commissure. Congenital webs result from incomplete recanalisation of the primitive larynx during the tenth week of embryogenesis.
A variety of conditions are associated with congenital anterior glottic webs. The incidence of 22q11 microdeletion (DiGeorge syndrome) in patients presenting laryngeal webs is reported to be as high as 65%.
Laryngeal webs can be classified into four subtypes proposed by Cohen. Type I membranes consist of less than or equal to 35% of glottic involvement and do not extend to the subglottic region. Type II webs have 35–50% of glottic involvement and may present with concomitant isolated subglottic stenosis. Type III webs have a 50–75% glottic involvement, are thick and potentially have a cartilaginous involvement of the adjacent subglottic region. Type IV webs are uniformly thick and involve from 75% to 90% of the glottic area with cartilaginous subglottic extension [47].
13.5.7.2 Clinical Features
Clinical manifestations vary according to the extent of glottic involvement. Large webs are usually identified at birth presenting with biphasic stridor. Smaller webs may not be identified until later in life and can present with dysphonia, hoarseness, recurrent croup and impaired exercise tolerance.
13.5.7.3 Diagnosis
Microlaryngoscopy and bronchoscopy (MLB) under general anaesthesia is imperative to evaluate extension of the web to the subglottic area, size the airway and exclude other concomitant airway anomalies.
13.5.7.4 Management
Management of laryngeal webs consists of conservative, endoscopic and open approaches.
13.5.7.5 Surgery
Endoscopic approaches include division of the web with either cold knife instruments or laser. Mucosal flaps and/or keel placement may be used in order to prevent web reformation by separating the divided mucosa at the anterior commissure.
Mitomycin C has been used in the past, but for reasons discussed earlier, it has fallen out of favour [48].
Open surgery is seldom required nowadays and is reserved for patient with Cohen grade 3 or 4 webs with significant subglottic extension which cannot be managed endoscopically [48] (Fig. 13.9).

Anterior glottic web
Less extensive anterior glottic webs can be managed endoscopically.
13.5.8 Laryngeal Cleft
13.5.8.1 Introduction
Laryngotracheal clefts (LC) are congenital malformations of the upper aerodigestive tract resulting from a failure of posterior fusion of the larynx and trachea. This deformity creates an inappropriate communication between the larynx and oesophagus [49].
In 1989, Benjamin-Inglis classified laryngeal clefts into four types:
-
Type 1 is an interarytenoid cleft that extends no further than the level of the true vocal cords.
-
Type 2 is a partial defect of the cricoid cartilage.
-
Type 3 is a complete defect of the cricoid cartilage extending into the cervical trachea.
-
Type 4 is a defect involving the thoracic trachea which can be subdivided into type 4a (extension to the carina) and type 4b (extension into one of main bronchi) [50].
Estimates of the incidence of laryngeal clefts are challenging because type 1 clefts often go misdiagnosed for long periods or are asymptomatic.
Laryngeal clefts are associated with a number of syndromes including Opitz-Frias syndrome, Pallister-Hall syndrome, VACTERL syndrome and CHARGE syndrome. Approximately 12% of patients with LC have a concurrent tracheooesophageal fistula [51].
13.5.8.2 Clinical Features
The presenting symptoms of LC are varied, but generally the severity of the symptoms correlates with the severity of the cleft.
Patients with type 3 and 4 LC may present at birth with respiratory distress, cyanosis, stridor with feeds and florid aspiration. In contrast, the diagnosis of type 1 and 2 LC is frequently delayed due to non-specific signs and symptoms. Stridor, feeding difficulties, chronic cough, chronic aspiration and choking with feeds are commonly reported symptoms.
13.5.8.3 Diagnosis
The gold standard for diagnosis is direct laryngoscopy and bronchoscopy with palpation of the interarytenoid area.
Both modified barium swallow (MBS) and fiberoptic endoscopic evaluation of swallowing (FEES) can be used to diagnose laryngeal aspiration, while persistent chronic aspiration may be seen on chest X-rays.
13.5.8.4 Medical Management
The first-line treatment of children with symptomatic type 1 clefts is conservative management strategies with feeding therapy and anti-reflux medication. The goal is to achieve adequate nutrition while preventing pulmonary complications [52].
13.5.8.5 Surgery
Surgery should be considered for those patients with type 1 laryngeal clefts who do not respond to medical treatment as well as all type 2, 3 and 4 clefts.
13.5.8.6 Endoscopic
Type 1, type 2 and some type 3 laryngeal clefts can be repaired endoscopically with a suture repair. The endoscopic surgical technique involves removing the opposing mucosa of the cleft with laser or cold steel and then using absorbable sutures with an interrupted one- or two-layer closure.
Some patients may require concurrent supraglottoplasty to prevent postoperative obstruction.
13.5.8.7 Open
Some type 3 and all type 4 clefts require open surgery which often necessitates extracorporeal membrane oxygenation (ECMO) or cardiopulmonary bypass [52] (Fig. 13.10).

(a) Type 2 laryngeal cleft pre-op; (b) post-endoscopic suture repair
Symptomatic type 1, type 2 and some type 3 laryngeal clefts can be repaired endoscopically using an endoscopic suture repair.
13.5.9 Subglottic Haemangioma
13.5.9.1 Introduction
Infantile haemangiomas (IH) are the most common tumours of the head and neck, affecting 4–5% of the paediatric population. For reasons unknown, they affect females more than males and occur more commonly on the left side of the subglottis [13]. They are benign vascular tumours which can occur anywhere in the body. Classically, they develop in the first few months of life and grow rapidly for 3–6 months. This proliferative phase is then followed by an involution phase with regression of the lesion over a few years. Involvement of the subglottic region is rare but can lead to life-threatening airway obstruction. Children with a haemangioma in the beard distribution have a much higher incidence of subglottic haemangiomas. Approximately one-half of infants diagnosed with an airway IH also have a cutaneous IH, although only 1–2% of children with cutaneous IHs also have airway IHs.
Children with both subglottic and cutaneous facial haemangiomas are at significant risk for PHACE syndrome (posterior fossa malformation, haemangiomas, arterial anomalies, coarctation of the aorta/cardiac defects and eye abnormalities).
13.5.9.2 Clinical Features
The primary presenting symptom is biphasic stridor which often begins during the proliferation phase usually at 6–12 weeks old. Subglottic haemangiomas are often mistaken as croup especially because they typically worsen in the presence of an upper respiratory illness. Physicians should have a high index of suspicion in children with a beard distribution cutaneous haemangioma and respiratory symptoms.
13.5.9.3 Diagnosis
The diagnosis of IH can be made on direct visualisation with laryngoscopy and bronchoscopy. Characteristically, a smooth, rounded, vascular-appearing submucosal lesion in the left posterolateral subglottis is seen [13]. In the past, an asymmetrical subglottic narrowing seen on X-ray was considered pathognomonic of a subglottic haemangioma.
Computed tomography (CT) and magnetic resonance imaging (MRI) can provide more information on the degree of luminal narrowing and can differentiate the haemangioma from other vascular anomalies by demonstrating the internal architecture of the lesion.
Definitive diagnosis of PHACE syndrome requires MRI and MRA imaging of the head and neck, echocardiogram including the aortic arch and an ophthalmologic evaluation [53].
13.5.9.4 Management
Treatments for subglottic haemangiomas have evolved over time.
13.5.9.5 Medical Treatment
In 2008, Dr. Leaute-Labreze, a dermatologist from Bordeaux in France, accidentally discovered that propranolol, a nonselective beta-blocker, drastically reduced the size of cutaneous haemangiomas in an infant who had developed hypertrophic obstructive cardiomyopathy as a complication of the child’s initial systemic steroid treatment. Steroid therapy was the first-line treatment of haemangiomas at that time [54].
This discovery has revolutionised the management of haemangiomas and is now the first-line treatment. Side effects of propranolol are rare, but may include bradycardia, hypotension, bronchospasm, hyperkalaemia and hypoglycaemia [55].
Steroids may be helpful in refractory cases, but long-term steroid use carries a significant risk of complications such as severe gastrooesophageal reflux disease, hypertension, hyperglycaemia, osteoporosis and avascular joint necrosis.
13.5.9.6 Surgery
Surgical interventions may be required in children who are resistant to propranolol or in children with PHACE syndrome who are not suitable for propranolol due to the possible increased risk of stroke.
Operative interventions include intralesional injection of corticosteroids, partial ablation of the IH with laser or complete open resection with laryngotracheal reconstruction [56] (Fig. 13.11).

Subglottic haemangioma
Beta-blockers have revolutionised the management of haemangiomas and are now the first-line treatment.
13.5.10 Vallecular Cysts
13.5.10.1 Introduction
Congenital vallecular cysts are a rare cause of stridor in newborn infants. Numerous mucus glands line the vallecula, and ductal obstruction may lead to the formation of a mucous-filled vallecula cyst.
True vallecular cysts have an internal mucosal lining of nonkeratinising squamous or respiratory epithelium and a fibrous wall. Extralaryngeal extension into the neck through the thyrohyoid or cricothyroid membrane has been described [13].
13.5.10.2 Clinical Presentation
Clinical presentation includes stridor, feeding difficulties, failure to thrive and, in some cases, cyanotic episodes. The timing and severity of presentation of vallecular cysts are dependent on the size of cyst and its impact on airway.
13.5.10.3 Diagnosis
The gold standard for diagnosis is direct laryngoscopy under general anaesthesia.
A vallecular cyst may be diagnosed on flexible nasendoscopy although this can be challenging and the vallecula may not be visualised due to the presence of co-existing laryngomalacia.
A lateral airway radiograph may show an alteration in the airway contour in support of the diagnosis, while preoperative CT and MRI can help to determine the size, location and anatomic dimensions of a cyst and to plan for surgical resection.
13.5.10.4 Surgery
Endoscopic marsupialisation is the first-line treatment for the majority. Microlaryngeal scissors or a laser can be used to deroof the cyst.
Simple aspiration of the cyst carries a high risk of recurrence and is not recommended [57].
Rarely, an open approach is required for cases of recurrent cysts or cysts with extensive extralaryngeal extension (Fig. 13.12).

(a) Vallecular cyst; (b) post-CO2 laser excision of vallecular cyst
Endoscopic marsupialisation of vallecular cysts is the first-line treatment for the majority.
13.5.11 Laryngeal Manifestations of Systemic Diseases
13.5.11.1 Laryngeal Sarcoidosis
Laryngeal involvement is uncommon in sarcoidosis. Obstruction is most often supraglottic, due to preferential involvement of the arytenoids, epiglottis and aryepiglottic folds. This is thought to result from a comparatively rich lymphatic supply to this tissue.
First-line therapy remains corticosteroids. Treatment options that have been used with variable success in cases resistant to corticosteroid therapy include immunosuppressive agents such as methotrexate, azathioprine, cyclosporine, hydroxychloroquine, sirolimus and biological agents such as infliximab.
13.5.11.1.1 Surgery
Surgical options such as endoscopic laser photoreduction using carbon dioxide laser are useful in patients with significant airway compromise in order to avoid tracheostomy or in patients unresponsive to steroids [58]. Other approaches that have been used successfully include intralesional steroids, external beam radiotherapy and surgery. Spontaneous resolution of laryngeal sarcoidosis can occur, so watchful waiting is a reasonable strategy for asymptomatic or minimally symptomatic patients [59] (Fig. 13.13).

Laryngeal sarcoidosis
First-line therapy is systemic corticosteroids.
13.5.11.2 Granulomatosis with Polyangiitis of the Larynx
Granulomatosis with polyangiitis (GPA) is a necrotising granulomatous vasculitis primarily affecting the small- and medium-sized vessels.
Any portion of the body may be involved, but most commonly, the upper and lower respiratory tract are affected, with eventual renal involvement. Head and neck manifestations are present in up to 84% at diagnosis, and as such, otolaryngologists need to have a high level of suspicion. Patients may present in adolescence with subglottic stenosis or multilevel obstruction. The course of the disease tends to be relapsing and remitting, but in untreated instances, it can become rapidly fatal.
Treatment for GPA involves steroids as well as immunosuppressants and more recently monoclonal antibodies such as rituximab. Rituximab is a monoclonal anti-CD20 chimeric antibody that was originally used to treat B-cell lymphoma. The therapy depletes B cells as well as the antineutrophil cytoplasmic antibodies (ANCAs).
13.5.11.2.1 Surgery
Surgical approaches include removal of granulation and scar tissue, balloon dilatation and intralesional corticosteroid injections [60] (Fig. 13.14).

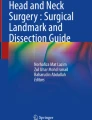
(a) GPA with subglottic stenosis, (b) immediately post-balloon dilatation and steroid injection, and (c) 1-month post-procedure
Surgical approaches include removal of granulation and scar tissue, balloon dilatation and intralesional corticosteroid injections.
13.5.11.3 Neurofibromas of the Larynx
Neurofibromas are benign proliferations of Schwann cells, perineurial cells and fibroblasts. They may occur in isolation, but more commonly, they are associated with neurofibromatosis type 1 or 2. The most common sites of laryngeal involvement include the aryepiglottic folds and the arytenoids, areas of the larynx rich in terminal nerve plexuses.
Neurofibromas may be classified as plexiform (expanding pre-existing nerves), diffuse (growing as a nodule) or both based on their pattern of growth.
Owing to its slow growth and variability of location and size, laryngeal neurofibroma can remain symptom-free for years or become symptomatic at birth.
Further evaluation with CT and MRI can help determine the extent of the lesion.
13.5.11.3.1 Surgery
Choice of treatment for neurofibroma of the larynx is based on the location, extension and severity of symptoms. A conservative approach is advisable when total resection is not possible and the patient has minimal symptoms. Subtotal excision has been the mainstay of therapy because of the propensity for diffuse involvement and poor margin control. Endoscopic laser excision is recommended for patients who present with a small, localised lesion that is accessible via suspension laryngoscopy. Complete resection of laryngeal neurofibroma and preservation of laryngeal functions are often impossible owing to the lesion’s infiltrative nature [61].
Subtotal endoscopic excision has been the mainstay of therapy because of the propensity for diffuse involvement and poor margin control.
References
Daniel M, Cheng A. Neonatal stridor. Int J Pediatr. 2012;2012:859104.
Ongkasuwan J, et al. Laryngeal ultrasound and vocal fold movement in the pediatric cardiovascular intensive care unit. Laryngoscope. 2017;127(1):167–72.
Smillie I, et al. The paediatric voice clinic. Arch Dis Child. 2014;99(10):912–5.
Ongkasuwan J, et al. Transoral rigid 70-degree laryngoscopy in a pediatric voice clinic. Laryngoscope. 2019;129(7):1657–9.
Zur KB, et al. Pediatric Voice Handicap Index (pVHI): a new tool for evaluating pediatric dysphonia. Int J Pediatr Otorhinolaryngol. 2007;71(1):77–82.
Lauder G, et al. Volatiles or TIVA: which is the standard of care for pediatric airway procedures? A pro-con discussion. Pediatr Anesth. 2020;30(3):209–20.
Londino A, Jagannathan N. Anesthesia in diagnostic and therapeutic pediatric bronchoscopy. Otolaryngol Clin N Am. 2019;52(6):1037–48.
Karsli C. Managing the challenging pediatric airway: continuing professional development. Can J Anesth. 2015;62(9):1000–16.
Landry A, Thompson D. Laryngomalacia: disease presentation, spectrum, and management. Int J Pediatr. 2012;2012:1–6.
Olney D, et al. Laryngomalacia and its treatment. Laryngoscope. 1999;109(11):1770–5.
Carter J, et al. International Pediatric ORL Group (IPOG) laryngomalacia consensus recommendations. Int J Pediatr Otorhinolaryngol. 2016;86:256–61.
Del Do M, et al. Supraglottoplasty surgery types 1–3: a practical classification system for laryngomalacia surgery. Int J Pediatr Otorhinolaryngol. 2018;111:69–74.
Parkes W, Propst E. Advances in the diagnosis, management, and treatment of neonates with laryngeal disorders. Semin Fetal Neonatal Med. 2016;21(4):270–6.
Daya H, et al. Pediatric vocal fold paralysis. Arch Otolaryngol Head Neck Surg. 2000;126(1):21.
Lesnik M, et al. Idiopathic bilateral vocal cord paralysis in infants: case series and literature review. Laryngoscope. 2014;125(7):1724–8.
Cohen J, Benyamini L. Voice outcome after vocal fold injection augmentation with carboxymethyl cellulose versus calcium hydroxyapatite. J Laryngol Otol. 2020;134(3):263–9.
Marie JP, et al. Nonselective reinnervation as a primary or salvage treatment of unilateral vocal fold palsy. Laryngoscope. 2020;130(7):1756–63.
Bouhabel S, Hartnick CJ. Current trends in practices in the treatment of pediatric unilateral vocal fold immobility: a survey on injections, thyroplasty and nerve reinnervation. Int J Pediatr Otorhinolaryngol. 2018;109:115–8.
Butskiy O, et al. Surgical interventions for pediatric unilateral vocal cord paralysis: a systematic review. JAMA Otolaryngol Head Neck Surg. 2015;141(7):654–60.
Rutter M, et al. Endoscopic anterior-posterior cricoid split for pediatric bilateral vocal fold paralysis. Laryngoscope. 2017;128(1):257–63.
Dahl J, et al. Endoscopic posterior cricoid split with costal cartilage graft: a fifteen-year experience. Laryngoscope. 2016;127(1):252–7.
Funk R, et al. Factors associated with tracheotomy and decannulation in pediatric bilateral vocal fold immobility. Int J Pediatr Otorhinolaryngol. 2015;79(6):895–9.
Montague GL, Bly RA, Nadaraja GS, Conrad DE, Parikh SR, Chan DK. Endoscopic percutaneous suture lateralization for neonatal bilateral vocal fold immobility. Int J Pediatr Otorhinolaryngol. 2018;108:120–4.
Chen E, Inglis A. Bilateral vocal cord paralysis in children. Otolaryngol Clin N Am. 2008;41(5):889–901.
Lee J, et al. Bilateral selective laryngeal reinnervation for bilateral vocal fold paralysis in children. JAMA Otolaryngol Head Neck Surg. 2020;146(5):401.
Marina M, et al. Laryngeal reinnervation for bilateral vocal fold paralysis. Curr Opin Otolaryngol Head Neck Surg. 2011;19(6):434–8.
Myer CM III, et al. Proposed grading system for subglottic stenosis based on endotracheal tube sizes. Ann Otol Rhinol Laryngol. 1994;103(4):319–23.
Leung R, Berkowitz RG. Incidence of severe acquired subglottic stenosis in newborns. Int J Pediatr Otorhinolaryngol. 2007;71(5):763–8.
Rutter M, Kuo I. Predicting and managing the development of subglottic stenosis following intubation in children. J Pediatr. 2020;96(1):1–3.
Sekioka A, et al. Serial intralesional triamcinolone acetonide injections for acquired subglottic stenosis in premature infants. Pediatr Surg Int. 2018;34(10):1047–52.
Yung KC, et al. A randomized controlled trial of adjuvant mitomycin-c in endoscopic surgery for laryngotracheal stenosis. Laryngoscope. 2020;130(3):706–11.
Bakthavachalam S, McClay JE. Endoscopic management of subglottic stenosis. Otolaryngol Head Neck Surg. 2008;139(4):551–9.
George M, et al. Management of severe pediatric subglottic stenosis with glottic involvement. J Thorac Cardiovasc Surg. 2010;139(2):411–7.
Lim J, et al. Subglottic cysts: the Great Ormond street experience. Int J Pediatr Otorhinolaryngol. 2003;67(5):461–5.
Steehler MK, et al. Management of subglottic cysts with Mitomycin-C—a case series and literature review. Int J Pediatr Otorhinolaryngol. 2011;75(3):360–3.
Hoff SR, Koltai PJ. Operative management of juvenile-onset recurrent respiratory papillomatosis. Oper Tech Otolaryngol Head Neck Surg. 2012;23(2):117–23.
Novakovic D, et al. A prospective study of the incidence of juvenile-onset recurrent respiratory papillomatosis after implementation of a national HPV vaccination program. J Infect Dis. 2018;217(2):208–12.
Lawlor C, et al. International Pediatric Otolaryngology Group (IPOG): juvenile-onset recurrent respiratory papillomatosis consensus recommendations. Int J Pediatr Otorhinolaryngol. 2020;128:109697.
Derkay CS, et al. A staging system for assessing severity of disease and response to therapy in recurrent respiratory papillomatosis. Laryngoscope. 1998;108(6):935–7.
Wiatrak BJ, et al. Recurrent respiratory papillomatosis: a longitudinal study comparing severity associated with human papilloma viral types 6 and 11 and other risk factors in a large pediatric population. Laryngoscope. 2004;114(S104):1–23.
Chadha NK, James A. Adjuvant antiviral therapy for recurrent respiratory papillomatosis. Cochrane Database Syst Rev. 2010;12(12):CD005053.
Birchall MA, Carding P. Vocal nodules management. Clin Otolaryngol. 2019;44(4):497–501.
Cohen W, et al. Development of a minimum protocol for assessment in the paediatric voice clinic. Part 1: Evaluating vocal function. Logopedics Phoniatrics Vocol. 2012;37(1):33–8.
Ongkasuwan J, Friedman EM. Is voice therapy effective in the management of vocal fold nodules in children? Laryngoscope. 2013;123(12):2930–1.
Martins RHG, et al. Clinical practice: vocal nodules in dysphonic children. Eur J Pediatr. 2013;172(9):1161–5.
Hartnick C, et al. Indirect vs direct voice therapy for children with vocal nodules: a randomized clinical trial. JAMA Otolaryngol Head Neck Surg. 2018;144(2):156–63.
Avelino MAG, et al. Congenital laryngeal webs: from diagnosis to surgical outcomes. Braz J Otorhinolaryngol. 2020; https://doi.org/10.1016/j.bjorl.2020.06.018.
Fussey JM, et al. Surgical management of acquired anterior glottic web: a systematic review. J Laryngol Otol. 2019;133(10):867–74.
Chiang T, et al. Surgical management of type I and II laryngeal cleft in the pediatric population. Int J Pediatr Otorhinolaryngol. 2014;78(12):2244–9.
Yeung JC, et al. International Pediatric Otolaryngology Group: consensus guidelines on the diagnosis and management of type I laryngeal clefts. Int J Pediatr Otorhinolaryngol. 2017;101:51–6.
Fraga JC, et al. The association between laryngeal cleft and tracheoesophageal fistula: myth or reality? Laryngoscope. 2015;125(2):469–74.
Johnston DR, et al. Laryngeal cleft: evaluation and management. Int J Pediatr Otorhinolaryngol. 2014;78(6):905–11.
Raol N, et al. Propranolol for the treatment of subglottic hemangiomas. Int J Pediatr Otorhinolaryngol. 2011;75(12):1510–4.
Léauté-Labrèze C, et al. Propranolol for severe hemangiomas of infancy. N Engl J Med. 2008;358(24):2649–51.
Hardison S, et al. The use of propranolol in the treatment of subglottic hemangiomas: a literature review and meta-analysis. Int J Pediatr Otorhinolaryngol. 2016;90:175–80.
Darrow DH. Management of infantile hemangiomas of the airway. Otolaryngol Clin N Am. 2018;51(1):133–46.
Li Y, et al. Vallecular cyst in the pediatric population: evaluation and management. Int J Pediatr Otorhinolaryngol. 2018;113:198–203.
Butler CR, et al. Endoscopic airway management of laryngeal sarcoidosis. Arch Otolaryngol Head Neck Surg. 2010;136(3):251–5.
Kelleher KJ, et al. Treatment-recalcitrant laryngeal sarcoidosis responsive to sirolimus. BMJ Case Rep. 2020;13(8):e235372.
Eustaquio ME, et al. Multilevel airway involvement in children with Wegener’s granulomatosis: clinical course and the utility of a multidisciplinary approach. Arch Otolaryngol Head Neck Surg. 2011;137(5):480–5.
Rahbar R, et al. The biology and management of laryngeal neurofibroma. Arch Otolaryngol Head Neck Surg. 2004;130(12):1400–6.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Lang, B., Mehanna, R., Russell, J. (2022). Laryngeal Surgery in Children. In: Remacle, M., Eckel, H.E. (eds) Textbook of Surgery of Larynx and Trachea. Springer, Cham. https://doi.org/10.1007/978-3-031-09621-1_13
Download citation
DOI: https://doi.org/10.1007/978-3-031-09621-1_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-09620-4
Online ISBN: 978-3-031-09621-1
eBook Packages: MedicineMedicine (R0)