
Abstract
Despite the existence of internationally approved guidelines, the diagnosis of gastroesophageal reflux (GER)-disease remains difficult (Rosen et al. J Pediatr Gastroenterol Nutr. 66:516-54, 2018). GER-disease is generally considered a clinical diagnosis. However, differentiation between physiologic GER, functional regurgitation, and GER-disease in infants and between functional heartburn, hypersensitive esophagus, rumination syndrome, symptoms of esophageal dysfunction, and GER-disease in older children can be difficult based on clinical grounds alone. In addition, some patients present with extra-esophageal problems such as chronic respiratory disease, chronic cough, or ENT problems.
Many diagnostic tests have been proposed, but none of them can truly be seen as a gold standard. Upper gastrointestinal endoscopy with biopsies can show erosive esophagitis and Barrett’s esophagus and is able to differentiate between reflux esophagitis and eosinophilic esophagitis, but cannot show or exclude non-erosive GER-disease. In theory, 24-h pH-impedance testing allows for detecting all GER events and establishing a temporal association between individual GER events and symptoms. However, no true normative data are available and its analysis can be difficult, especially in severe cases with low impedance baselines. Additionally, the statistical calculation of an association between GER and symptoms is dependent on sufficient symptoms and their adequate objective monitoring. A trial with acid suppression can be helpful to diagnose acid-related disease in older children, but not in patients where weakly acidic GER is predominant. The placebo effect of such a trial carries the risk of chronic over-treatment in functional heartburn. Several less invasive tests have been studied, but their diagnostic value is, as yet, limited.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Gastroesophageal reflux
- Gastroesophageal reflux disease
- Esophagus
- Motility
- Eosinophilic esophagitis
- Rumination
- Diagnostics
Introduction
Gastroesophageal reflux (GER), defined as the effortless retrograde flow of gastric contents into the esophagus, is a normal physiologic process occurring multiple times a day in children of all ages. It usually does not lead to symptoms or complications. GER can be liquid and gaseous (belch) and can vary from alkaline (pH > 7) to acid (pH < 4). If GER leads to flow of gastric contents into the oropharynx or above, it is referred to as regurgitation. Vomiting has a different underlying mechanism and leads to forceful expulsion of gastric contents out of the mouth.
GER-disease is defined as GER leading to troublesome symptoms that affect daily functioning or complications [1]. In the pediatric age range, complications include, but are not limited to, esophagitis, Barret’s esophagus, anemia, growth retardation, and extra-esophageal problems (e.g., recurrent pneumonia, dental erosions, cardiorespiratory events in infants and ENT problems).
Diagnosis of GER-disease is primarily based on clinical presentation. A thorough history and physical examination is essential in all patients, not only to differentiate between GER and GER-disease, GER-disease and rumination, and GER-disease and vomiting, but also to rule out other underlying diseases. If there is uncertainty about the diagnosis or a suspicion of complicated disease, additional testing may be necessary. Several diagnostic and therapeutic algorithms are available [1, 2]. The available diagnostic tests are outlined below.
History, Physical Exam, and Questionnaires
Typical Symptoms
Infants
GER-related symptoms, especially regurgitation and crying, are very common in infancy and not necessarily suggestive of or specific for any disease [3,4,5]. Regurgitation occurs at least regularly in 70% of 4 month old infants and at least daily in 13.8% of healthy children ranging from 0–12 months [6,7,8]. If excessive, it may simply be the result of overfeeding, which can be easily corrected [1]. Infants that regurgitate more than once daily for more than 3 weeks (without alarm symptoms) fulfil criteria for infant regurgitation as per Rome IV criteria for functional diseases, but do not suffer from GER-disease [8]. In physiologic GER and infant regurgitation, the regurgitation episodes resolve with age without treatment [3, 6, 9].
On the other hand, GER-disease can cause severe symptoms and complications, while infants may initially present with similar non-specific symptoms like regurgitation and crying.
To discern between physiological GER, infant regurgitation, and GER-disease, it is important to thoroughly evaluate the severity of symptoms as objective as possible and to investigate the presence of more signs and symptoms that may suggest pathology (Table 16.1) or alternative diagnoses. Alarm symptoms as shown in Table 16.2 should prompt for specific diagnostic workup and/or treatment, depending on the suspected disorder.
In addition, information about feeding type, volumes, frequency and associated problems is essential. Feeding problems may be the result of oropharyngeal dysphagia or eosinophilic esophagitis rather than GER-disease. Non-IgE mediated cow’s milk allergy may also present with atypical regurgitation and irritability. Other symptoms of allergy should be asked for and eczema should be specifically looked for during the physical exam. Note that true mono-symptomatic presentation of cow’s milk allergy is rare and, if present, involves dermatitis and not gastrointestinal symptoms [10]. It is, however, not uncommon for parents of patients with cow’s milk allergy to report only symptoms suggestive of GER-disease [11].
Finally, maternal depressive symptoms have been shown to be associated with a threefold higher risk of gastroesophageal reflux symptoms in the infant as compared to infants of mothers without depressive symptoms, so maternal mental health deserves attention during history taking [12, 13].
Several questionnaires have been developed to more objectively score GER-related symptoms in infants [14,15,16,17,18,19,20]. Although the IGERQ-R is most commonly used, was validated for symptom tracking over time [15] and a clinically meaningful difference in its total score was determined [21], it was not validated for the diagnosis of GER-disease, nor was any one of the other questionnaires. Its limited diagnostic value is likely related to the symptoms overlapping between GER-disease and pharyngeal dysphagia [22].
Older Children and Adolescents
New-onset regurgitation or increase thereof after the age of 12 months, should raise the suspicion GER-disease or other diseases that provoke GER. In infants with regurgitaion, which persists after the age of 18 months, true GER-disease should also be considered.
For other symptoms than regurgitation, it is hard to objectify a relation with GER. In toddlers and young children no data exist on the specificity or sensitivity of symptoms. A validated questionnaire exists for children up to 4 years of age, but robust testing of its sensitivity and specificity as compared to an objective reference test is lacking [20]. The same questionnaire was also adapted for, but not validated in children from 5–11 years [23].
With age, symptoms of GER-diseases tend to become more specific and they resemble adult symptomatology in adolescence. A history and physical exam by an expert gastroenterologist has a sensitivity of only 67% and a specificity of 70% for diagnosing GER-disease in adults, indicating that even with increased specificity, the clinical diagnosis of GER-disease remains similarly difficult in adolescents [24].
No diagnostic questionnaires are available for adolescents, but the Pediatric Gastroesophageal Reflux Disease Symptom and Quality of Life Questionnaire (PGSQ) is available for validated symptom assessment in patients from 2 to 17 years old [25]. Some studies in adolescents have used the Reflux Disease Questionnaire, which was purposely developed to separate GER-disease from other causes of upper abdominal and lower retrosternal symptoms in adults, and was thoroughly validated [26]. Its test characteristics approach those of an expert gastroenterologist in adults, but were not tested in adolescents [26, 27].
Extra-Esophageal Symptoms
Many extra-esophageal symptoms have been linked to GER (Table 16.1).
In (premature) infants brief resolved unexplained events (BRUEs) are commonly thought to be GER related. Most studies, however, do not provide evidence for such a relation and oropharyngeal dysphagia seems to be a larger contributing factor in the majority of these children [28,29,30]. Other presentations at different ages, like chronic cough, laryngitis, and wheezing, can be GER related [31, 32] but more common causes should be excluded first, especially when no typical GER-related symptoms are present. If still suspected to be GER related, history should focus on the presence of additional typical GER symptoms and on a possible temporal relation between the symptoms and feeding times. This is similarly true for older children and adolescents [31, 32].
Diagnostic Tests
Proton Pump Inhibitor (PPI) Trial
In infants, the use of PPI as an empiric diagnostic trial is not recommended. In this age group, PPI has been shown to lack additional efficacy as compared to placebo [33]. Because of the very high placebo effect observed in most clinical trials, a PPI-trial as diagnostic test additionally carries a large risk of over-diagnosing GER-disease and subsequent prolonged unnecessary treatment.
In adolescents, it seems reasonable to use a PPI-trial for 4–8 weeks as per adult guidelines, i.e., in treatment naïve patients with typical symptoms of heartburn and/or regurgitation and this test is now incorporated in pediatric guidelines too [1, 34]. Clinical improvement during such a trial has, however, poor test characteristics in adults (sensitivity 54%, specificity 65%, PPV 75% and NPV 41%) and the results should therefore be interpreted with caution, especially in younger children [24]. Unnecessary treatment of patients who respond based on a placebo effect remains a matter of concern in this age group and therapy based on the results of a PPI-trial should therefore be reconsidered regularly.
Endoscopy and Esophageal Biopsies
Endoscopy, albeit considered a relatively safe procedure, is invasive and requires sedation in children. Although clear macroscopic abnormalities during endoscopy confirm GER, negative predictive value is very low, and a normal-looking mucosa does not exclude GER-disease [35, 36]. In patients with GER-diseases, endoscopy can differentiate between erosive and non-erosive disease. Barrett’s esophagus (BE) as a complication of GER-disease, is very rare in children and can be demonstrated only in 0.13% of all children and adolescents undergoing endoscopy with biopsies [37]. Approximately 70% of children with BE have an underlying disorder that predisposes to severe GER-disease [38]. Endoscopy thus has limited clinical consequences when used as a first-line diagnostic test; both erosive esophagitis and non-erosive GER-disease need treatment with acid suppression.
Endoscopy should thus be reserved for patients with therapy-resistant GER-disease, alarm symptoms such as hematemesis, or those in whom another cause of their symptoms is suspected (eosinophilic esophagitis, Crohn’s disease or infectious esophagitis). If an endoscopy is performed, biopsies should be taken to rule out eosinophilic esophagitis and examine microscopic esophagitis, even if no macroscopic abnormalities are seen [1].
Function Tests
High-Resolution Manometry
High-resolution manometry (HRM) cannot be seen as a standard diagnostic test for GER-disease and should be reserved for specific indications in refractory cases. In these children, HRM can have an important role in the diagnostic process. First, many PPI-refractory patients in fact do not have GER-disease, and HRM can help to diagnose motility disorders as described by the Chicago classification, or, when combined with impedance rumination syndrome and supragastric belching [39, 40].
Second, all patients considered for anti-reflux surgery should have a manometry test to exclude rumination syndrome and disorders of esophagogastric junction outflow obstruction (such as achalasia) [41,42,43], accurately show and subtype the presence of a hiatus hernia (HH) [44] and evaluate esophageal peristalsis. Although debated, patients with severe forms of hypomotility may have more post-fundoplication dysphagia, especially when a Nissen fundoplication is performed [45,46,47,48]. In children HRM in combination with impedance has shown promising results in predicting post-fundoplication dysphagia [49, 50].
HRM can accurately localize the position of the lower esophageal sphincter, which can be used to position a 24-hour pH(−impedance) catheter.
Finally, high-resolution impedance manometry can evaluate impedance baseline at the moment of maximal esophageal contraction (contractile segment impedance), which shows promise in augmenting the diagnosis of GER-disease [51, 52]. This metric, however, needs further validation in adults and children, before its role in the diagnostic process can be determined.
24-Hour Esophageal pH—Monitoring
24-Hour esophageal pH monitoring is able to detect pH changes at a single level in the esophagus and thus indirectly measures acid GER. Although esophageal acid exposure is an important factor in symptom generation and the development of complications, especially in older children, this test has some drawbacks, which should be considered when results are interpreted [53].
First, the cut-off value for the amount of acid exposure that is pathological is still a matter of debate, because true normal values are not available with currently used pH-sensors [1]. Early pH-metry studies that used glass electrodes, were validated using other reference standards that have severe limitations [36, 54, 55]. In addition, the most commonly used parameter, the reflux index or acid exposure time (AET), does not answer the essential question whether symptoms are related to GER.
Second, adult pH monitoring results have shown a significant day-to-day variability, which complicates its interpretation [56]. The use of Bravo wireless capsules allows for 48–72 hours of pH recording and was used to show that the variability may be less in children [57]. Nevertheless, Bravo capsules are not widely available and seldomly used in children as they require endoscopy for their placement.
Third, pH monitoring also possesses intrinsic qualities, which limit sensitivity and specificity. First of all, GER episodes are indirectly detected by acidification of the lumen surrounding the pH sensor, which is normally positioned at 3 or 5 cm proximal to the lower esophageal sphincter. Observations have shown marked regional differences in pH levels throughout the esophagus and it is as yet unclear what position of the pH sensor gives best diagnostic results [58]. Second, for standard automated recognition of a GER episode, pH must drop by at least 1 point and to a value lower than 4. As a result, weakly acidic (4 < pH ≤ 7) and alkaline (pH > 7) GER episodes are per definition not detected by standardized esophageal pH monitoring. This is especially problematic in infants, in whom frequent feeding and subsequent buffering of stomach contents causes gastric pH to be only weakly acidic during most of the day [59]. Because most GER episodes occur in the early post-prandial period, when pH in the stomach is highest, it is not surprising that in infants, the majority of GER episodes is weakly acidic and therefore not detected by standardized esophageal pH monitoring [60]. Another consequence of the indirect measurement of GER is that acid re-reflux or “superimposed” acid GER (i.e., acid GER during the period in which the acid of a previous GER episode is still being cleared) is not detected. Finally, the results of pH monitoring are influenced by dietary intake during the test, because acidic food and drinks will also cause a drop in pH in the surroundings of the pH sensor. Dietary restrictions are, therefore, commonly imposed on patients, resulting in test conditions that do not necessarily reflect daily routine. Despite its limitations, esophageal pH monitoring is still performed in many centers worldwide due to the fact that it is readily available, analysis is automated and it is relatively inexpensive. A 24 h pH-metry can be considered in the suspicion of acid-related disease with/without symptom correlation (see below) and to evaluate the efficacy of acid-suppressive therapy in patients with already proven GER-disease [1].
24-Hour Esophageal pH-Impedance Monitoring
With the introduction of pH-impedance monitoring, some disadvantages of pH monitoring seem to have been overcome. Because pH-impedance detects esophageal flow directly, it is possible to detect all GER episodes and classify these into acidic, weakly acidic, and weakly alkaline GER [53]. Due to the multiple measuring sites, the direction of flow can be determined. Hence, GER can be discerned from swallowed material, making dietary restrictions unnecessary. Furthermore, this makes it possible to study the mechanisms of bolus and acid clearance and provides information on the proximal extent of a GER episode which can be helpful for determining a relation between GER and extra-esophageal symptoms [61].
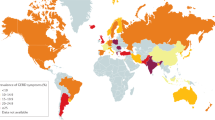
pH-impedance has its limitations, too. Again, normal values do not exist in the pediatric age range, and although efforts to establish these have been made (Fig. 16.1), it is unlikely that truly normative data will ever become available because of ethical considerations preventing the study of healthy children with invasive techniques [60, 62, 63]. Although available and continuously improving, the sensitivity and specificity of the software currently used for automated recognition of MII GER patterns require further optimization and is unlikely to obviate the need for some degree of manual review of the tracing, which makes analysis time-consuming.

Available reference data for the number of GER events per 24 hour and their distribution. From: Singendonk MMJ, Benninga MA, van Wijk MP. Reflux Monitoring in Children. Neurogastroenterol Motil. 2016; 28(10): 1452–9. With permission from John Wiley and Sons
A clear statistical association between GER episodes and symptoms theoretically provides convincing evidence of causality. Multiple statistical measures of association have been described: the symptom index (SI), and the symptom association probability score (SAP) are the most commonly used. The SI is the percentage of symptoms related to a GER episode and is considered positive when above 50% [64]. The SI does not take the total number of GER events into account and, by chance, leaves room for a false positive result when many GER events are present. The SAP was developed to overcome these problems. It is a statistical means (Fisher exact test) of calculating the probability that the symptoms and GER episodes found are unrelated. The p-value of this test is then subtracted from 100% to reveal the SAP [65].
With the ability of pH-impedance to detect all GER episodes, symptom association scores are indeed valuable in the diagnosis of GER-disease. However, several difficulties arise. First, not all patients experience symptoms during a 24-h study period and if they do, reporting is not always accurate [66]. Second, clear criteria defining a temporal association are lacking and are a matter of debate [67].
Apart from detecting GER episodes, pH-impedance tests can be used to evaluate other parameters. Baseline impedance is a marker for mucosal integrity and was shown to be low in infants and children with esophagitis [68, 69]. Its calculation is time-consuming and there is no consensus on which method should be used. Mean nocturnal baseline impedance is a simplified means of calculating baseline impedance and was shown to correlate with AET and esophagitis in adults [70] and with AET in children and could be supportive of a diagnosis of GER-disease [34]. Where the MNBI measures mucosal integrity, another novel metric, the post-reflux swallow-induced peristaltic wave (PSPW) index, is a measure of esophageal clearance. Although not studied in children yet, it was also included in adult guidelines as a measure that can support the diagnosis of GER-disease [34].
In clinics, pH-impedance testing can be used to correlate symptoms with GER episodes in all age groups; to discriminate between the different phenotypes in patients with typical GER symptoms and without esophagitis [71]:
(1) patients with abnormal esophageal acid exposure (non-erosive reflux disease (NERD)); (2) those with a positive symptom association to acid or non-acid reflux but without abnormal AET (reflux hypersensitivity), and (3) patients with normal esophageal acid exposure and a negative symptom association (functional heartburn).
In addition, it can also be used in a patient with persistent symptoms despite acid suppression. Both the efficacy of the medication can be checked and a relation between GER and the persisting symptoms can be found, if present [72].
The role of pH-impedance in confirming supragastric belching, aerophagia, and rumination is beyond the scope of this chapter.
Function Testing in Extra-Esophageal Symptoms
If infants or children present with atypical or extra-esophageal symptoms, other, more common causes of these symptoms should be excluded, before any diagnostic tests for GER-disease are performed. To identify GER as a cause of such symptoms, very few diagnostic tests are available. If a temporal relation between single GER episodes and symptoms can be shown, a causative relation is likely. This can be done using pH monitoring when symptoms are related to acid GER. However, it is likely that especially these symptoms can be related to weakly acidic GER, so symptom association scores using pH-impedance tests can be helpful.
It should be noted that, especially in infants with atypical GER symptoms, functional testing is only appropriate when symptoms are thought to be directly related to bolus GER episodes, and not so much to the cumulative effect of excessive GER. Furthermore every effort should be made to obtain symptoms as objective as possible [66].
Other Tests
Imaging
Barium contrast studies, ultrasound and real-time MRI can be used to show single reflux events. Because reflux episodes in itself are not pathologic, study time is short and it is unlikely that a patient has typical symptoms during the investigation, their diagnostic value is very limited.
However, barium contrast studies and ultrasound have a important role in ruling out anatomical abnormalities and other diseases [1].
Non-invasive Tests
The non-invasive test that is most thoroughly studied, is the presence of pepsin in different body secretions (tracheal fluid, ear effusion, exhaled breath and saliva). Pepsin is the main human digestive protease and is excreted by gastric chief cells as a zymogen, pepsinogen. Salivary pepsin was proposed to be a potential biomarker of GERD in adults and children [73,74,75,76]. Although some adult studies report promising sensitivity and specificity of a salivary pepsin assay as compared to pH-metry or pH-MII [73], it was shown that current test characteristics limit its clinical use [77].
Conclusion
GER-disease is primarily a clinical, yet difficult diagnosis. A PPI-trial may be considered in older children but its limited sensitivity and specificity should be considered when interpreting improvement. If additional testing is required, endoscopy and pH-impedance are the most useful tests and together allow for excluding GER-disease or phenotyping it.
References
Rosen R, Vandenplas Y, Singendonk M, Cabana M, DiLorenzo C, Gottrand F, et al. Pediatric Gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. J Pediatr Gastroenterol Nutr. 2018;66(3):516–54.
Vandenplas Y, Alarcon P. Updated algorithms for managing frequent gastro-intestinal symptoms in infants. Benef Microbes. 2015;6(2):199–208.
Hegar B, Dewanti NR, Kadim M, Alatas S, Firmansyah A, Vandenplas Y. Natural evolution of regurgitation in healthy infants. Acta Paediatr. 2009;98(7):1189–93.
Kramer MS, Barr RG, Dagenais S, Yang H, Jones P, Ciofani L, et al. Pacifier use, early weaning, and cry/fuss behavior: a randomized controlled trial. JAMA. 2001;286(3):322–6.
Curien-Chotard M, Jantchou P. Natural history of gastroesophageal reflux in infancy: new data from a prospective cohort. BMC Pediatr. 2020;20(1):152.
Nelson SP, Chen EH, Syniar GM, Christoffel KK. One-year follow-up of symptoms of gastroesophageal reflux during infancy. Pediatr Practice Res Group Pediatr. 1998;102(6):E67.
Osatakul S, Sriplung H, Puetpaiboon A, Junjana CO, Chamnongpakdi S. Prevalence and natural course of gastroesophageal reflux symptoms: a 1-year cohort study in Thai infants. J Pediatr Gastroenterol Nutr. 2002;34(1):63–7.
Benninga MA, Faure C, Hyman PE, St James Roberts I, Schechter NL, Nurko S. Childhood functional gastrointestinal disorders: neonate/toddler. Gastroenterology. 2016;150(6):1443–55.
Nelson SP, Chen EH, Syniar GM, Christoffel KK. Prevalence of symptoms of gastroesophageal reflux during childhood: a pediatric practice-based survey. Pediatric Practice Research Group. Arch Pediatr Adolesc Med. 2000;154(2):150–4.
Host A, Halken S, Jacobsen HP, Christensen AE, Herskind AM, Plesner K. Clinical course of cow's milk protein allergy/intolerance and atopic diseases in childhood. Pediatr Allergy Immunol. 2002;13(s15):23–8.
Schrander JJ, van den Bogart JP, Forget PP, Schrander-Stumpel CT, Kuijten RH, Kester AD. Cow's milk protein intolerance in infants under 1 year of age: a prospective epidemiological study. Eur J Pediatr. 1993;152(8):640–4.
Ruohomaki A, Toffol E, Airaksinen V, Backman K, Voutilainen R, Hantunen S, et al. The impact of postpartum depressive symptoms on self-reported infant health and analgesic consumption at the age of 12 months: a prospective cohort study. J Psychiatr Res. 2021;136:388–97.
de Kruijff I, Choenni V, Groeneweg JT, Vlieger AM, Benninga MA, Kok R, et al. Gastrointestinal symptoms in infants of mothers with a psychiatric history and the role of depression and bonding. J Pediatr Gastroenterol Nutr. 2019;69(6):662–7.
Kleinman L, Rothman M, Strauss R, Orenstein SR, Nelson S, Vandenplas Y, et al. The infant gastroesophageal reflux questionnaire revised: development and validation as an evaluative instrument. Clin Gastroenterol Hepatol. 2006;4(5):588–96.
Orenstein SR. Symptoms and reflux in infants: infant gastroesophageal reflux questionnaire revised (I-GERQ-R)--utility for symptom tracking and diagnosis. Curr Gastroenterol Rep. 2010;12(6):431–6.
Orenstein SR, Shalaby TM, Cohn JF. Reflux symptoms in 100 normal infants: diagnostic validity of the infant gastroesophageal reflux questionnaire. Clin Pediatr (Phila). 1996;35(12):607–14.
Salvatore S, Hauser B, Vandemaele K, Novario R, Vandenplas Y. Gastroesophageal reflux disease in infants: how much is predictable with questionnaires, pH-metry, endoscopy and histology? J Pediatr Gastroenterol Nutr. 2005;40(2):210–5.
Pados BF, Repsha C, Hill RR. The gastrointestinal and Gastroesophageal reflux (GIGER) scale for infants and toddlers. Glob Pediatr Health. 2021;8:2333794X211033130.
Riley AW, Trabulsi J, Yao M, Bevans KB, DeRusso PA. Validation of a parent report questionnaire: the infant gastrointestinal symptom questionnaire. Clin Pediatr (Phila). 2015;54(12):1167–74.
Deal L, Gold BD, Gremse DA, Winter HS, Peters SB, Fraga PD, et al. Age-specific questionnaires distinguish GERD symptom frequency and severity in infants and young children: development and initial validation. J Pediatr Gastroenterol Nutr. 2005;41(2):178–85.
Smith AB, Fawkes N, Kotze H, Hodgkinson V, Coyle C. Clinically meaningful difference for the infant Gastroesophageal questionnaire revised version (I-GERQ-R): a quantitative synthesis. Patient Relat Outcome Meas. 2020;11:87–93.
Duncan DR, DiFilippo C, Kane M, Lurie M, McSweeney ME, Rosen RL. Overlapping symptoms of gastroesophageal reflux and aspiration highlight the limitations of validated questionnaires. J Pediatr Gastroenterol Nutr. 2021;72(3):372–7.
Tolia V, Bishop PR, Tsou VM, Gremse D, Soffer EF, Comer GM, et al. Multicenter, randomized, double-blind study comparing 10, 20 and 40 mg pantoprazole in children (5-11 years) with symptomatic gastroesophageal reflux disease. J Pediatr Gastroenterol Nutr. 2006;42(4):384–91.
Dent J, Vakil N, Jones R, Bytzer P, Schoning U, Halling K, et al. Accuracy of the diagnosis of GORD by questionnaire, physicians and a trial of proton pump inhibitor treatment: the diamond study. Gut. 2010;59(6):714–21.
Kleinman L, Nelson S, Kothari-Talwar S, Roberts L, Orenstein SR, Mody RR, et al. Development and psychometric evaluation of 2 age-stratified versions of the pediatric GERD symptom and quality of life questionnaire. J Pediatr Gastroenterol Nutr. 2011;52(5):514–22.
Shaw MJ, Talley NJ, Beebe TJ, Rockwood T, Carlsson R, Adlis S, et al. Initial validation of a diagnostic questionnaire for gastroesophageal reflux disease. Am J Gastroenterol. 2001;96(1):52–7.
Bolier EA, Kessing BF, Smout AJ, Bredenoord AJ. Systematic review: questionnaires for assessment of gastroesophageal reflux disease. Dis Esophagus. 2015;28(2):105–20.
Smits MJ, van Wijk MP, Langendam MW, Benninga MA, Tabbers MM. Association between gastroesophageal reflux and pathologic apneas in infants: a systematic review. Neurogastroenterol Motil. 2014;26(11):1527–38.
Duncan DR, Amirault J, Mitchell PD, Larson K, Rosen RL. Oropharyngeal dysphagia is strongly correlated with apparent life-threatening events. J Pediatr Gastroenterol Nutr. 2017;65(2):168–72.
Duncan DR, Growdon AS, Liu E, Larson K, Gonzalez M, Norris K, et al. The impact of the American Academy of Pediatrics brief resolved unexplained event guidelines on gastrointestinal testing and prescribing practices. J Pediatr. 2019;211:112–9 e4.
Borrelli O, Marabotto C, Mancini V, Aloi M, Macrì F, Falconieri P, et al. Role of gastroesophageal reflux in children with unexplained chronic cough. J Pediatr Gastroenterol Nutr. 2011;53(3):287–92.
Zenzeri L, Quitadamo P, Tambucci R, Ummarino D, Poziello A, Miele E, et al. Role of non-acid gastro-esophageal reflux in children with respiratory symptoms. Pediatr Pulmonol. 2017;52(5):669–74.
van der Pol RJ, Smits MJ, van Wijk MP, Omari TI, Tabbers MM, Benninga MA. Efficacy of proton-pump inhibitors in children with gastroesophageal reflux disease: a systematic review. Pediatrics. 2011;127(5):925–35.
Gyawali CP, Kahrilas PJ, Savarino E, Zerbib F, Mion F, Smout A, et al. Modern diagnosis of GERD: the Lyon consensus. Gut. 2018;67(7):1351–62.
Ravelli AM, Villanacci V, Ruzzenenti N, Grigolato P, Tobanelli P, Klersy C, et al. Dilated intercellular spaces: a major morphological feature of esophagitis. J Pediatr Gastroenterol Nutr. 2006;42(5):510–5.
Arasu TS, Wyllie R, Fitzgerald JF, Franken EA, Siddiqui AR, Lehman GA, et al. Gastroesophageal reflux in infants and children comparative accuracy of diagnostic methods. J Pediatr. 1980;96(5):798–803.
El-Serag HB, Gilger MA, Shub MD, Richardson P, Bancroft J. The prevalence of suspected Barrett's esophagus in children and adolescents: a multicenter endoscopic study. Gastrointest Endosc. 2006;64(5):671–5.
Putra J, Arva NC, Tan SY, Melin-Aldana H, Bass LM, Mitchell PD, et al. Barrett esophagus and intestinal metaplasia of the Gastroesophageal junction in children: a Clinicopathologic study. J Pediatr Gastroenterol Nutr. 2020;70(5):562–7.
Herregods TV, Troelstra M, Weijenborg PW, Bredenoord AJ, Smout AJ. Patients with refractory reflux symptoms often do not have GERD. Neurogastroenterol Motil. 2015;27(9):1267–73.
Gyawali CP, Penagini R. Clinical usefulness of esophageal high resolution manometry and adjunctive tests: an update. Dig Liver Dis. 2021;53(11):1373–80.
Yadlapati R, Kahrilas PJ, Fox MR, Bredenoord AJ, Prakash Gyawali C, Roman S, et al. Esophageal motility disorders on high-resolution manometry: Chicago classification version 4.0((c)). Neurogastroenterol Motil. 2021;33(1):e14058.
Smits M, van Lennep M, Vrijlandt R, Benninga M, Oors J, Houwen R, et al. Pediatric achalasia in the Netherlands: incidence, clinical course, and quality of life. J Pediatr. 2016;169:110–5 e3.
Fisichella PM, Raz D, Palazzo F, Niponmick I, Patti MG. Clinical, radiological, and manometric profile in 145 patients with untreated achalasia. World J Surg. 2008;32(9):1974–9.
Gyawali CP, Roman S, Bredenoord AJ, Fox M, Keller J, Pandolfino JE, et al. Classification of esophageal motor findings in gastro-esophageal reflux disease: conclusions from an international consensus group. Neurogastroenterol Motil. 2017;29(12):e13104.
Tran S, Gray R, Kholmurodova F, Thompson SK, Myers JC, Bright T, et al. Laparoscopic fundoplication is effective treatment for patients with Gastroesophageal reflux and absent esophageal contractility. J Gastrointest Surg. 2021;25(9):2192–200.
van Hoeij FB, Bredenoord AJ. Clinical application of esophageal high-resolution manometry in the diagnosis of esophageal motility disorders. J Neurogastroenterol Motil. 2016;22(1):6–13.
Watson DI, Jamieson GG, Bessell JR, Devitt PG. Laparoscopic fundoplication in patients with an aperistaltic esophagus and gastroesophageal reflux. Dis Esophagus. 2006;19(2):94–8.
Chan WW, Haroian LR, Gyawali CP. Value of preoperative esophageal function studies before laparoscopic antireflux surgery. Surg Endosc. 2011;25(9):2943–9.
Loots C, van Herwaarden MY, Benninga MA, VanderZee DC, van Wijk MP, Omari TI. Gastroesophageal reflux, esophageal function, gastric emptying, and the relationship to dysphagia before and after antireflux surgery in children. J Pediatr. 2013;162(3):566–73.e2.
Omari T, Connor F, McCall L, Ferris L, Ellison S, Hanson B, et al. A study of dysphagia symptoms and esophageal body function in children undergoing anti-reflux surgery. United European Gastroenterol J. 2018;6(6):819–29.
Horton A, Posner S, Sullivan B, Cornejo J, Davis A, Fields M, et al. Esophageal contractile segment impedance from high-resolution impedance manometry correlates with mean nocturnal baseline impedance and acid exposure time from 24-hour pH-impedance monitoring. Dis Esophagus. 2020;33(12):doaa063.
Cock C, Chen CL, Lei WY. Diagnostic utility of contractile segment impedance for the diagnosis of gastro-esophageal reflux disease. Gastroenterology. 2018;156:S-224.
Sifrim D. Acid, weakly acidic and non-acid gastro-oesophageal reflux: differences, prevalence and clinical relevance. Eur J Gastroenterol Hepatol. 2004;16(9):823–30.
Cucchiara S, Minella R, Iervolino C, Franco MT, Campanozzi A, Franceschi M, et al. Omeprazole and high dose ranitidine in the treatment of refractory reflux oesophagitis. Arch Dis Child. 1993;69(6):655–9.
Boix-Ochoa J, Lafuenta JM, Gil-Vernet JM. Twenty-four hour exophageal pH monitoring in gastroesophageal reflux. J Pediatr Surg. 1980;15(1):74–8.
Yadlapati R, Ciolino JD, Craft J, Roman S, Pandolfino JE. Trajectory assessment is useful when day-to-day esophageal acid exposure varies in prolonged wireless pH monitoring. Dis Esophagus. 2018;32(3):doy077.
Ravi A, Gunasekaran T, Berman J. Continuous 48-hour wireless esophageal pH monitoring in children: comparison between days 1 and 2. J Pediatr Gastroenterol Nutr. 2016;62(1):87–9.
Emerenziani S, Ribolsi M, Sifrim D, Blondeau K, Cicala M. Regional oesophageal sensitivity to acid and weakly acidic reflux in patients with non-erosive reflux disease. Neurogastroenterol Motil. 2009;21(3):253–8.
Omari TI, Davidson GP. Multipoint measurement of intragastric pH in healthy preterm infants. Arch Dis Child Fetal Neonatal Ed. 2003;88(6):F517–20.
López-Alonso M, Moya MJ, Cabo JA, Ribas J, del Carmen MM, Silny J, et al. Twenty-four-hour esophageal impedance-pH monitoring in healthy preterm neonates: rate and characteristics of acid, weakly acidic, and weakly alkaline gastroesophageal reflux. Pediatrics. 2006;118(2):e299–308.
Thilmany C, Beck-Ripp J, Griese M. Acid and non-acid gastro-esophageal refluxes in children with chronic pulmonary diseases. Respir Med. 2007;101(5):969–76.
Pilic D, Frohlich T, Noh F, Pappas A, Schmidt-Choudhury A, Kohler H, et al. Detection of gastroesophageal reflux in children using combined multichannel intraluminal impedance and pH measurement: data from the German pediatric impedance group. J Pediatr. 2011;158(4):650–4 e1.
Mousa H, Machado R, Orsi M, Chao CS, Alhajj T, Alhajj M, et al. Combined multichannel intraluminal impedance-pH (MII-pH): multicenter report of normal values from 117 children. Curr Gastroenterol Rep. 2014;16(8):400.
Wiener GJ, Richter JE, Copper JB, Wu WC, Castell DO. The symptom index: a clinically important parameter of ambulatory 24-hour esophageal pH monitoring. Am J Gastroenterol. 1988;83(4):358–61.
Weusten BL, Roelofs JM, Akkermans LM, Van Berge-Henegouwen GP, Smout AJ. The symptom-association probability: an improved method for symptom analysis of 24-hour esophageal pH data. Gastroenterology. 1994;107(6):1741–5.
Rosen R, Amirault J, Giligan E, Khatwa U, Nurko S. Intraesophageal pressure recording improves the detection of cough during multichannel intraluminal impedance testing in children. J Pediatr Gastroenterol Nutr. 2014;58(1):22–6.
Omari TI, Schwarzer A, vanWijk MP, Benninga MA, McCall L, Kritas S, et al. Optimisation of the reflux-symptom association statistics for use in infants being investigated by 24-hour pH impedance. J Pediatr Gastroenterol Nutr. 2011;52(4):408–13.
Jadcherla SR, Hanandeh N, Hasenstab KA, Nawaz S. Differentiation of esophageal pH-impedance characteristics classified by the mucosal integrity marker in human neonates. Pediatr Res. 2019;85(3):355–60.
Cohen Sabban J, Bertoldi GD, Ussher F, Christiansen S, Lifschitz C, Orsi M. Low-impedance baseline values predict severe esophagitis. J Pediatr Gastroenterol Nutr. 2017;65(3):278–80.
Frazzoni L, Frazzoni M, De Bortoli N, Ribolsi M, Tolone S, Russo S, et al. Application of Lyon consensus criteria for GORD diagnosis: evaluation of conventional and new impedance-pH parameters. Gut. 2021; https://doi.org/10.1136/gutjnl-2021-325531.
Mahoney LB, Nurko S, Rosen R. The prevalence of Rome IV nonerosive esophageal phenotypes in children. J Pediatr. 2017;189:86–91.
Rosen R, Lord C, Nurko S. The sensitivity of multichannel intraluminal impedance and the pH probe in the evaluation of gastroesophageal reflux in children. Clin Gastroenterol Hepatol. 2006;4(2):167–72.
Hayat JO, Gabieta-Somnez S, Yazaki E, Kang JY, Woodcock A, Dettmar P, et al. Pepsin in saliva for the diagnosis of gastro-oesophageal reflux disease. Gut. 2015;64(3):373–80.
Dy F, Amirault J, Mitchell PD, Rosen R. Salivary pepsin lacks sensitivity as a diagnostic tool to evaluate Extraesophageal reflux disease. J Pediatr. 2016;177:53–8.
Farhath S, He Z, Saslow J, Soundar S, Amendolia B, Bhat V, et al. Detection of pepsin in mouth swab: correlation with clinical gastroesophageal reflux in preterm infants. J Matern Fetal Neonatal Med. 2013;26(8):819–24.
Luebke K, Samuels TL, Chelius TH, Sulman CG, McCormick ME, Kerschner JE, et al. Pepsin as a biomarker for laryngopharyngeal reflux in children with laryngomalacia. Laryngoscope. 2017;127(10):2413–7.
Woodland P, Singendonk MMJ, Ooi J, Nikaki K, Wong T, Lee C, et al. Measurement of salivary pepsin to detect Gastroesophageal reflux disease is not ready for clinical application. Clin Gastroenterol Hepatol. 2018;17(3):563–5.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
van Wijk, M. (2022). Diagnosis of GERD. In: Vandenplas, Y. (eds) Gastroesophageal Reflux in Children. Springer, Cham. https://doi.org/10.1007/978-3-030-99067-1_16
Download citation
DOI: https://doi.org/10.1007/978-3-030-99067-1_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-99066-4
Online ISBN: 978-3-030-99067-1
eBook Packages: MedicineMedicine (R0)