
Abstract
Mobility impairment has deleterious effects at various levels, affecting the functional capacity of people, being more evident in the elderly population. The approach to the elderly person subject to mobility restriction should include a rehabilitation program that integrates early mobilization and the RNSN will be an important professional for this goal to be achieved. It is of interest to know the sensitive indicators for RN care, which allow measuring the gains in health, in terms of functionality and quality of life. Objective: To identify the indicators sensitive to RN care, at the level of functionality, in the elderly with mobility impairment, inserted in rehabilitation programs. Methodology: Performed SLR through the EBSCO Host platform, including the databases: Academic Search Complete; Business Source Complete; CINAHL Plus with full text; ERIC; Library, Information Science & Technology Abstracts; MedicLatina; MEDLINE with full text; Psychology and Behavioral Sciences Collection; Regional Business News; SPORTDiscus with full text, using the PICO method. Results: A total of 37 indicators sensitive to RN care are identified, with the outcome dimension producing the greatest number of indicators, supporting the importance of results in achieving health gains. Conclusions: In order to achieve health gains, the interventions of the RNSN should be guided by specific indicators. Thirty-seven indicators sensitive to Nursing Rehabilitation care were identified, dominating indicators within the outcome dimension, highlighting the importance of the results achieved in the translation of health gains. We highlight indicators that aim at maximizing the functional capacities of people, through rehabilitation programs, promoting muscle movement and walking, as a way to prevent or counteract the harmful effects of immobility.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others

Keywords
1 Introduction
Aging may be characterized by the complex interaction between the processes of cellular aging and multi-organ system, with environmental, physical, psychological, and social factors, leading to biological changes that deteriorate the person's defense and homeostasis mechanisms. As a consequence, the disease process is more frequent, and some pathologies predominate and coexist simultaneously, precipitating an exponential increase of multi-morbidities, since this phenomenon is associated with increased average life expectancy [1].
Supporting this trend, the World Health Organization (WHO) [2] marks an increase in life expectancy from 66.5 years to 72 years, for the period between 2000 and 2016, and for the same period and as for healthy life expectancy, it marks an increase from 58.5 years to 63.3 years. In Portugal, there has been an increase in average life expectancy at birth from 67.1 years in 1970 to 80.9 years in 2018, and life expectancy at age 65 corresponding to the same period, increases from 13.5 years to 19.6 years [3].
In 2019, the elderly population in Portugal was around 2,262,325 representing 22% of the general population, whereas in 1971 the proportion was 9.7%. The ageing rate in Portugal has also been increasing, from 101.6% in 2001 to 161.3% in 2019 [3].
According to EUROSTAT [4], healthy life expectancy at age 65 in Portugal was 7.3 years in 2018, noting also that, according to PORDATA [3], the total dependency ratio in Portugal in the year 2019 was 55.3%, with 34.2% relating to the elderly dependency ratio. Portugal can be portrayed as a country that has a low birth rate, an aging population, and multiple chronic pathology [5], and in the short and long term, the increase in the number of these chronic diseases implies an increase in the prevalence of functional disability [6].
Functional limitations and declining physical and mental well-being increase with age, and few lifestyle interventions are available to prevent adverse events in frail or pre-frail elderly [7].
According to Fonseca and Lopes [8], international organizations such as the WHO, the United Nations (UN) and the European Commission (EC) advocate a restructuring of health systems, not only aimed at the disease, but also focusing on issues such as functionality, promoting its sustainability by increasing the activity of people aged 65 and over, promoting active aging, since, with the global trend towards population aging, health care consumption and associated costs tend to increase in the future [7].
Høy et al. (2007) cited by Fonseca [8], point to self-care as a health resource, since intervening in it increases functional status and decreases health care costs.
Orem, through his theory of self-care deficit, conceptualizes that everyone has the potential for self-care, with skills and experience throughout life. However, when the demands of self-care are greater than the ability to perform them, they need support, either from caregivers (family, friends, neighbors), or from health professionals, namely nurses [9].
It seems essential to us, agreeing with Petronilho and Machado [9], given the aging population and the high prevalence of chronic diseases, we must move towards the production of knowledge, through intervention models that address sustainable responses, adapting to the needs of self-care, from a perspective of functionality and promoting the autonomy of people.
Most adults preserve their ability to mobilize until they are allowed to, that is, until it is restricted, compromised, or causes pain, realizing that movement is essential for the person to interact with the environment, and problems resulting from immobility are readily apparent in the person's health [10] and believing that the major goal for most people, and more specifically for the elderly population, is to maintain their independence and live at home as long as possible [7].
Periods of acute inactivity, or bed rest associated with hospitalization or illness, pose a real threat to muscle tissue and functional capacity. Even for people who ambulated before the disease process, immobility is common during hospitalization. Particularly in the elderly, physical inactivity during hospitalization is almost accepted as part of the hospitalization experience, but leads to markedly negative outcomes, including a reduced ability to perform activities of daily living (ADLs), an increased incidence of readmissions, and increased length of stay [11], as well as admissions to convalescent units and long-term care facilities [12].
Immobility and functional limitation represent enormous challenges and can promote processes of increased pain, incontinence, balance changes, as well as depressive syndromes, disorientation, and irritability [10], leading health professionals, with emphasis on the Rehabilitation Nursing Specialist Nurse (RNSN), to permanently seek strategies that help optimize the functional abilities of people, particularly the elderly [13].
The functional mobility may be altered, due to a physical or clinical situation, derived from certain pathologies, surgeries or injuries, with possible repercussions at the respiratory, cardiovascular, gastrointestinal, musculoskeletal, genitourinary, metabolic, cutaneous, neurological levels, among others [14, 15].
Inactivity and loss of innervation promote a decline in muscle mass, strength, and endurance, and can lead to neuromuscular, pulmonary, cognitive, and quality of life complications that can endure over time [15].
Supported by scientific and technological advances, it is promoted that the restriction of mobility, as an adjunct to the therapeutic process, is prescribed less and less frequently, since the negative effects of immobility are now recognized. The early recovery, after a prolonged disease situation, is essential to try to revert the harmful picture of organic alterations, potentiated by immobility/inactivity, being particularly more important in the elderly population, which is itself more vulnerable to the effects of mobility alterations [14].
With the evolution of scientific knowledge, an earlier mobilization is now possible, decreasing the risks associated with mobility alterations/immobility syndrome, which can, by themselves, have more serious consequences than the pathology that originated them [14], aiming at progressive mobility, minimizing its loss and optimizing autonomy, being important in terms of gains in functional capacity, independence of the person and improvement in quality of life [15].
Even in people admitted to Intensive Care Units (ICUs) who, due to multiple etiologies, including medication-associated effects, electrolyte changes, and systemic dysfunctions, are more limited in mobility and where bed rest was often used as a therapeutic modality, we have witnessed a paradigm shift, with the promotion of early mobilization, as a way to avoid complications associated with immobility and avoid more or less permanent disabilities in people, when they return home, and also showing results, with improvement in some indicators, such as, length of stay either in ICU or hospital, time needed to wean from mechanical ventilation, incidence of delirium and also in terms of readmission rates [11, 16].
Early mobilization plays an important role, too, for a successful hospital-to-home transition process [11].
Hoeman [10] points to benefits in the person's overall health status, namely in age-related changes in muscle function, in the practice of both aerobic and strength training exercises. Benefits are also pointed to load exercises, both in terms of strength, postural stability, and the ability to be alert.
Regular exercise, appropriate to the patient's situation and functional goals are beneficial, and before the person is clinically stabilized, the goal is to prevent contractures or atrophy, as well as to avoid joint pain or injury, maintain muscle tone, strength, and function. The exercise should also be adapted in order to conserve energy and avoid fatigue [10].
For Dirkes and Kozlowski [11], the nurse plays an important role in promoting early mobilization, even in people hospitalized in critical care units, a view also shared by Cerqueira and Grilo [17], who argue that the RNSN working in an ICU has a key role in the design and implementation of rehabilitation programs, in order to minimize the consequences of immobility, including respiratory, motor and functional, and Hoeman [10], believes that the RNSN helps patients develop their potential, optimizing function and advocating for patients to achieve maximum autonomy and independence, outlining appropriate goals together with the person that promote quality of life and satisfaction. For Hoeman [10], therapeutic interventions for mobility and self-care are a cornerstone of rehabilitation nursing care, and maintaining mobility is of utmost importance to avoid complications associated with immobility and for the efficient performance of ADL and instrumental activities of daily living (IADL).
Therefore, an adjusted planning of nursing care, including interventions directed to the maintenance of mobility, promoting self-care, is a fundamental contribution to avoid these complications [14].
The care we provide must be adapted throughout the life cycle, and there are certain specificities associated with old age that must be taken into account and where rehabilitation nursing plays a key role, not only by producing scientific evidence for the development of specific care plans, but also in their execution [13].
Supporting the analysis about the importance of the RNSN intervention, at the level of self-care and ADL, we point out that it is written in the Regulation of the specific skills of the RNSN, (Regulation no. 392/2019 of May 3) [18], as some of its competence units, that this professional “designs intervention plans with the purpose of promoting adaptive capacities, aiming at self-control and self-care in health/illness and/or disability transition processes” and “designs and implements ADL training program aiming at adapting to mobility limitations and maximizing autonomy and quality of life” [18] (p. 13567).
The RNSN develops its practice based on evidence, oriented to results, responding to people's specific needs and to new demands in terms of care, using sensitive indicators for Rehabilitation Nursing (RN) care, in order to assess health gains, both in terms of empowerment, autonomy and quality of life [18, 19].
Assuming that the approach to the elderly person subject to mobility restriction, in different contexts, should include a rehabilitation program that integrates early mobilization and that the RNSN is an important professional for this goal to be achieved, it is of interest to know the sensitive indicators of RN care, which allows assessing the health gains in terms of functionality and quality of life, through a Systematic Literature Review (SLR), formulating the following question: “What are the sensitive indicators of RN care in terms of functionality, in the elderly person with mobility impairment, through a rehabilitation program?” following the PICO methodology.
2 Methodology
SLR seeks to aggregate evidence that meets pre-defined eligibility criteria in order to answer a particular research question, trying to minimize any bias by making use of systematic, explicit, and reproducible methods [20].
In building this SLR, we followed the guidelines of the Joanna Briggs Institute (JBI) and, using the PICO method (P - Participants; I - Intervention; C - Context/Control; O - Outcomes), we defined inclusion criteria that allowed us to select the appropriate studies according to the research question formulated, as shown below: P - People aged 65 years or older, with mobility impairment; I - Submitted to a Rehabilitation program; C - At the level of functionality; O - Sensitive indicators to Rehabilitation Nursing.
A search was carried out on the EBSCO Host - Research Databases platform, in January 2021, selecting all available databases: Academic Search Complete; Business Source Complete; CINAHL Plus with full text; ERIC; Library, Information Science & Technology Abstracts; MedicLatina; MEDLINE with full text; Psychology and Behavioral Sciences Collection; Regional Business News; SPORTDiscus with full text, using the validated descriptors, either by MeSH (Medical Subject Heading) or by CINAHL Subject Headings: “nursing”, “nursing interventions”, “nursing care”, “outcomes”, “nursing outcomes”, “education”, “physical mobility”, “elderly”, “geriatrics” and “self-care”, using the Booleans “AND” and “OR” and respecting the search inclusion criteria: full text available, in the English language, for publications dated between the year 2015 and 2020.
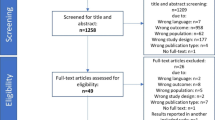
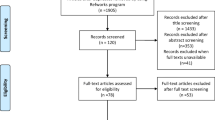
The search resulted in a total of 208 articles, which, after eliminating duplicate results, derives in 103 records for title and abstract analysis. After reading the titles/abstracts, 90 records are eliminated for not fitting the theme of the study, resulting in 13 articles for full-text analysis. From the full-text analysis, four articles were excluded for not meeting the inclusion criteria and one for not providing access to the full text, resulting in a total of eight articles to be included in this review.
Articles were submitted to JBI Critical Appraisal Tools evaluation of methodological quality and levels of evidence [21, 22], meeting more than 50% of the proposed quality criteria. All articles were analyzed by two authors.
In a systematized way, the flow chart in Fig. 1 details the research path:

Research methodology, PRISMA type [23]
3 Results and Discussion
From the search carried out, the articles identified in Table 1 appear as the result:
The idea of quality in health care is brought to us by the Donabedian theory, which proposes three essential components - structure, process, and outcome - that are interconnected and evolve sequentially, in the sense that the quality of the structure promotes quality to the process and, in turn, the quality of the process adds quality to the outcome. «Structure» is understood as the physical space, material, human and organizational resources where health care takes place; «process» can be understood as the sum of care actions and interpersonal relationships and «outcome» is what emerges from the care provided [24].
Thus, based on this perspective, we found sensitive indicators for RN care, with the purpose of promoting the intervention of the RNSN, in order to obtain health gains, promoting the continuous improvement of the quality of care provided to people [25].
In Table 2, we analyze the sensitive indicators of RN care to the elderly person with mobility impairment, at the level of functionality, in a rehabilitation program, which stand out from the selected articles.
It was possible to identify 37 indicators that stand out from the theme under study.
In the “structure” dimension, indicators referring to the use of scales and equipment, both for the evaluation of body balance and muscle movement, and also in the scope of the organization of RN care, stand out, regarding the time available for nurses to develop their care, also standing out in the work of Young et al. [28], other barriers that influence the intervention of these professionals.
In the dimension «process», stands out, largely, the indicator «Percentage of clients for whom a rehabilitation plan and/or program was applied to maximize functional abilities» within the scope of health promotion, followed by indicators for muscle movement, standing, and walking, respectively, «Percentage of clients with potential to improve knowledge of muscle and joint exercise techniques», «Percentage of clients with potential to improve ability to perform muscle and joint exercise techniques»; «Percentage of clients with potential to improve knowledge about adaptation technique for standing up», «Percentage of clients with potential to improve ability to use adaptation technique to stand up»; «Percentage of clients with potential to improve knowledge about walking adaptation technique»; «Percentage of clients with potential to improve walking ability».
In the dimension «outcome», the emphasis is on indicators related to muscle movement, «Gains in improved muscle movement», «Gains in knowledge about muscle and joint exercise techniques» and «Gains in ability to perform muscle and joint exercise techniques», followed by those related to walking «Gains in knowledge about walking adaptation technique» and «Gains in walking ability».
The outcome dimension is the one that produces the largest number of indicators in this review, meeting the importance of results, which translate into health gains, through sensitive indicators to RN care and since this is not a watertight system, it also demonstrates the importance of proper planning and intervention in care.
In line with what has been previously explained, the indicators related to the application of a rehabilitation program to maximize the functional capacities of people and those that are directly related to muscle movement and walking stand out, confirming that one should counteract the adverse effects caused by immobility, especially to a more fragile group such as the elderly, through structured rehabilitation programs that include joint mobilization interventions with muscle strengthening, in order to maximize the person's functionality, promoting mobility and gait.
4 Conclusions
Aiming at excellence of care, and to obtain health gains, the RNSN's interventions must be evidence-based and guided by specific indicators for its intervention.
From the studies analyzed, we were able to identify 37 indicators sensitive to RN care, for the intervention with the elderly person with mobility impairment, through a rehabilitation program.
Indicators within the "outcome" dimension dominate, highlighting the importance of the results achieved in the translation of health gains through the RN intervention. It is also highlighted indicators that aim to maximize the functional capacities of people, through rehabilitation programs, promoting muscle movement and walking, to prevent or counteract the deleterious effects of immobility.
More studies are needed, in the promotion of sensitive indicators of RN care, especially in the dimension «structure», having been the one that was least developed throughout this work.
References
Faria, M., Ramalho, J., Nunes, A., Fernandes, A. (coords.): Visões sobre o envelhecimento. IPBeja Editorial, Beja (2020)
World Health Organization: World health statistics 2021: monitoring health for the SDGs, sustainable development goals ISBN. World Health Organization (2021). https://www.who.int/publications/i/item/world-health-statistics-2019-monitoring-health-for-the-sdgs-sustainable-development-goals
PORDATA: Base de Dados de Portugal Contemporâneo (2020). https://www.pordata.pt/Portugal
EUROSTAT: EUROSTAT data Browser - Healthy life years at age 65 by sex (2020). https://ec.europa.eu/eurostat/databrowser/view/tepsr_sp320/default/table?lang=en
Ministério da Saúde: Direção Geral da Saúde: Plano nacional de saúde: Revisão e extensão a 2020. Direção Geral da Saúde (2015). http://1nj5ms2lli5hdggbe3mm7ms5-wpengine.netdna-ssl.com/files/2015/06/Plano-Nacional-de-Saude-Revisao-e-Extensao-a-2020.pdf.pdf
Menoita, E. (ed.): Reabilitar a pessoa idosa com AVC. Lusociência, Loures (2012)
van Lieshout, M.R.J., Bleijenberg, N., Schuurmans, M.J., de Wit, N.J.: The effectiveness of a proactive multicomponent intervention program on disability in independently living older people: a randomized controlled trial. J. Nutr. Heal. Aging 22, 1051–1059 (2018). https://doi.org/10.1007/s12603-018-1101-x
Fonseca, C., Lopes, M.: Modelo de autocuidado para pessoas com 65 e mais anos de idade, necessidades de cuidados de enfermagem. Tese de Doutoramento, Universidade de Lisboa (2013). https://repositorio.ul.pt/bitstream/10451/12196/1/ulsd069058_td_tese.pdf
Petronilho, F., Machado, M.: Teorias de Enfermagem e Autocuidado: Contributos para a Construção do Cuidado de Reabilitação. Em: Marques-Vieira, C., Sousa, L. (eds.) Cuidados de Enfermagem de Reabilitação à pessoa ao longo da vida, pp. 3–14. Lusociência, Loures (2017)
Hoeman, S.: Enfermagem de reabilitação: prevenção, intervenção e resultados esperados. Lusodidacta, Loures (2011)
Dirkes, S.M., Kozlowski, C.: Early mobility in the intensive care unit: evidence, barriers, and future directions. Crit. Care Nurs. 39, 33–42 (2019). https://doi.org/10.4037/CCN2019654
Augustine, M.R., et al.: Implementation of post-acute rehabilitation at home: a skilled nursing facility-substitutive model. J. Am. Geriatr. Soc. 1584–1593 (2020). https://doi.org/10.1111/jgs.16474
Pires, R., Martins, M.M., Gomes, B., Monteiro, C., Ribeiro, O.: Intervenção do Enfermeiro Especialista em Reabilitação na Mobilidade da Pessoa Idosa Institucionalizada – Programa TEIA. Rev. Port. Enferm. Reabil. 2, 90–101 (2019). https://doi.org/10.33194/RPER.2019.V2.N1.11.4557
Ordem dos Enfermeiros: Guia Orientador de Boas Práticas: Cuidados à pessoa com alterações da mobilidade – posicionamentos, transferências e treino de deambulação. Ordem dos Enfermeiros (2013). https://www.ordemenfermeiros.pt/arquivo/publicacoes/Documents/GOBP_Mobilidade_VF_site.pdf
Cerol, P., Martins, J., Sousa, L., Oliveira, I., Silveira, T.: Mobilização Precoce Em Pessoas Submetidas a Ventilação Mecânica Invasiva: Revisão Integrativa Da Literatura. Rev. Port. Enferm. Reabil. 2, 49–58 (2019). https://doi.org/10.33194/RPER.2019.V2.N1.07.4563
Schober, A.E., Thornton, K.C.: Early mobilization in the intensive care unit. Curr. Anesthesiol. Rep. 32(3), 73–78 (2013). https://doi.org/10.1007/S40140-013-0013-X
Cerqueira, A.V.B., Grilo, E.N.: Prevenção Das Consequências Da Imobilidade Na Pessoa Em Situação Crítica. Rev. Port. Enferm. Reabil. 2, 78–89 (2019). https://doi.org/10.33194/RPER.2019.V2.N1.10.4574
Diário da República: Regulamento n.º 392/2019 de 3 de maio: Regulamento das Competências Específicas do Enfermeiro Especialista em Enfermagem de Reabilitação. Diário da República, 2a série - n.o 85 - 3 maio 2019, 13565–13568 (2019). https://www.ordemenfermeiros.pt/media/11871/1356513568.pdf
Ordem dos Enfermeiros: Assembleia do Colégio da Especialidade de Enfermagem de Reabilitação: Padrões de Qualidade Especializados em Enfermagem de Reabilitação. Ordem dos Enfermeiros (2018). https://www.ordemenfermeiros.pt/media/8141/ponto-4_regulamento-dos-padr%C3%B5es-qualidade-ceer.pdf
Chandler, J., (eds.). Cochrane Handbook for Systematic Reviews of Interventions version 6.2, Cochrane (2021). https://training.cochrane.org/handbook/current/chapter-i
Joanna Briggs Institute: Critical Appraisal Tools - Joanna Briggs Institute. https://jbi.global/critical-appraisal-tools (2021)
The JBI EBP Database: Ovid Database Guide. https://ospguides.ovid.com/OSPguides/jbidb.htm (2021)
Page, M.J., et al.: The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 372 (2021). https://doi.org/10.1136/BMJ.N71
Begicheva, S.: Fuzzy model for evaluating the quality of medical care. In: Proceedings - 21st IEEE Conference Business Informatics, CBI 2019, vol. 2, pp. 5–8 (2019). https://doi.org/10.1109/CBI.2019.10088
Ordem dos Enfermeiros: Bilhetes de identidade dos indicadores que integram o core de indicadores por categoria de enunciados descritivos dos Padrões de Qualidade dos Cuidados de Enfermagem de Reabilitação. Ordem dos Enfermeiros (2018). https://www.ordemenfermeiros.pt/media/5443/enfermagemreabilitacao.pdf
Imhof, L., Suter-Riederer, S., Kesselring, J.: Effects of mobility-enhancing nursing intervention in patients with ms and stroke: randomised controlled trial. Int. Sch. Res. Not. 2015, 1–6 (2015). https://doi.org/10.1155/2015/785497
Crotty, M., et al.: Should we provide outreach rehabilitation to very old people living in nursing care facilities after a hip fracture? A randomised controlled trial. Age Ageing 48, 373–380 (2019). https://doi.org/10.1093/AGEING/AFZ005
Young, D.L., et al.: identifying barriers to nurse-facilitated patient mobility in the intensive care unit. Am. J. Crit. Care. 27, 186–193 (2018). https://doi.org/10.4037/ajcc2018368
Lowthian, J.A., et al.: Predicting functional decline in older emergency patients—the Safe Elderly Emergency Discharge (SEED) project. Age Ageing 46, 219–225 (2017). https://doi.org/10.1093/AGEING/AFW210
Liang, L., Pan, Y., Wu, D., Pang, Y., Xie, Y., Fang, H.: Effects of multidisciplinary team-based nurse-led transitional care on clinical outcomes and quality of life in patients with ankylosing spondylitis. Asian Nurs. Res. (Korean. Soc. Nurs. Sci). 13, 107–114 (2019). https://doi.org/10.1016/J.ANR.2019.02.004
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this paper

Cite this paper
Lopes, M.J., Silva, C., Nunes, I., Pimenta, E., Seromenho, V. (2022). Sensitive Indicators for Rehabilitation Nursing Care in Older Persons with Mobility Impairment Through a Rehabilitation Program: A Systematic Literature Review. In: García-Alonso, J., Fonseca, C. (eds) Gerontechnology IV. IWoG 2021. Lecture Notes in Bioengineering. Springer, Cham. https://doi.org/10.1007/978-3-030-97524-1_15
Download citation
DOI: https://doi.org/10.1007/978-3-030-97524-1_15
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-97523-4
Online ISBN: 978-3-030-97524-1
eBook Packages: EngineeringEngineering (R0)