
Abstract
The paper presents a series of aspects regarding the design and FEA analysis of an intramedullary nail used for tibial fractures. The theoretical section consists of the analysis of bone fractures and orthopedical implants. The practical section contains the CAD model and Finite Element Analysis (FEA) of the intramedullary nail most commonly used during the tibial prosthesis intervention. The last part of the work is dedicated to the results and conclusions in order to determine if the movement of the nail inserted in the intramedullary canal is due to its design or due to design of the external guidance system.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others

Keywords
1 Introduction
People have been trying to replace or support bones and joints for thousands of years. At first, they addressed the consequences of trauma and fractures. Later they became concerned about abnormalities in bone structure. For this reason, some of the oldest implants were not designed to accurately reproduce bone anatomy, but to support or reshape it. Orthopedics uses a variety of implants in the treatment of injuries, diseases, and musculoskeletal deformities. The orthopedic implant can be grouped into the following categories: fracture fixation, joint restoration or replacement, soft tissue replacement, and spinal implants.
It is important that orthopedic implants be designed so that they have mechanical and chemical properties appropriate to the anticipated clinical requirements. This requires understanding the properties of the materials and biomechanics. It also requires mechanical testing of implants to ensure that they meet performance specifications.
2 Tibial Fractures and Instruments
2.1 Tibial Fractures
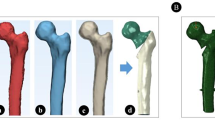
The diaphysis of the long bones corresponds to the middle portion, located between the two epiphyseal extremities (Fig. 1). A cross section of the diaphyseal axis allows us to observe that the diameter of the diaphysis is not constant, the medullary canal progressively widening toward the extremities. The diaphyseal medullary canal does not contain hematopoietic bone marrow (located at the level of the epiphyses), but fatty bone marrow and vessels of medullary origin.

Distal tibial fractures [1].
The cortical bone follows a different evolution during the life of the individual. Thus, aging leads to a progressive physiological resorption of the cortex. This decrease in cortical thickness also occurs in pathological cases, such as during prolonged immobilizations that lead to the appearance of immobilizing osteoporosis, much more pronounced in the case of spongy bone than in cortical bone.
The vascularization of the diaphyseal bone has a double origin, namely endosteal vascularization and periosteal vascularization [2].
Fractures can be found in practice in a wide variety of types but, for practical reasons, they can be divided into two well-defined groups, namely complete fractures and incomplete fractures. In complete fractures, there is a complete disruption of bone continuity and the bone is completely fractured into two or more fragments. Displacement in a complete fracture occurs, partly due to the force of the trauma, partly due to gravity, and partly due to the muscles that are inserted on the fractured bone fragments (Fig. 2).

Different types of fracture [3].
Incomplete fractures are fractures in which the anatomical continuity of the skeletal part is preserved. The bone is incompletely fractured and the periosteum retains its continuity. In adults, this type of fracture occurs through cracking or compression, when the spongy bone is compacted [3].
Thus, simple diaphyseal fractures of the tibia include spiroid fractures, oblique fractures that are composed of two types of fractures (oblique fractures below 30° and oblique fractures with an angle of more than 30°) and transverse fractures. Complex fractures are fractures where a third bone fragment appears and they can be bifocal, oblique or transverse.
2.2 Intramedullary Locked Nails
The principle of the intramedullary nail is to use the cavitary medullary canal to insert it and ensure the rigidity of the fractured bone until it is strengthened. Cominutive fractures and fractures located at the extremities of the diaphysis do not allow to obtain a satisfactory mechanical restraint.
The locked intramedullary shaft is perforated at both ends and 4–6 screws are inserted transversely into the bone and into the holes in the shaft. This locking method can also be applied to unstable fractures, complex metaphysics. Dynamization involves removing the lower or upper screws, which block (depending on the location of the fracture), which allows the compression of the fracture focus and promotes the corticalization of the callus.
The insertion of the intramedullary stem destroys the bone marrow and therefore part of the cortical vascularization. After a few days, a cortical neovascularization occurs, which covers this initial loss. The absence of a direct approach to the fracture site plays an important role because it avoids deperiostation and therefore devitalization of the fragments, as well as the risk of infection [4].
At present, two concepts of treatment of diaphyseal fractures of long bones are confronted: the concept of rigid fixation, with open focus and the concept of elastic fixation, of the intramedullary beginning, in which the fracture area is respected by approach with closed focus; the introduction of a nail into the neutral axis of the diaphysis, mechanically as effective as possible, authorizes a certain elasticity, and is, indisputably, a benefit in relation to open focus osteosynthesis [4] (Fig. 3).

Static intramedullary locked nail [4].
2.3 The External Guidance System
To perform the intramedullary blockage with the nail by surgical method we need the surgery kit composed of the nail guide and anxillary instruments as well as a kit for opening and entering the intramedullary canal of the tibia. The nail will be chosen according to the anatomical structure of the tibia of each patient (Fig. 4).

The nail fixed in the external guidance system.
3 Designing and FEA Analyzing an Intramedullary Nail
3.1 The Computer-Aided Design Model of the Intramedullary Nail
In this paper, the CAD (Computer-Aided Design) model of the nail was made using the CATIA v5R21 program. Since its fifth version, CATIA introduces the notion of virtual prototype. This term is used to describe the whole data that allows handling CAD objects as in real life (Fig. 5).

The Kuntscher nail after which the CAD model was made [5].
The modeling of the geometric domain was made starting from the dimensions of the nail existing in the catalogs offered by the manufacturer. The next step was to describe the plane profiles that formed the basis for generating 3D elements in “Sketcher” mode. Another step was to describe the 3D elements, using the “Pad” mode. The description of the assemblies and subassemblies was made using the “Assembly Design” mode by using specific options.
3.2 FEA Analysis
The Finite Element Analysis (FEA) provides solutions to problems in identifying the fields of variation in stresses and displacements, mainly. Discretization is the fundamental approach required by the finite element method and consists in moving from the continuous structure (with an infinity of points) to a discrete model with a finite number of points [6, 7].
To generate the finite element model, the CATIA Analysis & Simulation package is launched, from which the Generative Structural Analysis mode is selected and then the Static Analysis option from the New Analysis Case window, which involves static structure analysis under imposed constraints and time-independent loads.
The generation of the structure with finite elements was done in 2 stages: discretization and introduction of finite element properties. Discretization was performed by selecting the three-dimensional domain using the Octree Tetrahedron Mesh option. Constraint modeling was done by:
-
modeling the connections with the base using the Clamp option;
-
modeling the connections with the elements adjacent to Rigid Connection.
After discretizing and modeling the constraints, was established the load to which the assembly is subjected.
Depending on the weight of the subject, the force acting on the bone has different values. For the present situation, a subject weighing 60 kg was chosen, so the force was loaded vertically, on the tibial plateau, about 250 MPa, evenly distributed.
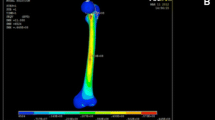
The figures (Figs. 6, 7) represents the Von Mises stress resulting in case if the assembly is subjected to the load.

The 250 MPa tension applied on the nail.

Tensions arising in the designed assembly.
During the surgery of distal fractures of the tibia, on the intramedullary nail is applied a load similar to the one used in the FEM analysis.
Commonly intramedullary nails used for tibial fractures have important disadvantages, such as complicated orientation, handling, and positioning in the bone, and at the same time difficulty in positioning the distal screws using the classical nail guide. Also, all these aspects can lead to errors or additional holes in the tibia, causing a decrease in bone strength and at the same time increasing the duration of surgery with unpredictable effects on bone recovery.
4 Results and Conclusions
Following the aspects related to the fixation system of the diaphyseal fractures of the tibia and the problems encountered during the operations, it was wanted to make a study to determine the stresses of the nail in the distal area, to see if the main problem is in the design of the nail or in the design of the guidance system used to insert the nail.
Several factors are important to determine the stability of the nail, including the size of it, the stresses applied, and where the number of locking screws are positioned.
Due to the fact that during the insertion of the nails, they often bend under the influence of the displacement of the fractured bone fragments and the muscular traction, the position of the distal guide holes of the screws in the guide level no longer corresponds to the position of the distal holes, following this virtual simulation, it can be seen that the most requested area is the one where the distal screws are located, more precisely near the proximal hole of the distal block.
In this case, the surgeon is being forced to fix the distal screws without guide, through numerous successive attempts to trigger the distal holes under the radiological-TV screen, which leads to a significant additional irradiation of the medical staff and the patient (sometimes more greater than the irradiation required to fix the nail).
In conclusion, this paper was based on the study of the importance of implants such as intramedullary nails in the healing of bone skeletal injuries, but especially the importance of good implant functionality, subjected to the demands of the biological environment, the importance generated by the appropriate modeling of the mechanical elements through the FEM analysis.
It can be stated that, in order to obtain a short healing time of the affected bone structure, as well as to avoid a failure of the implant, it is important to observe some major conditions:
-
choosing the nail following a detailed study on the fractured bone, reported to the patient;
-
choosing the right material of the nail so it can face external forces;
-
improving the guidance system so it can show more precisely the distal holes position;
References
Cristoiu, F.C.: Diaphyseal fractures of the leg. University of Medicine and Pharmacy Dr, Carol Davila-Bucharest (2014)
Tomoaia, G.: Osteoarticular traumatology. In: Anatomical and physiological bases of the bone system, Cluj (2004)
Botez, P.: Orthopedics, caduceus collection. Publishing House. ISBN: 978-973-756-075-9, Iași (2008)
Nicolescu, M., Ravcica, G., Ojoga, F.: Orthopedic-surgical treatment, and physiotherapy in musculoskeletal disorders, part I, Alma Mater Bacau Publishing House (2008)
www.zimmerbiomet.com. Accesed 21 June 2021
Lates, M.T.: Metoda elementelor finite, Ed. Universității Transilvania din Brasov (2008)
Cotoros, D.: Analysis of Skeletal prosthesis component elements at structural level. Metal. Int. 15(7):116–120 (2010)
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this paper

Cite this paper
Ionita, I., Druga, C., Rosca, I., Șerban, I. (2022). Designing and FEA Analyzing an Intramedullary Nail for Tibial Fractures. In: Herisanu, N., Marinca, V. (eds) Acoustics and Vibration of Mechanical Structures – AVMS-2021. Springer Proceedings in Physics, vol 274. Springer, Cham. https://doi.org/10.1007/978-3-030-96787-1_22
Download citation
DOI: https://doi.org/10.1007/978-3-030-96787-1_22
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-96786-4
Online ISBN: 978-3-030-96787-1
eBook Packages: Physics and AstronomyPhysics and Astronomy (R0)