
Abstract
The chapter describes the reactions in leprosy, clinical and pathophysiological. It also includes its treatment. Attention is paid to nerve damage and follow-up, especially clinical. Type 1 leprosy reaction, old name reversal reaction and type 2 leprosy reaction old name erythema nodosum leprosum are discussed and compared.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Nerve damage leading to impairments and permanent disability is still the major problem in the course of a leprosy infection. Were it not for this damage, leprosy would be a rather innocuous skin disease, whereas even today it is one of the most feared diseases, often associated with severe social repercussions for the sufferer.
Despite the claim of the World Health Organization (WHO) that it would not be a public health problem anymore after the year 2000 (later extended to 2005), leprosy still remains one of the main causes of peripheral nerve damage.
The main reason is that there is a lack of awareness and knowledge, frequently leading to a major delay in diagnosis. Among others, the WHO elimination policy is therefore to blame.
Nerve damage may occur before antimycobacterial treatment, during this treatment, and even in patients who are released from treatment, labelled cured by the leprosy programme. It can be stated that there is no leprosy without nerve damage. This damage usually occurs during episodes of disturbances in the immune status of the patient, the so-called reactions. Reactions belong to the normal course of a leprosy infection. Leprosy treatment can prevent or precipitate them.
There are three types of reactions: type 1 leprosy reaction (T1R), also called reversal reaction (RR); type 2 leprosy reaction (T2R), also called erythema nodosum leprosum (ENL); and Lucio’s phenomenon, a reaction occurring specifically in multibacillary patients from Mexico. The latter does not cause nerve damage and is discussed in another chapter.
Type 1 leprosy reaction (T1R) occurs in borderline leprosy (BT, BB and BL). In these forms of leprosy, nerve damage occurs early in the course of the disease; it is usually rather gradual, taking weeks or even months to become irreversible, but, occasionally, severe nerve damage may occur overnight.
Type 2 leprosy reaction (T2R) occurs in lepromatous leprosy (BL, LLs and LLp). In these forms of leprosy, nerve damage occurs late in the course of the disease; it may take years to develop the damage; however, it may increase suddenly during an episode of T2R. Both reactions, T1R and T2R, can occur in BL leprosy, even at the same time.
Reactions must be diagnosed early and treated appropriately if permanent disability is to be avoided. Ideally, the reactions should not occur at all, being prevented by treatment. To achieve this, it is of utmost importance to understand the mechanisms behind the reactional states and the principles of management.
Much knowledge on immunology and pathology has been accumulated over the past 50 years; methods of detection have been introduced as well as adequate treatment for most of the patients. This chapter covers these aspects. It must be emphasized that the experienced clinician is still the centre of diagnosis and treatment of a reaction. A major problem is that this experience has disappeared due to the decentralization of the leprosy services and the dismantling of the vertical leprosy programmes.
2 Type 1 Leprosy Reaction
Many names have been attached to this type of reaction, which has led to fierce arguments among leprologists who did not understand each other’s definition and terminology and hardly listened to each other’s arguments. As a result, for quite some time, there was an Anglo–Saxon–French leprology, a Spanish–Portuguese–South American one and an Indian one. Some of the terms used are reversal reaction, borderline leprosy reaction, tuberculoid reaction, tuberculoid in reaction, active tuberculoid leprosy, downgrading borderline leprosy, upgrading versus downgrading reaction and Jopling type 1 reaction. Some of these terms overlap with one another partially, and others completely while being conceptually different. However, recently, leprologists have started to speak the same language and call it type 1 leprosy reaction (T1R).
2.1 Signs and Symptoms of T1R
T1R usually only involved the nerves and the skin, but it must be emphasized that liver and joints may be affected occasionally. Skin involvement frequently accompanies nerve involvement, but may also precede or follow nerve damage.
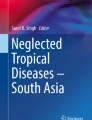
Clinically, a reaction may be suspected when in borderline patients there is increased inflammation of pre-existing skin lesions. Hypopigmented or only slightly erythematous macules become red and swollen, form plaques (Figs. 21.1, 21.2, 21.3, 21.4) and occasionally undergo ulceration. Crops of new lesions may suddenly appear in previously clinically uninvolved skin. Sometimes, extensive oedema of the extremities or face may be present, i.e. acroedema, in particular in BL patients (Fig. 21.5). Patients may complain of a burning, stinging sensation in the skin lesions and complain of aches and pains in the extremities or in the face and of loss of strength and/or sensory perception.

BT leprosy in T1R. Erythematous, oedematous plaques on the face. (© Enrico Nunzi 2021)

BT leprosy in T1R. Erythematous, oedematous plaques on the face. (© Salvatore Noto 2021)

BT leprosy in T1R. Large erythematous lesion on the face; on the right cheek, oedema is evident. (© Enrico Nunzi 2021)

BB leprosy in T1R. Erythematous and oedematous lesions all over the trunk and the upper limbs. The punched-out lesions and the immune areas are evident. (© Enrico Nunzi 2021)

Acro-oedema in T1R. (© Bernard Naafs 2021)
The peripheral nerve trunks at specific sites may become swollen and tender on palpation (Chap. 14). The Tinel sign may become positive, i.e. lightly tapping over the nerve elicits a sensation of tingling or “pins and needles” in the distribution of the nerve.
Loss of strength may involve the muscles serving eyelids, face, hands and feet. Patients may suddenly start to drop things from their hands or stumble when walking.
To diagnose a reaction early, one may ask the patient to close his eyes lightly, and to notice any, even minimal, movement of an eyelid or a slight gap in the closure (Chap. 14), which may herald further damage. It must be noted that, when a patient is asked to close his or her eyes firmly, such minimal damage will pass unnoticed. Loss of vision is one of the major disabilities and should be prevented.
Another early sign to note is whether hands and feet are sweating or have new dry areas. The appearance or an increase in size of dry areas is often a first sign of an incipient reaction. If sensory loss is severe, patients may injure their hands and feet and also may start to develop blisters without knowing the cause.
However, patients with T1R, contrary to patients with T2R, are not ill. Some have remarkably few complaints and symptoms; therefore, detection may be delayed or even missed.
Early diagnosis and treatment of these complications need objective clinical parameters. These consist of mapping (drawing) the lesions, which is tedious but certainly worthwhile, and of careful assessment of nerve functions by voluntary muscle testing (VMT) and graded sensory bristle test (GST) [1, 2]
2.2 Laboratory in Type 1 Leprosy Reaction (T1R)
Laboratory tests have little to contribute, such as follow-up of cytokines, tumour necrosis factor-alpha (TNF-α), interleukin, (IL)-1 or IL-2, measurement of the acute-phase response, the ratio of serum amyloid A-/C-reactive proteins and activation products such as neopterin, nor the presence of antibodies against specific Mycobacterium leprae (M. leprae) antigens (phenolic glycolipid 1 or LID 1) [3]. This also, but less, applies for more elaborate testing of cell-mediated immunity (CMI); functional tests such as lymphocyte transformation tests, migration inhibition tests and INF-ƴ and IL-2 release essays.
A new development is that a transcriptomic signature of risk for T1R consisting of five messenger RNA genes (CCL2, CD8A, IL2, IL15 and MARCO) is identified based on cross-sectional comparison of their RNA expression. In addition, intra-individual longitudinal analyses of leprosy patients before, during and after treatment of T1R indicated that several IFN-induced genes increased significantly at onset of reaction, whereas IL15 genes decreased. Importantly, the prospective five-gene signature for T1R could predict a T1R at least 2 weeks before onset [4]. Thus, the transcriptomic biomarkers provide promise for in the future early detection of these acute inflammatory episodes and thereby help to prevent permanent neuropathy and disability in leprosy patients. But for the time being, it is still the experienced clinician who by careful observation and simple clinical tests has to detect the reaction. Pathology and immunopathology are of only limited help to confirm the diagnosis [5]. However, the above-mentioned investigations are very useful for research purposes.
2.3 Immunology and Pathology of Type 1 Leprosy Reaction (T1R)
Histopathologically , the lesions show all the characteristics of a delayed-type hypersensitivity reaction (Chap. 12). In the initial lesion, only mild extracellular oedema with some proliferation of fibroblasts may be seen, with an increased number of lymphocytes in the leprosy granuloma. Later, there is further increase in the oedema and a change in the cellular composition in and around the epithelioid cell granuloma, due to an influx of lymphocytes that are mainly of CD4 subtype, especially the Th1 class [6,7,8,9].
Using methods for detection of messenger RNA (mRNA), it was shown that, besides interferon-gamma (IFN-ƴ ), production of IL-2 and TNF-α was increased, which confirms a shift to the Th1 subtype during a reaction [5,6,7,8,9,10]. Possibly due to this shift, humoral immunity during a T1R seems to be diminished [5]. However, there also may occur a shift to Th2 activity in the course of a reaction, since there is an increase in mRNA for IL-4 in some of the lesions [7, 8]. During a reaction and when it subsides, the relative number of CD8+ cells (suppressor/cytotoxic) increases.
The importance of cells with the CD4 marker is emphasized by the observation that leprosy and especially T1R may occur when human immunodeficiency virus (HIV)-infected patients are treated with effective antiretroviral therapy, the CD4+ cells increase and T1R pathology occurs as an immune reconstitution inflammatory syndrome (IRIS) [11].
It is still not known which antigens or antigenic determinants are responsible for T1R [5]. Neither is the orchestration of the cytokines and chemokines known. Moreover, the events may compartmentalize. What happens in the tissues may be different from what is found in the blood.
It has been shown that, during T1R, peripheral blood lymphocytes show increased immune response towards M. leprae antigens. This was demonstrated in vitro using leukocyte migration inhibition tests and lymphocyte transformation tests. When the reaction subsides, the immune response decreases. In vivo, such reactions may be seen after pregnancy [12], starvation and immunosuppressive therapy and as mentioned before after starting treatment for an HIV infection. However, which of the M. leprae antigens, let alone which antigenic determinants are involved, is still unknown. Heterogeneity has been shown, not only between different patients but also over time in one patient, when the maximum CMI response may change from one antigen to another. Since M. leprae is very difficult to find in paucibacillary leprosy patients, especially in those with T1R, autoimmune phenomena have been incriminated by some to play a role in the reactional process.
It has been shown that human nerve and skin have a number of antigenic determinants in common with M. leprae [13]. Many of those epitopes are on heat-shock proteins (HSPs) [14]. This can be demonstrated in particular in macrophages and epithelioid cells of granulomatous diseases such as sarcoidosis, necrobiosis lipoidica, and granuloma annulare [15]. In animal models, it has been shown by electron microscopy that M. leprae-primed macrophages attack Schwann cells [16], not only in the presence but also in the absence of detectable M. leprae. It was also observed in vitro that T cells that reacted with M. leprae also reacted with components of Schwann cells [17]. In serology, it was already demonstrated a long time ago that most leprosy patients have antibodies against nerve components.
That the innate immunity is involved in a T1R can be seen because there is a marked signature in the blood, comprising genes mostly related to the innate immune responses, including type 1 IFN components, autophagy, parkins and Toll like receptors [18]. Leprosy reactions in general show increased Th17 cell activity and a reduced FOXP3+ Tregs with concomitant decrease in TGF-β and increase in IL-6 [19].
2.4 Up- and Downgrading Reactions
In the presulphone era, it was observed that, after an exacerbation—reactions are exacerbations—of the disease, patients became more or less bacilliferous or even “cured”. As a result, they most likely suffered nerve damage. It was considered that, had they become more tuberculoid, the event had been upgrading, while had they become more lepromatous, downgrading had occurred [20]. The original publications mention regression, less bacilli and lepromatous transformation and more bacilli.
When sulphones became available, many noticed the occurrence of exacerbations or pseudo-exacerbations of the disease after introduction of treatment, after which the patients may have been more damaged but the bacillary load seemed to have diminished. The term “reversal reaction” was coined for these phenomena. One tried to prevent it to happen by introducing treatment with low-dose sulphones and thereafter slowly increasing the dose, but in fact paved the way for sulphone resistance.
Many discarded the concept of a downgrading reaction, since during effective antibacterial treatment, no bacterial multiplication was expected, and used only the term reversal reaction. The concept, however, was never abandoned entirely, since reactions still occurred in untreated patients and some pathologists had the strong impression that, when a reaction occurred, they observed, even in treated patients, the appearance of, or temporary increase in, the number of M. leprae, some of which were solid staining [20]. This concept became even more relevant with the introduction of WHO-advised multiple drug treatment (MDT). Reactions now did occur not only before and during treatment but also after antimycobacterial treatment. The latter often was very difficult to distinguish from relapse [20]. Moreover, an increase in the number of solid-staining bacteria could occasionally be observed, which only disappeared after the reaction settled. This was explained by assuming that this late reaction had been effective in clearing the bacillary load, thus being an upgrading reaction. After the decline of the number of bacilli with effective antimycobacterial treatment, enough of the cell-mediated immune resistance was restored to deal with the bacteria multiplying anew [20]. Interestingly, the same authors who noticed an increase in bacterial load during a reaction occurring when on dapsone monotherapy and during late T1R hardly observed this phenomenon during multidrug treatment.
Initially, to explain the disappearance of bacilli during one type of reaction and not during the other, the concept of protective immunity and nonprotective delayed type of hypersensitivity was introduced [21]. When the reaction was directed against certain antigens, the bacteria were killed. When it was directed against others, only the tissue was damaged due to a bystander effect, but not the bacteria. However, this concept was increasingly challenged.
Another explanation that was proposed is that, during an upgrading reaction, immunity is directed against antigenic determinants that are essential for the bacterium to survive, and that during a downgrading reaction, the reaction is directed against antigenic determinants of secreted antigens and remnants of dead and dying bacteria, or even against antigenic determinants of the host that the host has in common with M. leprae [13].
A third concept, that in both upgrading and downgrading reactions the same antigenic components may be involved, is the most likely. There is competition between enhanced cell-mediated immunity, stimulated by certain antigenic determinants of the bacteria or determinants of the human host, and a suppressive effect induced by others.
It is not unlikely that the orchestration of the cytokines that result from the immunological events is responsible for the final effect of up- or downgrading. An observation supporting this concept is the finding that different antigenic determinants induce a different cytokine profile in different individuals depending on their genetic make-up and immunological history, including their contact with environmental microorganisms. It should also be realized that events may differ from site to site in the tissues and that peripheral blood does not necessarily need to mirror this [22].
2.5 Treatment of Type 1 Leprosy Reaction
Editor note: The treatment of reactions is dealt with herewith and in Chap. 28 “Medical Therapy”. The chapters represent two approaches, both largely used, to the management of these complications.
Treatment should be based on the understanding of the immunopathology, namely, a harmful delayed-type hypersensitivity reaction against M. leprae antigens. A logical approach, therefore, would be to reduce the amount of stimulating antigens with chemotherapy while suppressing the cell-mediated immune response.
It is important to realize that dapsone, which is a major constituent of chemotherapy when given at dose of 50 mg or higher, on its own has suppressive effect on the occurrence and development of T1R. In some countries, the prevalence of T1R during treatment has reduced after the introduction of the WHO-advised multiple drug treatment (MDT), during which 100 mg dapsone is given daily.
For immunosuppression, prednisolone is the drug of choice, though azathioprine, cyclosporin, methotrexate (MTX) and some biologicals also have been shown to be effective. Prednisolone, however, has a triple action. It reduces the oedema immediately, is immunosuppressive and decreases post-inflammatory scar formation.
The duration of the immunosuppression should be long enough to cover the period that the antigen load is able to trigger the CMI response [23, 24]. For tuberculoid (TT, BT) patients, this may be 2–6 months, for mid-borderline (BB) patients 4–9 months and for some borderline lepromatous (BL) patients even up to 2 years.
The initial dose (particular at the lepromatous range (BL, LLs)) usually does not need to exceed 40 mg daily. A higher initial dose has, only at the beginning of the treatment, some positive effect on the oedema, but does not improve the outcome in the long run. The crucial starting dose seems to be between 25 and 40 mg, depending on the classification, higher in tuberculoid than lepromatous. After 1–3 months, 15–20 mg suffice, but this should not be tapered too quickly. When 10 mg is reached, the treatment can be discontinued within 1 month. Sensory testing and voluntary muscle testing can guide tapering. Graded sensory test has been shown to be the most sensitive.
Some programmes, wrongly, give only 2 months prednisolone at doses above 15–20 mg and taper within 1 month. Immediately after these 3 months, their results are excellent; however, 3 months later, most of the patients have nerve damage as before [23, 25].
It is important to check patients who will be treated with prednisolone for intercurrent infections, since infections may exacerbate during immunosuppressive therapy (especially worm infections should be taken care of). However, since the duration of therapy is relatively short, serious adverse effects of prednisolone are not frequently observed [26, 27].
When, during an otherwise effective anti-reaction treatment, one or two nerves are not responding, but other nerves do, it may be assumed that “venostatic oedema” is involved (explanation further on). A nerve decompression operation should be considered [28]. This should be done as soon as possible, but within 2–3 months at the latest. The operation should be performed under steroid cover as this prevents postoperative oedema and decreases postoperative scarring. It should be remarked that, though nearly all leprosy surgeons are convinced of the positive effect of nerve release in selected patients, some, usually not involved with surgery, consider the evidence to be insufficient.
3 Type 2 Leprosy Reaction (T2R)
The nomenclature of T2R, erythema nodosum leprosum (ENL), lepra reaction, lepromatous leprosy reaction or Jopling type 2 reaction is as confusing as its variations in clinical presentation.
3.1 Signs and Symptoms of T2R
The name erythema nodosum leprosum describes the most common manifestation of this reaction—an eruption of tender, red papules and nodules—which develops in a few hours to days and lasts a few days to weeks. The patient feels unwell, has pyrexia, may have granulocytosis and often has albumin in the urine.
The papules and nodules are red to purple in light-skinned patients (Fig. 21.6) and skin-coloured (Fig. 21.7) or dark blue–red nearly black in dark-skinned patients. When they resolve, they leave a greyish-blue lesion resembling a bruise in light-skinned patients (Fig. 21.6) and a deep blue–brown or black discoloration in dark-skinned patients. The resolving lesions usually desquamate. Active and fading lesions may be present at the same time. Occasionally, the lesions coalesce and become plaques. Both plaques and nodules may ulcerate (Orbaneja’s necrotic nodules). Most frequently, the lesions occur along the extensor side of the arms and thighs, on the trunk and on the face, but may also occur elsewhere. They differ in their distribution from the erythema nodosum lesions that occur during sarcoidosis or tuberculosis, chlamydia, yersinia or streptococcal infection, which have a predilection for the shins. Sometimes, the lesions can be more easily palpated than seen. They feel firm, and palpation is frequently painful to the patient. They often extend downwards to the deeper layers of the dermis and into the subcutaneous fat.

BL leprosy in T2R. On the upper part of the thigh, erythema multiforme-like lesions. On the knee, erythematous nodules. The darker macules are old ENL lesions. (© Salvatore Noto 2021)

T2R nodules on the dorsum of the wrist. (© Bernard Naafs 2021)
Also other clinical manifestations of T2R have been reported: the so-called erythema multiforme type often seen in Brazil, but with the increasing awareness reported from other parts of the world too (Fig. 21.8). Some patients display superficial bullous ulcerative cutaneous lesions (Fig. 21.9) associated with high fever, malaise and oedema. Histopathology of this bullous form demonstrates dermal oedema with mononuclear cell infiltrates and the presence of M. leprae within the capillary endothelium and neutrophilic infiltration in the dermis.

BL leprosy in T2R. Erythema multiforme-like lesions on the upper limb. One lesion shows central necrosis. (Courtesy of E. Nunzi, 2020, All rights reserved)

Bullous T2R. (© Bernard Naafs 2021)
In T2R the skin is not the only organ involved. Painful enlargement of lymph nodes, the liver and the spleen may occur, as well as episcleritis and iridocyclitis with glaucoma. Involvement of lymph nodes may lead to oedema of the extremities, particularly the legs. This oedema should not be confused with that which occurs as a result of a nephrotic syndrome that however may be caused by chronic T2R. In men, epididymo-orchitis can be seen. Nerves as well as joints can become swollen and tender. Periostitis, tendovaginitis and myositis are observed. Glomerulonephritis can be present too, which also may lead to oedema. Even peritonitis has been noticed during abdominal operation and confirmed with histopathology.
In short, since lepromatous leprosy is a generalized disease, each organ or tissue may be involved in the T2R process, with the CNS as a possible exception.
T2R usually occurs in episodes, lasting from only a few days to 1 to 2 weeks. Over 95% resolve spontaneously within 1 month [29] (Fig. 21.10). Some patients may experience widespread and recurrent lesions which continue to appear for months or even years, and in a few patients, the condition may become chronic. Blindness and chronic T2R probably are the most serious complications of leprosy. Chronicity and treatment may even lead to death [30].

Severity and duration of T2R. (© Bernard Naafs 2021)
Though T2R occasionally occurs in untreated patients, a great number, sometimes over 50–60%, of the lepromatous patients under or after treatment develop one or more attacks. The frequency of the occurrence and the severity of T2R seem to be related to the progress of the disease before treatment is started. In programmes with early detection, only 10–15% of multibacillary patients may experience a T2R attack, which then is often mild. In most programmes, occurrences of 30–40% may be observed.
3.2 Immunology and Pathology of Type 2 Leprosy Reaction
In the initial T2R lesions, there is, against a background of borderline lepromatous (BL) or lepromatous (LL) histopathology, a slight increase in the number of lymphocytes, especially perivascularly. The majority of these infiltrating cells are CD4+ Th2 cells [31]. When the reaction continues, the number of these cells increases further and exceeds the number of CD8+ cells that normally form the majority in a lepromatous leprosy lesion. This shift can be shown by an increase in mRNA for IL-4, IL-5, IL-13 and perhaps also IL-10 cytokines, which are indicative of a Th2 type of reaction.
It has been observed that, early during T2R, in the lepromatous granuloma in between the foamy cells, smaller cells—probably monocytes turned into active young macrophages—can be detected, and these may be responsible for destruction of inert foamy macrophages and, as a consequence, release of antigens. These can then be presented by fresh macrophages to the immune system and stimulate the CMI. The involvement of the CMI can be witnessed by the observation that the number of IL-2 receptors on the immune-competent cells increases, as does HLA-DR expression, not only within the infiltrate but also on the keratinocytes of the overlying epidermis [31].
It has further been shown that, within ENL lesions, the plasma cells, stimulated by the IL-4-producing cells, produce antibodies against M. leprae antigenic determinants. These antibodies then will combine with the omnipresent antigens and, when not engulfed by a macrophage, form immune complexes [31, 32]. These gives rise to complement activation and full-blown T2R (Fig. 21.11). Antigen, IgG, IgM, complement and IL-4 mRNA have been shown to be present in the tissues. Particular important is the IL-4, because it is known to be a B cell stimulator, increases the HLA-DR expression and is a growth factor for the mast cells.

ENL immunopathology (Adapted from Naafs B. Reactions: New Knowledge. Trop Geogr Med 46 (1994) 80–84)
When the T2R reaction is full blown, polymorphonuclear granulocytes dominate the picture (Chap. 12); a few leu7-positive (natural killer) cells can also be seen, as well as an increased number of mast cells.
Involvement of both immune complexes and cell-mediated immunity has also been shown in peripheral blood. During T2R there is, in vitro, an increase in the response of peripheral blood leukocytes to mitogens, indicating a generalized increase in CMI. Complement factor C3d is found to be increased in peripheral blood, which may indicate complement activation and is probably a spillover from tissues and not a sign of a classic Arthus phenomenon.
IL-4, IL-5 and TNF-α are, together with IFN-ƴ, the most prominent cytokines present; TNF-α is known to be a pyrogen and may be responsible for the increase in body temperature during T2R, and certainly will contribute to further tissue damage. There are some indications that autoimmunity might also play a role in tissue damage during T2R.
It was found using flow cytometry and immunohistochemistry that T2R patients showed significantly higher Toll-like receptor-9 (TLR-9) expression when compared with nonreactional lepromatous patients, both locally in the skin lesions and in circulating mononuclear cells. TLR-9 preferentially binds DNA present in bacteria and viruses, and triggers signalling cascades that lead to a pro-inflammatory cytokine response. The levels of endogenous and pathogen-derived TLR-9 ligands in the circulation of T2R patients were also higher. Furthermore, peripheral blood mononuclear cells (PBMCs) isolated from the T2R patients secreted higher levels of TNF, IL-6 and IL-1β in response to a TLR-9 agonist than those of the nonreactional patients and healthy individuals [33]. According the authors, these data strongly indicate that DNA sensing via TLR-9 constitutes a major innate immunity pathway involved in the pathogenesis and evolution of T2R.
It was further noticed by Vieira et al. [34] that T2R patients showed a decrease in Tregs and increase in IL-17+ cells in biopsy of an active lesion. It must however be realized that in biopsy there is a compartmentalization and a visible ENL (T2R) lesion may already be in the progress to resolving.
3.3 Differential Diagnosis: Type 1 Versus Type 2 Leprosy Reaction
Sometimes, especially in BL and subpolar LL patients, it is difficult to distinguish T1R from T2R. They may even occur together, or one after the other. Some signs and investigations may be of help in differential diagnosis. T2R is a generalized disease in which, besides skin and nerves, other organs such as joints and lymph nodes may be involved. The patient may be ill (during T1R he usually is not), may have a raised temperature and erythrocyte sedimentation rate (ESR) and may even have protein in his urine.
The skin lesions in T2R are mostly tender, whereas in T1R they are not. Lesions in T1R may have sensory loss in comparison with surrounding skin, while in T2R this is usually not the case. Palpating the lesions, a T2R plaque consists of confluent papules and nodules, whereas in T1R the lesions are more homogeneous. Both T2R and T1R lesions may ulcerate, but a smear from a T2R lesion shows predominantly polymorphs , while that from a T1R lesion shows lymphocytes. Two old tests may be of help. The Ryrie test involves stroking the sole of the foot with the back of a reflex hammer, which in T2R elicits a burning pain which also may be noticed when watching the patient walk, as if on hot coals. Another test is the Ellis test, which involves squeezing the wrist; during T2R, this elicits a painful reaction, which does not occur during T1R unless the radiocutaneous nerve is tender. It has been described that neuro-electrophysiology also can be used to distinguish T1R from T2R. T2R may develop a conduction block, whereas T1R shows only temporal dispersion [35].
3.4 Treatment of Type 2 Leprosy Reaction
Since T2R is an episodic self-limiting disease, as was already shown by de Souza Araújo in 1929 [29], many drugs have been wrongly judged to be of therapeutic value [25].
Treatment of this reaction is less straightforward than that of T1R. Like in T1R, the antigenic load should be reduced, preferably with WHO MDT. Clofazimine (Lamprene), a normal constituent of this MDT, has been shown to suppress T2R, and since its introduction, the prevalence of T2R seems to have decreased.
It has been shown that clofazimine inhibits neutrophil mobility in vitro and the lymphocyte response to mitogens. It also appears to decrease C3d levels, suggesting that it interferes with the breakdown of C3.
3.4.1 Mild T2R
Mild T2R or ENL with only a few erythematous papules and no signs of involvement of other organs except the skin is usually not very damaging, although the patient may feel uncomfortable. In these patients, the symptoms can easily be treated with mild analgesic and anti-inflammatory drugs such as aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs). Although an attack will subside spontaneously, these prostaglandin suppressant drugs may help to alleviate the reaction.
3.4.2 Moderate T2R
When the reaction is slightly more severe and accompanied by pyrexia, leucocytosis and some involvement of other organs except nerves, eyes or testes, additional treatment is required. In the 1990s, chlorpromazine has been used by some leprologists. This drug had been shown to inhibit complement-mediated reaction in rabbits, and it actually prevented tissue injuries [36]. Promethazine has also been advocated. This has some inhibiting action on the complement cascade, and since the number of mast cells is increased during T2R, it may interfere with its mediators such as histamine and alleviate the reactional symptoms.
When a reaction involves joints (arthritis) or nerves with no obvious nerve damage, a combination of a NSAID and antimalarials (chloroquine or hydroxychloroquine) is frequently effective. Chloroquine stabilizes lysosomal membranes, preventing tissue destruction, and it modulates complement activation by immune complexes.
3.4.3 Severe T2R
In severe cases of T2R with orchitis, iridocyclitis with glaucoma or neuritis with deterioration of nerve function, corticosteroids or thalidomide should be considered, some give both, particularly when there is acute nerve involvement.
A high initial dose of prednisolone is often required. The action of this drug on T2R is complex and results in suppression of cell-mediated immunity, inhibition of release of lysosomal enzymes and cytokines, decrease of fluid leakage at the site of inflammation, decrease in the response of neutrophils to chemotaxis, inhibition of prostaglandin synthesis and response to prostaglandins.
Prednisolone therapy has been shown to be very effective, although at the high dose which is necessary, side effects are numerous, especially in patients with chronic or recurrent T2R. At present, steroid dependence seems to be a major problem in many leprosy control programmes; this may be induced by the more freely use of steroids.
It should be realized that part of the T2R is complement mediated [32] and that these types of reactions need a high dose of steroids. The usually given 20–30 mg proves not to be enough and even does not prevent new reactions from occurring. Therefore, it is advisable to give a high dosage of steroids (60–120 mg) for a short period, a few days, and then taper off within 1 month, the natural duration of most T2Rs. When the reaction reoccurs during tapering, the initial dose should be restarted and the tapering started again.
At present, thalidomide seems to be the drug of choice [37]. Since it became more easily available, American, European and recently Indian leprologists resorted more often to this drug. It is extremely effective and better than prednisolone [38]. Thalidomide has a number of side effects that usually do not warrant discontinuation of the drug. Teratogenicity is well known and limits its use. Neuropathy may occur more frequently than is reported, because when it occurs, it is usually masked by the leprosy neuropathy.
The mode of action of thalidomide is still unclear. It has been shown to be effective in adjuvant disease in rats. It inhibits de novo synthesis of IgM. Since IgM and especially IgM rheumatoid factor(s) may play a role in perpetuation of T2R, this could be an important finding. It stabilizes lysosomal membranes. It inhibits granulocyte chemotaxis. It inhibits induction of ENL (T2R) lesion via immunomodulation, which results in a significant decrease in the observed CD4/CD8 ratio. It is agonistic to synthesis of IL-2 and it may be agonistic or antagonistic to synthesis of TNF-α.
In most papers, its action is thought to be mediated through TNF-α. But why then does it not work in T1R, where TNF-α seems also to be an important molecule? An anti-TNF-α biological was tried in T2R, and the reaction subsided, but it is not unlikely that this was the normal course of the reaction in these patients.
Thalidomide is given at the dosage of 100–300 mg daily for a period of a few days and then tapered to a dose that prevents new occurrence of T2R.
It has been shown that a combination of low-dose steroids together with thalidomide could be counterproductive, and therefore thalidomide alone should be given for prevention of new reactions, in general at the dosage of 50–100 mg, sometimes lower or higher as judged by the attending physician. However, in several countries, restrictive political legislations limit its use.
Colchicine, which inhibits vascular injury in experimental Arthus reaction by inhibiting chemotaxis of neutrophils, has been shown to have some effect on T2R, but the results are not as impressive as claimed in initial trials.
Cyclosporin A has been shown by some to be effective in severe T2R and may be a substitute for thalidomide, though thalidomide is more effective. However, in our hands, cyclosporin A was of little benefit in preventing T2R, indicating that it may be less effective in suppressing the Th2-type CD4 cells than the Th1-type CD4 cells involved in the reversal reaction (T1R).
A strong anti-T2R effect has been claimed for pentoxifylline at high dosage. Others however were not that impressed. It was tried because some investigators were of the opinion that TNF-α is of major importance in ENL and pentoxifylline is known to suppress its production effectively. However, as mentioned before TNF-α is also present in T1R, in which neither thalidomide nor pentoxifylline is of much help, though pentoxifylline also diminishes leukocyte adherence. Pentoxifylline diminishes only the leg oedema during T2R more effectively than thalidomide, but this was to be expected. In a comparative trial, it was shown to be inferior to thalidomide [39].
3.4.4 Recurrent T2R
Presently, one of the main problems in management of T2R is the large number of patients who become steroid dependent. Often, clofazimine is used to diminish the severity and frequency of the reaction. It is given at the dose of 100–300 mg daily.
Recently, it has been shown that methotrexate is effective to wean patients off steroids provided steroids are only given when there is active T2R. In the period between T2R episodes, steroids should not be given, only the MTX.
It has been reported that immunotherapy with bacillus Calmette–Guérin (BCG) alone and together with M. leprae was able to reduce the frequency and severity of T2R. This was shown too for M. vaccae, M. “W” and the ICRC bacilli. More research should be directed at the mechanisms involved in this phenomenon, and controlled trials to study the clinical effect of mycobacterial immunotherapy should be done, especially since some patients with chronic severe recurrent T2R are not properly controlled with presently available therapies.
4 Nerve Damage
In leprosy nerve damage may occur at three levels:
-
At the level of the cutis (skin) where nerve endings are affected,
-
At the level of the subcutaneous nerves
-
At the level of the nerve trunks
The histopathology of reactional tuberculoid leprosy [40] shows granuloma formation high in the dermis and dermal papillae. The granulomatous infiltrate sometimes seems even to erode the epidermis, but obviously destroys the nerve endings in the papillae. It is not unlikely that the driving forces behind these damaging reactions are antigenic determinants in the epidermis and in the peripheral nerve endings which are similar to those of M. leprae antigens. The reaction could be an autoimmune phenomenon [13].
In borderline leprosy, the nerves of the lower dermis and especially those located around the adnexa are most often involved. Granuloma formation can be seen in and around these nerves together with a proliferation of Schwann cells in and around the perineurium. Damage can be attributed to compression and destruction of nerve fibres by the epithelioid granuloma. During the reactional episode, there is a further influx of immunocompetent cells with oedema formation and expanding granuloma. This contributes further to nerve damage, especially when extracellular oedema accumulates inside the thickened perineurial sheath, converting it into a rigid compressing tube compromising the axons inside [41].
The mechanisms that occur in nerve trunks and larger subcutaneous nerves are more complicated. At the tuberculoid end of the spectrum, these processes are similar to those in the skin, with massive granuloma formation with occasional colliquation and abscess formation. Further into the borderline range, these features are usually less distinct and often even absent. Frequently, only oedema is observed [41].
Damage to cutaneous and subcutaneous nerves causes loss of sensation in the affected areas and loss of autonomic nerve function such as sweating and regulation of vascular tone. However, it is the damage to the peripheral nerve trunk which is the major consequence of T1R. This damage is partly caused by immunological reactions, but mechanical factors are also involved [41] (Fig. 21.12). During T1R, inflammation and consequently oedema occur in the nerve, as it occurs in the skin. The reaction leads to oedema located within the interstitial tissues of the epi-, peri- and endoneurium. Unlike the skin, the nerve cannot expand without limit. The perineurium, which is largely impermeable to fluids, forms a rigid compressing tube around the expanding endoneurium. This results in an increase in pressure within the nerve. As a result, the axons in the endoneurium are compressed by the increased pressure [28] (Fig. 21.12). As a consequence, there is a loss of conducting nerve fibres and thus loss of muscular strength, peripheral sensation and autonomic functions. The intra-axonal flow which brings nutrients from the cell to the peripheral nerve ending is interrupted, and sooner or later, the peripheral nerve fibre dies off and is destroyed [28].

Mechanical nerve damage. (© Bernard Naafs 2021)
When the pressure and the tension along and within the perineurium increase due to an increase in pressure in the endoneurium, there is an increase in the pressure exerted on the blood vessels which transverse obliquely through the perineurium. These blood vessels are then compressed. The venules with relatively low pressure are compressed more than arterioles with higher pressure. The compression of the venules will lead to higher pressure in the capillaries of the endoneurium, which may start “leaking” and thus increase the pressure in the endoneurium. This “venostatic oedema” is able to maintain itself even when the immunological events subside (Fig. 21.13).

Pathogenesis of “venostatic oedema” in peripheral nerves during reaction. (© Bernard Naafs 2021)
In the histopathology of nerve in T2R, an increase in neural cell adhesion molecules (N-CAM) can be observed, and N-CAM-positive CD8+ cells can be isolated from the tissues. In vitro it was shown that, during active T2R, when peripheral blood mononuclear cells (PBMC) were exposed to M. leprae, there was an increase in cytolysis of N-CAM-expressing Schwann cells by CD8+ N-CAM-positive cells. It is interesting to note that IL-15 is capable of inducing N-CAM expression and that IL-15 mRNA is increased in leprosy tissues [42].
In T2R, the mechanisms leading to tissue destruction, i.e. activation of granulocytes, also contribute to damage of nerves fibres and endings. It also has been shown that TNF-α, which seems to be a major cytokine involved in T2R, is able to demyelinize nerve fibres. Demyelination seems to be a major factor in nerve damage due to multibacillary leprosy as shown by nerve conduction studies, as described in Chapter 14. The damage in multibacillary leprosy can also be caused by lipoarabinomannan that on its own may lead to demyelination by complement activation and membrane attack complex (MAC) formation when in contact with the Schwann cell [43]. Moreover, in the large nerve trunks, the immunological processes may give rise to venostatic oedema with compression of axons as described for T1R [28, 41].
5 Voluntary Muscle Testing (VMT)
In the mid-1960s, a numerical system for use in leprosy was developed to assess muscle strength, i.e. voluntary muscle testing (VMT) [1]. When this test is regularly and carefully done, it assists in early detection of a reaction. The facial, median, ulnar and peroneal nerves should be assessed. Deterioration in VMT may precede more obvious clinical signs.
In the field, extensive VMT is out of reach. However, limited testing has been shown to be possible. Experience has been gained with VMT of the orbicularis oculi for the facial nerve, of the opponens pollicis brevis for the median, of the abductor digiti minimi for the ulnar and of the muscles of the anterior compartment of the leg for the peroneal nerve (dorsal flexion of the foot and/or the big toe). Since the use of only three grades, as is often done, is too crude, the five-point scale (Chap. 14) should be used even under field conditions, provided proper supervision and training are continuously provided. However, because the test is not sensitive enough, minimal damage may go unnoticed.
6 Graded Sensory Bristle Test (GST)
A more sensitive method, in particular for minimal and mild nerve damage, is the graded sensory bristle test (GST) , which uses standardized nylon monofilaments developed by Weddell in the mid-1930s, nowadays usually called Semmes–Weinstein monofilaments. The test was later validated and used for follow-up of nerve lesions during leprosy reactions [2]. Over the years, it has proved to be a reliable and reproducible test, for which the filaments are now standardized (Fig. 21.14).

The graded sensory bristle test using standardized nylon monofilaments. (© Enrico Nunzi 2021)
The graded bristle test can be done by mapping areas of sensory loss and grading this loss which is usually done by physiotherapists. However, due to its sensitivity and tediousness, it is prone to inaccuracy and can therefore only be used effectively by experienced investigators under quiet conditions.
For the busy clinicians , it is simpler to assess a small, defined area such as the thenar area for the median nerve, the hypothenar area for the ulnar nerve [2] or the plantar forefoot and heel for the posterior tibial nerve. Care must be taken not to assess within a skin patch when present. The same areas can be assessed in the field, provided again that proper supervision and training are continuously provided.
7 Two-Point Discrimination Test
Another sensory test which may be useful, especially for the foot, is the two-point discrimination test (moving or static) that is done by means of a paper clip bent to a calliper. It is less sensitive than the graded bristle test when used for mapping of the hand, but nearly as sensitive as graded bristles when used on defined areas such as the forefoot or heel to assess peripheral nerve function. Importantly, it is not time consuming.
8 Other Tests
The WHO has advised that ballpoint and pinprick testing are too crude, while graded sensory bristle testing (GST) is not.
It should be noted that more sophisticated physiological methods such as electromyography (EMG), sensory and motor nerve conduction velocity testing, evoked response testing and measuring of autonomic reflexes as well as ultrasound of nerves add little to early detection of T1R or T2R in the field, but they do in research centres and may even help to distinguish T1R from T2R [35].
9 Triggering of Leprosy Reactions (Focussed on Covid-19)
Because it is not certain what influence a Covid-19 infection or vaccination will have on the development of reactions in leprosy, it is necessary to extrapolate what we know in this regard.
Leprosy clinical course seems to be dictated by the CMI. The CMI is responsible for the T1R. When there are enough M. leprae antigenic determinants present, a rise in CMI may lead to a reaction.
The total available antigenic determinants of M. leprae for the cells responsible for the CMI against these determinants may increase because of the treatment of leprosy or other infections. Bacteria such as M. tuberculosis, other mycobacteria or nocardia and even streptococci (heat-shock protein 65) have similar antigenic determinants and early infection, or treatment may cause a T1R response. Advanced infections may suppress CMI.
A BCG vaccination increases the CMI and in this way can lead to a T1R. Immune reconstitution at the end of pregnancy, after initiation of treatment for human immunodeficiency virus (HIV) infection and after immunosuppressive treatment can also lead to a T1LR as well as recovery from any disease. This may also happen after a Covid-19 infection, particularly when this has been treated with immunosuppression.
The mechanism of a type 2 leprosy reaction (T2R) is not clear, but it is thought to be an immunocomplex disease in which neutrophils play an important role. Increase in antigen load is a major factor (relapse and resistance).
It is also known that T2R can be triggered by several events, ranging from psychological stress, pregnancy or anaemia to infections like tuberculosis and intestinal worm infestations. Stopping of clofazimine treatment seems also to play a role, like lowering the doses of steroids for T2R (this however could be the same previously suppressed T2R). It is generally accepted that every vaccination can trigger a T2lR.
Interesting is to realize that during Covid disease, there is a cytokine “storm” with influence on the neutrophils. Some think that it resembles T2R.
But till today, there are no well-described case reports with any leprosy reaction we are aware off.
References
Brandsma JW. Basic nerve function assessment in leprosy patients. Lepr Rev. 1981;52:161–71.
Naafs B, Dagne T. Sensory testing: a sensitive method in the follow-up of nerve involvement. Int J Lepr. 1977;45:364–8.
Silva EA, Iyer A, Ura S, Lauris JR, et al. Utility of measuring serum levels of antiPGL-1 antibody, neopterin and C-reactive protein in monitoring leprosy patients during multi-drug treatment and reactions. Tropical Med Int Health. 2007;12:1450–8.
Tió-Coma M, van Hooij A, Bobosha K, et al. Whole blood RNA signatures in leprosy patients identify reversal reactions before clinical onset: a prospective, multicenter study. Sci Rep. 2019;29:17931. https://doi.org/10.1038/s41598-019-54213-y.
Verhagen CE, Faber WR, Klatser PR, et al. Immunohistological analyses of in situ expression of mycobacterial antigens in the skin lesions of leprosy patients across the histopathological spectrum. Am J Pathol. 1999;154:1793–804.
Yamamura M, Wang XH, Ohmen JD, et al. Cytokine patterns of immunologically mediated tissue damage. J Immunol. 1992;149:1470–81.
Modlin RL, Yamamura M, Salgame P, Bloom BR. Lymphokine patterns in leprosy skin lesion. In: Burgdorff WHC, Katz SI, editors. Dermatology: progress and perspectives. New York: Parthenon Publishing Group; 1993. p. 893–6.
Verhagen CE, Wieringa EEA, Buffing AAM, et al. Reversal reaction in Borderline leprosy is associated with a polarized shift to Type-1-like Mycobacterium leprae T cell reactivity in lesional skin: a follow-up study. J Immunol. 1997;159:4474–83.
Narayanan RB, Laal S, Sharma AK, et al. Differences in predominant phenotype and distribution pattern in reactional lesions of tuberculoid and lepromatous leprosy. Clin Exp Immunol. 1984;55:623–8.
Khanolkar-Young S, Rayment N, Brickell PM, et al. Tumour necrosis factor alpha (TNFa) synthesis is associated with skin and peripheral nerve pathology of leprosy reversal reaction. Clin Exp Immunol. 1995;99:196–202.
Trindade MA, Manini MI, Masetti JH, et al. Leprosy and HIV co-infection in five patients. Lepr Rev. 2005;76:162–6.
Duncan ME, Pearson JM. Neuritis in pregnancy and lactation. Int J Lepr Other Mycobact Dis. 1982;50:31–8.
Naafs B, Kolk AHJ, Chin A, Lien RAM, et al. Anti-Mycobacterium leprae monoclonal antibodies cross-reactive with human skin. An alternative explanation for the immune responses in leprosy. J Invest Dermatol. 1990;94:685–8.
Khanolkar-Young S, Young DB, et al. Nerve and skin damage in leprosy is associated with increased intralesional heat shock proteins. Clin Exp Immunol. 1994;96:208–13.
Njoo D, Hu RVP, Tank B, et al. Detection of shared antigenic determinants between Mycobacterium leprae heat shock protein 65 and human heat shock protein 60. Hansen Int. 2003;28:19–43.
Stanley JNA, Doyle D, Colston MJ, Fisher TR. Macrophage mediated immune responses in the Sciatic nerves of M. leprae infected nude mice with possible bystander and autoimmune demyelination—an electron microscopic study. 13th International leprosy congress FP 034. 1988.
Spierings E, de Boer T, Wieles B, et al. Mycobacterium leprae-specific, HLA class II restricted killing of human Schwann cells by CD4/Th1 cells: a novel immuno pathogenic mechanism of nerve damage in leprosy. J Immunol. 2001;166:5883–8.
Rêgo JL, de Lima SN, Machado PRL, et al. Whole blood profiling of leprosy type 1(reversal) reactions highlights prominence of innate immune response genes. BMC Infect Dis. 2018;24(18(1)):422.
Saini C, Siddiqui A, Ramesh V, Nath I. Leprosy reactions show increased Th17 cell activity and reduced FOXP3+ tregs with concomitant decrease in TGF-β and increase in IL-6. PLoS Negl Trop Dis. 2016;10(4):e0004592. https://doi.org/10.1371/journal.pntd.0004592.
Trindade AB, Benard AG, Ura S, et al. Granulomatous reactivation during the course of leprosy infection: reaction or relapse. PLoS Negl Trop Dis. 2010;4:e921.
Mitra DK, Joshi B, Dinda AK, et al. Induction of lepromin reactivity in cured lepromatous leprosy patients: impaired chemokine response dissociates protective immunity from delayed type hypersensitivity. Microbes Infect. 2009;11:1122–30.
Naafs B. Current views on reactions in leprosy. Indian J Lepr. 2000;72:97–122.
Naafs B. Treatment duration of reversal reaction: a reappraisal. Back to the past. Lepr Rev. 2003;74:328–36.
Naafs B, Pearson JMH, Wheate HW. Reversal reaction: prevention of permanent nerve damage. Comparison of short- and long-term steroid treatment. Int J Lepr. 1979;47:7–12.
Naafs B. Treatment of reactions and nerve damage. Int J Lepr. 1996;64:S21–8.
Sugamaram DST. Steroid therapy for paralytic deformities in leprosy. Int J Lepr. 1997;65:337–44.
Walker SL, Lockwood DNJ. Leprosy Type 1 (reversal) reactions and their management. Lepr Rev. 2008;79:372–86.
Naafs B, Van Droogenbroeck JBA. Decompression des névrites réactionnelles dans la lèpre: justification physopathologique et méthodes objectives pour en apprécier les résultats. Méd Trop. 1977;37:763–70.
De Souza Arauyo HC. Thesis Inst Oswaldo Cruz. Rio de Janeiro; 1929.
Walker SL, Lebas E, Doni S, et al. The mortality associated with erythema nodosum leprosum in Ethiopia: a retrospective hospital-based study. PLoS Negl Trop Dis. 2014;8(3):e2690. eCollection 2014 Mar
Naafs B. Leprosy reactions: new knowledge. Trop Geogr Med. 1994;46:80–4.
Ridley MJ, Ridley DS. The immunopathology of erythema nodosum: the role of extravascular complexes. Lepr Rev. 1983;54:95–107.
Dias AA, Silva CO, Santos JP, et al. DNA sensing via TLR-9 constitutes a major innate immunity pathway activated during erythema nodosum leprosum. J Immunol. 2016;197(5):1905–13. https://doi.org/10.4049/jimmunol.1600042. Epub 2016 Jul 29
Vieira AP, Trindade MÂ, Pagliari C, et al. Development of Type 2, but not Type 1, leprosy reactions is associated with a severe reduction of circulating and in situ regulatory T-cells. Am J Trop Med Hyg. 2016;94(4):721–7. Epub 2016 Feb 22
Garbino JA, Naafs B, Ura S, et al. Neurophysiological patterns of ulnar nerve neuropathy in leprosy reactions. Lepr Rev. 2010;81:206–15.
Asghar SS, Dingemans KP, Kammeijer A, et al. Suppression of complement-mediated vascular injury at Arthus reaction sites by complement inhibitors. Complement. 1986;3(1):40–8.
Walker SL, Waters MFR, Lockwood DNJ. The role of thalidomide in the management of ENL. Lepr Rev. 2007;78:197–215.
Kar HK, Gupta L. Comparative efficacy of four treatment regimens in Type 2 leprosy reactions prednisolone alone, thalidomide alone, prednisolone plus thalidomide and prednisolone plus clofazimine. Indian J Lepr. 2016;88(1):29–38.
Sales AM, de Matos HJ, Nery JA, et al. Double-blind trial of the efficacy of pentoxifylline vs thalidomide for the treatment of type II reaction in leprosy. Braz J Med Biol Res. 2007;40(2):243–8.
Noto S, Clapasson A, Nunzi E. Classification of leprosy: the mystery of reactional tuberculoid. G Ital Dermatol Venerol. 2007;142:294–5.
Naafs B. Nerve damage and repair. Hyderabad, India (AIFO): International Leprosy Congress; 2008. http://www.aifo.it/english/resources/online/books/leprosy/ila-india08/nerve-damageBen_Naafs.pdf
Spierings E, de Boer TJ, Dekker T, et al. Tcell subsets expressing neural cell adhesion molecule: association with antigen independent MHC unrestricted T cell toxicity in leprosy pathology. In: Spierings E, editor. Thesis Immunopathogenesis of leprosy neuritis. University of Leiden; 2000.
Bahia El Idrissi N, Das PK, Fluiter K, et al. M. leprae components induce nerve damage by complement activation: identification of lipoarabinomannan as the dominant complement activator. Acta Neuropathol. 2015;129(5):653–67. Epub 2015 Mar 15
Acknowledgements
This chapter is based on B. Naafs (2000) Current views on reactions in leprosy. Indian J Lepr 72: 97–122. (With kind permission by the Indian Journal of Leprosy.).
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Naafs, B., Noto, S. (2022). Reactions in Leprosy. In: Nunzi, E., Massone, C., Portaels, F. (eds) Leprosy and Buruli Ulcer. Springer, Cham. https://doi.org/10.1007/978-3-030-89704-8_21
Download citation
DOI: https://doi.org/10.1007/978-3-030-89704-8_21
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-89703-1
Online ISBN: 978-3-030-89704-8
eBook Packages: MedicineMedicine (R0)