
Abstract
The desire for optimal dental rehabilitation after the loss of teeth has spanned most of human history. Ancient historians have found evidence of teeth being replaced (likely postmortem) in edentulous sites with bamboo, metals, woods, and/or other natural teeth either from animals or cadavers, beginning as early as 2000 BCE. It was not until the nineteenth century that many looked to replace teeth by filling the extraction sockets with metals in the shape of tooth roots and splinting to adjacent teeth. The search for the best biomaterial and shape for dental implants consumed much of the twentieth century. Early metals allowed for fibrous-osseous stability, but it was not until the understanding of osseointegration with titanium that dental implants became a mainstay treatment. Work on bone grafting substances to regenerate bone have allowed providers to place dental implants in atrophic mandibles. Professor Per-Ingvar Brånemark is often credited as the father of modern dental implantology, and his work on osseointegration has been instrumental in the evolution of dental implants. Work in the twentieth century revealed that titanium appears to be the metal most biocompatible with bone. The first two decades of the twenty-first century have seen refinement of titanium to increase success rates, as well as increased accuracy of placement and restorations using technological advances such as cone beam computed tomography (CBCT) and intraoral scanners. Treatment planning software has further advanced accuracy through virtual planning and milling of surgical guides and the creation of dynamic navigation. While dental implants have come a long way, the future of tooth replacement likely resides not in the world of biomaterials but in molecular and cell biology.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Humans have waged a long battle against edentulism. Ancient history is poorly documented in the scientific literature. A simple Google search supplies tales of the earliest evidence of tooth replacement that is suspected to begin in 2000 BCE when bamboo was carved into peg teeth and used as replacement in edentulous sites (López-Píriz et al. 2019). A millennium later, a copper peg was hammered into the upper jaw of an Egyptian king (Smith 2019). It is unknown, however, whether the tooth was replaced during life or postmortem. In 500 BCE, Hippocrates wrote about using artificial teeth bonded with gold or silk. Archaeological excavations in France have uncovered a Celtic grave with a fake tooth composed of iron that is believed to have originated from approximately 300 BCE (Smith 2019). Archeologists have found many ancient civilizations with evidence of such tooth replacements made from ivory, metals, and the teeth of other animals. Most scholars believe that these replacements occurred postmortem as these implants would have likely had early failure. In the first century CE, Aulus Cornelius Celsus mentioned the possibility of replacing missing teeth with cadaver teeth. The collections of the Peabody Museum of Archaeology and Ethnology at Harvard University include a Mayan mandible dated to the seventh to eighth CE in which three shell pieces were used as lower incisor replacements (Pasqualini and Pasqualini 2009; Bobbio 1972).
The earliest evidence of attempted bone repair with a foreign material comes from the Neolithic period between 10,000 and 4500 BCE. The skull of an ancient Peruvian tribal chief was discovered with a large frontal bone defect that was repaired with an implanted hammered gold plate (Pryor et al. 2009). While this may seem quite primitive by modern standards, the Neolithic period is known widely for the development of metallurgy and directly preceded the Bronze and Iron ages, so this approach would have represented the absolute forefront of medical technology (Lubbock 1865).
Jumping forward to 2000 BCE, we see the first example of a xenograft from the ancient Khurtis people that inhabited modern Armenia. The anthropologist A. Jagharian, former head of operative surgery at the Erivan Medical Institute in Armenia, discovered two skulls with evidence of attempted grafting not far from Lake Sevan (Pryor et al. 2009). One of the skulls showed a 7 mm traumatic injury repaired with a single piece of animal bone. We can tell several millennia later that the patient survived this procedure for several years afterward because the cranium demonstrated signs of regrowth surrounding the grafted material (Pryor et al. 2009). The second skull discovered by Jagharian demonstrated a similar repair of a smaller 2.5 mm defect caused by a sharpened instrument (Pryor et al. 2009). Unfortunately, these finds predate reliable archival documentation by several thousand years. Therefore, it is impossible to get a sense of whether these procedures were commonplace or one-off experiments. Thankfully, much of the early history of dental implants has been described elsewhere in the literature. The authors implore you to explore the wonderful work of Ugo Pasqualini and Marco Pasqualini entitled “Treatise of Dental Implant Dentistry: The Italian Tribute to Modern Implantology (Pasqualini and Pasqualini 2009).” As an entire textbook can and has been devoted to this subject, the authors herein will attempt to highlight some of the monumental work that allowed for the development of modern implantology.
Several centuries after the collapse of the Mayan civilization, many scholars during the European Renaissance advocated for the splinting of lost teeth to adjacent teeth using wire or thread. Pierre Fauchard, considered to be one of the founders of dentistry, reported several cases of replantation and transplantation of teeth (Pasqualini and Pasqualini 2009). The idea of replantation of natural teeth occurred through the 1700s, until 1806 when Giuseppangelo Fonzi invented the first porcelain tooth (Anonymous 1968). Maggiolo then introduced the use of gold in the shape of tooth roots, stating that it added stability when stabilizing to adjacent teeth (Maggiolo 1809; Tanunja 2018). The use of metals for implantation into extraction sockets became widespread during the nineteenth century. It is believed that in the 1840s, Chapin Harris and Horace Hayden, founders of the Baltimore College of Dental Surgery, attempted implants with lead-coated platinum posts into artificial sockets. Others in the United States tried different metals including lead, gold, silver, platinum, and nickel (Pasqualini and Pasqualini 2009).
2 Implants in the Early Twentieth Century
The central focus of this chapter is the beginning of the twentieth century, during which procedures that resemble the modern implant began to emerge. Advancements in implantology during this period primarily occurred through two avenues. The first was new understanding in dental and osseous materials, and the second was biomechanical principles and the refinement of the implant shape. In 1913, Greenfield developed an endosseous hollow-cylinder basket shape implant made of iridium and gold soldering as artificial roots (Greenfield 2008; Block 2018a). He presented the stepwise use of drills increasing diameters that is still practiced today. These implants were used as a single tooth replacement. In the 1930s, Drs. Alvin and Moses Strock were researching the Vitallium® orthopedic screw fixtures used in hips. They used this metal to place a series of implants for teeth in animals and humans at Harvard. Vitallium is a cobalt-chrome-molybdenum alloy (originally manufactured by Howmedica Osteonics Corporation, now Stryker, Mathway, NJ) that was fabricated into a threaded design and placed as an immediate implant. In 1938, Adams developed and patented a submergible threaded cylindrical implant with a smooth gingival portion and healing abutment. The prosthetic used was a ball-hitch design for an overdenture (Burch 1997). Many new designs were fabricated at this time, many of which mirrored the typical wood screw with a helical thread pattern. Implants were typically a solid screw or hollow basket design composed of different alloy materials that result in a fibrous implant interface (Linkow 1966).
Prior to the hypothesis of osseointegration, implants used a fibrous-osseous integration system, which at the time was believed to be the ideal circumstance for stability of the prosthesis. It was not until the concept of osseointegration or direct integration of the bone to the metal that changed this fundamental thinking. In 1924, Zierold researched the reaction of different metals in dogs (Zierold 1924). Some of his observations were “gold, aluminum, and stellite were readily tolerated by bone and tended to be encapsulated with fibrous tissue; they were inert materials, unaffected by the living cells and body fluids; (2) silver and lead were slightly less tolerable to bone, but they easily underwent corrosion, and created a greater connective tissue response; (3) zinc corroded easily and caused a slight connective tissue reaction; (4) copper caused definite stimulation of bone, although it underwent slow corrosion; (5) steel and iron definitely inhibited bone regeneration and steel readily underwent corrosion (Rudy et al. 2008).” The search of the perfect biocompatible material continued. In 1940, the concept of osseointegration, specifically titanium, was first described by Bothe et al. in Great Britain (Bothe et al. 1940; Jokstad 2017). Later, a researcher in the United States reaffirmed this proposition stating, “since titanium adheres to bone, it may prove to be an ideal metal for prosthesis (Leventhal 1951).” In the same year, Dahl invented the subperiosteal implant design (Linkow and Dorfman 1991).
Linkow reported on the blade implant in 1968 (Linkow 1966). Prior to this, vertical post-type implants with spiral shafts, vents, and pins were primarily used as anchors for prosthetic support. Linkow noted difficulties with knife-edge ridges in terms of placement and resorption. This observation led to the idea of thin blades of larger anterior-posterior length rather than diameter. These were preformed after raising full-thickness flaps, exposing all the bone. High-speed drills were used to create channels, and the blades were tapped into the final position. Blade implants were used with some initial success. Linkow stated the blade implants formed a fibro-osseous integration that he believed was like the periodontal ligament of teeth from a histological perspective (Linkow and Rinaldi 1987).
In the mid-1970s, trans-osseous implants were used for overdentures in the anterior mandible. Kent et al. reported on the use of a mandibular staple bone plate to support a dental prosthesis through an extraoral incision in the submental parasymphysis region from the late 1970s. The plate was made from a titanium alloy (6% aluminum and 4% vanadium). They reported promising results in terms of stability in 160 patients. Bosker and van Dijk subsequently reported on 368 patients who underwent the procedure, 43 had reversible complications, and 1 had unilateral hypesthesia (Bosker and van Dijk 1989). The disadvantages to this approach were the extraoral incision, the need for general anesthesia, and less than ideal gingival implant interface.
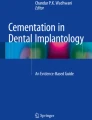
In 1978, the National Institutes of Health (NIH) held a Dental Implant Consensus Conference in Boston, Massachusetts, with the Harvard Tooth Implant-Transplant Research Unit at the School of Dental Medicine (Anonymous 1978). At this point, thousands of patients had been treated with dental implants for years. While many had been successful, many others had early failures and complications. The American Dental Association (ADA) had developed an implant registry to establish uniform case reports. The Food and Drug Administration (FDA) had begun to implement standards, classifications, and limitations on medical devices including implants. The panel described success as “functional service for five years in 75% of the cases.” The subject criteria for success included “adequate function, absence of discomfort, improved aesthetics, and improved emotional and psychological attitude.” The conference reported statistics on subperiosteal, transosteal, blade, and staple implants (Fig. 1). Ultimately, the conference identified the need for clinical trials to determine the best protocols for dental implants.

The X-ray controlling from 1976 to 1977 shows a subperiosteal implant (according to Cherchéve) in the maxilla. Two implant tripods (according to Pruin) in the lower canine region and two stabilized blade implants (according to Heinrich) in the molar region. (Image from Wikimedia commons. Public domain image. Reproduced without alterations. https://commons.wikimedia.org/w/index.php?search=blade+implants&title=Special:Search&go=Go&ns0=1&ns6=1&ns12=1&ns14=1&ns100=1&ns106=1#/media/File:Panoramic_radiograph_of_historic_dental_implants.jpg. This image is licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license. https://creativecommons.org/licenses/by-sa/3.0/deed.en. CC BY-SA 3.0)
Professor George Zarb in Toronto, Canada, recognized the need for the continued clinical research expressed in the 1978 NIH conference. Notably, titanium was not even mentioned at this 1978 conference. In 1982, the first Toronto Osseointegration Conference was held. It was the first opportunity for the most prominent prosthodontic and oral and maxillofacial surgery community in North America to come and learn from the most prominent dental implant researchers in the world at the time (Jokstad 2008). Among them was Dr. Brånemark and his research team.
3 Brånemark and the Foundations of Modern Implantology
The development of the dental implant relied heavily on the progression of various businesses throughout the second half of the twentieth century. Many different companies played important roles. While it would be too time-consuming to discuss the history of every business in the industry, we would be remiss not to include the contributions of Straumann and Nobel BioCare due to the contributions of Drs. Brånemark and Straumann. Reinhard Straumann founded the research institute Dr. Ing R. Straumann AG in Waldenburg, Germany, in 1954. In 1981, Professor Brånemark and the Swedish company Bofors cofounded Nobelpharma which later became Nobel Biocare in 1996.
It was not until 1982 that Per-Ingvar Brånemark, MD, PhD, introduced the titanium osseointegration implant to North America (Fig. 2). Professor Brånemark was a physician and anatomist in Sweden who discovered the concept of osseointegration in 1952 while studying blood flow in rabbit bone. He placed a titanium-housed optical component to a rabbit’s leg which allowed him to study the bones microcirculation (Fig. 3) (Brånemark 1983). After the completion of the study, he found he was unable to remove the device. He noted that titanium components can bond irreversibly with bone. This resulted in a pivotal movement in his team’s work, which quickly identified the value of titanium in this context.

Photograph of Professor Brånemark in June 2013. (Image from Wikimedia commons. Public domain image. Reproduced without alterations. https://commons.wikimedia.org/wiki/File:Branemark_headshot2. This image is licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license. https://creativecommons.org/licenses/by-sa/3.0/deed.en. CC BY-SA 3.0)

Radiograph of Per-Ingvar Brånemark’s rabbit specimen, showing a titanium optic chamber fixed to the rabbit’s tibia and fibula. (Image from Wikimedia commons. Public domain image. Reproduced without alterations. https://upload.wikimedia.org/wikipedia/commons/4/47/Branemark%27s_initial_radiograph.jpg. This image is licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license. https://creativecommons.org/licenses/by-sa/3.0/deed.en. CC BY-SA 3.0)
Brånemark was not the first to propose that titanium was a suitable biomaterial for implantation in bone. Biological researchers in dentistry and medicine, including Beder, Ploger, Emneus, and Stenram, were some of Professor Brånemark’s early mentors who demonstrated that bone tolerated implanted titanium well (Emneus and Stenram 1960; Beder and Ploger 1959). “A simple search for titanium on PubMed generates some 350 papers published before December 31, 1970 (Jokstad 2017).” But while his background was in orthopedics and anatomy, he saw the immense opportunity in dental implants. His group extracted teeth in dogs and replaced them by screw-shaped titanium implants. The implants were allowed to heal under a mucoperiosteal flap. Fixed prosthesis was connected after 3 to 4 months without loading. Radiological and histological analyses of the anchoring tissues showed integration at 10 years (Brånemark 1983). In 1977, Brånemark et al. reported on the osseointegration system for clinical jaw reconstruction using titanium-based implants (Brånemark et al. 1977). In 1983, they published a 5- to 9-year success rate of 3000 osteointegrated implants inserted into edentulous jaws of 400 consecutive patients in Gothenburg, Sweden (Brånemark et al. 1983). Two revelations were noted at this time. The first is the concept of osseointegration between the implant and the bone. The second was the establishment of a biological seal around the abutments penetrating the soft tissue, thus decreasing the inflammatory reaction. In 1974, Straumann engineered the first titanium hollow cylinder implant (Sutter et al. 1983). In 1997, NobelReplace released the first tapered dental implant designs, a design that better mimics tooth root morphology.
Brånemark quickly understood the issue with successive bone loss over time as well as the issue of inadequate bone for implant placement. In 1984, he and his colleagues reported on osseointegrated implants penetrating the maxillary sinus. They first conducted an experimental study in dogs and later a clinical study in humans. A total of 139 implants were placed that pierced the sinus or nasal cavity in 101 patients. At 5- to 10-year follow-up, the success rate was 70% in sinus-penetrating implants and 72% in nasal bone/mucosa implants (Brånemark et al. 1984). In 1988, Smalley et al. with the aid of Brånemark published on osseointegrated titanium implants in the maxilla, zygomatic, frontal, and occipital bones for maxillofacial protraction in Macaca nemestrina monkeys (Smalley et al. 1988). While this was monumental in the world of orthodontics in terms of eliciting skeletal changes, it was also the foundation for zygomatic implants in dental rehabilitation in the atrophic maxilla. The 1990s saw the use of maxillofacial implants for various reconstructions of the skeletal complex after trauma or ablative therapy.
Many important advancements occurred in the 1990s that allowed for further work with zygomatic implants. In 1995, Brånemark et al. described 156 edentulous patients who were fully rehabilitated by fixed prosthesis with either four or six titanium implants. After 3–4 months in the mandible and 5–8 months in the maxilla, abutments were placed, and prostheses were fabricated. This landmark study was the cornerstone for modern full-arch dental rehabilitation concepts we use today (Brånemark et al. 1995). Two years later, Tarnow et al. reported on immediate loading of threaded implants in 10 patients. Of 69 implants that were loaded, 67 integrated. Six patients were treated with Nobel Biocare implants, one with ITI Bonefit, two with Astra Tech TiOblast implants, and one with 3i implants (Tarnow et al. 1997). This was groundbreaking evidence as up until this point, Adell and Brånemark had maintained that a prerequisite for successful osseointegration was a non-loaded environment. The ITI® (International Team for Implantology by Straumann) released the SLA (sandblasted, large grit, acid-etched) surface implant in June 1998, increasing our understanding of osseointegration and implant success (Scacchi et al. 2000).
In the search for a suitable esthetic fixed prostheses supported by dental implants, Fortin et al. described the Marius bridge in 2002 (Fortin et al. 2002). The Marius bridge was named after the first patient treated with this prosthesis. The implants were placed between 1991 and 1994, and the bridge restorations were placed in patients between 1993 and 1995 and followed for a period of 5 years. The process required utilization of the concept of anterior-posterior spread, a fundamental principle in 2020. The authors noted that moderate to severely resorbed maxilla often have too thin of bone to allow vertical placement of implants, specifically in the posterior region. The authors used tilted implants to overcome this obstacle. It is a principle that will be carried forward over the next two decades. The “All-on-Four” concept was first learned in 1998 with Maló, Rangert, and Nobre in collaboration with Nobel Biocare. In 2003, Maló et al. described in the literature the use of the “All-on-Four” immediate function with the Brånemark System for complete edentulous maxillae with a 1-year follow-up in 32 patients. They used both straight and angulated (17° and 30°) implants with Brånemark System multiunit abutments. Immediate provisional complete arch acrylic prostheses were delivered the day of the surgery, and a final prosthetic was delivered at 12 months postoperatively (Maló et al. 2003).
Armed with information about immediate loading and anterior-posterior spread, tremendous advancements in zygomatic implants for dental rehabilitation were possible. Prior to this, implants in the maxillofacial complex were targeted for reconstruction of the skeletal structure rather than dental function. In 2000, Tamura et al. published a case report of zygomatic implants following subtotal maxillectomy with fabrication of a maxillary prosthesis (Tamura et al. 2000). In 2004, Brånemark et al. published on 52 zygomatic fixtures for the atrophic maxilla with an overall prosthetic rehabilitation rate of 96% after at least 5 years of function (Brånemark et al. 2004). Two years later, Anlgren et al. reported on 25 successful zygomatic implants placed from 199 to 2001, with an 11- to 49-month follow-up (Ahlgren et al. 2006). That same year, Bedrossian et al. described the immediate function with the zygomatic implants in 14 patients (28 bilateral zygomatic implants and 55 premaxillary implants) that supported an immediate fixed provisional prosthesis (Bedrossian et al. 2006).
The desire for flapless surgery and immediate loading accelerated the development of computer-aided treatment planning and fabrication of surgical stents and prosthesis. In 2005, NobelGuide was released by Nobel Biocare as one of the first guided surgery systems (Marchack 2005). In 2007, Bedrossian published a report on the use of NobelGuide for a computer-guided, implant-supported complete maxillary rehabilitation (Bedrossian 2007).
4 Bone Augmentation
The modern era of bone grafting began in the mid-seventeenth century with a Dutch surgeon named Job Van Meekeren. In 1668, Van Meekeren performed the first heterologous grafting procedure on an injured soldier (de Boer 1988). He used a fragment of dog bone to repair a skull puncture wound, and the procedure was successful overall (de Boer 1988). However, in the eyes of the Christian church at that time, the implantation of nonhuman tissues was considered blasphemous and resulted in the excommunication of the soldier from the church. After enduring the unfortunate consequences of excommunication from the permanent institution of the church, the soldier returned to Van Meekeren to have the dog bone fragment removed so he could be readmitted to the church. Unfortunately for the soldier, upon reentering the site of the graft, Van Meekeren discovered that the fragment had completely incorporated into the surrounding tissues (de Boer 1988).
In the late seventeenth and early eighteenth centuries, orthopedic surgeons began to focus their research efforts on the microscopic structure of bone aided by advances in microscope technology. The earliest of descriptions of the microscopic anatomy of bone came from Antonie van Leeuwenhoek. In 1674, van Leeuwenhoek published the first description of the canal-based structure of cancellous bone and also began to define the terms “implant,” “resorption,” and “bone callus” (de Boer 1988). This foundational work opened the door for later research advances in bone physiology and grafting. The discoveries and descriptions provided by van Leeuwenhoek’s publications started an era of intense debate over the origins of osteogenic potential in bone. In 1739, Henri-Louis Duhamel performed an animal experiment in which he implanted silver wires beneath the periosteum and allowed the surgical wound to heal for several weeks before reentering the site (Hernigou 2015). When he observed the wires several weeks later, he discovered that they had become buried in bone (Hernigou 2015). Duhamel used these experimental results and repeated the experiments of some of his predecessors to validate his assertion that the periosteum had osteogenic potential (Hernigou 2015).
Duhamel’s publications were met with mixed reception by his contemporaries. His biggest opponent, Albrecht Von Haller, believed instead that the periosteum was merely a support system for the blood vessels and that exudation from blood vessels was the true cause of osteogenesis (Hernigou 2015). In 1763, Von Haller published his book Experimentorum de Ossium Formatione in which he elaborated on the idea that blood vessels carried the mineral elements required for osteogenesis and therefore were the major source of osteogenic potential. At the time, this was an extremely controversial notion. The feud between the two men, who represented the two leading theories of the era, became notorious enough that it came to be known as “Duhamel-Haller Controversy” (Hernigou 2015). Unfortunately, neither of the two men would live to see the dispute settled. Jean Pierre Marie Flourens went a long way in settling this controversy when he conclusively showed in his 1842 publication that periosteum was osteogenic and was the chief agent in healing and repair of bone defects (Hernigou 2015).
Surgeons did not stand idle awaiting the resolution of academic conflicts and chose to forge ahead with experimental procedures. In 1820, the German surgeon Phillips Von Walters described the first use of a bone autograph (Henkel et al. 2013). Walters successfully repaired trepanation holes – created during a procedure to relieve intracranial pressure – with pieces of bone harvested from other sites on the patient’s skull (Henkel et al. 2013).
Advances in both bone biology and bone grafting technology in the mid-nineteenth century were dominated by Louis Léopold Ollier. Ollier was a French surgeon who began his career as a botanist and closely studied the microscopic organization of tree bark, which perhaps sparked his eventual interest in periosteum (Donati et al. 2007). In 1858, Ollier took the first scientific experimental approach to solve the riddle of osteogenesis. Despite a lack of sterile surgical technique or modern histological tools, Ollier made several discoveries and is credited with the first use of the term “bone graft” in an 1861 publication (Donati et al. 2007). He determined that transplanted bone and periosteum survived and became osteogenic if given the proper conditions. In a textbook published in 1867, Ollier noted that periosteum-coated grafts were best for transplanting and further stated that the contents of the haversian canals and the endosteum were also osteogenic (Hernigou 2015).
These assertions were considered and incorporated into cutting-edge subperiosteal and subcapsular surgical excision techniques, which became the standard of care in the treatment of bony malunion secondary to traumatic fracture (Hernigou 2015). At this time, malunion was commonly treated with large resections or even amputations. Therefore, the subperiosteal resection technique offered another means to achieve bone healing and avoid amputation. These contributions earned Ollier the Great Prize for Surgery established by Napoleon III. Despite being widely considered an authority in the field by his colleagues and contemporaries, Ollier’s publications were not without dissenters (Donati et al. 2007). In the late 1800s, Arthur Barth, a German surgeon, began publishing the findings of his own experiments in which he directly refuted the claim that the graft survived past the first few days of implantation. Barth asserted that the implanted material underwent gradual necrotic change (Henkel et al. 2013). He used rabbit and dog models to show that dead graft material was resorbed and replaced by native tissues (Henkel et al. 2013). This difference of opinions was one of the innumerable scientific feuds that would not be resolved until after the time of both Ollier and Barth.
Around 1885, Ollier began to revisit some of his earlier experiments in xenografting. With the emergence of sterile surgical technique in the mid-1860s, he was curious to see if new sterilization protocols would improve the outcomes of some of his earlier failures (Hernigou 2015). Grafts were found to experience less morbidity when the recipient [rabbit or cat] was from a higher species and the donor [chicken] was a member of a less advanced species (Hernigou 2015). Ollier was also able to successfully graft from one mammal to another; however, he noted that over time, the graft material would disappear. He further noted that there was no guarantee of a graft taking in a human recipient unless the donor material had come from a very closely related species, such as monkeys, and even in that case, the graft only provided transient benefit (Hernigou 2015). With this in mind, Ollier concluded that homographs and autographs were the most reliable options to repair bony defects with the limitation of technology.
Despite focused research efforts from Ollier and his contemporaries, use of non-autologous grafts in human patients were seriously considered until late in the nineteenth century. The reason is not exactly clear; perhaps there were some religious or moral concerns stemming from the experience of Van Meekeren a few centuries earlier. In 1880, the Scottish surgeon William Macewen pushed the field into the modern era when he published his case report from 1879, in which tibial bone from one child infected with rickets was grafted into the heavily deformed humerus of another child that had been resected secondary to osteomyelitis (Hernigou 2015). This represented the first successful documented bone allograft in a human. The achievement effectively opened up a new field in bone surgery. In the years that followed this initial success, Macewen would earn further recognition by being the first surgeon to repair a mandibular defect with bone harvested from the ribs (de Boer 1988).
Abel M. Phelps was another important contributor to the early development of bone grafting technology. In 1891, he published a landmark case report of a young man with ununited leg fractures who has undergone several previous surgeries with minimal success. Phelps was initially reluctant to continue attempting surgical repair; however, sensing the desperation of the patient’s parents to avoid amputation, he agreed to try one last-resort measure (Hernigou 2015). Phelps transplanted a portion of bone from the foreleg of a dog into the leg of his patient. Both donor and host were left attached to each other for 2 weeks to maintain circulation to the graft. Phelps believed that leaving the vascular supply of the graft intact would initiate the growth of new bone in the boy’s limb (Hernigou 2015). About 15 days after the graft, the patients were separated, and Phelps noted that the boy’s bone graft had become irregularly covered in new bone. Both patients had a brief convalescence after the operation (Hernigou 2015). Phelps claimed no specific references when asked how he planned and designed the procedure. Instead, he said that “observation in my studies during the past two years convinced me that circulation between two opposite species could be established with safety” (Hernigou 2015). While the procedure was ultimately a failure, it still represents a landmark in the overall field as it was the first example of a vascularized flap used in a human patient. Abel Phelps’ meticulous documentation of his procedure, observations, and insightful commentary on possible reasons for his failure allowed even his unsuccessful work to become a stepping stone and invaluable training resource for the surgeons and researchers that would follow.
The early twentieth century saw a new group of researchers such as Putti, Phemister, and Albee rise to the forefront of bone grafting research and publication. In 1912, Vittorio Putti, an Italian orthopedic surgeon, published a review of the state-of-the-art research in the field of bone grafting and biology at the time. He reviewed the work of previous authors, his contemporaries, and combined this information with his own personal clinical experience and observations to elucidate some generalized clinical indications for the use of bone grafts (Donati et al. 2007). Putti also proposed a bone-lengthening technique, which is now called distraction osteogenesis, and suggested novel uses of bone grafts such as grafting growth-plate cartilage into adult patients (Donati et al. 2007). This report represented a unification and clarification of many emerging principles of the era and formed the foundation of much of the progress to follow.
In 1914, Dallas Burton Phemister performed several experiments in dogs to further investigate osteogenesis. Earlier works had heavily debated the osteogenic potential of the graft itself. There was ongoing disagreement about whether grafts integrated via osteogenesis or if the existing donor tissue was responsible for integration (Donati et al. 2007). Phemister took a big step in introducing the modern concept of bone resorption when he described a phenomenon he called “creeping substitution” (Donati et al. 2007). He went further to say that the amount of time a graft needed to complete its resorption was anywhere from 3 to 12 months depending on the size, thickness, and location of the graft (Donati et al. 2007). He explained how the proximity of the endosteum and periosteum to adequate blood supply would allow those tissues to survive, while the relative lack of circulation of the deeper portions of the graft would cause cellular necrosis and resorption of the inorganic portion of the cellular matrix (Hernigou 2015). Phemister’s 1914 publication would become one of the most frequently cited English works in the field. This authoritative publication was followed by an almost equally important work from FH Albee. Albee published his “Rules for Using Bone Grafts” in 1915 which described data from his own surgeries on various autologous bone harvesting sites such as the iliac crest, trochanter, tibia, metatarsal, olecranon, fibula, and cranium (Albee 1923).
By the mid-1940s, autologous and homologous bone grafting had become widely used procedures. Alberto Inclan published an article in the Journal of Bone and Joint Surgery in 1942 in which he presented the outcomes of a large number of his cases and discussed the common issues of the current technology (Inclan 1942). At that time, medical science was beginning to understand the immunological challenges related to homologous grafts. Inclan discussed that a homologous graft between two living patients of the same blood group was possible, albeit inconvenient at times. He and his colleagues began to hint at the modern concept of storing bone material for future use (Donati et al. 2007). In his 1942 publication, Inclan began to outline a storage protocol for bone grafts. He wrote that grafts should be kept immersed in the donor or host’s blood within a sterile glass container in a refrigerated environment between 2 and 5 °C (Donati et al. 2007). While the implementation of the modern bone bank would have to wait for improved refrigeration technology, the idea of uncoupling the harvesting and use of bone grafts was revolutionary for the time (Donati et al. 2007).
While many of the brightest and most influential minds of the scientific community were trying to define the best way to perform bone grafts using human tissues, an equally dedicated group was beginning to research alternative materials to replace bone. As early as 1892, Dressman was exploring the use of calcium sulfate (plaster of Paris) for the repair of large bony defects (Donati et al. 2007). In his 1912 publication, Putti also commented on the use of ivory as a possible bone substitute when harvesting adequate material from the donor or the host was not possible (Donati et al. 2007). However, many early bone substitutes at this time led to the same unfortunate outcome: infection, graft rejection, and, ultimately, failure of the procedure. Medical science would need to make several key advances before materials could be designed to avoid some of the pitfalls of their earlier predecessors.
Calcium orthophosphates were discovered and described as early as the 1770s. However, the use of materials such as hydroxyapatite (HA) in bone grafting studies only began to gain momentum in the 1950s (Kattimani et al. 2016). HA has properties that make it nonreactive with the adjacent living tissues. For that reason, it remains one of the more popular materials that accounts for a large quantity of the regenerative graft materials available today (Kattimani et al. 2016). HA-based grafting materials were truly revolutionary for the field of bone grafting overall. These materials gave rise to what would later be called the first generation of biomaterials (Hench and Thompson 2010). Professor Bill Bonfield, a medical materials researcher at Cambridge University, was one of the pioneers whose research efforts led to the widespread incorporation of bioactivity as a consideration in the design of new materials and allowed the acceleration of the field from the 1960s forward (Hench and Thompson 2010). During the 1960s and 1970s, the primary goal in the development of new grafting materials was to diminish the biological response to the foreign body (Hench and Thompson 2010). This was achieved by eliminating release of toxic by-products. These materials are called “bioinert” as they create no response in the surrounding tissues (Hench and Thompson 2010).
Despite the success of the first generation of biomaterials and the improvements they provided in the lives of millions of patients, Bonfield recognized the need for an improved generation of biomaterials. The 1980s saw the rise of the second-generation biomaterials, such as Hapex, a material trademarked by Bonfield’s research laboratory (Hench and Thompson 2010). Second-generation biomaterials were designed to incorporate the concept of bioactivity, which aimed not only to closely mirror the architecture of native tissues and their mechanical properties but also to create a beneficial response in the tissues surrounding the graft (Hench and Thompson 2010). These innovative materials were composed of polymeric matrices of polyethylene with HA particles dispersed throughout. Bonfield continued designing and discovering new biomaterials, such as Si-substituted HA, which is still considered a successful bone grafting material (Hench and Thompson 2010). By the mid-1980s, bioactive bone grafting had reached clinical use in a variety of orthopedic and dental applications, largely thanks to the research and commercialization efforts of the Bonfield laboratory.
Second-generation biomaterials explored the utility of bioactivity and materials that were reliably and predictably resorbed by the host. These advances converged in the third generation of biomaterials starting in the 2000s (Hench and Thompson 2010). Now, resorbable polymer systems are being modified on the molecular level to elicit specific interactions with cellular integrins and thereby encouraging cellular differentiation and extracellular matrix production and organization (Hench and Thompson 2010). These materials generally fit into one of two categories: bioactive glass or hierarchical porous foams that activate genes in neighboring tissues and stimulate regeneration of living tissues (Hench and Thompson 2010).
The future of bone grafting materials is likely to be governed by two competing schools of thought. In one camp, there are materials designed for in situ tissue regeneration, and in the other, there is tissue engineering. The emerging field of tissue engineering aims to seed progenitor cells on molecularly modified scaffolds outside the body to allow the cells to become differentiated and mimic native tissues. Engineered tissues are then implanted to replace diseased or damaged tissues. By contrast, in situ tissue regeneration materials aim to achieve the same result by implanting a material initially that will encourage the local tissue to regenerate or repair itself. The addition of these concepts to improving knowledge of immunology and endocrinology will lead to the emergence of new materials with multifaceted effects on regeneration and repair of local tissues.
5 Guided Bone Regeneration
Guided bone regeneration (GBR) procedures are dental surgical procedures which use a membrane to guide the growth of bone and gingival tissues in areas that may be lacking tissue for a variety of reasons. At present time, GBR is the intersection of bone grafting technology with clinical dentistry. The rising popularity of dental implants has driven interest in both the preservation and creation of bone as means of developing sites for later prostheses. In 1976, Dr. Tony Melcher began defining the basic principles and theories of GBR for use in dental applications (Melcher 1976). One of Melcher’s largest contributions was his recognition of the importance of using implantable barriers to exclude unwanted cell lineages from prematurely colonizing graft material (Melcher 1976). The positive results of Melcher’s studies up to the 1980s and their application to periodontics sparked interest in the study of rebuilding larger alveolar bone defects with guided bone regeneration. GBR was first attempted by Dahlin et al. in 1988 on rats. They found that if the bone was protected and kept away from adjacent tissues, via a membrane, there was improved ingrowth of bone-forming cells into a bony defect; this was confirmed in a study by Kostopoulos and Karring in 1994 (Kostopoulos and Karring 1994). Recent systematic review has shown that the outcomes following GTR are highly variable, both between and within studies, meaning that clinicians must still take great care in case selection to ensure the best possible outcomes (Needleman et al. 2006).
6 Sinus Lifts
The maxillary sinuses sometimes are in the way of placing maxillary posterior implants. The development of both dental implants and bone augmentation materials has allowed this procedure to develop and evolve. The first lateral window or direct sinus-lift procedure is credited to Dr. Hilt Tatum in 1973. Dr. Tatum graduated from the Emory University Dental School in 1957. He performed the first sinus graft in 1975 at Lee County Hospital in Opelika, Alabama. This was followed by successful placement of two implants. As many are aware, the sinus membrane is quite thin and easily damaged. Early on, the sinus elevation was done using inflatable catheters. Eventually, instruments were fabricated to better handle this delicate tissue. Dr. Tatum was presenting his findings at the American Academy of Implant Dentistry in the late 1970s, and Dr. Philip Boyne was in attendance. Dr. Boyne and his colleague Dr. James would advance this technique and publish their methods in 1980 (Tatum Jr. 1986; Boyne and James 1980). Dr. Robert Summers is believed to have described first the internal/indirect sinus lift for sinuses that needed to be lifted less than 4 mm. This technique is accomplished by preforming the osteotomies with drills just shy of the sinus floor and using osteotomes to tap up the sinus floor leaving the membrane intact. Bone particulate graft is then placed to keep the sinus elevated, and the dental implants can be placed (Summers 1998). The lateral window for direct sinus lift is an invasive approach and may be falling out of favor. Dr. Block published a technique in 2019 describing a crestal window approach for direct sinus elevation with successful outcomes (Block 2018b). While sinus lift will likely always have some indications, with the use of smaller implants, this technique could become less utilized.
7 The Twenty-First Century
Recently, there has been a renewed interest in the use of platelet-rich plasma (PRP) and platelet-rich fibrin (PRF). Marx first described the use of PRP and PRF in the dental field in 1998, where he reported positive healing of the alveolar bone with its use (Marx et al. 1998). PRP is a concentration of platelet and plasma proteins derived from whole blood that is placed in a centrifuge to remove the red blood cells. PRP is believed to work via the degranulation of the alpha granules in platelets which contain several growth factors (Scully et al. 2018). PRP contains a variety of growth factors/cytokines such as transforming growth factor beta (TGF -beta), platelet-derived growth factor (PDGF), insulin-like growth factor (IGF), and epidermal growth factor (EGF).
A study performed using 72 dental implants in nine beagles dogs attempted to analyze the bone remodeling using PRP and PRF. After 3-month follow-up, the authors concluded that there was no increase in primary or secondary implant stability, but they did see a biological improvement in the peri-implant bone volume and structural integration (Huang et al. 2019). Although clinical effects have yet to be established, a biological effect is being consistently observed. In one in vitro study, in which roughened titanium dental implants were treated with PRP, the authors found that the number of cells observed around the implant at day 5 was double that of the non-PRP-coated implant (Lee et al. 2016). Research into the use of such biologics to increase osseointegration and soft tissue healing will likely continue over the next several decades. A randomized, split mouth design was conducted for eight patients who needed bilateral widening of keratinized mucosa around dental implants in the mandible. On one side of the mouth, a free gingival graft was placed, while on the other, a PRF membrane was placed. The mean amount of keratinized mucosa at the implant at the PRF-only site was 3.3 mm ± 0.9 and 3.8 mm ± 1.0 at the free gingival graft site (Temmerman et al. 2018). Now that integration of the implants is well established, the interest in dental implants have pivoted to longevity and precision. Soft tissue appears to be a key component in implant longevity and late failure.
One of the greatest advancements so far of the early twenty-first century was not so much in the dental materials but in treatment planning. Much of this is due to better data collection primarily from computer-aided technology such as cone beam computed tomography (CBCT), intraoral scanners, and treatment planning software allowing virtual planning and milling of surgical guides. The twentieth century had emphasis on getting stability and integration of the implant. The twenty-first century has been about placing the implants in the ideal location to allow for optimal dental prosthetic rehabilitation. When CBCTs first became available, radiographic stents with fiducial markers are needed to be used with the planning software that made its utilization cumbersome and required significant time by the provider. With the advancement of scanners and software, fiducial markers are no longer needed. Many companies have created user-friendly planning software to design implant treatment plans and seamlessly use 3D printing technology to make surgical stents. The use of a well-designed surgical stent results in less than 2 mm crestal and apical deviation and less than 5-degree angulation error (Block 2018a; Luebbers et al. 2008; Nijmeh et al. 2005; Ewers et al. 2005).
Dynamic navigation has become common practice in the operating room, especially in cancer ablative surgery, and in surgery with difficult access. Dynamic navigation uses the data from CT scans and optical sensors to track in live time where the surgeon’s instruments are in relation to the patient’s anatomical structures on the computer, allowing for more precision in operative technique. Dynamic navigation has found its way into the world of dental implants with companies such as X-Nav Technologies®. These systems have many advantages including more precision with smaller flap designs given the improved accuracy even with less surgical access.
8 Future Direction
The twentieth century revealed that titanium appears to be the metal most biocompatible with bone. The first two decades of the twenty-first century has seen refinement of titanium to increase success rates as well as escalate accuracy of placement and restorations. Sandblasting, acid etching, and other techniques to cause roughened surfaces of the titanium have allowed more successful bone-implant interfaces (Wennerberg et al. 2018). Companies like Straumann and Nobel Biocare are continuing to refine their implant systems. In 2020, it is well established that long-term implant survival relies on adjacent healthy soft tissue. Nobel Biocare has released the TiUltra, which has advanced the field from focusing strictly on the bone-implant interface to also incorporate the soft tissue-implant interface (Karl and Albrektsson 2017).
The future of tooth replacement is likely not in the world of implantology but in regeneration. While full summarization of the current knowledge of tooth regeneration is outside the scope of this chapter, the authors felt it was appropriate to address the path that tooth replacement will likely take. Through the understanding of odontogenesis, tooth regeneration can be divided into scaffold-based and scaffold-free models (Bhanja and D’Souza 2016). In 2002, Young et al. used a poly L-lactide-co-glycolide scaffold using third molar tooth buds of pigs and were able to grow mineralized tooth structures in immunodeficient rat hosts (Young et al. 2002). This scaffolding work continues by many researchers including Duailibi, Honda, and Young with promising results (Young et al. 2005; Honda et al. 2005; Duailibi et al. 2004). The major drawback of the scaffold technique is the developed teeth are often very small and the size and shape are difficult to control. In 2004, Ohazama et al. developed a primordial tooth by recombination technique with a scaffold-free design that successfully developed normal histology (Ohazama et al. 2004). Nakao et al. in 2007 developed a novel 3D organ culture method in which they regenerated a tooth germ in a renal capsule and later transplanted to the jaw (Nakao et al. 2007). In 2009, Ikeda et al. used a similar 3D organ method and transplanted tooth germ into the first upper molar region of mice. The tooth demonstrated correct structure, including enamel, dentin, cementum, pulp, and periodontal ligament space, but the tooth was smaller than the natural teeth (Ikeda et al. 2009). Many challenges still exist in tooth regeneration, the first being an appropriate cell source and the second induction of odontogenic potency. Human urine-induced pluripotent stem cells (iPSCs) have been shown to possess odontogenic competence in the right microenvironment, but there is still a need for identification of a “tooth inducer (Li et al. 2019).” Whether it be full tooth regeneration or cell-biased repair, the future of tooth replacement is likely not in the world of biomaterials but in molecular and cell biology.
9 Summary
The search for the optimal way to replace missing teeth is still at large. The search for the best biomaterial and shape for dental implants consumed much of the twentieth century. Early metals allowed for fibrous-osseous stability, but it was not until the understanding of osseointegration with titanium that dental implants became a mainstay treatment. Work on bone grafting substances to regenerate bone has allowed providers to place dental implants in atrophic mandibles. The first two decades of the twenty-first century have seen refinement of titanium to increase success rates, as well as increased accuracy of placement and restorations using technological advances such as cone beam computed tomography (CBCT) and intraoral scanners. Treatment planning software has further advanced accuracy through virtual planning and milling of surgical guides and the creation of dynamic navigation. While dental implants have come a long way, the future of tooth replacement likely resides not in the world of biomaterials but in molecular and cell biology.
References
Ahlgren F, Størksen K, Tornes K. A study of 25 zygomatic dental implants with 11 to 49 months’ follow-up after loading. Int J Oral Maxillofac Implants. 2006;21:421.
Albee FH. Fundamentals in bone transplantation: experiences in three thousand bone graft operations. J Am Med Assoc. 1923;81:1429.
Anonymous. [In honor of Giuseppangelo Fonzi, inventor and maker of the 1st porcelain teeth in 1806]. Dent Cadmos. 1968;36:1185.
Anonymous. Dental implants: benefit and risks. In: Online NCS, editor. Dental implant consensus conference. Boston; 1978. p. 13.
Beder OW, Ploger WJ. Intraoral titanium implants. Oral Surg Oral Med Oral Pathol. 1959;12:787.
Bedrossian E. Laboratory and prosthetic considerations in computer-guided surgery and immediate loading. J Oral Maxillofac Surg. 2007;65:47.
Bedrossian E, Rangert B, Stumpel L, Indresano T. Immediate function with the zygomatic implant: a graftless solution for the patient with mild to advanced atrophy of the maxilla. Int J Oral Maxillofac Implants. 2006;21:937.
Bhanja A, D’Souza DS. Mapping the milestones in tooth regeneration: current trends and future research. Med J Armed Forces India. 2016;72:S24.
Block MS. Dental implants: the last 100 years. J Oral Maxillofac Surg. 2018a;76:11.
Block MS. The Crestal window approach for sinus floor grafting with delayed implant placement: a preliminary report. J Oral Maxillofac Surg. 2018b;76:2319.
Bobbio A. The first endosseous alloplastic implant in the history of man. Bull Hist Dent. 1972;20:1.
Bosker H, van Dijk L. The transmandibular implant: a 12-year follow-up study. J Oral Maxillofac Surg. 1989;47:442.
Bothe S, Beaton R, Davenport H. Reaction of bone to multiple metallic implants. Surg Gynecol Obstet. 1940;71:592.
Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38:613.
Brånemark PI. Osseointegration and its experimental background. J Prosthet Dent. 1983;50:399.
Brånemark PI, Hansson BO, Adell R, Breine U, Lindström J, Hallén O, Ohman A. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 1977;16:1.
Brånemark PI, Adell R, Albrektsson T, Lekholm U, Lundkvist S, Rockler B. Osseointegrated titanium fixtures in the treatment of edentulousness. Biomaterials. 1983;4:25.
Brånemark PI, Adell R, Albrektsson T, Lekholm U, Lindström J, Rockler B. An experimental and clinical study of osseointegrated implants penetrating the nasal cavity and maxillary sinus. J Oral Maxillofac Surg. 1984;42:497.
Brånemark PI, Svensson B, van Steenberghe D. Ten-year survival rates of fixed prostheses on four or six implants ad modum Brånemark in full edentulism. Clin Oral Implants Res. 1995;6:227.
Brånemark PI, Gröndahl K, Ohrnell LO, Nilsson P, Petruson B, Svensson B, Engstrand P, Nannmark U. Zygoma fixture in the management of advanced atrophy of the maxilla: technique and long-term results. Scand J Plast Reconstr Surg Hand Surg. 2004;38:70.
Burch RH. Dr. Pinkney Adams – a dentist before his time. Ark Dent. 1997;68:14.
de Boer HH. The history of bone grafts. Clin Orthop Relat Res. 1988;226:292.
Donati D, Zolezzi C, Tomba P, Viganò A. Bone grafting: historical and conceptual review, starting with an old manuscript by Vittorio putti. Acta Orthop. 2007;78:19.
Duailibi MT, Duailibi SE, Young CS, Bartlett JD, Vacanti JP, Yelick PC. Bioengineered teeth from cultured rat tooth bud cells. J Dent Res. 2004;83:523.
Emneus H, Stenram U. Reaction of tissues to alloys used in osteosynthesis. Experimental, histological examination of reaction of soft tissues in animals. Acta Orthop Scand. 1960;29:315.
Ewers R, Schicho K, Undt G, Wanschitz F, Truppe M, Seemann R, Wagner A. Basic research and 12 years of clinical experience in computer-assisted navigation technology: a review. Int J Oral Maxillofac Surg. 2005;34:1.
Fortin Y, Sullivan RM, Rangert BR. The Marius implant bridge: surgical and prosthetic rehabilitation for the completely edentulous upper jaw with moderate to severe resorption: a 5-year retrospective clinical study. Clin Implant Dent Relat Res. 2002;4:69.
Greenfield EJ. Implantation of artificial crown and bridge abutments. 1913. Compend Contin Educ Dent. 2008;29:232.
Hench LL, Thompson I. Twenty-first century challenges for biomaterials. J R Soc Interface. 2010;7:S379.
Henkel J, Woodruff MA, Epari DR, Steck R, Glatt V, Dickinson IC, Choong PF, Schuetz MA, Hutmacher DW. Bone regeneration based on tissue engineering conceptions - a 21st century perspective. Bone Res. 2013;1:216.
Hernigou P. Bone transplantation and tissue engineering. Part II: bone graft and osteogenesis in the seventeenth, eighteenth and nineteenth centuries (Duhamel, Haller, Ollier and MacEwen). Int Orthop. 2015;39:193.
Honda MJ, Sumita Y, Kagami H, Ueda M. Histological and immunohistochemical studies of tissue engineered odontogenesis. Arch Histol Cytol. 2005;68:89.
Huang Y, Li Z, Van Dessel J, Salmon B, Huang B, Lambrichts I, Politis C, Jacobs R. Effect of platelet-rich plasma on peri-implant trabecular bone volume and architecture: a preclinical micro-CT study in beagle dogs. Clin Oral Implants Res. 2019;30(12):1190–9.
Ikeda E, Morita R, Nakao K, Ishida K, Nakamura T, Takano-Yamamoto T, Ogawa M, Mizuno M, Kasugai S, Tsuji T. Fully functional bioengineered tooth replacement as an organ replacement therapy. Proc Natl Acad Sci. 2009;106:13475.
Inclan A. The use of preserved bone graft in orthopaedic surgery. JBJS. 1942;24:81–96.
Jokstad A. The Toronto Osseointegration conference revisited. Osseointegration; 2008.
Jokstad A. Why did Professor Per-Ingvar Brånemark never receive the Nobel Prize in Medicine? Clin Exp Dent Res. 2017;3:79.
Karl M, Albrektsson T. Clinical performance of dental implants with a moderately rough (TiUnite) surface: a meta-analysis of prospective clinical studies. Int J Oral Maxillofac Implants. 2017;32:717.
Kattimani VS, Kondaka S, Lingamaneni KP. Hydroxyapatite–past, present, and future in bone regeneration. Bone Tissue Regen Insights. 2016;7:BTRI.S36138.
Kostopoulos L, Karring T. Augmentation of the rat mandible using guided tissue regeneration. Clin Oral Implants Res. 1994;5:75.
Lee JH, Nam J, Nam KW, Kim HJ, Yoo JJ. Pre-treatment of titanium alloy with platelet-rich plasma enhances human osteoblast responses. Tissue Eng Regen Med. 2016;13:335.
Leventhal GS. Titanium, a metal for surgery. J Bone Joint Surg Am. 1951;33-a:473.
Li L, Tang Q, Wang A, Chen Y. Regrowing a tooth: in vitro and in vivo approaches. Curr Opin Cell Biol. 2019;61:126.
Linkow LI. Clinical evalusation of the various designed endosseous implants. J Oral Implant Transplant Surg. 1966;12:35.
Linkow LI, Dorfman JD. Implantology in dentistry. A brief historical perspective. N Y State Dent J. 1991;57:31.
Linkow LI, Rinaldi AW. The significance of “fibro-osseous integration” and “osseointegration” in endosseous dental implants. Int J Oral Implantol. 1987;4:41.
López-Píriz R, Cabal B, Goyos-Ball L, Fernández A, Bartolomé JF, Moya JS, Torrecillas R. Current state-of-the-art and future perspectives of the three main modern implant-dentistry concerns: aesthetic requirements, mechanical properties, and peri-implantitis prevention. J Biomed Mater Res A. 2019;107:1466.
Lubbock J. Pre-historic times: as illustrated by ancient remains, and the manners and customs of modern savages. London: Edinburgh, Williams and Norgate; 1865.
Luebbers H-T, Messmer P, Obwegeser JA, Zwahlen RA, Kikinis R, Graetz KW, Matthews F. Comparison of different registration methods for surgical navigation in cranio-maxillofacial surgery. J Cranio-Maxillofac Surg. 2008;36:109.
Maggiolo J. Manuel de l’art dentaire (Manual of dentalart). Nancy, France: C Le Seure; 1809.
Maló P, Rangert B, Nobre M. “All-on-Four” immediate-function concept with Brånemark System implants for completely edentulous mandibles: a retrospective clinical study. Clin Implant Dent Relat Res. 2003;5(Suppl 1):2.
Marchack CB. An immediately loaded CAD/CAM-guided definitive prosthesis: a clinical report. J Prosthet Dent. 2005;93:8.
Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR. Platelet-rich plasma: growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85:638.
Melcher AH. On the repair potential of periodontal tissues. J Periodontol. 1976;47:256.
Nakao K, Morita R, Saji Y, Ishida K, Tomita Y, Ogawa M, Saitoh M, Tomooka Y, Tsuji T. The development of a bioengineered organ germ method. Nat Methods. 2007;4:227.
Needleman IG, Worthington HV, Giedrys-Leeper E, Tucker RJ. Guided tissue regeneration for periodontal infra-bony defects. Cochrane Database Syst Rev. 2006;(2):CD001724.
Nijmeh AD, Goodger NM, Hawkes D, Edwards PJ, McGurk M. Image-guided navigation in oral and maxillofacial surgery. Br J Oral Maxillofac Surg. 2005;43:294.
Ohazama A, Modino SAC, Miletich I, Sharpe PT. Stem-cell-based tissue engineering of murine teeth. J Dent Res. 2004;83:518.
Pasqualini U, Pasqualini ME. Treatise of implant dentistry: the Italian tribute to modern implantology. Carimate: Ariesdue; 2009. © Copyright 2009 Azienda Pubblica di Servizi alla Persona “Suor Agnese”.
Pryor LS, Gage E, Langevin CJ, Herrera F, Breithaupt AD, Gordon CR, Afifi AM, Zins JE, Meltzer H, Gosman A, Cohen SR, Holmes R. Review of bone substitutes. Craniomaxillofac Trauma Reconstr. 2009;2:151.
Rudy RJ, Levi PA, Bonacci FJ, Weisgold AS, Engler-Hamm D. Intraosseous anchorage of dental prostheses: an early 20th century contribution. Compend Contin Educ Dent. 2008;29:220.
Scacchi M, Merz BR, Schär AR. The development of the ITI dental implant system. Part 2: 1998–2000: steps into the next millennium. Clin Oral Implants Res. 2000;11(Suppl 1):22.
Scully D, Naseem KM, Matsakas A. Platelet biology in regenerative medicine of skeletal muscle. Acta Physiol (Oxf). 2018;223:e13071.
Smalley WM, Shapiro PA, Hohl TH, Kokich VG, Brånemark PI. Osseointegrated titanium implants for maxillofacial protraction in monkeys. Am J Orthod Dentofac Orthop. 1988;94:285.
Smith Y. History of dental implants. 2019.
Summers RB. Sinus floor elevation with osteotomes. J Esthet Dent. 1998;10:164.
Sutter F, Schroeder A, Straumann F. Engineering and design aspects of the I.T.I. hollow-basket implants. J Oral Implantol. 1983;10:535.
Tamura H, Sasaki K, Watahiki R. Primary insertion of implants in the zygomatic bone following subtotal maxillectomy. Bull Tokyo Dent Coll. 2000;41:21.
Tanunja. A complete review of Dental Implant Materials. Int J Recent Scientific Res. 2018;9:29665.
Tarnow DP, Emtiaz S, Classi A. Immediate loading of threaded implants at stage 1 surgery in edentulous arches: ten consecutive case reports with 1- to 5-year data. Int J Oral Maxillofac Implants. 1997;12:319.
Tatum H Jr. Maxillary and sinus implant reconstructions. Dent Clin N Am. 1986;30:207.
Temmerman A, Cleeren GJ, Castro AB, Teughels W, Quirynen M. L-PRF for increasing the width of keratinized mucosa around implants: a split-mouth, randomized, controlled pilot clinical trial. J Periodontal Res. 2018;53:793.
Wennerberg A, Albrektsson T, Chrcanovic B. Long-term clinical outcome of implants with different surface modifications. Eur J Oral Implantol. 2018;11(Suppl 1):S123.
Young CS, Terada S, Vacanti JP, Honda M, Bartlett JD, Yelick PC. Tissue engineering of complex tooth structures on biodegradable polymer scaffolds. J Dent Res. 2002;81:695.
Young C, Abukawa H, Asrican R, Ravens M, Troulis M, Kaban L, Vacanti J, Yelick PC. Tissue-engineered hybrid tooth and bone. Tissue Eng. 2005;11:1599.
Zierold AA. Reaction of bone to various metals. Arch Surg. 1924;9:365.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

{kind=link}
{kind=link}
Cite this chapter
Halepas, S., MacCormac, K., Ferneini, E.M. (2022). Dental Implants and Bone Augmentation. In: Ferneini, E.M., Goupil, M.T., Halepas, S. (eds) The History of Maxillofacial Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-89563-1_10
Download citation
DOI: https://doi.org/10.1007/978-3-030-89563-1_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-89562-4
Online ISBN: 978-3-030-89563-1
eBook Packages: MedicineMedicine (R0)