
Abstract
When positioning for sleep, the spine must be in optimal alignment. For that, during sleep, the use of a proper sleeping system constituted by a head pillow, a mattress and its surface is a must. Therefore, the sleeping system should have different elastic properties, the so-called custom-made arrangement, as we differ individually from biotypes, anthropometry, bodyweight distribution, height and weight, and sleeping habits. Individuals with different sleeping characteristics require different zonal stiffnesses in the mattress in order that the mattress maintains their spine in natural alignment during the recumbent posture we adopt to sleep. Physiotherapists should encourage patients/clients to have an individually adapted sleep system according to their physical needs and conditions.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
It is during sleep that the whole body recomposes and prepares itself for the next day. Being asleep is a state of physical and mental restoration, essential to the body, where the plasticity of the entire organism occurs. Thus, body supporting during sleep is of major importance. The human spine must be supported by the combination of a mattress, a bed base, and a pillow to adopt its natural position. The acquisition of a non-neutral position may influence painful processes, and in particular, musculoskeletal system pathologies.
Sleep quality and comfort are frequent questions of patients in the daily practice of physiotherapists, as the number of hours and the quality of sleep is well established to affect overall health – and to acquire that one must sleep on a proper surface. The posture adopted during sleep influences the physical health of the individual and may be correlated with musculoskeletal disorders in the shoulders, neck, lumbar region, as well as headaches, for example, that can, in turn, predispose to sleep fragmentation, poor quality, and quantity, leading to sleep disturbances.
A proper sleep system (i.e., mattress and support structure, and head pillow) can align the spine to some extent in its neutral posture which is the same as the spine alignment in the upright position [1]. A non-neutral posture can affect lateral bending and unbalanced loading on intervertebral disks and facet joints. For the intervertebral disks, growth and restoration depend on the amount of pressure and its manner of application on them, as to hydrate the soft tissues. During sleep, there is a change of the direction of the gravity vector; the intervertebral disks are unloaded and can rehydrate to restore their elasticity [2]. Supplying a patient/client with proper surfaces upon which to relax is also the focus of physical therapy.
The causes of pain in the axial skeletal muscle system may be due to mechanical disorder, postural and ergonomic factors, or excessive overload of the upper or lower limbs. Mechanical factors can be attributed to resting postures such as deviations in the position of the head, static or repetitive contractions of the neck muscles [3, 4]. For instance, sleeping with an incorrect height of the pillow: high, low, or no pillow (too low), or even sleeping in an incorrect posture may lead to frequent awakenings, to pain during the night and following day, or even to chronic pain in a course of time.
1 What Is a Good Posture for Sleep?
How is the correct body alignment during sleep? Having a good posture can increase body awareness and injury prevention. Posture can be defined as the distribution of body masses in space, this distribution being harmonious, involving a minimum amount of effort and overload and leading to what we call “good posture.” The alignment of body mass and joints is one of the fundamental characteristics to acquire the “good posture”. However, maintaining alignment does not depend on our voluntary control; the movement is often carried out involuntary during the recumbent posture that we adopt when asleep, and also via reflexes. There are several factors that influence and configure posture during sleep.
Proper maintenance of postures, body parts with the centerline of gravity, is associated with lower energy expenditure due to lower demand for antigravity muscles [5,6,7]. The muscular effort spent to maintain the different postures adopted is based on the position of the different parts of the body according to their relative weight, that is, head 6–8%; trunk, 40–46%; upper limbs, 11–14%; and lower limbs, 33–40% of the total body weight [8]. According to the assumed posture, there is a change in the internal pressure of the intervertebral discs [9].
Changes in body posture are one of the problems often faced by young people, adults, and older ones. In this context, the prophylactic approach of a postural reeducation with an intervention in the posture aims to minimize the effects of the degenerative process and the mechanical overload caused by the continued bad posture in all day and also night periods [10].
A posture is called “bad, poor” when it is ineffective, when it does not reach its intended purpose or when a great muscular force is used to maintain it, consuming more energy than it should [5]. A poor posture can result in pain due to mechanical overload for a prolonged period (i.e., sleep), adaptive shortening of soft tissues, and consequent muscle weakness [11]. Mechanical stresses, such as those imposed by postures outside the anatomical alignment for a prolonged period, lead to an increase in the production of fibroblasts and collagen, with the loss of the need for tissues such as muscles and soft tissues [12]. When the posture is maintained statically for a long time, that is, with isometric and repetitive contractions, the phases of muscle relaxation become noticeably short, promoting muscle fatigue that can translate into a sensation of discomfort or pain [13] (Fig. 1).

Illustration of ineffective postures, with a mechanical overload of joints and muscles. (Image courtesy from Dr. Silmara Bueno.)
In the biomechanics of the spine, aspects such as length, strength, endurance, and muscle coordination are involved, maintaining the balance between them. The lack of application of healthy biomechanics to the spine during sleep is associated with a decrease in range of motion, changes in alignment, and normal control in kinesthetic perception due to inadequate postural habits, maintained for a prolonged period. Among the lengths associated with postural dysfunctions, the decrease in range of motion due to changes in flexibility, pain, and increased muscle tension due to overload stands out. In addition, there is a decrease in strength and resistance leading to muscle fatigue due to the postures adopted or due to disuse and inadequate trunk stabilization [11, 14]. The increase in static, repetitive, and excessive resistance increases the risk of inflammatory or degenerative processes that affect the skeletal muscle system [14].
Postural assessment at bedtime makes it possible to assess imbalances to restructure posture through ideal support for the entire skeletal muscle system. The pelvic area of the human body is broader and heavier than other body parts. The thoracic area, because of the presence of the lungs is wider but not heavier. When lying in a lateral decubitus for sleep, on a very firm mattress, there is unsuitable spinal support, as only the broader areas of the body are supported (e.g. pelvis and shoulder). When these forces are not respected, ischemia may appear in body regions that are in contact with the surface. Ischemia generates metabolic substances (which will stimulate the nerve extremities and lead to discomfort and pain in lumbar and neck regions. The continuity of this factor can cause chronic muscular pain in the neck spine [15, 16]. Postural discomfort due to continuous muscle contraction can decrease blood supply, increase tension (stretching tight), or ligament compression, usually leading the individual to change the posture. Different studies have shown the association of microtrauma with pain and functional disability caused by poor posture during sleep [14, 17,18,19], highlighting the importance to have ideal support for the body and a correct and aligned posture.
The adopted posture for sleeping is something incredibly unique and particular. We move more than 10 times during sleep, this tends to decrease with age, and most of the time we are unable to remember the position in which we fall asleep or wake up. The body requires a position according to the degree of comfort and habit, so the body tends to adapt during a change in the musculoskeletal system.
2 Mattress: Alignment of the Body
In comparison about the mattress, custom-made surface, firm, and soft matters showed that the custom-made matters have maintained the natural alignment of the spine, arranged with different stiffness zones (Fig. 2a).

Alignment of the spine on custom-made (a), firm (b), and soft (c), surfaces. (Reprinted with permission from Leilnahari et al. [20])
In the firm matters, the spine has bent down in the lumbar area, as only the shoulder and pelvis received good support on these surfaces (Fig. 2b). The softness of the soft mattress caused the pelvic area to sag more into the mattress, while the position of the vertebra C7 on soft surfaces is higher than that of the pelvis, due to the relatively lower mass of the upper part of the body (Fig. 2c) [20]. Therefore, the custom-made mattress allowed the neutral alignment of the spine, close to the natural standing position.
In the supine position, the center of gravity is a result of all segmental centers of gravity in relation to weight, having as many centers of gravity as there are positions to be adopted. The individual is in stable balance in the supine position when the line drawn from their centers of gravity coincides with the base of support [21].
The most common sleeping position in adults is the lateral decubitus (57%) [22], most likely due to the increased support of the spinal structures [23], followed by the supine position (17%) and the prone position (11%), despite this last one not being indicated for sleep. The other postures are variations of the positions in which the individual lies down to sleep [24]. The supine and the lateral decubitus are the sleeping postures most indicated, as they allow greater comfort and efficiency [25]. Yet, both positions require the use of two pillows (or a bigger one): one supporting the head and the other, below or between the knees (Fig. 3). The supine position allows the alignment of the spine with the use of pillows, cushions, and supports. For this case, it is recommended to use a pillow for the head and another pillow under the knees to align the pelvis.

Supine position with roll under the knees to protect the lumbar region, hips, and knees; and lateral decubitus with supported contour-shaped body pillow. (Image courtesy from Dr. Silmara Bueno.)
3 Pillows: Neck Support
When sleeping in the prone position, the head is usually turned to the side, which increases the rotation of the neck. This rotation is up to 90° and flexion of 10°–20° of the neck, with negative repercussions on muscular structures, nerves, vessels, ligaments, and other segments. This posture constitutes a potential source of neck pain, fatigue, muscle tension, tension headache, and pain in the temporomandibular joint [11]. Consequently, there is an increase in spinal load, because several facet joints of the most cranial vertebra are compressed on the ipsilateral side, while the contralateral ligaments will be under tension and stretching. Blood vessels can also be compressed, causing headaches, dizziness, and other disorders [1]. Despite all the disadvantages, many people prefer the prone position. It is therefore advisable to improve the alignment of the spine by placing a pillow, under the shoulder and the ribcage next to which the head is facing, or by raising your arm from that side, or even by placing a pillow under the belly to restore lumbar lordosis. The same alignment of an eventual hyperlordosis can be achieved by raising the knee and the hip next to which the head is rotated, or by placing a pillow under the hip and knee on this side. In fact, most of the aforementioned corrections implement a slight change of position to an almost lateral position [1].
Inadequate posture of the head when sleeping imposes a considerable consumption of muscle energy in the neck region. Poor neck posture during sleep, increase biomechanical stresses on neck spine structures, producing neck pain and stiffness, headache, and scapular or arm pain, resulting in low-quality sleep [26]. A suitable pillow is a proper support for neck lordosis [27]. Choosing an adequate pillow can reduce pain and improve sleep quality [28]. The big question is: “How is the suitable pillow? How do I chose one? Where do we have it on the market?” There is still no consensus regarding the best type of material for pillows, or their shapes and heights, which are still under debate in the literature (Fig. 4).

Different materials with different supports for pillows. (Image courtesy from Dr. Silmara Bueno.)
The main role of a pillow during sleep is to support the neck spine in a neutral position. A neutral position of the spine prevents loss of neck spine curvature and neck waking symptoms by minimizing end-range positioning of spinal segments [23, 29]. In addition, proper support can increase the contact area between the neck and the pillow so the pressure exerted upon the muscles can be evenly distributed [30]. Modifications of the neck inclination from 10 to 15 degrees alter muscle activity and blood supply in the region [31]. During the neck flexion, the horizontal distance between the center of gravity of the head and the axis joint at the atlanto-occipital joint increases considerably. The contraction of the scapular elevator muscles, with repercussions on the brachial plexus, is expressed by symptoms of pain, tingling, and decreased strength of the upper limbs [31]. Likewise, such manifestations can be observed when lying down, maintaining the prolonged positioning of the neck in semi-flexion.
Neck and spine pain as a whole has been described as one of the factors that can interfere with sleep quality. Pain and discomfort were related to higher and longer electromyographic (EMG) activities of trapezius in participants who have neck and shoulder pain. However, the relation of comfort and EMG activity of the neck and upper trunk during lateral sleeping position in different pillow heights is still a gap in the literature [32].
We already know that many people might not fall asleep when the neck was stiff and shoulder muscles were not relaxed. In addition, we should use props to relax the joints and loosen stiff muscles having proper support [33].
Pillow temperature must also be taken into consideration. A pillow that helps reduce core and head temperatures during nighttime sleep has been shown to be important for deep sleep (slow wave sleep) [34]. The reason individuals using a pillow made of a material that helps the pillow surface stay cool could fall asleep more easily and sleep well is strongly related to the lowered core and head temperatures and slowed heart rate [35]. Moreover, a pillow designed to reduce the temperature of the head can reduce sweating and whole-body temperature, and indirectly improve sleep quality [36].
An investigation on the effects of three types of pillows with different contents on neck lordosis, pillow temperature, and pillow comfort was conducted [37]. The three pillows were made of different materials: the orthopedic pillow (a roll-shaped pillow containing multiple polypropylene capsules), the memory foam pillow (contoured pillow consisting of polyurethane foam), and the feather pillow (regularly shaped pillow filled with 100% goose feathers). The Cobb angle from C2-C7 of the participants was measured from a radiograph, and when comparing the pre-Cobb angle in a standing position and the post-Cobb angle in a supine position with the use of the three different pillows, the researches found that the angle was significantly increased with the orthopedic pillow, from −3.83° at baseline to 7.70° (Fig. 5). The memory foam pillow increased the Cobb angle from −3.83° to −0.33°, and the feather pillow decreased the Cobb angle from −3.83° to −6.20°, but with no statistically significant differences (that might be because of the small sample size). The variations in pillow temperature were measured using an infrared thermometer, and the temperatures of each of the three pillows increased significantly after 20 minutes of lying on the pillows. However, the degree of temperature increase was significantly lower for the orthopedic pillow (1.53 °C) than for the memory foam (3.13 °C) and feather pillows. The orthopedic pillow was also considered the most comfortable one by the participants [37].

Measurement of the Cobb angle in a standing position (a) and a supine position with an orthopedic pillow (b). (Reprinted with permission from Jeon et al. [37])
In another investigation, neck pain and quality of sleep were tested with six different pillows [38]. The participants tested all the pillows in a random order over the course of 3 weeks. Pillows with firm support for neck lordosis could be recommended for the management of neck pain and improvement of sleep quality [38].
The use of the wrong type of pillow can compromise pain-sensitive structures and produce waking symptoms, such as neck pain and stiffness, headache, and arm pain leading to low sleep quality. The height of the pillow affects the comfort and quality of sleep and was identified as one of the factors that influence the alignment of the neck spine [39, 40]. It is believed that using an “ideal” pillow for adequate neck support to maintain neck lordosis while sleeping can lead to high-quality sleep [30]. However, many people make poor choices of pillows, which leads to the adoption of bad postures of the neck during sleep, resulting in biomechanical stress [26]. The pillow intends to avoid the discomfort caused by the posture adopted when sleeping, promoting the alignment of the axial skeleton in any decubitus, and supports the skeletal muscle system, being considered compensating support [41].
The traditional dimension of the pillow used in many countries is 50 × 70cm, with a height of 10–18 cm. In order to make them soft and comfortable, they can be made in different materials, (e.g., feathers, polyurethane flakes, polyester fiber, viscoelastic, latex, and others), and in different formats (e.g., the traditional rectangular ones, format of soap, triangular and ergonomic ones). The pillow should adjust to the different decubitus positions adopted during sleep. For instance, in the supine position, if the height of the pillow is too high, it will cause flexion of the neck. Similarly, if the height of the pillow is too low, there is hyperextension of the neck. Both can impair respiratory function during sleep, increase muscle activity, and generate pain.
The EMG activity of the neck and mid-upper back of asymptomatic adults using foam pillows of three different heights (5, 10, and 14 cm) was evaluated by a group of Brazilian researchers [42]. The 10 cm pillow foam elicited the lowest EMG activity of the middle trapezius in lateral decubitus and was considered by the participants the most comfortable one [42]. A study conducted with participants with a high variation in height, from 155 to 180 cm, found the intermediate pillow height of 10 cm as an ideal [34], as other investigations also have proposed [30]. Indeed, the ideal height for each person is a fundamental aspect of pillow use. This is a product that needs to be designed specifically for a population according to their anthropometry.
4 Positional Therapy for Sleep Apnea
A sleep-positioning pillow can heltp to resolve or resolve positional obstructive sleep apnea (OSA) in some cases. It is a simple accessory, many times used toghether with PAP therapy, deserving consideration as an alternative or complementary treatment. Please refer to Chapter “Obstructive Sleep Apnea: Physiotherapeutic Approach” for more on sleep position for OSA, and for pictures of devices for positional therapy, such as chest belts, inflatable dampers and tennis ball technique.
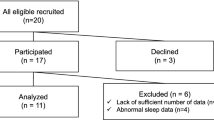
Only four studies up to now investigated the use of different sleep positioning pillows in patients with OSA, two of them using objective parameters. The effect of the positional pillow (Fig. 6a) was investigated using objective measures derived from polysomnography on both respiratory variables and sleep architecture (baseline, consecutive treatment response at 1 and 6 months, and follow-up polysomnography) along with questionnaires to identify sleepiness, fatigue, and sleep quality [43]. The satisfaction of both participants and bed partnerers was assessed. The use of the positional pillow statistically significantly reduced supine position, sleep fragmentation, apnea-hypopnea index, respiratory disturbance index, and oxygen desaturation, both at 1 and 6 months. Sleepiness and fatigue also showed reductions and sleep quality improved in all-time points [43].

Different types of sleep positioning pillows for obstructive sleep apnea. (a) Visual aspect of the pillow’s external cotton cover; observable underlying foam structure beneath illustrated velvet cover; subject’s head and neck placement in lateral position; (b) pillow that only adjusts the head and neck in lateral decubitus with an arm space; (c) polyurethane head positioning pillow. (Modified with permission from Newell et al. [43])
There was a significant reduction in respiratory disturbance index, hypoxemia, and snoring after one night with a triangular pillow in participants with mild to moderate OSA (Fig. 6b) [44]. Therefore, we must be aware of shoulder pain when using this pillow. One night of positional therapy with a head-positioning pillow (Fig. 6c) in a sample of post-stroke patients showed a significant reduction of supine position and AHI, having an acceptable adherence following 3 months [45].
In addition, the head positioning pillow for 2 consecutive nights in mild to moderate positional OSA patients showed significant reductions of subjective and objective snoring severity in normal-weight patients, in contrast to overweight patients where only a reduction in subjective snoring was shown [46].
Positional therapy may therefore present as a valuable first-time intervention in positional OSA. Individualized care for positional OSA treatment by determining who will benefit from positional therapy alone or as an adjunct therapy is still needed, as well as guidelines on the theme.
5 Final Words
Material properties of a sleep system should be adjusted to personal needs in an objective way and preferences, for the reason that they are the underlying determinants of most physical ergonomic features (e.g., spine support). For example, obese patients need a firmer mattress in order to prevent the pelvic girdle from dropping too deep into the mattress. Materials therefore must be developed and combined to optimize general sleep system characteristics. Here, we point out a new avenue for research and increase the interest for the physical therapist to be evolved in positioning for better sleep.
References
Haex B. Back and bed. Ergonomic aspect of sleeping. 2nd ed. New York: CRC Press; 2004.
Huysmans T, et al. A 3D active shape model for the evaluation of the alignment of the spine during sleeping. Gait Posture. 2006;24(1):54–61.
Sakata RK, Issy AM, Vlainich R. Cervicobraquialgias. Rev Faces Dor. 2002;2:5–6.
Grandjean E, Manual de ergonomia: adaptando o trabalho ao homem. Stein, João Pedro 4a ed. 1998, Porto Alegre: Artes Médicas.
Gardiner MD. Manual de terapia por exercícios. São Paulo: Santos; 1995.
Kendall FP, McCreary EK, Provance PG. Músculos: provas e funções. 4th ed. Manole: São Paulo; 1995.
Smith LK, Weiss EL, Lehmkuhl LD. Cinesiologia clínica de Brunnstrom. 5th ed. São Paulo: Manole; 1997.
Iida I. Ergonomia: projeto e produção. São Paulo: Edgar Blucher; 1990.
Nachemson AL. The lumbar spine: an orthopedic challenge. Spine. 1976;1(1):59–71.
Almeida GCD. Efeitos de uma intervenção postural durante o sono na percepção da dor na coluna vertebral, na qualidade de vida e na qualidade do sono. In: Faculdade de Motricidade Humana. Lisboa: Universidade de Lisboa, FMH/FL; 2015. p. 244.
Kisner C, Colby LA. Exercícios terapêuticos: fundamentos e técnicas. 3rd ed. São Paulo: Manole; 1995.
Oliver J, Middleditch A. Anatomia funcional da coluna vertebral. Rio de Janeiro: Revinter; 1998.
Chaffin DB, Anderson GB, Martin BJ. Biomecânica ocupacional. Belo Horizonte: Ergo; 2001.
Grandjean E, Hunting W. Ergonomics of posture--review of various problems of standing and sitting posture. Appl Ergon. 1977;8(3):135–40.
Haex B. Back and bed: ergonomic aspects of sleeping. Reino Unido: CRC Press; 2005.
Yim JE. Optimal pillow conditions for high-quality sleep: a theoretical review. Indian J Sci Technol. 2015;8(5):135–9.
Bork BE, et al. Work-related musculoskeletal disorders among physical therapists. Phys Ther. 1996;76(8):827–35.
Cromie JE, Robertson VJ, Best MO. Work-related musculoskeletal disorders in physical therapists: prevalence, severity, risks, and responses. Phys Ther. 2000;80(4):336–51.
Mierzejewski M, Kumar S. Prevalence of low back pain among physical therapists in Edmonton. Canada Disabil Rehabil. 1997;19(8):309–17.
Leilnahari K, et al. Spine alignment in men during lateral sleep position: experimental study and modeling. Biomed Eng Online. 2011;10:103.
Bienfait M. Os desequilíbrios estáticos: fisiologia, patologia e tratamento fisioterápico. 2nd ed. São Paulo: Summus; 1995.
De Koninck J, Lorrain D, Gagnon P. Sleep positions and position shifts in five age groups: an ontogenetic picture. Sleep. 1992;15(2):143–9.
Gordon SJ, Grimmer-Somers KA, Trott PH. A randomized, comparative trial: does pillow type alter cervico-thoracic spinal posture when side lying? J Multidiscip Healthc. 2011;4:321–7.
Santiago R. Para uma noite bem dormida. Cited 2018 December 4th, 2018. http://ruisantiago.com/Docs/dormir.pdf.
Locks RT, Merino GSAD, Merino EAD. Levantamento e identificação dos aspectos básicos para a correta escolha do travesseiro de fibra. Blucher Design Proc. 2014;1(4):2331–43.
Gordon SJ, Grimmer-Somers KA, Trott PH. Pillow use: the behavior of cervical stiffness, headache and scapular/arm pain. J Pain Res. 2010;3:137–45.
Ambrogio N, et al. A comparison of three types of neck support in fibromyalgia patients. Arthritis Care Res. 1998;11(5):405–10.
Lavin RA, Pappagallo M, Kuhlemeier KV. Cervical pain: a comparison of three pillows. Arch Phys Med Rehabil. 1997;78(2):193–8.
Mc DJ. Sleep posture; its implications. Br J Phys Med. 1946;9:46–52.
Chen HL, Cai D. Body dimension measurements for pillow design for Taiwanese. Work. 2012;41 Suppl 1:1288–95.
Mercúrio R. Dor nas costas nunca mais. São Paulo: Manole; 1997.
Mork PJ, Westgaard RH. The association between nocturnal trapezius muscle activity and shoulder and neck pain. Eur J Appl Physiol. 2004;92(1–2):18–25.
Hannon JC. Pillow talk: the use of props to encourage repose. J Bodyw Mov Ther. 1999;3(1):55–64.
Liu SF, Lee YL, Liang JC. Shape design of an optimal comfortable pillow based on the analytic hierarchy process method. J Chiropr Med. 2011;10(4):229–39.
Kawabata A, Tokura H. Effects of two kinds of pillow on thermoregulatory responses during night sleep. Appl Human Sci. 1996;15(4):155–9.
Okamoto-Mizuno K, Tsuzuki K, Mizuno K. Effects of head cooling on human sleep stages and body temperature. Int J Biometeorol. 2003;48(2):98–102.
Jeon MY, et al. Improving the quality of sleep with an optimal pillow: a randomized, comparative study. Tohoku J Exp Med. 2014;233(3):183–8.
Persson L, Moritz U. Neck support pillows: a comparative study. J Manipulative Physiol Ther. 1998;21(4):237–40.
Her JG, et al. Development and comparative evaluation of new shapes of pillows. J Phys Ther Sci. 2014;26(3):377–80.
Verhaert V. Ergonomic analysis of integrated bed measurements: towards smart sleep systems. Lovaina: Universidade Católica de Leuven; 2011. p. 210.
Hage M. Dor nas costas: deixe de reclamar e resolve de uma vez. São Paulo: Gente Editora; 1997.
Sacco IC, et al. The effect of pillow height on muscle activity of the neck and mid-upper back and patient perception of comfort. J Manipulative Physiol Ther. 2015;38(6):375–81.
Newell J, Mairesse O, Neu D. Can positional therapy be simple, effective and well tolerated all together? A prospective study on treatment response and compliance in positional sleep apnea with a positioning pillow. Sleep Breath. 2018;22(4):1143–51.
Zuberi NA, Rekab K, Nguyen HV. Sleep apnea avoidance pillow effects on obstructive sleep apnea syndrome and snoring. Sleep Breath. 2004;8(4):201–7.
Svatikova A, et al. Positional therapy in ischemic stroke patients with obstructive sleep apnea. Sleep Med. 2011;12(3):262–6.
Chen WC, et al. Treatment of snoring with positional therapy in patients with positional obstructive sleep apnea syndrome. Sci Rep. 2015;5:18188.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Bueno, S., Frange, C. (2022). Sleep Ergonomics. In: Frange, C., Coelho, F.M.S. (eds) Sleep Medicine and Physical Therapy. Springer, Cham. https://doi.org/10.1007/978-3-030-85074-6_32
Download citation
DOI: https://doi.org/10.1007/978-3-030-85074-6_32
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-85073-9
Online ISBN: 978-3-030-85074-6
eBook Packages: MedicineMedicine (R0)