
Abstract
The 2006 Chicago Consensus Statement heralded a new era in the approach to managing disorders of sex development which has come to include a complex group of patients in whom there has been much controversy as to terminologies and management strategies. It comprises a spectrum of disorders with protean manifestations characterized by atypical development of chromosomes, gonads, or phenotypic sex. Previous terminologies such as “indeterminate sex,” “ambiguous genitalia,” “hermaphroditism,” “pseudohermaphroditism,” or “intersex” are no longer in use.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Disorders of Sex Development (DSD)
- Ambiguous genitalia
- Gonads
- Genitoplasty
- Intersex
- Anomalies of genital development
- Congenital adrenal hyperplasia
- Severe hypospadias
Disorders of Sex Development (DSD) represents a complex congenital condition with atypical development of chromosomes, gonads, or anatomic sex. Much controversy and debate have transpired between professionals and the non-medical community however this exists in a sea of many unknowns, one of them being the long-term consequences of no intervention. The current approach is founded on a multidisciplinary team decision-making process involving the family, supported by psychology. Although the 2006 consensus statement makes an attempt to simplify and be inclusive, the current approach is to individualize care to the patient and family in conjunction with all the psychological, cultural, and social aspects rather than to categorize them.
1 Embryology
From 6 weeks, early bipotential gonads develop within the genital ridge from primordial germ cells (Fig. 40.1).

Embryology of sex development
2 Clinical Features
The spectrum broadly and simplistically includes either an undervirilized male or an overvirilized female. However, that is far from complete and the following table makes an attempt to be comprehensive (Table 40.1).
The newborn period raises much anxiety, uncertainty, and social pressures in parents, especially in the presence of ambiguous genitalia. It is critical that life-threatening conditions like salt-wasting congenital adrenal hyperplasia (CAH) are immediately evaluated and information gathered to facilitate gender assignment. Subsequent management should proceed in a logical and timely manner in a specialized center with multidisciplinary input. Guessing the sex and usage of “he” and “she” should be avoided, with phrases such as “your baby” being more appropriate.
A complete clinical history (maternal, fetal, and family) and examination is important. Particular points to be noted when examining include:
-
Presence/absence of a palpable gonad on either side- position and size.
-
Phallic appearance including length, width, and presence of chordee.
-
Appearance of scrotum/labio-scrotal folds, degree of skin rugosity/pigmentation.
-
Location of external urethral opening and number of orifices present on the perineum; position of the anal margin.
-
Dysmorphic/syndromic features.
Some children will only present later in life such as complete sex reversal (Swyer syndrome) who look unequivocally female (XY, complete gonadal dysgenesis), but who are unable to develop secondary sexual characteristics or menstruate.
In general, symmetrical genital appearance suggests a biochemical etiology (e.g., congenital adrenal hyperplasia (CAH)), whereas asymmetrical appearance implies a chromosomal abnormality (e.g., 45x0/46XY).
3 Investigations
The following investigations may be required and each patient should be individualized:
-
1.
Genetic—karyotype and specific gene arrays.
-
2.
Endocrine—blood and urine biochemistry, hormone assays.
-
3.
Imaging—ultrasound (renal/pelvic), contrast studies (cystogram/genitogram), and MRI.
-
4.
Surgical—cystovaginoscopy, laparoscopy, and skin/gonadal biopsies.
4 Principles of Management
The ESPU-SPU Consensus statement 2020 outlines “a one size fits all” approach does not exist for DSD patients. It recommends an individualized non-mandated management taking into account all medical, psychological, social, and cultural considerations of the patient and their parents and caregivers.
Medical Management
-
Electrolyte balance maintenance (salt losing CAH)
-
Hormone replacement or supplementation if needed
-
Corticosteroid therapy (CAH)
-
Spironolactone for acne/hirsutism
-
Oral contraceptive pills (OCP) for menstrual irregularities (CAH)
Medical noncompliance with corticosteroid therapy can cause increasing clitoromegaly, virilization, and short stature due to premature epiphyseal plate closure in 46XX CAH patients.
Surgical Management
Currently, there are ongoing contentious debates from various medical and non-medical groups regarding the optimal management of DSD patients particularly regarding surgical intervention. The ethics behind the surgical decision-making, the timing of surgical intervention, and the functional and cosmetic outcomes that can be expected or have been reported are evolving and under discussion. However, the general surgical principles would include:
-
Emergency—to create outlets for urine/stool
-
Elective
-
Diagnostic investigations: EUA, cystourethroscopy, vaginoscopy, laparoscopy, gonadal biopsy
-
Gonadal Surgery- to reduce the risk of gonadal tumors (streak gonads and Y material)
-
Genital Surgery
-
Masculinizing surgery: Hypospadias repair, chordee correction, orchidopexy, scrotoplasty, excision of Mullerian structures
-
Feminizing Surgery: Vaginoplasty, labioplasty, introitoplasty, clitoroplasty
-
-
Psycho-Social Management
-
Genetic counseling regarding future pregnancies
-
Psychological support for family and patient
Congenital Adrenal Hyperplasia—Usually 21-Hydroxylase Deficiency.
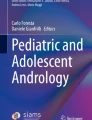
This is the most common type. Infants present with ambiguous genitalia and bilateral impalpable gonads (Fig. 40.2b). It can be life-threatening due to salt-losing nature (75%) with ↓ aldosterone.
-
Urgent karyotype—46XX.(CAH can occur in 46XY but genitalia are usually not ambiguous).
-
Steroid profile—↑ 17-hydroxy progesterone ↑ androstenedione levels.
-
46XX CAH babies have clitoromegaly, scrotalization of labio-scrotal folds, and a urogenital sinus. 46XY CAH in most have a normal male phenotype.
-
Medical Management with corticosteroid therapy. Feminizing surgery has become more conservative due to better medical management in terms of clitoral size however timing and outcomes of urogenital sinus surgery is still controversial and debated.

(a) 46, XY DSD (severe hypospadias and impalpable testes). (b) 46, XX DSD (congenital adrenal hyperplasia)
5 Gender Assignment
It is important to avoid guessing the sex and using terms “he” or “she.” Phrases such as “your baby” are more appropriate. Birth is not registered until the final decision has been made, as the reversal process is complex (42 days are allowed to register a birth in the UK except Scotland which is 21 days). Wherever possible, gender is assigned according to karyotype, rather than being reassigned to suit the initial appearances of the external genitalia, although this may not always be possible.
An experienced multidisciplinary clinical team should undertake the decision-making of the gender assignment with full involvement of the parents and the child if appropriate. The important factors to be considered during the assignment are: expected gender identity, sexual function, fertility potential, and the psychosocial development of the child.
6 Long-Term Outcomes
-
Data on the long-term outcome of surgery for DSD conditions are sparse.
-
There are no controlled trials comparing early vs. late surgery and no data exist for the long-term outcome of newer techniques in feminizing genitoplasty, such as total or partial urogenital mobilization and nerve-sparing or corporal-sparing clitoral reduction or clitoroplasty.
-
Retrospective reviews suggest that there is much dissatisfaction with the results of surgery performed in the past with regard to cosmetic appearance and function, but this is very difficult to quantify as there is a significant underestimation of the denominator.
-
In the current climate of minimal or no intervention what remains to be clarified is the long-term outcome of such an approach. Although there are islands of understanding, it is still in a sea of unknowns. Prospective evaluation over birth to adulthood is recommended for all. Several countries have now started registries to recruit patients and document outcomes which will be invaluable in the future.
Further Reading
Lee PA, Houk CP, Hughes IA, Ahmed SF, Houk C, et al. Consensus statement on management of intersex disorders. Pediatrics. 2006;118:e488–500. https://doi.org/10.1136/adc.2006.098319.
Mouriquand P, Caldamone A, Malone P, Frank J, Hoebeke P. The ESPU/SPU standpoint on the surgical management of sex development (DSD). J Pediatr Urol. 2014;10(1):8–10. https://doi.org/10.1016/j.jpurol.2013.10.023.
ESPU-SPU Consensus statement 2020: Management of differences of sex development (DSD) [Online] https://www.espu.org/members/documents/383-espu-spu-consensus-statement-2020-management-of-differences-of-sex-development-dsd
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Kumar, N., Cherian, A. (2022). Disorders of Sex Development. In: Sinha, C.K., Davenport, M. (eds) Handbook of Pediatric Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-84467-7_40
Download citation
DOI: https://doi.org/10.1007/978-3-030-84467-7_40
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-84466-0
Online ISBN: 978-3-030-84467-7
eBook Packages: MedicineMedicine (R0)