
Abstract
Ultrasound can be employed to facilitate central and peripheral vascular access. In some cases, such as internal jugular vein cannulation, the use of ultrasound makes the procedure faster and safer, while limiting the number of attempts. In other cases, such as subclavian vein cannulation, the role of ultrasound in facilitating the procedure is less clear. Additionally, ultrasound can be utilized to confirm proper guidewire placement in the right atrium prior to central venous cannulation and aid in the placement of pulmonary artery catheters. While ultrasound has not yet been proven to decrease the time to placement of pulmonary artery catheters or reduce complications secondary to placement, it does facilitate real-time guidance and final positioning.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Internal jugular vein cannulation
- Subclavian vein cannulation
- Femoral vein cannulation
- Arterial cannulation
- Central venous catheter
- Pulmonary arterial catheter
Introduction
Proper vascular access is imperative for appropriate perioperative care and includes the use of peripheral venous access for fluid and drug administration, central venous access for vasoactive infusion and central venous pressure (CVP) monitoring, and lastly, arterial access for continuous blood pressure monitoring and arterial blood sampling. The indications of each type of access are outside of the scope of this text; however, the utility of ultrasound for obtaining vascular access will be discussed. Ultrasound imaging during vascular procedures can be used to “scout” the anatomy prior to skin puncture, provide needle guidance towards the intended structure, as well as confirm wire placement during the Seldinger technique. The intention of ultrasound imaging is often to reduce complications, reduce the time to vascular access, and aid in difficult cannulations; however, the magnitude of this benefit may vary depending upon the vessel selected and the patient’s individual anatomy.
Probe Orientation
Unlike the standard orientations found in echocardiography, ultrasound for vascular access can have varying probe and image orientations based on the vessel being cannulated and the operator’s position. In general, it is recommended that the probe be oriented to display the same anatomy on the screen that would be visible to the operator from that vantage point. Thus, anatomic structures on the left side of the probe should appear on the left side of the screen, and right-sided structures should appear on the right side of the screen. Although it is common for ultrasound probes to have an indicator that denotes one side of the probe that correlates with a specific side of the screen, the user can also briefly confirm anatomic and screen orientation alignment by moving the probe left to right or by applying gentle external pressure on one side of the probe confirming correlation with the image on the screen.
Ultrasound may be used for vascular access both in the long (in-plane) axis (LAX) and in the short (out-of-plane) axis (SAX). Both views may be utilized to guide needle movement; however, the in-plane technique serves to keep the entire needle length in view while the out-of-plane technique catches a cross section of the needle. The advantage that an out-of-plane technique has over an in-plane technique is the ability to visualize surrounding structures during needle movement (e.g., carotid artery during internal jugular cannulation) , and the imaging plane can be moved to follow the trajectory of the needle. Oblique views can also be obtained but are not conventionally used and are not addressed further here.
In the SAX view, the probe is placed perpendicular to the desired vessel, providing a cross section of the vessel and needle, which appears as a hyperechoic point (Fig. 23.1; Videos 23.1a, b). In the LAX view, the probe is placed parallel to the desired vessel, providing an image that shows the course of the vessel across the screen and the needle shaft as it is advanced (Fig. 23.2; Videos 23.2a, b). Again, the advantage of the SAX view is that it provides superior visualization of anatomic structures surrounding the vessel of interest. This advantage can be critical because ultrasound is often used to access central veins that run in close proximity to critical arteries. It appears that for novice users, the SAX view also results in faster cannulation times and is perceived to be an easier approach by the operator [1]. The LAX view provides the advantage of better visualization of the needle itself during its approach to and its course within the vessel. However, maintaining proper alignment of both the ultrasound transducer and the access needle can be challenging. Any malalignment results in the cannulating needle not being imaged and may lead to unsuccessful cannulation or inadvertent damage to surrounding structures.

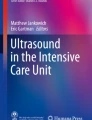
Out-of-plane or short-axis (SAX) imaging of the right internal jugular vein (green arrow). The yellow arrow indicates the carotid artery just to the medial aspect of the larger, collapsible internal jugular vein

In-plane or long-axis (LAX) imaging of the right internal jugular vein (green arrow) from the same patient in Fig. 23.1
Vessel Selection
There are a number of factors involved in selecting the site for vessel cannulation. Anatomic considerations, patient positioning, patient tolerance, venous drainage and vessel patency, and relative rates of complications should all be considered for arterial, peripheral, or central venous cannulation. In general, larger central venous catheters and those with more lumens have a higher risk for infections [2]. Subclavian central venous catheters have the lowest risk for infection (1.5–4%) and thrombosis (1.2–1.9%). Internal jugular catheters have an infection rate of 4–8% and a thrombosis rate of 7.6%. The femoral site has the highest incidence of both infection and thrombosis at 19.8% and 21.5%, respectively [3, 4].
Vessel Identification
Differentiation of veins from arteries is a critical aspect of the appropriate use of ultrasound for obtaining vascular access. Both have anechoic (black) lumens, but arteries generally have thicker walls that are more hyperechoic (white) than the walls of veins. Additionally, arteries are typically pulsatile and the higher pressure makes them less compressible than veins (though a completely noncompressible vessel suggests thrombosis).
With the vessel viewed in the short axis, as gentle pressure is applied, veins will compress, while nearby arteries should remain patent and pulsatile. However, with excessive pressure both arteries and veins can collapse. Color flow Doppler imaging may also be used to identify pulsatile flow (Figs. 23.3 and 23.4; Videos 23.3 and 23.4). Venous blood flow will be more uniform in color, have lower velocity, and may be present during systole and diastole, whereas arterial flow will be of higher velocity and detected predominantly during systole. The Doppler scale can be lowered and the color gain increased to detect flow if not initially observed. In addition, the probe should be oriented so that flow is toward or away from the transducer in order to register a Doppler signal. Flow perpendicular to the probe will not demonstrate a Doppler shift (see Chap. 4).

Out-of-plane imaging (SAX view) of the right internal jugular vein (green arrow) with color flow Doppler. The yellow arrow indicates the carotid artery. Color flow Doppler imaging demonstrates faster pulsatile laminar flow in the carotid artery, with slower flow in the jugular vein

In-plane imaging (LAX view) of the right internal jugular vein (green arrow) with color flow Doppler
Because techniques for vessel identification can be rendered less reliable in low-flow states or cardiac arrest, it is crucial that the operator understands the normal anatomic relationships between arteries and veins surrounding the vessel selected for cannulation. Additionally, other confirmatory measures and verification of correct placement of the guidewire and/or catheter are necessary and will be covered in later sections.
Static Versus Dynamic Imaging
Static imaging uses ultrasound to identify the vessel selected for cannulation and the appropriate site of needle entry after which the ultrasound is no longer used to guide the procedure. The dynamic approach uses real-time ultrasound throughout the procedure to guide needle placement and vessel entry, either in a long-axis plane (in-plane) or with a stepwise series of movements of the short-axis imaging plane (out-of-plane). Dynamic imaging provides faster cannulation with fewer attempts, but reported complication rates for both techniques appear to be similar [5,6,7].
Performing the Procedure
Proper positioning of the patient will aid in vessel detection and in the performance of the procedure. Trendelenburg positioning during central venous cannulation of the internal jugular or subclavian veins may increase central venous pressure and thereby the size of the vessel on imaging. After identifying the appropriate vessel with ultrasound, the desired trajectory of the needle should be determined. Typically, the needle should be directed towards the middle of the vessel, which is best determined using the SAX view. If the LAX view is used, the needle should be visualized throughout its course towards and within the vessel.
The angle of approach should be such that the needle will avoid nearby structures, both during approach and in the event the needle penetrates through the posterior aspect (“backwall”) of the target vessel. Care should be taken to avoid posterior wall puncture, but having the nearby structures away from the trajectory of the needle will minimize the risk of complication in the event of accidental posterior wall puncture.
In the SAX view, the needle tip can be visualized entering the imaging plane as a hyperechoic dot appearing on the screen, often with a ring-down artifact. The imaging plane can then be moved slightly ahead of the needle tip, and the needle can be advanced again to come into the new imaging plane. This careful, stepwise approach allows for small corrections in the needle trajectory, and almost continuous visualization of the needle tip. It is important to note that if the needle is advanced through the imaging plane, a cross section of the needle will be seen as a hyperechoic dot, but the needle tip is not visualized. A stepwise progression ahead of the needle tip, with visualization of the needle entering the imaging plane, can avoid inadvertent needle tip misplacement.
As the needle reaches the edge of the target vessel, it may be seen to indent the wall of the vessel. With gentle traction on the syringe connected to the needle, a flash of blood will be seen in the syringe as the needle enters the vessel. After placement of the guidewire, ultrasound can be used in both SAX and LAX to confirm that the guidewire is both in the target vessel and not in surrounding vessels (Fig. 23.5a, b; Videos 23.5a, b). Other techniques to aid in confirming appropriate vessel cannulation include direct pressure transduction, manometry, blood gas analysis, visualization of the wire with transesophageal echocardiography, and fluoroscopy. With the concurrent use of transesophageal echocardiography, a midesophageal bicaval view can confirm venous placement of the wire, noting the “J” tip of the wire in the right atrium (Fig. 23.6; Video 23.6). The American Society of Echocardiography (ASE) and the Society of Cardiovascular Anesthesiologists (SCA) recommend that real-time ultrasound be used to confirm vessel cannulation. The ASE/SCA recommendation is that if the combination of SAX and LAX is not utilized for confirmation of wire placement, manometry should be used [8].

(a) Short-axis imaging of right internal jugular vein with a wire within its lumen. (b) Long-axis imaging of the right internal jugular vein with a wire noted to be within its lumen (no evidence of “backwall”). The green arrow indicates the wire within the jugular vein

Midesophageal bicaval view demonstrating the “J-tip” of the central access wire within the right atrium, confirming venous access. The green arrow indicates the “J-tip.” LA left atrium, RA right atrium
Internal Jugular Vein Cannulation
The superiority of ultrasound guidance over landmark-based techniques for internal jugular (IJ) vein cannulation has been well documented [5, 9,10,11]. The use of ultrasound improves the overall and first-pass success rate, decreases time to cannulation and rate of arterial punctures, and decreases the total number of needle advances [11]. The ASE and SCA recommend that properly trained clinicians use real-time ultrasound for IJ cannulation whenever possible [8].
Any practitioner using ultrasound for IJ venous access should be familiar with the sonographic appearance of the local anatomy. The size of the IJ can be increased (potentially improving cannulation success) with Valsalva techniques and Trendelenburg positioning. These maneuvers also decrease the risk of air entrainment in the spontaneously ventilating patient [12, 13]. There is an intimate relationship between the IJ and the carotid artery (CA) at the location where IJ cannulation is typically pursued. This relationship explains the benefit of using ultrasound for IJ cannulation. Overlap between the IJ and the CA can lead to unintentional puncture and/or cannulation of the CA due to a through-and-through puncture of the vein . Ultrasound can be used to angle the approach such that CA puncture would be avoided in the event of accidental through-and-through puncture [14, 15]. Additionally, ultrasound can be used in both SAX and LAX to visualize the guidewire in the IJ and confirm that it is not in the CA, to avoid accidental CA dilation and cannulation [16]. Real-time ultrasound imaging can also potentially decrease the risk for pneumothorax by allowing for recognition of pleural tissue.
Subclavian/Axillary Vein Cannulation
While ultrasound-guided IJ vein access provides clear complication and success rate benefits over landmark-based techniques, evidence supporting ultrasound-guided subclavian (SC) vein cannulation is evolving. There are studies, however, that document higher success rates with ultrasound-guided cannulation of the SC vein compared to landmark techniques [17,18,19]. Obese patients and others with obscured external landmarks appear to benefit the most from the use of ultrasound for SC vein cannulation [20, 21].
The ASE and SCA state that the current literature does not support the routine use of ultrasound for uncomplicated patients undergoing SC vein cannulation. However, these associations do indicate that high-risk patients may benefit from the use of ultrasound to identify vessel location and patency prior to cannulation [8].
Although the supraclavicular approach is rarely used with landmark-based techniques because of the high incidence of pneumothorax, it is being used more frequently now as ultrasound identification of supraclavicular vessels is becoming more commonplace. Nevertheless, the infraclavicular approach remains the most common technique for SC vein cannulation with both landmark and ultrasound-guided techniques.
The middle third of the clavicle is typically chosen as the site for ultrasound imaging and needle insertion. The vein and artery should be identified just below the distal half of the clavicle (Fig. 23.7; Video 23.7). A short-axis approach is usually preferred due to the difficulty of differentiating vein and artery at this location in the LAX. A more lateral approach, targeting the axillary vein after it emerges from under the clavicle may also facilitate the use of ultrasound and minimize the risk for complications [22]. Trendelenburg position does not increase relative SC vein size to the same degree as with the IJ vein and thus, supine positioning is commonly used except in the case of a spontaneously breathing patient where Trendelenburg position will reduce the risk for air embolism [23].

Short-axis imaging of the right subclavian artery and vein. The green arrow indicates the vein and the yellow arrow indicates the artery
Femoral Vein Cannulation
The benefit of ultrasound-guided femoral vein (FV) cannulation in reducing incidence of vascular-related complications to the femoral artery and FV, as well as improved first-pass and overall success rates has been established [24,25,26]. However, the evidence is insufficient to support a recommendation for routine use by the ASE and SCA, who recommend that ultrasound be used when feasible for FV cannulation to identify vessel overlap and patency [8], although other societal recommendations do support the routine use of ultrasound guidance for femoral arterial and venous cannulation [27,28,29].
Although infection and thrombosis are the most common serious complications related to femoral venous catheters, the most common complication related to the FV cannulation procedure itself is vascular injury. Of particular concern is common femoral artery puncture, which would occur when the needle is directed too laterally or when there is significant vessel overlap. The common femoral artery is typically located at the midpoint of the inguinal ligament connecting the anterior iliac spine to the pubic tubercle. The FV is located just medial to the common femoral artery, and it is this close anatomic relationship that makes the use of ultrasound-guided examination prior to cannulation beneficial (Fig. 23.8; Video 23.8).

Short-axis imaging of the left femoral artery and vein. The green arrow indicates the vein and the yellow arrow indicates the artery
Ultrasound for Arterial Access
Ultrasound can be used to guide arterial access at any site at which arterial access is typically obtained, including the radial, brachial, femoral, and dorsalis pedis arteries. The cannulation technique should not differ from the techniques used for ultrasound-guided venous access. The patient should be appropriately positioned, the orientation of the ultrasound probe and its correlation with the image on the screen should be confirmed, and measures such as a manual compression with the ultrasound probe and color flow Doppler should be taken to appropriately differentiate the target artery from surrounding vessels. Either the SAX or LAX can be used to cannulate the artery (Fig. 23.9a, b; Video 23.9a, b). The catheter can be inserted either over the needle or utilizing a guidewire.

(a) Short-axis imaging the radial artery. (b) Short-axis imaging of the same patient with color flow Doppler imaging. The yellow arrow indicates the radial artery
Use of ultrasound for radial arterial access has been demonstrated to improve both first-attempt and overall success rates and reduce time to cannulation when compared with palpation-based techniques [30,31,32]. Ultrasound can be particularly useful in patients who are obese, who have low perfusion or non-pulsatile blood flow, or who have had previous unsuccessful cannulation attempts [33]. The ASE and SCA recognize the evidence supporting the use of ultrasound to improve first-pass success rates, but do not recommend routine use of real-time ultrasound for arterial access [8], although, again, several other societies do [27,28,29].
Ultrasound for Peripheral Venous Access
Ultrasound can be used to facilitate peripheral venous cannulation, particularly in deeper veins that are not palpable or visible. There are a number of reports of successful use of ultrasound in both the SAX and LAX for peripheral venous cannulation [34, 35]. Due to the collapsibility of peripheral veins, this can often be a difficult technique to achieve. The use of a tourniquet will increase peripheral venous pressure, improving success (Fig. 23.10; Video 23.10). It may be advantageous to advance the needle under direct ultrasound visualization, past the point where the “flash” of blood returns, as this may indicate the needle tip, but not the overlying catheter, is within the vessel. If the needle tip is continuously visualized within the vessel, the risk for “backwalling” or additional vascular injury is minimized. Some societies recommend the use of ultrasound guidance for difficult peripheral venous access [28, 29].

Short-axis imaging of a left basilic peripheral vein (green arrow)
Ultrasound for Guidewire Confirmation and Pulmonary Arterial Catheter Placement
Guidewire Placement and Catheter Patency
As previously mentioned, there are multiple modalities by which a guidewire can be confirmed in the target vessel, including pressure transduction, manometry, radiography, and ultrasound. Visualization of the guidewire in the intended vessel in either the SAX or LAX view provides some evidence to the practitioner that the vessel has been appropriately accessed (Fig. 23.5; Videos 23.5a, b). However, visualization of the guidewire in the right atrium (RA) with either transesophageal echocardiography (TEE) (Fig. 23.6; Video 23.6) or transthoracic echocardiography (TTE) (Fig. 23.11; Video 23.11) further confirms proper venous placement of the guidewire prior to central venous catheter (CVC) placement. TTE or TEE can also be used to confirm patency of either a peripheral venous catheter or CVC via the presence of agitated saline in the right atrium or right ventricle shortly after injection (Fig. 23.12). While only two TTE views – a modified subcostal and parasternal RV inflow – have been provided as examples in this chapter, a number of other TTE and TEE views can be used to either confirm guidewire placement or catheter patency.

Modified subcostal four-chamber view. A guidewire is visible in the right atrium (red arrow)

Modified parasternal long-axis RV inflow view showing agitated saline in the right atrium (RA) and right ventricle (RV). In comparison, the left ventricle (LV), which is located in the far field, lacks agitated saline (Reproduced with permission from Fretwell et al. [39])
Finally, TTE or more commonly TEE, is frequently utilized in the operating room to confirm guidewire placement in the lumen of the central arterial system prior to arterial stent placement, femoral cannulation, or intra-aortic balloon pump insertion (Fig. 23.13; Video 23.12). A view of the descending aorta can be obtained by rotating the probe to the left from the midesophageal position. The distal and proximal descending aorta can then be interrogated in either the SAX or LAX view by advancing and withdrawing the probe, respectively.

Descending aorta short-axis view (depth reduced) with the distal tip of an intra-aortic balloon pump (red arrow) in the lumen of the aorta
Pulmonary Arterial Catheter Placement with Ultrasound
Pulmonary arterial catheters (PACs) have traditionally been placed using pressure waveform tracings and length-insertion norms. With the increasing utilization of ultrasound (i.e., TTE and TEE) in the perioperative period, it is not surprising that ultrasound has also been integrated into this procedure. While it was theorized that ultrasound guidance would increase success rates, decrease the time to placement, and decrease associated complications, this has not been confirmed. However, TEE-guided placement did result in greater precision in the final location of the catheter in a study completed by the authors [36]. The authors contend that positioning the distal PAC in the proximal right pulmonary artery may reduce the incidence of pulmonary artery damage, accidental wedging, and arrhythmia generation.
Risk factors for difficult PAC placement and indications that ultrasound may be useful include low cardiac output states, right-sided chamber dilation, tricuspid valve regurgitation, tricuspid annuloplasty or replacement, and pulmonary hypertension [37]. In the authors’ experience, the most common manipulation required is a counterclockwise turn to redirect the distal tip of the PAC from the right atrial appendage towards the tricuspid valve (Fig. 23.14) [38]. A midesophageal modified bicaval view is extremely useful for manipulations of the catheter in the RA, as it permits imaging of the superior vena cava, right atrial appendage, right atrium, and tricuspid valve (Fig. 23.15; Video 23.13).

Pulmonary artery catheter manipulations used to pass through the tricuspid valve (viewed from the superior vena cava). A catheter in the right atrial appendage should have counterclockwise torque applied to direct it towards the tricuspid valve. A catheter near the inferior vena cava or coronary sinus should have clockwise torque applied to direct it to the tricuspid valve. CCW counterclockwise, CW clockwise, IVC inferior vena cava, CS coronary sinus (Reproduced with permission from Cronin et al. [38])

Midesophageal modified bicaval view. A PAC with the balloon inflated (red arrow) is present in the right atrial appendage. SVC superior vena cava, RA right atrium, LA left atrium, TV tricuspid valve, RAA right atrial appendage (Reproduced with permission from Cronin et al. [38])
Once the catheter passes through the tricuspid valve, a midesophageal RV inflow-outflow view can confirm orientation of the catheter towards the pulmonic valve and facilitates manipulations within the RV (Fig. 23.16; Video 23.14). Finally, the PAC can be positioned in the main pulmonary artery or proximal right pulmonary artery in the ascending aorta SAX view (Fig. 23.17). For a more detailed description of the TEE views and manipulations employed during TEE-guided PAC placement, please see the referenced article. In situations where TEE is either not indicated or contraindicated, TTE can also be used to guide placement and confirm the final position (e.g., left parasternal RV inflow, left parasternal basal SAX, and subcostal views) (Fig. 23.18; Video 23.15).

Midesophageal RV inflow-outflow view (diastole). A PAC is seen traversing the RV with the catheter (red arrow) and balloon (white arrow) clearly visualized. LA left atrium, RA right atrium, RV right ventricle, PA pulmonary artery (Reproduced with permission from Cronin et al. [38])

Midesophageal ascending aorta short-axis view. The PAC balloon (red arrow) is visualized in the proximal right pulmonary artery. SVC superior vena cava, Ao aorta, RPA right pulmonary artery, PA pulmonary artery. (Reproduced with permission from Cronin et al. [38])

Subcostal basal short-axis view. The distal tip of a PAC (red arrow) is located in proximal right pulmonary artery (yellow arrow)
Conclusion
Ultrasound can facilitate central and peripheral venous and arterial access. It may increase success rates, decrease the time required for the procedure, and minimize the risk for complications. Additionally, echocardiography can be utilized to confirm proper guidewire placement and aid in the placement of aortic, central venous, or pulmonary artery catheters.
Abbreviations
- ASE:
-
American Society of Echocardiography
- CA:
-
Carotid artery
- CVC:
-
Central venous catheter
- CVP:
-
Central venous pressure
- FV:
-
Femoral vein
- IJ:
-
Internal jugular (vein)
- LAX:
-
Long-axis
- PAC:
-
Pulmonary arterial catheter
- SAX:
-
Short-axis
- SC:
-
Subclavian (vein)
- SCA:
-
Society of Cardiovascular Anesthesiologists
- TEE:
-
Transesophageal echocardiography
- TTE:
-
Transthoracic echocardiography
References
Blaivas M, Brannam L, Fernandez E. Short-axis versus long-axis approaches for teaching ultrasound-guided vascular access on a new inanimate model. Acad Emerg Med. 2003;10:1307–11.
Merrer J. Complications of femoral and subclavian venous catheterization in critically ill patients: a randomized controlled trial. JAMA. 2001;286:700.
McGee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med. 2003;348:1123–33.
Parienti JJ, Mongardon N, Mégarbane B, et al. Intravascular complications of central venous catheterization by insertion site. N Engl J Med. 2015;373:1220–9.
Hosokawa K, Shime N, Kato Y, et al. A randomized trial of ultrasound image–based skin surface marking versus real-time ultrasound-guided internal jugular vein catheterization in infants. Anesthesiology. 2007;107:720–4.
Milling TJ, Rose J, Briggs WM, et al. Randomized, controlled clinical trial of point-of-care limited ultrasonography assistance of central venous cannulation: the Third Sonography Outcomes Assessment Program (SOAP-3) trial*. Crit Care Med. 2005;33:1764–9.
Schnadower D, Lin S, Perera P, et al. A pilot study of ultrasound analysis before pediatric peripheral vein cannulation attempt. Acad Emerg Med. 2007;14:483–5.
Troianos CA, Hartman GS, Glas KE, et al. Guidelines for performing ultrasound guided vascular cannulation. Anesth Analg. 2012;114:46–72.
Denys BG, Uretsky BF, Reddy PS. Ultrasound-assisted cannulation of the internal jugular vein. A prospective comparison to the external landmark-guided technique. Circulation. 1993;87:1557–62.
Karakitsos D, Labropoulos N, De Groot E, et al. Real-time ultrasound-guided catheterisation of the internal jugular vein: a prospective comparison with the landmark technique in critical care patients. Crit Care. 2006;10:R162.
Troianos CA, Jobes DR, Ellison N. Ultrasound-guided cannulation of the internal jugular vein. A prospective, randomized study. Anesth Analg. 1991;72:823–6.
Bellazzini MA, Rankin PM, Gangnon RE, et al. Ultrasound validation of maneuvers to increase internal jugular vein cross-sectional area and decrease compressibility. Am J Emerg Med. 2009;27:454–9.
Terai C, Anada H, Matsushima S, et al. Effects of mild Trendelenburg on central hemodynamics and internal jugular vein velocity, cross-sectional area, and flow. Am J Emerg Med. 1995;13:255–8.
Blaivas M, Adhikari S. An unseen danger: frequency of posterior vessel wall penetration by needles during attempts to place internal jugular vein central catheters using ultrasound guidance*. Crit Care Med. 2009;37:2345–9.
Stone MB, Hern HG. Inadvertent carotid artery cannulation during ultrasound guided central venous catheterization. Ann Emerg Med. 2007;49:720.
Moak JH, Lyons MS, Wright SW, et al. Needle and guidewire visualization in ultrasound-guided internal jugular vein cannulation. Am J Emerg Med. 2011;29:432–6.
Balls A, LoVecchio F, Kroeger A, et al. Ultrasound guidance for central venous catheter placement: results from the Central Line Emergency Access Registry Database. Am J Emerg Med. 2010;28:561–7.
Gualtieri E, Deppe SA, Sipperly ME, et al. Subclavian venous catheterization. Crit Care Med. 1995;23:692–7.
Lalu MM, Fayad A, Ahmed O, et al. Ultrasound-guided subclavian vein catheterization: a systematic review and meta-analysis. Crit Care Med. 2015;43:1498–507.
Beaulieu Y. Bedside ultrasonography in the ICU *. Chest. 2005;128:1766.
Hind D. Ultrasonic locating devices for central venous cannulation: meta-analysis. BMJ. 2003;327:361–0.
Maddali MM, Arora NR, Chatterjee N. Ultrasound guided out-of-plane versus in-plane transpectoral left axillary vein cannulation. J Cardiothorac Vasc Anesth. 2017;31:1707–12.
Tan B-K, Hong S-W, Huang MHS, et al. Anatomic basis of safe percutaneous subclavian venous catheterization. J Trauma. 2000;48:82.
Iwashima S, Ishikawa T, Ohzeki T. Ultrasound-guided versus landmark-guided femoral vein access in pediatric cardiac catheterization. Pediatr Cardiol. 2007;29:339–42.
Kwon T, Kim Y, Cho D. Ultrasound-guided cannulation of the femoral vein for acute haemodialysis access. Nephrol Dial Transplant. 1997;12:1009–12.
Seto AH, Abu-Fadel MS, Sparling JM, et al. Real-time ultrasound guidance facilitates femoral arterial access and reduces vascular complications. J Am Coll Cardiol Intv. 2010;3:751–8.
Timsit JF, Baleine J, Bernard L, et al. Expert consensus-based clinical practice guidelines management of intravascular catheters in the intensive care unit. Ann Intensive Care. 2020;10:118.
Lamperti M, Biasucci DG, Disma N, et al. European Society of Anaesthesiology guidelines on peri-operative use of ultrasound-guided for vascular access (PERSEUS vascular access). Eur J Anaesthesiol. 2020;37:344–76.
Frankel HL, Kirkpatrick AW, Elbarbary M, et al. Guidelines for the appropriate use of bedside general and cardiac ultrasonography in the evaluation of critically ill patients-part I: general ultrasonography. Crit Care Med. 2015;43:2479–502.
Levin PD, Sheinin O, Gozal Y. Use of ultrasound guidance in the insertion of radial artery catheters. Crit Care Med. 2003;31:481–4.
Shiloh AL. Ultrasound-guided catheterization of the radial artery. Chest. 2011;139:524.
Shiver S, Blaivas M, Lyon M. A prospective comparison of ultrasound-guided and blindly placed radial arterial catheters. Acad Emerg Med. 2006;13:1275–9.
Sandhu NS, Patel B. Use of ultrasonography as a rescue technique for failed radial artery cannulation. J Clin Anesth. 2006;18:138–41.
Keyes LE, Frazee BW, Snoey ER, et al. Ultrasound-guided brachial and Basilic vein cannulation in emergency department patients with difficult intravenous access. Ann Emerg Med. 1999;34:711–4.
Sandhu NPS. Mid-arm approach to basilic and cephalic vein cannulation using ultrasound guidance. Br J Anaesth. 2004;93:292–4.
Cronin B, Kolotiniuk N, Youssefzadeh K, et al. Pulmonary artery catheter placement aided by transesophageal echocardiography versus pressure waveform transduction. J Cardiothorac Vasc Anesth. 2018;32:2578–82.
Turnage WS, Fontanet H. Transesophageal echocardiography-guided pulmonary artery catheter placement. Anesth Analg. 1993;77:858–9.
Cronin B, Robbins R, Maus T. Pulmonary artery catheter placement using transesophageal echocardiography. J Cardiothorac Vasc Anesth. 2017;31:178–83.
Fretwell D, Smith M, Martin E, et al. Epidural intravascular injection detection by transthoracic echocardiography. J Cardiothorac Vasc Anesth. 2020;34:1288–91.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Electronic Supplementary Material
Out-of-plane or short-axis (SAX) imaging of the right internal jugular vein (MP4 13974 kb)
Out-of-plane or short-axis (SAX) imaging of a vessel, showing stepwise introduction of a needle, through serial parallel imaging planes (MP4 1406 kb)
In-plane or long-axis (LAX) imaging of the right internal jugular vein from the same patient in Video 23.1 (MP4 12320 kb)
In-plane or long-axis (LAX) imaging of a vessel, showing introduction of a needle from the left side of the screen (MP4 1355 kb)
Out-of-plane imaging (SAX view) of the right internal jugular vein with color flow Doppler. Color flow Doppler imaging demonstrates faster pulsatile laminar flow in the carotid artery with slower flow in the jugular vein (MP4 245 kb)
In-plane imaging (LAX view) of the right internal jugular with color flow Doppler (MP4 218 kb)
Short-axis imaging of right internal jugular vein with a wire within its lumen (MP4 308 kb)
Long-axis imaging of the right internal jugular vein with a wire noted to be within its lumen (no evidence of “backwall”) (MP4 317 kb)
Midesophageal bicaval view demonstrating the “J-tip” of the central access wire within the right atrium, confirming venous access (MP4 982 kb)
Short-axis imaging of the right subclavian artery and vein (MP4 277 kb)
Short-axis imaging of the femoral artery and vein (MP4 294 kb)
A. Short-axis imaging of the right radial artery (MP4 455 kb)
B. Short-axis imaging of the same patient with color flow Doppler imaging (MP4 380 kb)
Short-axis imaging of the left basilic vein (MP4 593 kb)
Modified subcostal 4-chamber view with a guidewire in the right atrium (MOV 1311 kb)
Descending aorta short-axis view (depth reduced) with the distal tip of an intra-aortic balloon pump in the lumen of the aorta (MOV 3853 kb)
Midesophageal modified bicaval view. A PAC with the balloon inflated is being advanced from the superior vena cava; then a slight counterclockwise rotation redirects it from the right atrial appendage to the tricuspid valve (MOV 6337 kb)
Midesophageal RV inflow-outflow view with a PAC (balloon inflated) being advanced from just below the tricuspid valve through the right ventricle and towards the pulmonic valve (MOV 9740 kb)
Subcostal basal short-axis view with a PAC traversing the tricuspid valve and right ventricle, with its distal tip positioned in the proximal right pulmonary artery (MOV 1763 kb)
Questions
Questions
-
1.
The following image is obtained while attempting to place a radial arterial catheter. Which of the following is most true?
-
A.
This site is not suitable, because the radial artery is occluded
-
B.
The depth should be increased
-
C.
The angle of the probe should be adjusted
-
D.
This site is suitable for cannulation
-
A.
-
2.
While attempting peripheral venous access, the following image is obtained. There is no return of blood in the catheter. What is the next best step?
-
A.
Withdraw the needle and advance again
-
B.
Advance the needle further into the vessel
-
C.
Rotate the probe to obtain a long-axis view
-
D.
Agitate the needle to confirm visualization
-
A.
-
3.
Which of the following statements is most accurate?
-
A.
Subclavian catheters have a lower infectious risk, but higher thrombotic risk than femoral catheters.
-
B.
Internal jugular catheters have the lowest risk for infection.
-
C.
Ultrasound cannot be used for guidance for subclavian cannulation.
-
D.
Femoral catheters have the highest risk for both thrombosis and infection.
-
A.
-
4.
Which of the following statements regarding pulmonary arterial catheter (PAC) placement is most true?
-
A.
A midesophageal ascending aorta SAX view can confirm appropriate catheter position.
-
B.
A midesophageal RV inflow-outflow view can confirm appropriate catheter position.
-
C.
Ultrasound decreases time to placement and the success rate of PACs.
-
D.
A midesophageal modified bicaval tricuspid valve view can confirm appropriate catheter position.
-
A.
-
5.
Which of the following sites would be most appropriate for insertion of a LEFT femoral venous catheter in the following image?
-
A.
A
-
B.
B
-
C.
C or D
-
D.
None of the above
-
A.



Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Herway, S.T., Cronin, B. (2022). Ultrasound for Vascular Access. In: Maus, T.M., Tainter, C.R. (eds) Essential Echocardiography. Springer, Cham. https://doi.org/10.1007/978-3-030-84349-6_23
Download citation
DOI: https://doi.org/10.1007/978-3-030-84349-6_23
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-84348-9
Online ISBN: 978-3-030-84349-6
eBook Packages: MedicineMedicine (R0)