
Abstract
Gastrostomy tube placement is indicated for either enteral feeding or for palliative gastric decompression. Percutaneous endoscopic gastrostomy (PEG) tube placement has largely supplanted the need for surgical gastrostomy tubes. However, surgical gastrostomy is still indicated in cases when the esophagus cannot be traversed endoscopically, or when PEG is otherwise not technically possible. In other instances when enteral feeding directly to the jejunum is preferred, the Witzel jejunostomy can be performed. The techniques of PEG and Stamm gastrostomy as well as Witzel jejunostomy technique are described in this chapter. This chapter describes the preoperative preparation, pitfalls and danger points, operative strategy, and identification of complications. Step-by-step technical instructions, supplemented by operative photographs, are included. The chapter concludes with a list of selected references.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Indications
Percutaneous Gastrostomy
-
Enteral feeding
-
Gastric decompression, such as may be required with motility disorders or for palliation of malignant bowel obstruction
Surgical Gastrostomy
-
Failed percutaneous approach
-
Inability to traverse esophagus endoscopically
-
Need for gastrostomy tube at the time of laparotomy for other indication
Jejunostomy
-
Enteral feeding in cases where gastrostomy is not feasible, for example, esophageal or gastric malignancy, gastro-colonic fistula, etc.
-
Abdominal procedure with expected prolonged nothing by mouth (NPO) status
-
Intolerance to gastric feeds due to aspiration or gastric paresis
Historically, gastrostomy tubes were used only for venting while jejunostomy tubes were used for feeding; however, with the data that jejunostomy tubes do not decrease the risk of aspiration, this practice has been abandoned. Known complications of jejunostomy tubes, such as obstruction of the small bowel, dislodgement with enteric leak, and small bowel volvulus are other reasons that its use has declined. Special gastrostomy tubes with a second jejunostomy limb can be used in selected cases when both gastric venting and jejunostomy feedings are necessary.
Pitfalls and Danger Points
PEG (or surgical gastrostomy) may not be feasible in patients who have had extensive left upper quadrant surgery, such as gastric bypass – consider jejunostomy in these cases
Injury to large bowel or small bowel
Enteric leak into the peritoneal cavity
Tube dislodgment
Obstruction of bowel lumen by the tube (jejunostomy)
Volvulus around the tube site (jejunostomy)
Operative Strategy
The PEG tube is widely available and has the benefit of allowing enteral access while causing minimal discomfort to the patient. Placement depends on the stomach being able to be distended enough with insufflation to come into direct contact with the anterior abdominal wall. In addition, the stomach must be located below the costal margin, since most patients requiring a PEG tube have had a nasogastric tube in place at some point, an abdominal X-ray is adequate to ensure that the patient does not have largely intrathoracic stomach. The procedure is most easily performed with two surgeons – one to operate the endoscope and the second to place the tube. The procedure can also be done with a surgeon (to place the tube) and a trained assistant (to manipulate the endoscope).
In cases where the endoscopic approach is not feasible, a surgical gastrostomy tube can be performed. The Stamm gastrostomy is a safe and technically easy procedure in which the serosa around the gastrostomy site is inverted to prevent leakage of gastric contents around the tube. The Stamm gastrostomy can also be performed laparoscopically.
When constructing a tube gastrostomy, the opening to the stomach is sutured to the anterior abdominal wall around the stab wound made for the exit of the tube. This allows for the formation of a scar tract that can be re-intubated in the future to replace a dislodged tube. It is important that the tube remain in place for at least 6 weeks to allow formation of this scar tract, otherwise gastric contents may leak out of the gastrostomy opening into the abdominal cavity. Surgical G-tubes provide additional security afforded by suturing the anterior gastric wall to the abdominal wall; however, earlier concerns about an increased leak rate for PEG versus surgical gastrostomy have not been realized.
Similar concepts apply for the construction of the Witzel jejunostomy. The creation of the tunnel facilitates spontaneous closure after removal and also decreases the risk of tube dislodgement. Small bowel should be sutured to the abdominal wall for a distance of at least 10cm to prevent volvulus.
Operative Technique
Percutaneous Endoscopic Gastrostomy (PEG) Tube Placement
This procedure is performed with a standard gastroscope and any of a number of commercially available PEG tube kits. We prefer PEG tubes with a traction removable bumper. It is important to position the tube site at least two fingerbreadths below the costal margin to prevent discomfort from the tube when the patient is sitting. Prepare the abdomen and mark a line in the left upper quadrant two fingerbreadths below the costal margin for a proposed tube puncture site. In order to prevent formation of a gastrocutaneous fistula, the tube should pass through a muscular portion of the abdominal wall and not through a hernia sac or a broad diastasis recti. Operating room lights are dimmed and the gastroscope is inserted through the oropharynx into the esophagus and advanced into the stomach. We take this opportunity to evaluate the stomach and duodenum for abnormalities, such as stress ulceration or peptic ulcer disease. Insufflate the stomach until all rugal folds have flattened out. Maintain this distension throughout the procedure, as it helps to displace the colon from the upper abdomen and brings the gastric wall in apposition to the anterior abdominal wall.
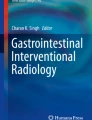
Then press vigorously with the index finger over the tube site as the anterior gastric wall is observed with the gastroscope. A clear focal indentation should be seen on the gastric wall when the finger is pressing to indicate that the gastric wall is directly adjacent to the anterior abdominal wall without other structures (such as the colon) in the way. Next, bring the gastroscope up against the gastric wall at the exact location of the finger indentation and increase the gastroscope light source intensity to the transilluminate setting. A spot of light (focal light reflex) should shine through the abdominal wall at the proposed tube site (Fig 32.1). Failure to see both focal indentation of the gastric wall with finger ballotment and a focal light reflex with transillumination suggests that another structure, such as the colon, is interposed between stomach and abdominal wall. This means that it is unsafe to proceed with PEG tube placement and surgical gastrostomy tube placement should be considered. Infiltrate local anesthetic into the skin and abdominal wall at the proposed tube site and make a 5 mm puncture wound with an 11 blade scalpel. Insert an angiocatheter through the puncture site and observe it endoscopically entering the gastric lumen (Fig. 32.2). Pass an endoscopy snare through the working channel of the gastroscope and position the open loop around the angiocatheter. Insert a long-looped string through the angiocatheter and grasp it by tightening the pre-positioned endoscopy snare. Then withdraw both the gastroscope and one end of the snared looped string through the patient’s mouth. Tie or secure (with an interlocking loop) the looped string to the tapered end of the PEG tube. By applying strong steady traction to the part of the string passing out through the abdominal wall, pull the looped end and gastrostomy tube back through the patient’s mouth, through the stomach, and back through the puncture wound in the abdominal wall. Since the gastroscope needs to be reintroduced into the stomach, we grasp the PEG tube bumper with the biopsy snare so that the gastroscope is pulled back into the stomach along with the PEG tube. The tapered end of the PEG tube is pulled through the anterior abdominal wall until the bumper is clear in the stomach. Use care to watch the numbers on the shaft of the PEG tube and not to pull too hard, as it is possible to inadvertently pull the bumper out of the stomach at this stage.

Fig. 32.1

Fig. 32.2
Re-insufflate the stomach, disengage the biopsy snare from the bumper by opening the loop of the snare, and further withdraw the PEG tube until the bumper gently indents the gastric mucosa. Test that the bumper is not too tight by twisting the tube and confirming that the bumper can spin easily against the gastric mucosa. If the bumper is too tight against the gastric wall, necrosis can result. Note the depth of tube by looking at numbered gradations on the side of the tube (Fig. 32.3) and place the skin-level retention disk over the PEG tube to secure it in this position. Place the tube clamp is placed, cut the tube to the desired length, and place the feeding tube adaptor (Fig. 32.4). We keep the tube on gravity drainage overnight before beginning tube feedings.

Fig. 32.3

Fig. 32.4
Stamm Gastrostomy
When performed as part of another abdominal procedure, any incision providing access to the upper abdomen can be used. When gastrostomy is performed as the sole procedure, a very limited transverse incision in the left upper quadrant can be used in thin patients. In overweight patients, an upper midline incision is generally necessary.
Choose a portion of the stomach that easily apposes to the anterior abdominal wall in the left subcostal region. Generally, the gastrotomy should be closer to the greater curvature of the stomach to allow room for inversion of gastric serosa around the tube (Fig. 32.5). Using 2-0 atraumatic absorbable suture, insert a deep seromuscular or full-thickness circular purse-string suture just larger than the diameter of the tube to be placed.

Fig. 32.5
Generally, at least an 18F tube is used to prevent occlusion with tube feeds, and larger diameter tubes can be used for more efficient drainage. While Foley, Malecot, or mushroom catheters have been used in the past, specifically designed feeding tubes are now encouraged for use to prevent medical tubing misconnection errors (i.e., EnFIT). Grasp the abdominal wall fascia with a Kocher clamp and place the fascia on traction. The tube should exit at least two fingerbreadths below the left costal margin to prevent patient discomfort when sitting. The tube should pass through the rectus muscle to prevent formation of a gastrocutaneous fistula, and to allow the tube site to contract and close down once the tube is removed. Make a stab wound at the proposed tube exit site and pass a hemostat full thickness through the abdominal wall. Grasp the tip of the feeding tube and pull it through the abdominal wall into the abdominal cavity. Incise the stomach wall in the center of the purse string suture and pass the feeding tube into the gastric lumen (Fig. 32.5). The purse-string suture should now be tightened down snuggly around the tube and tied (Fig. 32.6). As long as the purse-string suture material is absorbable, the tails of suture material may be tied around the tube itself to prevent the tube from dislodging during the remainder of the procedure. Inversion of the tube so that a generous layer of gastric serosa is brought into apposition circumferentially around the tube is critical to prevent leakage of gastric contents into the peritoneal cavity. This can be done either with a second concentric purse-string suture (Fig. 32.7) or with a several generous Lembert sutures on either side of the tube. The stomach should now be brought up toward the anterior abdominal wall and silk Lembert sutures should be placed circumferentially around the tube to anchor the stomach securely to the abdominal wall (Figs. 32.8 and 32.9). At the tube exit site, the G-tube is now fastened securely to the skin with a non-absorbable suture.

Fig. 32.6

Fig. 32.7

Fig. 32.8

Fig. 32.9
Witzel Jejunostomy
Witzel Jejunostomy is a common procedure for jejunostomy creation. The creation of the seromuscular Witzel tube is critical to prevent leakage of enteric contents from the jejunostomy into the abdominal cavity. Just as with the gastrostomy tubes, when the jejunostomy is no longer needed, removal of the tube usually results in prompt closure of the tract.
Generally, at least a 12F tube is used to prevent occlusion with tube feeds. While red rubber catheters are still being used, specifically designed feeding tubes with EnFIT fittings applied are now encouraged to prevent medical tubing misconnection errors. When using a red rubber tube, we cut the end off the distal end of the tube so that it may later be replaced over a guidewire. When performed as part of another abdominal procedure, any incision giving access to the upper abdomen can be used. When open jejunostomy is performed as the sole procedure, a very limited transverse incision in the left upper quadrant can be used in thin patients, with upper midline incision generally necessary for overweight patients. The jejunostomy tube should be placed in the proximal jejunum in order to permit maximum absorption of nutrients. We generally select a segment of jejunum approximately 20 cm distal to the ligament of Treitz that will easily appose to a point on the anterior abdominal wall without tension. Grasp the abdominal wall fascia with a Kocher clamp and place the fascia on traction. Jejunostomy tube positioning is analogous to gastrostomy tube placement: the tube should exit at least two fingerbreadths below the left costal margin to prevent patient discomfort when sitting, and the tube should also pass through the rectus muscle to prevent formation of an enterocutaneous fistula, and to allow the tube site to contract and close down once the tube is removed. Make a stab wound at the proposed tube exit site and pass a hemostat full thickness through the abdominal wall. Grasp the tip of the jejunostomy tube and pull it through the abdominal wall into the abdominal cavity.
Using 3-0 atraumatic absorbable suture, insert a deep seromuscular or full-thickness purse-string suture just larger than the diameter of the tube to be placed (Fig. 32.5). Great care must be taken to limit the size of the purse-string so that it does not compromise the lumen of the jejunum, leading to obstruction. A 5mm incision is made in the antimesenteric border of the jejunum and the tube is inserted into the jejunum and directed distally for a distance of at least 15 cm. The purse-string suture is now tied down around the tube. As long as the purse-string suture material is absorbable, the tails of suture material may be tied around the tube itself to prevent the tube from dislodging during the remainder of the procedure. If the tube used has an inflatable balloon, we place the balloon in the jejunum at least 5 cm distal to the purse string and inflate it with only 3 ccs of water. This is to prevent occluding the lumen of the jejunum. Starting at the jejunostomy and proceeding distally approximately 5cm, the Witzel tunnel is created by placing 3.0 silk seromuscular Lembert sutures (Fig. 32.6). Again, great care must be taken to prevent the Witzel tunnel from occluding the lumen of the jejunum. We also place a Lembert suture just proximal to the jejunostomy to invert the purse string in order to prevent leakage of enteric contents into the abdominal cavity (Fig. 32.7). The needles should be left on the two sutures adjacent to the tube, and the most distal suture of the Witzel tunnel. The jejunum should now be brought up toward the anterior abdominal wall and these sutures are used anchor the jejunum securely to the abdominal wall (Fig. 32.8). Broad apposition of the jejunum to the anterior abdominal wall resists the tendency for volvulus, and will allow for percutaneous access to this loop of the jejunum by interventional radiology, should the tube become dislodged and the tract closed down. At the tube exit site, the jejunostomy tube is now fastened securely to the skin with a non-absorbable suture. Feeding can start same day of placement or after return of bowel function, in the case of ileus.
In instances when there is concern of possible obstruction after the Witzel tunnel creation due to a small bowel caliber, we recommend doing a seromuscular incision 5cm in length where the feeding tube will be placed and closure of the seromuscular layers on top (Fig. 32.9). This will elongate the area that will be used to create the Witzel tunnel, thereby preventing obstruction.
Further Reading
Al-Bawardy B, Gorospe EC, Alexander JA, Bruining DH, Coelho-Prabhu N, Rajan E, Wong Kee Song LM. Outcomes of double-balloon enteroscopy-assisted direct percutaneous endoscopic jejunostomy tube placement. Endoscopy. 2016;48:552–6.
Goncalves Pereira Bravo J, Ide E, Kondo A, Turiani Hourneaux de Moura D, Turiani Hourneaux de Moura E, Sakai P, et al. Percutaneous endoscopic versus surgical gastrostomy in patients with benign and malignant diseases: a systematic review and meta-analysis. CLINICS (Sao Paulo, Brazil) 2016;71(3):169–178
Strong AT, Sharma G, Davis M, Mulcahy M, Punchai S, O’Rourke CP, et al. Direct Percutaneous Endoscopic Jejunostomy (DPEJ) Tube Placement: A Single Institution Experience and Outcomes to 30 Days and Beyond. J Gastrointest Surg. 2017;21:446–52.
Toh Yoon EW, Yoneda K, Nakamura S, Nishihara K. Percutaneous endoscopic transgastric jejunostomy (PEG-J): a retrospective analysis on its utility in maintaining enteral nutrition after unsuccessful gastric feeding. BMJ Open Gastro. 2016;3:e000098. https://doi.org/10.1136/bmjgast-2016-000098.
Young MT, Troung H, Gebhart A, Shih A, Nguyen NT. Outcomes of laparoscopic feeding jejunostomy tube placement in 299 patients. Surg Endosc. 2016;30:126–31.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Rivera, M., Schiller, H. (2022). Enteral Access. In: Scott-Conner, C.E.H., Kaiser, A.M., Nguyen, N.T., Sarpel, U., Sugg, S.L. (eds) Chassin's Operative Strategy in General Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-81415-1_32
Download citation
DOI: https://doi.org/10.1007/978-3-030-81415-1_32
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-81414-4
Online ISBN: 978-3-030-81415-1
eBook Packages: MedicineMedicine (R0)