
Abstract
Over several years, functional tumour imaging has often relied on abnormal patterns of specific metabolic pathways or the overexpression of tumour specific receptors. Initial observations that demonstrated the alterations in Kennedy pathway in cancerous tissues fueled the development of radiolabelled choline and exploration of its uptake patterns in tumour cells. Subsequently, several trials and research studies established the invaluable role of choline-based radiotracers in accurate detection of biochemical relapse in patients of prostate cancer, following initial definitive treatment. In this chapter, we review the physiological distribution and pitfalls of FCH PET/CT imaging that a clinician should be aware of during the interpretation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Over several years, functional tumour imaging has often relied on abnormal patterns of specific metabolic pathways or the overexpression of tumour specific receptors. Initial observations that demonstrated the alterations in Kennedy pathway in cancerous tissues fueled the development of radiolabelled choline and exploration of its uptake patterns in tumour cells. Subsequently, several trials and research studies established the invaluable role of choline-based radiotracers in accurate detection of biochemical relapse in patients of prostate cancer, following initial definitive treatment.
Although preliminary studies linked the increased phosphocholine (PCho) levels in tumour cells to increased cell membrane turnover and thus to proliferative activity, it was only subsequently realised to be due to overexpression of the choline transporters (e.g. CLT-1) and the key enzyme, choline 1-α-kinase. Several molecules were developed to target these mechanisms; however, only 11C-choline, 18F-methylcholine (FCH) and 18F-ethylcholine garnered widespread utilisation [1]. Since 11C-choline is biochemically indistinguishable from natural choline and shows similar kinetics, it is believed to follow the pathways of naturally occurring choline. Although its favourable imaging characteristic of limited urinary clearance had the advantage in urological malignancies, the short half-life of 11C (20 minutes) restricted its utilisation only to centres equipped with an on-site cyclotron. Flourine-18 methylcholine (FCH) was subsequently developed by DeGrado et al., which demonstrated slightly slower rates of incorporation than choline and higher rates of urinary clearance than 11C-Choline. However, better image quality and longer half-lives provided logistic advantage over 11C-choline [2]. Currently, both these tracers are in use depending on their availability and validation in various regions.
Several authors have previously reported and reviewed the several pitfalls of PET imaging with radiolabelled choline derivatives [3, 4]. In this chapter, we review the physiological distribution and pitfalls of FCH PET/CT imaging that a clinician should be aware of during the interpretation.
8.1 Physiological Tracer Distribution
After intravenous administration, significant fraction of radiolabelled choline is rapidly cleared from the circulation within 10 min, after which the plasma concentration reaches a plateau. Physiological uptake of tissues is noted most prominently in the liver, pancreas, followed by salivary glands, spleen and lacrimal glands. Mild diffuse tracer uptake is noted in the bone marrow and muscles. A recent multicentre evaluation demonstrated no significant difference in the extra-prostatic distributions of 11C-choline, 18F-methylcholine (FCH) and 18F-ethylcholine [1]. Table 8.1 lists the organs with physiological uptake graded as per the degree of uptake.
8.2 Applications
Although choline labelled radiotracers were utilised in evaluating patients with several malignancies (including brain tumours, oesophageal cancer, hepatocellular carcinoma [5] and several others), the most important clinical application is prostate cancer imaging [6] (Fig. 8.1). Incidental detection of parathyroid adenoma in patients imaged for prostate cancer evaluation led to recent studies in evaluating its utility in evaluation of patients with primary hyperparathyroidism (Fig. 8.2). Table 8.2 lists the various malignancies evaluated using radiolabelled choline PET/CT imaging and various indications in prostate cancer.

58 year-old-man with incidentally detected elevated S. PSA—2000 ng/mL. Trans-rectal ultrasound guided biopsy from the prostate was done, which showed adenocarcinoma (Gleason’s score 4 + 4 = 8). 18F-Choline PET/CT done for staging showed multiple foci of increased tracer avidity in the thoracic region, abdomen and pelvis in the maximum intensity projection image (a). Transaxial CT and fused PET/CT images showed increased tracer avidity in a heterogeneously enhancing lesion in the entire prostate (b, c—arrow; SUVmax 5.4), multiple tracer avid bilateral lung nodules (d, e) with SUVmax 14.5 and tracer avid sclerotic lesion in the sacrum (f, g) with SUVmax 11. The patient was put on androgen deprivation therapy with anti-androgen therapy and concurrent docetaxel based chemotherapy

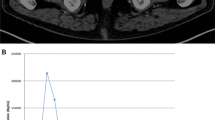
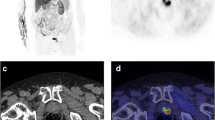
45 year-old-man with history of renal stone disease. Biochemical examination showed elevated serum levels of calcium (12.2 mg/dL) and intact parathyroid hormone (270 pg/mL). Ultrasound of neck did not reveal any abnormality. Sestamibi scan done for detection of parathyroid adenoma did not reveal any abnormality. 18F-Choline PET/CT showed a well-defined tracer avid (SUVmax 11.4) lesion postero-inferior to the right lobe of thyroid gland (~1.7 × 1.2 cm) (maximum intensity projection image—(a), transaxial CT—(b), fused PET/CT—(c), arrow). The patient underwent surgical resection of the lesion with the histopathology confirming the parathyroid adenoma
8.3 False Positive FCH Uptake
It is not uncommon to notice incidental sites of FCH uptake that are less likely to be related to the primary aetiology of concern (usually prostate cancer) (Figs. 8.3, 8.4, and 8.5). In such cases, all suspicious findings warrant further evaluation with imaging and/or histological correlation to rule out any atypical pattern of metastatic involvement or any synchronous malignancy (Table 8.3). Also, several benign inflammatory and non-inflammatory conditions can demonstrate variable FCH uptake due to its inherent non-specific mechanism of uptake. Knowledge of these conditions will avoid potential misinterpretation of these conditions as malignant/metastatic involvement (Table 8.4).

45 year-old-man with an incidentally detected intracranial space occupying lesion on CT. MRI showed an extra-axial mass in the left frontal—basi-frontal region—likely meningioma. 18F-Choline PET/CT showed increased tracer uptake (SUVmax 6.1) in a hyperdense lesion (~3.2 × 3.0 cm) in the left basi-frontal region (maximum intensity projection image—(a), transaxial PET—(b), CT—(c), fused PET/CT—(d)). Mass effect was also seen in the form of effacement of frontal horn of left lateral ventricle and midline shift (maximum ~7 mm) towards the right side with significant perilesional oedema. He subsequently underwent tumour resection and the histopathology was suggestive of meningioma

51 year-old-man with acromegaly. MRI examination suggestive of pituitary microadenoma. 18F-Choline PET/CT showed a tracer avid (SUVmax 5) hyperdense soft tissue lesion (~1.3 × 1.9 cm) in the pituitary fossa—likely pituitary macroadenoma (maximum intensity projection image—(a), transaxial PET—(b), CT—(c), fused PET/CT—(d), arrow). The patient underwent trans-sphenoidal resection of the tumour and had an uneventful post-operative recovery. The diagnosis on histopathologic examination of the resection specimen was pituitary macroadenoma

68-year-old-man presented with complaint of headache for 1 year, gradual in onset and with increasing severity. MRI of the head was suggestive of clival chondrosarcoma. 18F-Choline PET/CT showed a tracer avid (SUVmax 4.8) lytic expansile mass (~3.6 × 6.1 × 5.2 cm) at the base of the skull (maximum intensity projection image—(a), transaxial CT—(b), fused PET/CT—(c)). The mass was seen to cause lytic destructive changes of the base of the skull, clivus and the sella with anteriorly extension to the sphenoid sinus (arrow in (b, c)). The patient underwent tumour resection with the histopathology diagnosing the tumour as clival chordoma
8.4 False Negative Interpretation of FCH PET/CT (Table 8.5)
Some authors have reported lower detection rates of FCH PET/CT imaging in patients treated with androgen deprivation therapy [43]. However, subsequently results contrary to initial have been reported. Hence, due to lack of conclusive evidence for or against the hypothesis, currently withholding of therapy is suggested in hormone naïve patients planned for restaging. There is also report of impaired uptake of tracer in patients taking colchicine.
Administration of furosemide enhances the rapidity of tracer clearance and improves interpretation of perivesical space and avoids focal abnormal accumulations in the ureter. However, recently Rischke et al. reported that administration of furosemide reduced the degree of choline uptake in pelvic lymph nodes [42]. Hence, an early initial imaging followed by a delayed post-diuretic regional imaging seems to be a safer alternative. Some authors also reported that similar potential false negative interpretations are possible in patients treated with erythropoietin and chemotherapeutic drugs like docetaxel and paclitaxel [7, 41].
Key Points
-
Choline labelled radiotracers were utilised in evaluating patients with several malignancies and the most important clinical application is prostate cancer imaging.
-
Flourine-18 methylcholine (FCH) demonstrates slightly slower rates of incorporation and higher rates of urinary clearance than 11C-choline.
-
Physiological uptake of tissues is noted most prominently in the liver, pancreas, followed by salivary glands, spleen and lacrimal glands.
-
There is no significant difference in the extra-prostatic distributions of 11C-choline, 18F-methylcholine (FCH) and 18F-ethylcholine.
References
Calabria F, Gallo G, Schillaci O, et al. Bio-distribution, imaging protocols and diagnostic accuracy of PET with tracers of lipogenesis in imaging prostate cancer: a comparison between 11C-Choline, 18F-Fluoroethylcholine and 18F-methylcholine. Curr Pharm Des. 2015;21:4738–47.
DeGrado TR, Reiman RE, Price DT, et al. Pharmacokinetics and radiation dosimetry of 18F-fluorocholine. J Nucl Med. 2002;43:92–6.
Calabria F, Chiaravalloti A, Schillaci O. 18F-choline PET/CT pitfalls in image interpretation. Clin Nucl Med. 2013;39:1.
Beheshti M, Haroon A, Bomanji JB, et al. Fluorocholine PET/computed tomography. PET Clin. 2014;9:299–306.
Chalaye J, Baranes L, Costentin C, et al. Dual-tracer 18F-fluorocholine and 18F-fluorodeoxyglucose PET/CT for the diagnosis of tumoral portal vein thrombosis in patients with hepatocellular carcinoma. HPB. 2016;18:e531.
Hara T, Kosaka N, Kishi H. PET imaging of prostate cancer using carbon-11-choline. J Nucl Med. 1998;39:990–5.
Wallitt KL, Khan SR, Dubash S, et al. Clinical pet imaging in prostate cancer. Radiographics. 2017;37:1512–36.
Hara T, Kosaka N, Kishi H. Development of (18)F-fluoroethylcholine for cancer imaging with PET: synthesis, biochemistry, and prostate cancer imaging. J Nucl Med. 2002;43:187–99.
Hara T, Kosaka N, Shinoura N, et al. PET imaging of brain tumor with [methyl- 11C]choline. J Nucl Med. 1997;38:842–7.
Thanseer NTK, Parihar A, Sood A, et al. Evaluation of recurrent parathyroid carcinoma: a new imaging tool in uncommon entity. World J Nucl Med. 2019;18:198.
Li M, Peng Z, Liu Q, et al. Value of 11C-choline PET/CT for lung cancer diagnosis and the relation between choline metabolism and proliferation of cancer cells. Oncol Rep. 2013;29:205–11.
Talbot JN, Michaud L, Grange JD, et al. Use of choline PET for studying hepatocellular carcinoma. Clin Transl Imaging. 2014;2:103–13.
Sassa N, Kato K, Abe S, et al. Evaluation of 11C-choline PET/CT for primary diagnosis and staging of urothelial carcinoma of the upper urinary tract: a pilot study. Eur J Nucl Med Mol Imaging. 2014;41:2232–41.
Hara T. 18F-fluorocholine: a new oncologic PET tracer. J Nucl Med. 2001;42:1815–7.
Torizuka T, Kanno T, Futatsubashi M, et al. Imaging of gynecologic tumors: comparison of 11C-choline PET with 18F-FDG PET. J Nucl Med. 2003;44:1051–6.
Haroon A, Zanoni L, Celli M, et al. Multicenter study evaluating extraprostatic uptake of 11C-choline, 18F-methylcholine, and 18F-ethylcholine in male patients: physiological distribution, statistical differences, imaging pearls, and normal variants. Nucl Med Commun. 2015;36:1065–75.
Fallanca F, Giovacchini G, Picchio M, et al. Incidental detection by [11C]choline PET/CT of meningiomas in prostate cancer patients. Q J Nucl Med Mol Imaging. 2009;53:417–21.
Maffione AM, Mandoliti G, Pasini F, et al. Pituitary non-functioning adenoma disclosed at 18F-choline PET/CT to investigate a prostate cancer relapse. Clin Nucl Med. 2016;41:e460.
Wu H, Wang Q, Wang M, et al. Preliminary study of 11C-choline PET/CT for T staging of locally advanced nasopharyngeal carcinoma: comparison with 18F-FDG PET/CT. J Nucl Med. 2011;52:341–6.
Lalire P, Zalzali M, Garbar C, et al. Incidental detection of oxyphilic papillary thyroid carcinoma by 18F-fluorocholine PET/CT. Clin Nucl Med. 2016;41:512–3.
Eccles A, Challapalli A, Khan S, et al. Thyroid lymphoma incidentally detected by 18F-fluorocholine (FCH) PET/CT. Clin Nucl Med. 2013;38:755–7.
Kobori O, Kirihara Y, Kosaka N, et al. Positron emission tomography of esophageal carcinoma using (11)C-choline and (18)F-fluorodeoxyglucose: a novel method of preoperative lymph node staging. Cancer. 1999;86:1638–48.
Imperiale A, Cabral JF, Rust E, et al. 18F-fluorocholine uptake in a case of adrenal incidentaloma: possible diagnostic pitfall or potential tool for adrenocortical tumors characterization? Clin Nucl Med. 2013;38:83–4.
Ambrosini V, Farsad M, Nanni C, et al. Incidental finding of an 11C-choline PET-positive solitary plasmacytoma lesion. Eur J Nucl Med Mol Imaging. 2006;33:1522.
Florimonte L, Orunesu E, Castellani M, et al. 18F-choline PET/CT-positive lytic bone lesions in prostate cancer and accidental myeloma detection. Clin Nucl Med. 2016;41:394–6.
Dias AH, Bouchelouche K. Skeletal “superscan” on 18F-choline PET/CT: cases of myeloproliferative disease. Clin Nucl Med. 2016;41:173–4.
Garzon JG, Bassa P, Moragas M, et al. Incidental diagnosis of diffuse large B-cell lymphoma by 11C-choline PET/CT in a patient with biochemical recurrence of prostate cancer. Clin Nucl Med. 2014;39:742–3.
Goineau A, Colombié M, Rousseau C, et al. Incidental detection of a Hodgkin lymphoma on 18F-choline PET/CT and comparison with 18F-FDG in a patient with prostate cancer. Clin Nucl Med. 2015;40:670–1.
Agrawal K, Sajjan RS, Gavra M, et al. Incidental neurofibroma on 18F-fluorocholine PET/MR. Clin Nucl Med. 2015;40:e455–6.
Rahbar K, Fuchs M, Kemper S, et al. Imaging of a paraganglioma on C-11 choline PET/CT. Clin Nucl Med. 2009;34:119–21.
Cazaentre T, Clivaz F, Triponez F. False-positive result in 18F-Fluorocholine PET/CT due to incidental and ectopic parathyroid hyperplasia. Clin Nucl Med. 2014;36:328–30.
Balogova S, Michaud L, Vereb M, et al. 18F-fluorocholine may be taken-up by brown adipose tissue. Nuklearmedizin. 2013;52:3.
Vorster M, Stoltz A, Jacobs AG, et al. Imaging of pulmonary tuberculosis with 18F-fluoro-deoxy-glucose and 18F-ethylcholine. Open Nucl Med J. 2014;6:17–21.
Pinaquy J-B, Fernandez P, Pasticier G, et al. Anthracosis mimicking mediastinal lymph node metastases with 18F-FCholine in high-risk prostate cancer. Clin Nucl Med. 2015;40:e253–4.
Khor LK, Loi HY, Sinha AK, et al. Incidental possible diagnosis by 18F-fluorocholine PET/CT of Meckel’s diverticulum and potential pitfalls. Hell J Nucl Med. 18:157–9.
Leyendecker P, Imperiale A, Matern J-F, et al. Intense 18F-choline uptake after minor head injury: misleading PET/CT result in a patient with biochemical relapse of prostate adenocarcinoma. Clin Nucl Med. 2014;39:1012–3.
García JR, Alvarez Moro FJ, Bassa P, et al. Brown tumours due to secondary hyperparathyroidism detected by 11C-choline PET/CT. Rev Esp Med Nucl Imagen Mol. 35:209–10.
Gu CN, Hunt CH, Lehman VT, et al. Benign fibrous dysplasia on [(11)C]choline PET: a potential mimicker of disease in patients with biochemical recurrence of prostate cancer. Ann Nucl Med. 2012;26:599–602.
Savelli G, Perotti V, Rosso E, et al. 18F-fluorocholine PET/CT finding of a vertebral hemangioma. Clin Nucl Med. 2016;41(8):390.
Wartski M, Jehanno N, Gontier E, et al. Hyperfixation ostéomédullaire diffuse de la 18F-fluorocholine et hémopathies chroniques. Med Nucl. 2015;39:414–7.
Balogova S, Huchet V, Egrot C, et al. Effect of erythropoietin on bone marrow uptake of 18F-fluorocholine in prostate cancer. Clin Nucl Med. 2013;38:200–2.
Rischke HC, Beck T, Vach W, et al. Furosemide diminishes 18F-fluoroethylcholine uptake in prostate cancer in vivo. Eur J Nucl Med Mol Imaging. 2014;41:2074–82.
Chondrogiannis S, Marzola MC, Ferretti A, et al. Is the detection rate of 18F-choline PET/CT influenced by androgen-deprivation therapy? Eur J Nucl Med Mol Imaging. 2014;41:1293–300.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Gorla, A.K.R., Agrawal, K., Parihar, A.S., Mittal, B.R. (2022). 18F-methylcholine (FCH) PET/CT Imaging: Physiological Distribution, Pitfalls and Imaging Pearls. In: Agrawal, K., Skillen, A., Esmail, A., Usmani, S. (eds) PET/CT Imaging. Clinicians’ Guides to Radionuclide Hybrid Imaging(). Springer, Cham. https://doi.org/10.1007/978-3-030-75476-1_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-75476-1_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-75475-4
Online ISBN: 978-3-030-75476-1
eBook Packages: MedicineMedicine (R0)