
Abstract
Perinatal mortality is the combination of foetal deaths (or stillbirths) from the age of viability and early neonatal deaths (deaths within the first 7 days of life). Perinatal deaths, world over, occur as a result of poor health care during pregnancy, during labour and delivery and immediately after child birth. Although, the factors contributing to poor maternity and early neonatal care are similar across the globe, the bulk of perinatal deaths occur in the poor parts of the world. Some of the important clinical determinants of perinatal deaths include pregnancy complications such as ante-partum haemorrhage, severe maternal or intrauterine infection, abnormal labour which predisposes to preterm birth and low birth weight with the various complications, and severe intra-partum events such as foetal hypoxia and birth asphyxia.
The pattern of perinatal deaths often reflects the relationship between economic realities and access to good health services and development. Therefore, global attention is shifting towards addressing these health-related socio-economic inadequacies, which predispose to perinatal mortality. Several evidence-based interventions are coming up to improve the outcome of pregnancies through strengthening the existing weak health system in the resource-poor parts of the world, improve the standards of living and access to quality health care services.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Asphyxia
- Early neonatal deaths
- Perinatal mortality
- Prematurity
- Severe Intra-partum events
- Stillbirth
At the conclusion of this chapter, the reader will be able to:
-
Define perinatal mortality and perinatal mortality rate.
-
Describe the epidemiology of stillbirths and early neonatal mortality across continents and across parts of the developing world.
-
Itemise the predisposing factors in perinatal mortality.
-
List the common causes of perinatal mortality (maternal and foetal) in the developing world.
-
Describe specific effective preventive measures for perinatal mortality in the developing world.
-
Identify key global interventions targeted at preventing perinatal and neonatal mortality in the developing world.
1 Introduction
Perinatal death remains a common pregnancy outcome in developing countries. The developing parts of the world, presently re-classified into low-income and lower middle-income countries, are characterised by large population, poor socio-economic indices and low expenditure on health. The proportion of the population living on less than $1 per day, as at 2013, was 43.6% for low-income countries, compared to less than 2.0% for high-income countries [1]. Similarly, the expenditure on health as a percentage of Gross Domestic Product (as at 2012) was 2.9% for low-income countries, compared with 9.6% for high-income countries [1]. It is not surprising, therefore, that the perinatal mortality rate in the developing world is close to 50 per 1000 births, compared to about 10 per 1000 births in the developed world [2].
The perinatal mortality rate is a sensitive index of socio-economic development and quality of prenatal, delivery and early infant care practices available in a community. In addition, perinatal mortality is a major contributor to overall childhood mortality [3]. Recent estimates suggest that 75% of all neonatal deaths occur during the first week of life and perinatal mortality accounts for about 45% of under-five mortality globally [4]. According to the World Health Organization (WHO), the perinatal period extends from the 22nd week of pregnancy till the end of the first week of life [5], and this is the most vulnerable period in life when the foetus may have difficulty transiting to independent extra-uterine life. Perinatal deaths encompass foetal deaths (still births) and early neonatal deaths (neonatal deaths in the first 7 days of life). Each year, close to 7 million perinatal deaths occur worldwide (3 to 4 million stillbirths and 3 million early neonatal deaths), with close to 99% of these deaths occurring in the low- and middle-income parts of the world [6].
The demographic picture of most developing countries provides a background to poor reproductive health indices and the unusually high perinatal mortality. For example, Nigeria has a current population of over 190 million people (2017) (ref), with a woman having an average of six births during her reproductive years. Adolescents account for 22% of the population with an adolescent fertility rate of 122 per 1000. The current contraceptive prevalence rate in Nigeria is only 15% (ref). In spite of the fact that 46% of the population reside in the urban parts of Nigeria, over 60% of babies are delivered outside health facilities with 38% skilled attendance at birth [7]. This implies that the lack of quality reproductive health care services and the unfavourable socio-economic environment contribute to the high perinatal mortality. The need to reduce this alarmingly high perinatal death rate is a critical concern in the developing world [8, 9].
This chapter aims to highlight the pattern of perinatal mortality in low- and middle-income countries with emphasis on the common risk factors and known etiological factors for perinatal deaths. Evidence-based preventive measures and interventions which are applicable to the developing world situation will be discussed.
2 Definitions
Perinatal mortality is the combination of foetal deaths (or still births) and early neonatal deaths. The stillbirth rate (SBR) is defined as the number of foetal deaths prior to or during labour per 1000 total births, while the early neonatal death rate (ENDR) refers to the number of deaths occurring within the first week of life per 1000 live births. Therefore, the perinatal mortality rate (PNMR) is defined as the total number of stillbirths and early neonatal deaths per 1000 total births. Foetal death refers to death of a product of human conception occurring after 20 weeks of gestation but prior to the complete expulsion or extraction from the mother. According to the 10th Edition of the International Classification of Diseases (ICD-10), foetal deaths are sub-divided into early (22 to 27 weeks gestation, weight > 500 g, crown-rump-length ≥ 25 cm) or late (≥28 weeks of gestation, weight ≥ 1000 g, crown-rump-length ≥ 35 cm). Therefore, foetal deaths at 22 weeks gestation or more defines stillbirth while the foetal deaths before 22 weeks gestation or weight less than 500 g define miscarriages [10, 11]. However, the definition of stillbirth using the gestational age and foetal weight at birth varies in different regions of the world, and this contributes to the variation of perinatal mortality rates recorded in the different regions of the world. For instance, whilst foetal viability is defined by 20 weeks of gestation or 500 g birth weight in the developed world, 28 weeks of gestation and above or birth weight of 700 g and above is used in developing countries. The definition accepted in various parts of the world depends on cultural disposition to foetal losses, definitions of foetal viability and availability of vital health statistics such as birth rates and death rates. Therefore, to facilitate international comparability of data, the World Health Organization uses the definition spanning 28 weeks of gestation to the first 7 days of life for perinatal deaths [10].
3 Incidence of Perinatal Mortality
Perinatal mortality rates vary from place to place in all regions of the world. In addition to the accepted definition of terms, the difference in PNMR is related to the socio-economic conditions and availability of acceptable qualitative medical services. According to the World Health Organization, PNMR was highest in the poorest parts of the world (Africa, Asia and Oceania), where it varied between 42/1000 and 56/1000 births, compared with richer parts of the world (Latin America, Europe and North Americas), where PNMR varied between 7/1000 births and 20/1000 births [12].
The pattern of PNMR in some African countries is shown in Table 4.1. The more developed countries in northern and southern Africa have relatively lower perinatal mortality rates when compared with countries in the eastern and western parts of the continent.
The 2013 Demographic and Health Survey in Nigeria showed that the regional PNMR for the southwest, southeast, south-south, northwest, northeast and north-central zones were 42/1000, 36/1000, 37/1000, 44/1000, 45/1000 and 34/1000, respectively. In addition, hospital-based perinatal mortality rates recorded from different parts of Nigeria, as shown in Table 4.2, showed that most perinatal mortality rates varied between 60/1000 births and 134/1000 births over the years. These are not remarkably different from the range of rates reported from other parts of the developing world. A multi-centre study conducted in Burkina Faso, Cote d’Ivoire, Mali, Mauritania, Niger and Senegal reported a mean perinatal mortality rate of 42/1000 [24] and 118/1000 from Kenya [25]. Interestingly, the current trend of PNMR reported from countries in Africa (Table 4.1) shows no consistent pattern across the board.
While there is no strong evidence on which to base these observations, it is plausible that there had been deliberate efforts at tackling the problem of high perinatal mortality in most places, but the degree of success recorded in countries varies. Unfortunately, recent investigations suggest that the perinatal mortality rate in some parts of Nigeria may be rising. PNMR recorded in Ilesha, southwest Nigeria, rose from 57.8/1000 in 1995 to 77.03/1000 in 2003 [15, 26]. Similarly, the rate has not changed remarkably in Lagos, from 84.4/1000 in 2004 to 84.6/1000 in 2011 [17, 27]. These observations underscore the persistently high perinatal mortality rates in parts of Nigeria.
4 Epidemiology of Perinatal Deaths
Globally , about 2.6 million children die in the first 28 days of life, and a similar number are stillborn [28]. Over 98% of these perinatal deaths occur in low- and middle-income countries. Unfortunately, most of these deaths are unrecorded because they occur in parts of the world where vital statistics are poorly kept, and notifications of perinatal deaths are rarely made for socio-cultural reasons [29]. This implies that the figures presently used for local and international epidemiology, and for planning interventions, may indeed be under-estimations.
In 2015, for every 1000 total births, 18.4 babies were delivered stillborn and two-thirds of these stillbirths occurred following intrapartum complications. Although the bulk of these stillbirths occur in low- and middle-income countries, for example 28/1000 in sub-Saharan Africa, high-income countries are not spared as the stillbirth rates vary between 1.3/1000 and 8/1000 births [30]. This implies that stillbirth is a global problem and that there is a need for global attention to reduce the scourge of this important perinatal health issue. The global stillbirth rate declined from 22.1/1000 births in 1995 to 18.9/1000 births in 2009, representing a 14% decline.
Table 4.3 shows the rate of decline in stillbirth rates in different parts of the world. In low- and middle-income countries, the greatest rate of decline in stillbirth rates occurred in South East Asia and the Western Pacific regions, compared to Africa and the Americas. The stillbirth rates appear to remain high in parts of the world where access to quality perinatal health care is poor, with inequity in the distribution of the available health resources, poor maternal health indices such as fertility rates, contraceptive use and skilled attendance at birth. Therefore, it is not surprising that more recent literature shows that more than three-quarters of global stillbirths occur in sub-Saharan Africa (40.5%) and South Asia (36.9%), while the remaining one-quarter was spread across the other regions of the world [11].
A lot still needs to be done to further reduce neonatal deaths to 12/1000 live births by the year 2030, according to the tenets of the Sustainable Development Goals [4]. In 2013, the neonatal mortality rates were highest in Africa (30.5/1000), South East Asia (25.9/1000) and the Eastern Mediterranean (25.8/1000). On the other hand, the Western Pacific, the Americas and Europe recorded significantly lower neonatal mortality rates (8.4/1000, 7.6/1000 and 6.1/1000, respectively) during the same period. Although significant progress has been made from the 1990 neonatal mortality rates, the bulk of the countries with a neonatal mortality rate above 30/1000 births in 2013 are in the African region [1]. Apart from prematurity and its complications, severe intrapartum events are the next leading causes of neonatal deaths, constituting 11% of childhood deaths. These severe intrapartum events unarguably comprise foetal hypoxia, perinatal asphyxia and birth injuries. The slowest progress in the reduction of neonatal deaths was made with regard to prematurity and sepsis [31, 32]. This implies that with more efforts directed at severe intrapartum events, both stillbirths and early neonatal deaths will be further reduced. With the advent of the Sustainable Development Goals, the 2030 target is to achieve national neonatal mortality rates of 20/1000 live births or fewer. While a hundred countries globally had already met the stated target, 29 countries, which are in the low-income countries category, will have to double their rates of progress in order to meet that target. The national stillbirth rate is also targeted at 12/1000 total births or fewer. This translates into reducing stillbirths from 2.6 million to 1.1 million and this feat requires 56 countries to at least double their rate of progress [33, 34].
5 Factors Predisposing to Perinatal Mortality
Perinatal deaths, world over, occur as a result of poor health care during pregnancy, during labour and delivery, and immediately after child birth. Factors contributing to poor maternity and early neonatal care are similar across the globe, although with varying frequencies and relative import. These factors can be classified as follows:
5.1 Environmental Factors
Rural or urban slum residence is characterised by poor housing with poor environmental hygiene as a result of poor refuse and sewage disposal and poor supply of safe water. All these factors predispose to infections in pregnancy, which may adversely affect the foetus in utero or the baby soon after birth. Getting prompt and adequate health care in rural or urban slum settings may also be impaired by poor transportation (caused by bad roads or difficult water ways), lack of electricity and water supply, lack of facilities for emergency obstetric and neonatal care, as well as personnel with adequate expertise [35]. Other important factors which may predispose to perinatal death include poverty, ignorance, harmful cultural practices and religious beliefs, all of which ultimately affect health care-seeking practices. Poor nutrition also contributes remarkably to morbidities in pregnancy, resulting in perinatal losses [36]. The effect of unfavourable health-related policy reforms has been documented to adversely influence human behaviour, particularly with regard to accessing health care, and this worsens perinatal loss in a developing economy [26].
5.2 Biosocial Factors
Extremes of reproductive age (less than 20 and greater than 35 years) are known to be associated with poor perinatal outcomes arising from complications such as hypertensive diseases, malnutrition, malaria and anaemia. These complications may explain the higher frequencies of perinatal loss among women in those age groups [37]. Indeed, the best perinatal outcome is obtained among mothers aged between 20 and 24 years. Similarly, high parity (i.e. greater than four deliveries), elderly primigravida and very young primigravida are at increased risk of pregnancy and labour complications, which, in turn, increase their risk of perinatal mortality [38, 39]. Pregnant women in the lower social classes are most at risk of perinatal deaths compared with the other social classes due to factors such as poverty, ignorance and poor access to helpful health information. The overall effects of these factors include increased risk of poor nutrition, anaemia, infections and poor utilisation of available health resources. Neonatal tetanus is a good example of a leading cause of perinatal mortality in low-income and lower-middle-income countries, which is closely related to low socio-economic status of families. Tetanus is a major contributor to perinatal deaths in Nigeria and other developing countries [40, 41]. Mothers of newborn infants with tetanus in various parts of Nigeria have been repeatedly shown to be poor with no record of quality prenatal care, lack of adequate immunisation against tetanus during pregnancy and childbirth in unhygienic environments [42,43,44]. Similarly, mothers who did not register for facility-based prenatal care (unbooked) are more vulnerable to perinatal mortality compared with booked mothers [45]. In addition, both maternal obesity and short stature predispose to perinatal deaths through difficult labour and the various associated mechanical and hypoxic injuries in the baby [46, 47]. Birth weight and intra-uterine growth status also contribute to perinatal deaths. Babies with extremes of abnormal birth weight (low birth weight and macrosomic babies) and extremes of abnormal intra-uterine growth (small for gestational age or large for gestational age babies) have higher risks of complications, which frequently result in perinatal mortality [48].
5.3 Obstetric and Gynaecological Factors
Poor utilisation of family planning services, antenatal care services and quality delivery services characterise low- and middle-income countries, where economic indices are poor and fertility rate per woman is high, as shown in Table 4.4.
Previous abortion increases the risk of perinatal death in subsequent pregnancies [49]. Other important obstetric and gynaecological determinants of perinatal death include pregnancy complications, such as antepartum haemorrhage, abnormal labour and assisted deliveries. Assisted deliveries contribute to high perinatal mortality through higher risk of mechanical injuries to viscera and concealed haemorrhages. Other obstetric and gynaecological disorders predisposing to perinatal mortality include severe maternal or intrauterine infection, malposition, malpresentation and abnormal labour, which predispose to preterm birth and low birth weight with various complications such as perinatal asphyxia, intraventricular haemorrhage, idiopathic respiratory distress, hypothermia, hypoglycaemia, recurrent apnoea and septicaemia [50, 51].
6 Causes of Perinatal Mortality
The causes of perinatal mortality may be broadly classified into direct and indirect: the former are mainly medical disorders in the mother, foetus or baby, which may cause foetal or early neonatal death. The indirect causes are biological, cultural, socio-economic and anthropological problems, which enhance the occurrence and effects of the direct causes of perinatal death. The two classes of causes of perinatal deaths are usually interwoven, such that it is difficult in the developing world to ascribe perinatal death to a single factor. Unfortunately, most cases of foetal or neonatal death occur outside the hospital; thus, the exact causes of the foetal death may not be known.
6.1 Direct Causes
6.1.1 Prolonged Obstructed Labour
This is common in developing countries for reasons such as poor attendance of antenatal care and poor utilisation of quality delivery services [52]. The obstruction to foetal passage frequently follows cephalopelvic disproportion, either from contracted pelvis or a relatively big baby. The strong uterine contractions over a long period of time impair placental functions and cause intrapartum foetal hypoxic-ischaemic injury and perinatal asphyxia.
6.1.2 Anaemia and Malnutrition
Malaria , iron and folate deficiency, and haemoglobinopathies are common causes of anaemia and malnutrition in pregnancy. These factors cause placental dysfunction, impair nutrient supply to the foetus and cause restriction of foetal growth, thus predisposing to poor pregnancy outcomes [36]. The leading and synergistic roles of malaria, malnutrition and anaemia in the aetiology of intrauterine growth restriction and preterm delivery are well known [53]. Added to this burden is HIV infection, which further enhances the susceptibility of the placenta to the effects of malaria in pregnancy [54]. In addition, perinatal death from maternal anaemia in pregnancy is associated with foetal anaemia, premature labour, low birth weight and intrapartum hypoxia, causing stillbirth or early neonatal death [55]. Obesity is also becoming a matter of concern in the developing world despite widespread under-nutrition, due to westernisation of life styles and increasing consumption of unhealthy foods. Maternal obesity is associated with higher risk of hypertensive disorders in pregnancy, shoulder dystocia, foetal distress, stillbirth and early neonatal death from severe perinatal asphyxia [47].
6.1.3 Hypertensive Diseases of Pregnancy
Pre-eclampsia , eclampsia and pre-gestational essential hypertension are associated with higher rates of perinatal mortality. Eclampsia has been shown to cause more stillbirths than early neonatal deaths in Nigeria [56]. Perinatal death rate increases with the severity of the disease, and inversely with the gestational age at the onset of the disease [57, 58]. High perinatal loss in hypertensive diseases is related to macro-vascular damage, impaired placental blood flow or premature placental separation. These factors cause intrauterine hypoxia, intrauterine growth restriction and preterm delivery [59].
6.1.4 Antepartum Haemorrhage
Bleeding in pregnancy predisposes to perinatal death [60] from compromised foetal circulation, anaemia and intra-uterine hypoxia. Placental abruption, in particular, causes premature delivery in settings equipped for emergency obstetric practice, or intra-uterine death where such facilities are lacking. Other associated complications of haemorrhage which may contribute to perinatal deaths include congenital malformations (where bleeding occurs early in pregnancy), intra-uterine hypoxia resulting in perinatal asphyxia, neonatal anaemia and early-onset sepsis. The latter conditions may cause perinatal deaths from shock, congestive cardiac failure or multiple organ failure.
6.1.5 Diabetes Mellitus in Pregnancy
Sudden and unexplained foetal and early neonatal death occurs in about 30% of pregnancies complicated by diabetes mellitus [61]. However, improved hospital-based care for diabetes in pregnancy has drastically reduced the risk of associated adverse perinatal outcome. Although gestational diabetes increases the risk of preterm delivery [62], the perinatal mortality rate is higher among women with pre-gestational diabetes mellitus, especially when it is poorly controlled, compared with the gestational type [63]. In addition to the known co-existence of diabetes in pregnancy and hypertensive disorders [64], the common complications of diabetes mellitus in pregnancy which contribute to perinatal death include hydramnios, hydrops fetalis, congenital malformations, particularly of the intestine and heart, foetal macrosomia, intrauterine growth restriction and preterm birth with respiratory distress syndrome. Perinatal asphyxia and other forms of birth injury may be caused by difficulty delivery as a result of foetal macrosomia. However, foetal macrosomia is not universal in diabetes during pregnancy, as foetal size depends on the degree of glycaemic control and integrity of utero-placental circulation. With poor glycaemic control of diabetes in pregnancy, microvascular damage results in poor placental blood flow and secondary intra-uterine growth restriction. Both macrosomia and small-for-gestational age predispose to intrapartum stillbirth, and increased risk of early neonatal death from the complications of asphyxia.
6.1.6 Birth Trauma
Birth trauma contributes remarkably to perinatal loss, as factors predisposing babies to birth trauma such as macrosomia, cephalopelvic disproportion, shoulder dystocia, prolonged or difficult labour, precipitous delivery, abnormal presentations and instrumental delivery are frequent obstetric occurrences in parts of the developing world [65]. Soft tissue injuries are more frequently associated with perinatal deaths compared to bony or neuronal injuries. Soft tissue injuries such as intraventricular, cephalohaematoma, sub-galeal haemorrhage and visceral rupture, particularly adrenal gland rupture, may also cause life-threatening complications.
6.1.7 Infections
Apart from causing systemic inflammatory response, which may be harmful to the mother and the foetus through circulatory failure and multi-organ failure, systemic bacterial sepsis in pregnancy may cause perinatal death through anaemia and intra-uterine hypoxia. Localised infections in the gastrointestinal and genitourinary tract are also known to precipitate preterm delivery [66]. Prolonged rupture of foetal membranes or preterm premature rupture of membranes cause ascending intra-uterine infections, which predispose to perinatal deaths [67]. Intra-uterine infection with TORCHES organisms (Rubella, Toxoplasma gondi, Treponema pallidum, Herpes simplex and Epstein-Barr virus) are common in the developing world due to poor hygiene and poverty. These organisms are capable of causing perinatal deaths through severe congenital malformations, intrauterine growth restriction and preterm delivery. Perinatal HIV infection is important because it causes embryopathy and congenital malformations, with remarkably higher risk of perinatal mortality from intrauterine growth restriction and preterm delivery. Pregnant women who are sero-positive for HIV have been shown to be more likely to have preterm delivery, low-birth-weight babies, intrauterine growth restriction and perinatal mortality [68].
6.1.8 Prematurity
Perinatal death is jointly influenced by birth weight and gestational age. Perinatal mortality has an inverse relationship with gestational age and birth weight. Indeed, perinatal mortality increases in very preterm (less than 34 weeks) and very-low-birth-weight babies (less than 1500 g). Preterm delivery has been shown to be the leading single cause of perinatal deaths in the developing world, with contribution as high as 40% in India [69]. These babies are most at risk of severe conditions such as asphyxia, respiratory distress syndrome, septicaemia, hyperbilirubinaemia, hypothermia, hypoglycaemia, intraventricular haemorrhage, apnoea, anaemia, congenital cardiac malformations and serious gastrointestinal disorders such as necrotising enterocolitis [48, 50, 51]. These complications often require highly specialised expertise, huge infrastructural support and intensive care facilities, which are almost non-existent in the parts of the world where the incidence of preterm birth is paradoxically high. Therefore, preterm birth is associated with a high rate of perinatal death in the developing countries.
6.1.9 Intrauterine Growth Restriction
Intrauterine growth restriction is an important cause of perinatal mortality [6, 70]. Many maternal diseases in pregnancy which affect the utero-placental circulation cause intrauterine growth restriction. Other causes include specific intrinsic foetal disorders such as chromosomal anomalies, particularly the trisomies. High perinatal loss associated with IUGR is usually due to intrapartum asphyxia, hypoglycaemia, hypothermia, hyperviscosity syndrome from polycythaemia, hyperbilirubinaemia and congenital malformations, particularly, of the heart.
6.1.10 Malpresentation
Breech presentation is the commonest abnormal presentation and, like others such as shoulder, face, brow, transverse and cord presentation, accounts for high perinatal loss. Malpresentation may be a cause of prolonged or obstructed labour with a significant risk of intrapartum hypoxia, asphyxia and mechanical birth injuries. Inappropriate mode of delivery may contribute to high perinatal loss associated with malpresentation. This is because babies with abnormal presentations are usually risky to deliver, and experienced and well-trained obstetricians are required. The lack of the required equipment, and scarcity of highly skilled specialists, increase perinatal mortality in babies with malpresentation.
6.1.11 Perinatal Asphyxia
Most cases of stillbirth are caused by severe intrapartum events. Foetal loss in labour usually occurs as a result of intrapartum hypoxia due to sudden oxygen deprivation to the foetus, usually from severe compromise of the utero-placental circuit. Therefore, complications of pregnancy and labour such as hypoxic maternal conditions, post-maturity, intrapartum bleeding from placenta praevia, prolonged obstructed labour and malpresentation, particularly breech delivery, which are associated with intrapartum hypoxia, cause foetal death, and consequently, increased perinatal mortality.
Undue stress of labour associated with trial of labour or abnormal uterine action, and difficult assisted delivery, may be associated with stillbirth. In early neonatal life, the effects of perinatal asphyxia, which increase the chances of perinatal death, include hypoxic-ischaemic encephalopathy, apnoea, intracranial haemorrhage, pulmonary haemorrhage, cardiac failure, consumptive coagulopathy, hypothermia and hypoglycaemia [71].
6.1.12 Post Maturity
Perinatal loss in pregnancies prolonged beyond 42 weeks is three times higher than in pregnancies ending between 38 and 42 weeks. The decline in placental function, in some cases of macrosomic foetus, coupled with the stress of labour, makes post-term foetuses more susceptible to perinatal death.
6.2 Indirect Causes
Studies have shown that low socio-economic status is associated with increased risk of poor perinatal outcome [72]. Some of the reasons why the poor tend to have poorer pregnancy outcomes include poor access to health services, either in terms of physical location and transportation difficulties or in terms of cost, in the absence of social supports. Other factors include ignorance from poor access to helpful health information, poor feeding, poor hygiene, higher likelihood of pregnancy complications bordering on the state of maternal health and poor health care-seeking behaviours [73]. In the developing countries where adult literacy level averages 60% [1], it is commonplace for pregnant women to decline operative deliveries in the face of complicated labour. The rates of caesarean delivery in different parts of the world are depicted in Table 4.4, and the poor parts of the world (Africa and South East Asia) have the lowest rates of caesarean delivery compared to the more advanced countries. Studies in Nigeria have also shown the poor acceptability of caesarean section by pregnant women across various parts of the country [74,75,76]. The poor acceptability of caesarean section cannot be separated from low maternal education and socio-cultural disapproval by the family. The poor acceptability of caesarean section has implications for perinatal survival.
The socio-economic status of the inhabitants of any country influences perinatal mortality. For instance, perinatal mortality is seven times higher amongst the low socio-economic group in India than in the higher social class [77]. Malnutrition and poverty serve as major factors predisposing to poor perinatal outcome. Maternal malnutrition may arise from poverty, or from food insecurity in the form of drought and famine during natural disasters, or occurring in situations of war, civil strife, displacement and refuge, all of which are common in low-income and lower-middle-income countries compared to upper middle- and high-income countries. Poor maternal nutrition impairs foetal nutrition, retards intrauterine growth and causes low birth weight. It also worsens the depressed immunity of pregnancy, thus, predisposing to infections, which may either precipitate preterm delivery or cause foetal death. Chronic malnutrition, especially in the form of hypovitaminosis D, predisposes to maternal short stature, deformed pelvic bones and contracted pelvis, which will ultimately predispose to obstructed labour. Inequity in the distribution of health resources in the poor parts of the world contributes to the burden of high perinatal mortality in such places. Compared to urban areas, rural areas where the larger proportion of the population reside, usually lack personnel and equipment required to manage emergency obstetric services. Due to poor planning and inefficient health policies, most skilled personnel are located in urban areas, particularly in the secondary and tertiary levels of care, where they are less needed. This pattern of distribution further reduces the chances of survival of a large number of babies delivered in rural and less developed areas.
Appropriate health care-seeking behaviour is strongly influenced by socio-economic and cultural factors, culminating in delays in receiving appropriate care. Prominent among these factors is the patriarchal family system in most parts of Africa and Asia, by which the power to take decisions on when to seek care, where to seek care and what type of care to seek rests squarely on the male head of the family [78]. Therefore, the pregnant woman is deprived of the right to take decisions concerning her health and the pregnancy. The decision of the family head on when to seek medical help may be inappropriate, or may come too late, thus predisposing to poor perinatal outcomes. Even when the decision to seek appropriate obstetric care is eventually taken, there may be other confounding challenges such as transportation difficulties and lack of funds to contend with. These factors further worsen the delay in seeking quality care, and increase the risk of perinatal death. In addition, certain cultures in some developing countries permit teenage pregnancy, and make facility-delivery culturally unattractive for primigravida women. Teenage girls, who are immature in height and pelvic size, are exposed to complications of pregnancy and delivery with an overall increase in perinatal loss [37]. Other non-specific variables indirectly contributing to perinatal deaths include extremes of maternal age (<18 years and >35 years), high parity, multiple gestation and poor utilisation of antenatal care services. Women aged 35 years or more have been shown to have higher risk of perinatal mortality from obstructed labour compared to those aged 20 to 34 years [79]. Similarly, expectant mothers who did not receive antenatal care have been shown to be at higher risk of preterm birth, small-for-gestational babies and perinatal mortality, compared with mothers who were booked for antenatal care [45]. In addition, birth interval between 18 and 23 months is associated with the lowest risk of adverse perinatal outcome [79]. Female genital mutilation is a strong cultural practice in most parts of the developing world. This practice increases the risk of obstructed labour due to the restrictive effect of the scarred vulva, and also predisposes to perinatal loss in poor settings in the absence of highly skilled obstetric care. High perinatal mortality is associated with multiple gestations as a result of higher likelihood of preterm delivery and low birth weight in the babies. The second twin has been shown to be more susceptible to severe intrapartum events and mortality, possibly from partial placental separation and cord accidents following the delivery of the first twin [80]. Therefore, efforts must be made to identify these indirect causes of perinatal loss during antenatal care, and the delivery must be supervised to minimise perinatal losses.
7 Prevention
7.1 Primary Prevention
The general population in the low- and middle-income countries needs to be educated about the burden of perinatal deaths and the methods available to tackle the problem. This intervention should be community based and client focused, using mass media methods of health campaigns. This intervention is meant to improve the utilisation of the available health services, improve health during pregnancy and childbirth, accept life-saving delivery methods including caesarean section and stop harmful cultural practices, and to enhance maternal and neonatal outcomes of pregnancies. Such a community approach to perinatal health has been shown to reduce maternal morbidity, neonatal mortality, stillbirth rate and perinatal mortality, and to increase referrals to health facilities [81]. Similarly, educational interventions have been shown to improve child care practices in Tanzania [82]. Family planning and birth control interventions are helpful with adequate child spacing, enhanced maternal health, better family preparedness for pregnancy and child birth, and better pregnancy outcomes. This requires outreach programmes on maternal and child health that will incorporate family planning services as suggested [83]. Family planning services should be targeted at teenagers, the elderly, the excessively multiparous and those with short birth intervals, who are most at risk of poor perinatal outcome [84]. Nutritional interventions should start very early in childhood through adolescence, without sex discrimination, in order to prevent short maternal stature and small-for-gestational age babies, and to improve perinatal survival. Improved personal and environmental hygiene practices, both at home and in health facilities, are essential in the prevention of infections and infestations which may threaten perinatal survival [85]. The practice of clean birthing would reduce the risk of early-onset sepsis, which is a major contributor to perinatal mortality in the developing world.
The combination of poverty, ignorance and harmful cultural practices represents a major risk factor for perinatal mortality. Therefore, educational qualification, social status and the financial empowerment of mothers should be enhanced to improve their health status and to reduce the risk of perinatal mortality. Specially packaged interventions to improve perinatal survival should be targeted at the socially disadvantaged parts of the community, using good road networks, and affordable and safe means of transportation.
Furthermore, in order to effectively reduce perinatal mortality, efforts should be concentrated on three levels of participants. The first level is the health team, whose members must receive adequate training relevant to the health needs of the community, and be trained to deliver health education interventions. An additional task of collecting data and disseminating information on perinatal deaths should be routinely performed by the health team. Second, the government agencies and health policy makers must formulate appropriate policies to allow and encourage universal formal education. Finally, the community must be mobilised and sensitised to use quality and safe health services, invest in their own health, and raise resources to facilitate safe pregnancy and childbirth.
7.2 Secondary Prevention
Secondary prevention involves the prevention of perinatal loss through the establishment of properly organised and efficient antenatal care services. The early identification of high-risk pregnancies through an effective screening system and timely community-to-facility referral or inter-facility referral is essential. A major step towards the secondary prevention of perinatal deaths is the provision of skilled health workers to serve hard-to-reach areas where poverty, ignorance and social disadvantage make accessibility of quality maternity services difficult. Community health workers have been shown to have roles in providing pregnancy and childbirth care, mobilising communities to embrace life-saving interventions for care during labour and delivery, and changing some of the long-standing harmful practices on newborn care, especially for poor families [86, 87]. Successful actualisation of these roles requires innovative community based strategies and health system strengthening. The Midwives Service Scheme was introduced by the Nigerian government to increase accessibility to quality and safe obstetric care in the rural and socially disadvantaged parts of the country [88]. This scheme addresses the twin problem of inequity in the distribution of health resources, and poor obstetric and perinatal outcomes [89]. In addition, efforts should be made to engage traditional birth attendants in frequent training programmes, preferably, with incentives attached. The training of this group of care providers on safe clean delivery and newborn resuscitation has been shown to reduce neonatal mortality by almost half, though more efforts are required with respect to stillbirth and perinatal death rates [90]. With the introduction of the Focused Antenatal Care system, emphasis includes Birth Preparedness and Complications Readiness (BP/CP). This entails important decision-making before the onset of labour. The components include the identification of danger signs in pregnancy, identifying a health worker to attend labour and take safe decisions, saving money in preparation for delivery, arranging transport system in case referral becomes inevitable, and obtaining the support of the family and relations ahead of confinement [91]. Where home delivery is preferred, this can be planned ahead with the appropriate arrangements for prompt referral in case of emergencies. Efforts should be made to ensure that every delivery is supervised and attended by people skilled in basic live-saving skills, including neonatal resuscitation. It is desirable that every health worker should be skilled in neonatal resuscitation, particularly with bag and mask ventilation. This would reduce the number of babies lost to intrapartum hypoxia through stillbirth or early neonatal death. In Nigeria, some professional bodies now organise neonatal resuscitation training programme for nurse-midwives and physicians on a national scale and Help the Baby Breathe training programmes at the lower tiers of healthcare [92]. These efforts have been shown to be helpful and should be entrenched in national health policy.
For pregnancies at risk of preterm delivery, the current emphasis is on the prevention of preterm labour, and improved quality care for prematurely delivered babies. Tocolysis using magnesium sulphate is recommended by the WHO for prolonging pregnancies and protecting the immature foetal brain [93]. It has the advantage of reducing the risk of cerebral palsy among infants delivered preterm [94]. The other components of the management of preterm labour as recommended by the WHO include the use of antenatal corticosteroid therapy to improve lung maturity of the foetus and prevent idiopathic respiratory distress syndrome, as well as erythromycin therapy for foetuses at risk of sepsis [93]. Antenatal corticosteroids therapy is most useful when administered within 7 days of preterm delivery [95]. Other important components of care for the preterm infant, which have been found to reduce mortality by half among babies weighing less than 2 kg, include rapid and effective resuscitation, thermoregulation using the Kangaroo Mother Care Technique and feeding supports [96]. These measures cannot be separated from Essential Newborn Care, which is a key component of Every Newborn Action Plan. The plan includes the strategies of care at birth (to prevent intrapartum hypoxia), and care of small and sick newborn babies (to prevent deaths from prematurity, infections, jaundice) [97]. The focus of Essential Newborn Care includes basic preventive newborn care (support to breathe at birth, clean delivery, temperature maintenance, immediate exclusive breastfeeding, and eye and cord care), early detection of danger signs in the newborn, and treatment of key morbidities in early neonatal life, with emphasis on sepsis and asphyxia [98].
7.3 Tertiary Prevention
Cardiopulmonary supports are crucial to the survival of preterm and other critically ill babies. The facilities required for mechanical ventilation, including exogenous or synthetic surfactant, are usually expensive and may not be affordable for poor families. This strongly calls for the establishment of a special government funding system for such specialised care, at least on a regional basis, with an efficient referral system attached to it. In addition, community-based health insurance systems, which would subsidise the cost of specialised care like neonatal intensive care, may also be instituted to alleviate the cost of care of high-risk infants, to encourage presentation at well-equipped facilities for the desired care, and to minimise perinatal deaths.
The WHO estimated that 1.1 million stillbirths could be prevented using interventions such as comprehensive emergency obstetric and neonatal care, syphilis detection and treatment, detection and management of hypertension during pregnancy, detection and management of foetal growth restriction, identification and induction for mothers >41 weeks gestation, malaria prevention, including treated bed-nets and intermittent preventive treatment for malaria in pregnancy, folic acid fortification before conception, and detection and management of diabetes in pregnancy [6].
One of the major challenges in planning the reduction of stillbirths is inadequate data from the poor registration of births and deaths in low- and middle-income countries [10, 99]. Even in settings where data are available, the use of several classification systems, and multiple definitions of foetal death and stillbirth makes the comparison of the available data with other international datasets challenging. Therefore, international health agencies concerned with obstetric and perinatal health need to agree on a harmonised system of definitions and classifications, possibly including investigations such as post-mortem examinations and histologic studies [99]. In addition, the existing health systems need to be strengthened for more efficient delivery of perinatal services using the deployment of highly skilled personnel and task-shifting in hard-to-reach areas. Community-to-facility referral should be strengthened to save many foetuses with intrapartum hypoxia. Clinical genetics and paediatric surgical services should be made available to supplement obstetric and neonatal care services, particularly for babies with congenital malformations. This networking between specialties should be supported in ways that babies with congenital malformations may still be helped to survive with good quality of life.
8 Conclusion
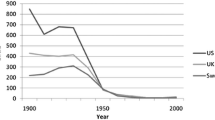
The bulk of perinatal deaths occur in the poorer parts of the world – the low- and middle-income countries. Early neonatal deaths also form about a quarter of under-five deaths and most cases occur in the perinatal period. These facts reflect the relationship between economic realities and access to good health and development. Therefore, global attention is shifting towards addressing these health-related socio-economic inadequacies. Although several evidence-based interventions and action plans are coming up to strengthen the existing weak health system in the resource-poor part of the world, and to improve the outcome of pregnancies, reduce stillbirth rates and increase the survival of newborn babies, improved literacy through formal education of women, and women empowerment through better employment and better rights of decision-making, are also essential. With improved education, the standard of living will equally improve and so will the access to health services. Government policies should aim at improved funding of health services through participatory local health insurance schemes. More importantly, interventions which had caused a sharp decline in perinatal mortality rates in high-income countries should be replicated in low- and middle-income countries.
References
WHO. World Health Statistics 2015. World Health Organization; 2015.
WHO. Neonatal and perinatal mortality: Country, Regional and Global Estimates. World Health Organization; 2006.
WHO. The World Health Report 2005: make every mother and child count. Geneva: World Health Organization; 2005.
WHO. Media Centre. Children: reducing mortality. Fact sheet. Updated January 2016.
Wikipedia. Perinatal mortality. Available at https://en.m.wikipedia.org/wiki/Perinatal_mortality.
WHO. 2.6 million babies stillborn in 2009. WHO News release 2011. Available at http://www.who.int/mediacentre/news/release/2011/stillbirths_20110414/en/.
UNICEF. State of the World’s Children 2015.
Liu L, Johnson HL, Cousens S, Perin J, Scott S, Lawn JE, Rudan I, Campbell H, et al. Global, regional and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379(9832):151–61.
Lawn JE, Kerber K, Enweronu-Laryea C, Cousens S. 3.6 million neonatal deaths – What is progressing and what is not? Semin Perinatol. 2010;34(6):371–86.
Barfield WD. Committee on Foetus and Newborn. Clinical reports – Standard Terminology for fetal, infant and perinatal deaths. Pediatrics. 2011;128(1):177–81.
Blencowe H, Cousens S, Jassir FB, Say L, Chou D, Mathers C, Hogan D, et al. National, regional and worldwide estimates of Stillbirth Rate in 2015, with trends from 2000: a systematic review. Lancet Glob Health. 2016;4:e98–108.
WHO. Perinatal mortality: country, regional and global estimates. World Health Organization 2007.
Adeleye JA. A two-year study of caesarean section and perinatal mortality at the University College Hospital, Ibadan, Nigeria. East Afr Med J. 1982;59(6):383–9.
Njokanma OF, Sule-Odu OA, Akesode FA. Perinatal mortality at the Ogun State University Teaching Hospital, Sagamu, Nigeria. J Trop Paediatr. 1994;40:78–81.
Kuti O, Orji EO, Ogunlola IO. Analysis of perinatal mortality in a Nigerian Teaching Hospital. J Obst Gynaecol. 2003;23(5):512–4.
Adimora GN, Odetunde IO. Perinatal mortality in University of Nigeria Teaching Hospital (UNTH), Enugu at the end of the last millennium. Niger J Clin Pract. 2007;10(1):19–23.
Ekure EN, Ezeaka VC, Iroha E, Egri-Okwaji MTC. Prospective audit of perinatal mortality among inborn babies in a tertiary health centre in Lagos, Nigeria. Niger J Clin Pract. 2011;14(1):88–94.
Ibekwe P, Ugboma H, Onyire N, Muoneke U. perinatal mortality in southern Nigeria: less than half a decade to the MDG. Ann Med Health Sci Res. 2011;1(2):215–22.
Fawole AO, Shah A, Tongo O, Dara K, El-Ladan AM, Umezulike AU, et al. determinants of perinatal mortality in Nigeria. Int J Gynecol Obstet. 2011;114(1):37–42.
Suleiman BM, Mokuolu OA, Adesiyun OO. Pattern of perinatal mortality in babies delivered at the University of Ilorin Teaching Hospital, Ilorin, Nigeria. West Afr J Med. 2012;31(2):102–8.
Mairami AB, Audu LI, Aikhionbare HA. Risk factors for perinatal deaths in Abuja, Nigeria. Peak J Med Med Res. 2014;2(3):23–32.
Suleiman MB, Mokuolu OA. Perinatal mortality in a Northwestern Nigerian City: a wake-up call. Front Pediatr. 2014;2:105.
Igberase GO. Perinatal mortality in a rural referral hospital in the Niger Delta, Nigeria. Afr J Med Health Sci. 2014;13(1):47–50.
Chalumeau M, Salanave B, Bouvier-Colle MH, de Bernis L, Prua A, Breart G. Risk factors for perinatal mortality in West Africa: a population-based study of 20326 pregnancies. Acta Paediatr. 2000;89(9):1115–21.
Weiner R, Ronsmans C, Dorman E, Jilo H, Muhoro A, Shulman C. Labour complications remains the most important risk factors for perinatal mortality in rural Kenya. Bull World Health Org. 2003;81(7):1–6.
Owa JA, Osinaike AI, Makinde O. Trends in utilisation of obstetric care at Wesley Guild Hospital, Ilesa, Nigeria. Effects of a depressed economy. Trop Geogr Med. 1995;47(2):86–8.
Ekure EN, Iroha EO, Egri-Okwaji MTC, Ogedengbe OK. Perinatal mortality at the close of the 20th century in Lagos University Teaching Hospital. Niger J Paediatr. 2004;31(1):14–8.
Richardus JH, Graafmans WC, Verloove-Vanhorick SP, Mackenbach JP. The perinatal mortality rate as an indicator of quality of care in international comparisons. Med Care. 1998;36(1):54.
UNICEF. Levels and trends in child mortality report. UNICEF, 2010.
WHO. Sexual and reproductive health. The Neglected tragedy of stillbirths. World Health Organization. Available at http://www.who.int/reproductivehealth/topics/maternal_perinatal/stillbirth/en/.
Lawn J. Millennium Development Goals to Sustainable Development Goals: What next for women and children health? Available at www.imperial.ac.uk/media/imperial-college/centre-for-international-child-health/public/Joy_CICH_Jan2016-keynote.pdf Accessed on 22 Dec 2018.
Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn J, et al. Global, regional and national causes of child mortality in 2000-2013 with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385(9966):430–40.
De Bernis L, Kinney MV, Stones W, Hoope-Bender P, Vivio D, Leishner SH. Stillbirths: ending preventable deaths by 2030. Lancet. 2016;387(10019):703–16.
WHO/UNICEF. Every newborn action plan. 2014.
Harrison KA, Briggs ND, Oruamabo RS. Technology free obstetrics. Letter to Editor. Lancet. 1991;358:383.
Abu-Saad K, Fraser D. Maternal nutrition and birth outcomes. Epidemiol Rev. 2010;32(1):5–25.
Ogunlesi TA, Ayeni VA, Jagun OE, Ogunfowora OB. Socio-clinical factors related to the perinatal outcome of teenage pregnancies in a Nigerian Teaching Hospital. Niger J Paediatr. 2013;40(3):290–4.
Kwast BE. Reduction of maternal and perinatal mortality in rural and pre-urban settings. What works? Eur J Obst Gynaecol Reprod Biol. 1996;69(1):47–53.
Adedoyin MA, Adetoro OO. Pregnancy and its outcome among teenage mothers in Ilorin. Nigeria East Afr Med J. 1989;66(7):448–52.
Oruamabo RS. Neonatal tetanus in Nigeria: does it still pose a major threat to neonatal survival? Arch Dis Child. 2007;92(1):9–10.
Ibinda F, Bauni E, Kariuki SM, Fegan G, Lewa J, Mwikamba M, Boga M, et al. incidence and risk factors for neonatal tetanus in admission to Kilifi County Hospital, Kenya. PLoS One. 2015;10(4):e0122606.
Ogunlesi TA, Okeniyi JAO, Owa JA, Oyedeji GA. Neonatal tetanus at the close of the 20th century in Ilesa, Nigeria. Trop Doct. 2007;37:165–7.
Fetuga MB, Ogunlesi TA, Adekanmbi AF, Runsewe-Abiodun TI, Ogunfowora OB. Neonatal Tetanus in Sagamu, Nigeria during the Expanded Programme on Immunisation and National Programme on Immunisation eras: a comparative analysis. Int J Pediatr Neonatol. 2010;12:1. Available at http://www.ispub.com/ijpn/.
Alhaji MA, Bello MA, Elechi HA, Akuhwa RT, Bukar FL, Ibrahim HA. A review of neonatal tetanus in University of Maiduguri Teaching Hospital, Northeastern Nigeria. Niger Med J. 2013;54(6):398–401.
Owolabi AT, Fatusi AO, Kuti O, Adeyemi A, Faturoti SO, Obianjunwa PO. Maternal complications and perinatal outcomes in booked and unbooked Nigerian mothers. Singap Med J. 2008;49(7):526.
Ozumba BC, Ucheagbu H. Incidence and management of obstructed labour in eastern Nigeria. Aust New Zealand J Obst Gynaecol. 1991;31(3):213–6.
Cedergren MI. Maternal morbid obesity and the risk of adverse pregnancy outcome. Obstet Gynecol. 2004;103(2):219–24.
KhoshnoodShariati M, Karmi Z, Rezaienejad M, Basiri A, Torkestani F, SalehGargari S. Perinatal complications associated with preterm deliveries at 24 to 33 weeks and 6 days gestation (2011-2012): a hospital-based retrospective study. Iran J Reprod Med. 2015;13(11):697–702.
Okonofua FE, Onwudiegwu U, Odutayo R. Pregnancy outcome after illegal induced abortion in Nigeria, a retrospective controlled historical study. Afr J Med Med Sci. 1994;23(2):165–9.
Ogunlesi TA, Ogunfowora OB. Predictors of mortality in neonatal septicaemia in an under-resourced setting. J Natl Med Assoc. 2010;102(10):915–21.
Adegoke SA, Ayoola AO, Bankole KP, Ogunlesi TA. Intravenous haemorrhage in newborns weighing <1500g: Epidemiology and short-term outcome in a resource-poor setting. Ann Trop Med Pub Health. 2014;7(1):48–54.
Ali AA, Adam I. Maternal and perinatal outcome of obstructed labour in Kassala Hospital, Sudan. J Obst Gynecol. 2010;30(4):376–7.
Uneke CJ. Impact of placental Plasmodium falciparum malaria on pregnancy and perinatal outcome in sub-Saharan Africa. Yale J Biol Med. 2007;80(2):39–50.
Ticconi C, Mapfuno M, Dorrucci M, Naha N, Tarira E, Pietropolli A, Rezza G. Effect of maternal HIV and malaria infection on pregnancy and perinatal outcome in Zimbabwe. J AIDS. 2003;34(3):289–94.
Adam I, Babiker S, Mohammed AA, Salih MM, Prins MH, Zaki ZM. Low body mass index, anaemia and poor perinatal outcome in a rural hospital in Eastern Sudan. J Trop Pediatr. 2008;54(3):202–4.
Adamu AN, Ekele BA, Ahmed Y, Mohammed BA, Isezuo SA, Abdullahi AA. Pregnancy outcome in women with eclampsia at a tertiary centre in northern Nigeria. Afr J Med Med Sci. 2012;41(2):211–9.
Gaugler-Senden IPM, Huijsson AG, Visser W, Stugers EAP, de Groot CJM. Maternal and perinatal outcome of pre-eclampsia with an onset before 24 weeks gestation. Eur J Obstet Gynaecol Reprod Biol. 2006;128(1):216–21.
Lisonkova S, Joseph KS. Incidence of pre-eclampsia: risk factors and outcomes associated with early versus late-onset disease. Am J Obstet Gynecol. 2013;209(6):544e1–e12.
Njokanma OF, Olanrewaju DM. A study of neonatal deaths at the Ogun State University Teaching Hospital, Sagamu, Nigeria. J Trop Med Hyg. 1995;98(3):155–60.
Kalter HD, Khazen RR, Barghouthi M, Odeh M. Prospective community-based cluster census and case-control study of stillbirths and neonatal deaths in the West Bank and Gaza Strip. Paediatr Perinat Epidemiol. 2008;22(4):321–33.
Maouris P. Reducing perinatal mortality in Vila Central Hospital, Vanuatu. Papau New Guinea Med J. 1994;35(5):495–501.
Gashim TI. Gestational diabetes mellitus: maternal and perinatal outcomes in 220 Saudi women. Oman Med J. 2012;27(2):140–4.
Abu-Heija AT, Al-Bash M, Mathew M. Gestational and pregestational diabetes mellitus in Omani Women: Comparison of obstetric and perinatal outcomes. Sultan Qaboos Univ Med J. 2015;15(4):e496–500.
Ozumba BC, Obi SN, Oli JM. Diabetes mellitus in pregnancy in an African population. Int J Gynecol Obstet. 2004;84(2):114–9.
Njokanma OF, Kehinde OA. Mechanical birth trauma – an evaluation of predisposing factors at the Ogun State University Teaching Hospital, Sagamu. Niger J Paediatr. 2002;29:61–5.
Ananya D, Subrat P, Ahanthem SS, Sourah GD, BhanuPratap SG. Preterm birth: analysis of risk factors and neonatal outcome. Gynecol Obstet Case Rep. 2015;1:1. Available at www.gynaecology-obstetrics.imedpub.com.
Yu H, Wang X, Gao H, You Y, Xing A. Perinatal outcome outcomes of pregnancies complicated by preterm premature rupture of the membranes before 34 weeks of gestation in a tertiary centre in China: a retrospective review. Biosci Trends. 2015;9(1):35–41.
Ellis J, Williams H, Graves W, Lindsay MK. Human immunodeficiency virus infection is a risk factor for adverse perinatal outcomes. Am J Obstet Gynaecol. 2002;186(5):903–6.
Viswanath K, Ps R, Charkaborty A, Prasad JH, Minz S, George K. A community-based case-control study on determination of perinatal mortality in a tribal population of southern India. Rural Remote Health. 2015;15(3):3388.
Simchen MJ, Beiner ME, Strauss-Liviathan N, Dulitzky M, Kuint J, Mashiach S, Schiff E. Neonatal outcome in growth-restricted versus appropriately grown preterm infants. Am J Perinatol. 2000;17(4):187–92.
Ogunfowora OB, Ogunlesi TA, Fetuga MB, Oyinlade AO. Clinical manifestations and outcome of hospitalised babies with birth asphyxia in Sagamu. Niger J Paediatr. 2009;35:12–8.
Dubay L, Joyce T, Kaestner R, et al. Changes in prenatal care timing and low birth weight by race and socioeconomic status: implications for the Medicaid expansion for pregnant women. Health Serv Res. 2001;36(2):399–403.
Kramer MS, Seguin L, Lydon J, et al. Socioeconomic disparities in pregnancy outcome: why do the poor fare so poorly? Paediatr Perinat Epidemiol. 2000;14(3):194–210.
Orji EO, Ogunniyi SO, Onwudiegwu U. Beliefs and perceptions of pregnant women at Ilesha about Caesarean section. Trop J Obstet Gynaecol. 2003;20:141–3.
Sunday-Adeoye I, Kalu CA. Pregnant Nigerian women’s view of Caesarean section. Niger J Clin Pract. 2011;14(3):276–9.
Aziken M, Omo-Aghoja I, Okonofua F. Perceptions and attitudes of pregnant women towards caesarean section in urban Nigeria. Acta Obstet Gynecol. 2007;86(1):42–7.
Kwast BE. Building a community based maternal program. Int J Gynaecol Obstet. 1995;48(Suppl 1):567–82.
Magoma M, Requejo J, Campbell OM, Cousens S, Filippi V. High ANC coverage and low skilled attendance in a rural Tanzanian district: a case for implementing a birth plan intervention. BMC Pregnancy Childbirth. 2010;10:13.
Zhu B-P, Rolfs RT, Nangle BE, Horan JM. Effect of the interval between pregnancy on perinatal outcomes. N Engl J Med. 1999;340:589–94.
Armson BA, O’Connell C, Persad V, Joseph KS, Young DC, Baskett T. Determinants of perinatal mortality and serious neonatal morbidity in the second twin. Obstet Gynecol. 2006;108(3):556–64.
Lassi ZS, Haider BA, Bhutta ZA. Community-based intervention packages for reducing maternal and neonatal morbidity and mortality and improving neonatal outcomes. Cochrane Database Syst Rev. 2010;11:CD007754.
Penfold S, Manzi F, Mkumbo E, Temu S, Jaribu J, Shamba DD, et al. Effect of home-based counselling on newborn care practices in southern Tanzania, one year after implementation: a cluster randomised controlled trial. BMC Pediatr. 2014;14:187.
Alan Guttmacher Institute. Facts on investing on family planning and maternal and newborn health. Issues in Brief 2010. Available at www.guttmacher.org.
Kozuki N, Katz J, Lee AC, Vogel JP, Silveira MF, Sania A, Stevens GA. Short maternal stature increases the risk of small-for-gestational age and preterm births in low-and middle-income countries; individual participants data meta-analysis and population attributable fraction. J Nutr. 2015;14(11):2542–50.
Jehan I, Harris H, Salat S, Zeb A, Mobeen N, Pasha O, et al. Neonatal mortality, risk factors and causes: a prospective population-based cohort study in urban Pakistan. Bull World Health Org. 2009;87:130–8.
Darmstadt GL, Lee AC, Cousens S, Sibley L, Bhutta ZA, Donney F, et al. 60 million non-facility births: who can deliver in community settings to reduce intrapartum related deaths? Int J Gynecol Obstet. 2009;107(Suppl 1):S89–S112.
Walswa P, Pariyo G, Kallander K, Akuze J, Namazzi G, Ekirapa-Kiracho E, Kerber K, et al. Effect of the Ugandan Newborn Study on care seeking and care practices; a cluster randomised controlled trial. Glob Health Action. 2015;8:24584.
National Primary Health Development Agency, Nigeria. Nigerian Midwives Service Scheme. Available at www.who.int/workforcealliance/forum/2011/hrhawardscs26/en/.
Enweronu-Larygea C, Dickson KE, Moxon SG, Simen-Kapen A, Nyange C, Niermeyer S, et al. Basic newborn care and neonatal resuscitation: a multi-country analysis of health system bottlenecks and potential solutions. BMC Pregnancy Childbirth. 2015;15 Suppl 2:S4.
Sibley LM, Sipe TA, Barry D. Traditional birth attendants training for improving health behaviours and pregnancy outcomes. Cochrane Database Syst Rev. 2012;8:CD005460.
JHPIEGO Trainer News. Focused antenatal care: planning and providing care during pregnancy – A Maternal and Neonatal Health Programme Best Practices. 2003.
Disu EA, Ferguson IC, Njokanma OF, Anga LA, Solarin AU, Olutekunbi AO, Ekure EU, Ezeaka CV, Esangbedo DO, Ogunlesi TA. National Neonatal Resuscitation Training in Nigeria (2008-2012): a preliminary report. Niger J Clin Pract. 2015;18(1):102–9.
WHO. WHO recommendations on interventions to improve preterm birth outcomes. Geneva; 2015.
Magee L, Sawchuck D, Synnes A, von Dadelszen P. SOGC Clinical Practice Guidelines: Magnesium sulphate for fetal neuroprotection. J Obstet Gynaecol Can. 2011;33(5):516–29.
Melamed N, Shah J, Soraishan A, Yoon EW, Lee SK, Shah PS, Murphy KE. Association between antenatal corticosteroid administration-to-birth interval and outcomes of preterm neonates. Obstet Gynecol. 2015;125(6):1377–84.
Lawn JE, Davidge R, Paul VK, von Xylander S, de Graft JJ, Costello A, et al. Born too soon: care for the preterm baby. Reprod Health. 2013;10(Suppl 1):55.
Akseer N, Lawn JE, Keenan W, Koustantopoulous A, Cooper P, Ismail Z, et al. Ending preventable newborn deaths in a generation. Int J Gynaecol Obstet. 2015;131(Suppl 1):S43–8.
Narayanan I, Rose M, Cordero D, Faillace S, Sanghvi T. The components of essential newborn care. Basics support for institutionalizing child survival project (BASICS II) for the United States Agency for International Development, 2004.
Maeda K. Global statistics of perinatal medicine. J Health Med Informt. 2013;S11:1.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Ogunlesi, T.A., Adetoro, O.O. (2021). Preventing Perinatal Mortality in the Developing Countries. In: Okonofua, F., Balogun, J.A., Odunsi, K., Chilaka, V.N. (eds) Contemporary Obstetrics and Gynecology for Developing Countries . Springer, Cham. https://doi.org/10.1007/978-3-030-75385-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-75385-6_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-75384-9
Online ISBN: 978-3-030-75385-6
eBook Packages: MedicineMedicine (R0)