
Abstract
The radiologic evaluation of occult GI bleeding (OGIB) includes computed tomography (CT), magnetic resonance enterography (MRE), barium fluoroscopy, nuclear medicine, and angiography. CT techniques include CT enterography (CTE), CT enteroclysis, CT colonography (CTC), CT angiography (CTA), and dual energy CT (DECT). Conventional angiography can be used as a diagnostic and therapeutic tool. In patients who are poor candidates for endoscopy, conventional double contrast upper GI examination (UGI), double contrast barium enema (BE), and CTC are useful imaging modalities.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
CT
CT is a valuable radiologic modality in the workup of occult GI bleeding. CT scans use X-rays, which produce ionizing radiation, to build cross-sectional images of the body. The images, or “slices,” are created based on the differential densities of the internal structures [1]. Densities can be measured directly on the image, utilizing the Hounsfield Units (HU) scale. CT has high patient throughput and, other than CTC, requires no patient preparation [2, 3].
Non-contrast CT has limited diagnostic utility in the workup of OGIB due to the poor contrast resolution of the image. Hemorrhage may be visualized as circumferential thickening of the bowel wall [4]. Intraluminal hemorrhage may be seen based on its density (30–45 HU for unclotted blood and 45–70 HU for clotted blood) [5, 6].
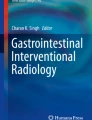
Techniques which use oral and/or IV contrast can significantly improve the diagnostic utility of CT. Imaging can be timed for assessment of the arteries (CTA), for identifying sources of active bleeding. CT enterography (CTE) is performed in an enteric phase (about 50 s after contrast administration) or portal venous phase (60–70 s after contrast administration) to accentuate bowel wall enhancement. These techniques can be performed in conjunction with a delayed phase (typically 90 s or longer after contrast administration) to improve conspicuity of bleeding sites. Standard CT scans with IV contrast can show sources of occult GI bleeding such as gastric ulcers (Fig. 4.1) and sigmoid adenocarcinoma (Fig. 4.2).

There is a focal discontinuity in the gastric antrum (arrow), relating to a gastric ulcer. Arrowhead relates to an adjacent focus of hemorrhage. Endoscopy one day later showed a gastric ulcer with blood clot and no perforation, NSAID induced

Precontrast (a) and postcontrast (b) CT shows high attenuation in the lumen of the sigmoid colon (encircled on b), representing the site of bleeding. Invasive adenocarcinoma was found on pathology
CT Enterography (CTE)
CT enterography (CTE) allows excellent visualization of the entire bowel wall, as well as evaluation of extraenteric structures [7]. In this technique, improved visualization of the bowel mucosa is obtained with fluid distention. Standard technique includes bowel distention with an orally ingested neutral oral contrast (such as Volumen, a 0.1% weight/volume barium suspension). Routine protocol typically involves ingestion of a volume of 1.35 liters Volumen in the 45–60 min prior to CT, with an additional volume of 500 mL water in the last 15 min prior to scanning [7, 8]. Optimal bowel distention is achieved by drinking the oral contrast material slowly, rather than rapidly.
Intravenous contrast administration is a required component of CTE. A routine CTE is performed with a single scan after the administration of IV contrast. Optimal small bowel wall enhancement corresponds to an “enteric phase”, about 50 s after the administration of IV contrast [8, 9]. Most institutions perform a single contrast CTE with a delay of 50 –70 s (portal venous phase).
While a single phase study is typically sufficient in the workup of patients with Crohn’s disease (Fig. 4.3), a multiphase CTE is often helpful in the workup of patients with occult GI bleeding [10, 11]. The multiple phases increase sensitivity for bleeding sites by showing the accumulation of intravenous contrast on more delayed phases. A non-contrast series is probably not necessary, though some centers will perform non-contrast imaging to avoid potential confusion from high density objects such as ingested tablets. Double contrast (arterial and portal venous or more delayed) and triple contrast (arterial, enteric, and delayed) techniques have been described [10]. Angiodysplasia can be identified as an avidly enhancing plaque in the enteric phase [7]. Hara showed a sensitivity of 33% and specificity of 85% in occult GI bleeding.

CTE demonstrates complications of Crohn’s disease, with ascending colitis (arrowhead in a) and inflammation related to enterocutaneous fistula (arrow in b). Note the adjacent iliacus myositis in a. Note the mucosal enhancement and wall thickening (arrows in c) in Crohn’s colitis
There are good data that video capsule endoscopy (VCE) and CTE provide complementary information [11,12,13,14,15,16,17]. While VCE is more sensitive than CTE for mucosal lesions, CTE is more sensitive for mural lesions [11, 18, 19]. CTE is more sensitive for small bowel neoplasms, a more common source of bleeding in younger patients (see Fig. 4.4). CTE could be considered as a first line of evaluation in younger patients and those with Crohn’s disease. There are also data that CTE is a very effective triage tool in determining who may benefit from double balloon enteroscopy [20].

CT enterography shows enhancing lesion of the terminal ileum (arrow in a), representing neuroendocrine tumor. Adjacent mesenteric metastasis is noted (arrowhead in b)
Disadvantages of CTE include ionizing radiation exposure, potential allergic reaction to IV contrast, and contrast induced nephropathy. Patients with GI bleeding are more likely to have compromised renal function, which may preclude the administration of IV contrast. Disadvantages of VCE include retained capsule.
CT Enteroclysis
In this technique, a neutral contrast is instilled through a fluoroscopically placed nasojejunal tube. The invasive and labor-intensive nature make enteroclysis a much less common option, and diagnostic yields have not been shown to be increased [3, 19]. Nevertheless, this option could be considered in patients who cannot tolerate the large volume of orally ingested contrast required for CTE.
CT Colonography
CT Colonography (CTC) is a non-invasive screening technique for colorectal cancer. After a complete bowel preparation, the patient is scanned in supine and prone positions, utilizing a low-dose technique [21]. Supine and prone imaging is performed to better detect polyps and move any residual fluid in the colon between the two positions. 3-dimensional “fly-through” images are created to aid detection, in addition to the standard 2-dimensional slices (Fig. 4.5).

3D-reformatted “fly through” image shows an 8 mm polyp in the sigmoid colon, color coded red by polyp selecting tool in Vitrea postprocessing software package (a).The polyp is demonstrated on the axial source image through the pelvis (b)
CT colonography may be considered in patients who cannot tolerate colonoscopy. After incomplete colonoscopy, CT colonography may have findings 19% of the time [22]. CT colonography can be obtained the same day after incomplete colonoscopy. If the patient wishes to have CT colonography instead of colonoscopy, a full bowel preparation is still required. Several studies have shown a high sensitivity and specificity for CTC for detecting polyps 6 mm or larger [23, 24].
CT Angiography
CT Angiography (CTA) has greater utility in the workup of patients with acute GI bleeding [25]. The arterial timing of contrast can be helpful in identifying sites of active hemorrhage by showing pooling of contrast at sites of active hemorrhage [26, 27]. In patients with intermittent episodes of gastrointestinal bleeding, CTA or multiphase CT that includes arterial phase is useful for identifying sites of hemorrhage [28]. See Fig. 4.6, with conventional angiography correlate.

There is active bleeding from a gastric vascular malformation (arrow in a). Bleeding site is confirmed at conventional angiography (arrow in b)
Dual Energy CT
Dual energy CT is a relatively new technology that uses X-rays of different energies to provide more information than a conventional CT. There is evidence that dual energy may aid in identifying sites of GI bleeding [29]. Iodine-based CT contrast can be made more apparent with low energy reconstructions of the CT data, as well as with iodine maps (Fig. 4.7). There is also potential for radiation dose reduction, as virtual non-contrast images can be created from the dual energy data.

Image from a dual energy CT in a patient with metastatic renal cell carcinoma to the small bowel. Fused image with iodine map accentuates the site of contrast accumulation (arrow), representing a site of active hemorrhage
MR Enterography
MR Enterography (MRE) is a technique to evaluate the small bowel. The oral preparation for MR enterography (MRE) is identical to that of CTE. Intravenous contrast is required, as it is with CTE. Advantages over CTE include lack of ionizing radiation, reduced risk of contrast allergy, greater contrast resolution, and lack of contrast induced nephropathy. There is a risk of nephrogenic systemic fibrosis (NSF), a debilitating multisystem process that affects the skin, with some contrast agents [30]. MRE has poorer spatial resolution compared to CTE, and artifact related to bowel peristalsis is greater due to the longer scan times. This can be minimized by giving glucagon by intramuscular injection or slow IV push [31].
MR Enterography is an excellent option in patients who have history of inflammatory bowel disease. Complications of Crohn’s Disease are well demonstrated with MRE (Fig. 4.8), and the cumulative radiation dose from repeated CT exams can be mitigated with MRE. MRE is also a good option for patients with allergy to contrast given for CT. A disadvantage of MRE compared to CT is a higher likelihood of poor or non-diagnostic studies in patients who are unable to tolerate the oral preparation or to remain motionless for the (longer) duration exam. Studies have shown that MRE is as or more accurate than CTE in the detection of small-bowel diseases, particularly in detecting neoplastic diseases [32]. See Figs. 4.9 and 4.10. Both CTE and MRE have been shown to be effective in evaluating small bowel vascular lesions which may be missed by endoscopy [33, 34], See Fig. 4.11.

Coronal T2 weighted image (a) and axial post contrast T1-weighted image (b) show skip areas of small bowel wall thickening (arrows in a and b), as well as wall hyperenhancement in b. Findings are compatible with areas of active Crohn’s disease

Coronal images from MR enterography demonstrate metastatic melanoma (arrows) to the jejunum. Coronal T2 weighted image (a) and Coronal post contrast image (b)

Coronal T2 weighted image from MR enterography shows nodular thickening of the jejunum (arrows in a) in a patient with celiac disease. Note the excellent bowel contrast compared to the patient’s conventional CT with oral contrast (b), which shows bowel wall thickening in this same region (arrows in b)

Small bowel varices are well seen on MRI (Coronal FIESTA image, a) and axial contrast enhanced CT (b)
Barium Studies
Barium studies can be useful in the workup of GI bleeding, particularly in patients who have contraindications for endoscopy. While no longer generally considered a first line modality, many important findings can be seen with double contrast barium studies, though diagnostic yields are low compared to endoscopy [35,36,37]. Barium studies have no role in the evaluation of patients with active GI bleeding. Double contrast upper GI exams may show causes of occult GI bleeding such as ulcers and cancers (see Figs. 4.12 and 4.13). Barium enema may occasionally be useful to find neoplastic causes of occult bleeding (see Fig. 4.14), though CTC has higher diagnostic yield for detecting colonic neoplasia [38].

There are three gastric ulcers on double contrast upper GI (arrows), which demonstrate pooling of contrast

Two examples of gastric adenocarcinoma. Pooling of contrast with radiating folds (arrows in a) are seen in this gastric adenocarcinoma. Irregular stricture (arrow in b) related to gastric adenocarcinoma, invading the lower esophagus. Note the irregular overhanging edges (arrowheads in b)

Irregular stricture (arrow) on barium enema with overhanging edges corresponds to a site of sigmoid adenocarcinoma
Nuclear Medicine
Technetium (Tc) 99 m sulfur colloid and Tc99m pertechnetate-labeled autologous red blood cells (RBCs) are two nuclear techniques for evaluating occult GI bleeding (Figs. 4.15-4.16) [39,40,41,42]. Tc99m sulfur colloid has a short circulating half-life of 3 min and rapid uptake by the reticuloendothelial system (liver, spleen, and bone marrow) [42]. Imaging is generally performed for only 20–30 min, decreasing the opportunity to identify intermittent lower GI bleed. High background counts in the liver and spleen can obscure upper GI bleeds. For these reasons, 99mTc-erythrocytes are generally superior [43, 44].

Patient underwent a GI bleeding scan performed with 10 mCi Tc-99 m sulfur colloid which did not show signs of gastrointestinal bleeding (a). Two days later, 25 mCi Tc-99 m labeled autologous red blood cells were injected intravenously (b). Active gastrointestinal bleeding is seen in the left lower abdomen (site is encircled)

GI bleeding scan demonstrates pooling of radiotracer in the right lower quadrant (arrow in a). Subsequent angiography shows a tangle of vessels (b) relating to a cecal arteriovenous malformation
Scintigraphy is indicated for overt gastrointestinal bleeding. Per the SNMMI guidelines for gastrointestinal bleeding scintigraphy (GIBS) , the goal is to determine whether the patient is actively bleeding, to localize the bleeding bowel segment, and to estimate the rate of blood loss [45]. This allows for treatment planning and risk stratification [16, 46,47,48]. GIBS is best for evaluation of the mid- to lower GI tract. Selected patients can then be sent to angiography (Fig. 4.16).
A Tc99m pertechnetate study, otherwise known as a Meckel’s scan, is typically used for identifying a Meckel’s diverticulum in the pediatric population [49]. This is due to its affinity for gastric mucosa, as evidenced by its sensitivity of up to 97% in children but only up to 60% in adults [50]. Its specificity remains high at 95% for both adult and pediatric populations.
If a Meckel’s scan (see Fig. 4.17) is employed for the workup of lower GI bleeding in an adult, images are typically taken at short intervals from 30 to 90 minutes and, in the event of a possible intermittent bleed, less frequent image captures can be performed over a 24 h period [49]. Diagnostic utility can be improved in adults with premedication with a histamine receptor antagonist with or without pentagastin, employment of bladder lavage with saline, or nasogastric suctioning [51, 52]. CT may be useful in identifying the Meckel’s diverticulum and Meckel’s vessel arising from the SMA (Fig. 4.17b) [53, 54].

Meckel’s scan demonstrates radiotracer uptake in the midline lower abdomen (arrow in a), corresponding to ectopic gastric mucosa in a Meckel’s diverticulum. Sagittal (b) reformatted images from contrast-enhanced CT shows peripheral enhancement of the Meckel’s diverticulum (arrow). Note the primary Meckel’s vessel arising directly from the SMA (arrowhead), well demonstrated on CT
Conclusions
There are multiple radiologic modalities that are useful in the workup patients with obscure GI bleeding. There are good data that CT and VCE provide complementary information. MRE is very useful, particularly for Crohn’s disease. Nuclear medicine RBC scans and Meckel’s scans are useful in selected patients, and angiography is helpful both for diagnosis and treatment. Fluoroscopy and CT colonography can be helpful particularly in patients who cannot tolerate endoscopy. Advanced techniques such as dual energy CT will likely become more ubiquitous and aid in the diagnosis of patients with GI bleeding.
References
Herman GT. Fundamentals of computerized tomography: image reconstruction from projection. 2nd ed: Springer; 2009.
Geoffroy Y, Rodallec MH, Boulay-Coletta I, Julies MC, Ridereau-Zins C, Zins M. Multidetector CT angiography in acute gastrointestinal bleeding: why, when, and how. Radiographics. 2011;31(3):E35–46.
He B, Yang J, Xiao J, Gu J, Chen F, Wang L, et al. Accuracy of computed tomographic enterography for obscure gastrointestinal bleeding. Acad Radiol. 2018;25:196–201.
Sugi MD, Menias CO, Lubner MG, Bhalia S, Mellnick VM, Kwon MH, Katz DS. CT findings of acute small-bowel entities. Radiographics. 2018;38(5):1352–69.
Hamilton JD, Kumaravel M, Censullo ML, Cohen AM, Kievlan DS, West OC. Multidetector CT evaluation of active extravasation in blunt abdominal and pelvic trauma patients. Radiographics. 2008;28(6):1603–16.
Lubner M, Menias C, Rucker C, et al. Blood in the belly: CT findings of hemoperitoneum. Radiographics. 2007;27(1):109–25.
Elsayes KM, Al-Hawary MM, Jagdish J, Ganesh HS, Platt JF. CT enterography: principles, trends, and interpretation of findings. Radiographics. 2010;30:1955–70.
Sheedy SP, Kolbe AB, Fletcher JG, Fidler JL. Computed tomography enterography. Radiol Clin N Am. 2018;56:649–70.
Schindera ST, Nelson RC, DeLong DM, et al. Multi-detector row CT of the small bowel: peak enhancement temporal window – initial experience. Radiology. 2007;243(2):438–44.
Hara AK, Walker FB, Silva AC, Leighton JA. Preliminary estimate of triphasic CT enterography performance in hemodynamically stable patients with suspected gastrointestinal bleeding. Am J Roentgenol. 2009;193:1252–60.
Huprich JE, Fletcher JG, Fidler JL, Alexander JA, Guimarães LS, Siddiki HA, et al. Prospective blinded comparison of wireless capsule endoscopy and multiphase CT enterography in obscure gastrointestinal bleeding. Radiology. 2011;260:744–51.
Agrawal JR, Travis AC, Mortele KJ, Silverman SG, Maurer R, Reddy SI, et al. Diagnostic yield of dual-phase computed tomography enterography in patients with obscure gastrointestinal bleeding and a non-diagnostic capsule endoscopy. J Gastroenterol Hepatol. 2012;27:751–9.
Boriskin HS, Devito BS, Hines JJ, Scarmato VJ, Friedman B. CT enterography vs. capsule endoscopy. Abdom Imaging. 2008;34:149–55.
Chu Y, Wu S, Qian Y, et al. Complimentary imaging modalities for investigating obscure gastrointestinal bleeding: capsule endoscopy, double-balloon enteroscopy, and computed tomographic enterography. Gastroenterol Res Pract. 2016;2016:1–8.
Haghighi D, Zuccaro G, Vargo J, Conwell D, Dumot J, Santisi J, et al. Comparison of capsule endoscopy (CE) findings of healthy subjects (HS) to an obscure gastrointestinal bleeding (OGIB) patient population. Gastrointest Endosc. 2005;61:AB104.
Kim BSM, Li BT, Engel A, et al. Diagnosis of gastrointestinal bleeding: a practical guide for clinicians. World J Gastrointest Pathophysiol. 2014;5:467–78.
Singh-Bhinder N, Kim DH, Holly BP, et al. ACR appropriateness criteria ® nonvariceal upper gastrointestinal bleeding. J Am Coll Radiol. 2017;14(5S):S177–S188.
Limsrivilai J, Srisajjakul S, Pongprasobchai S, Leelakusolvong S, Tanwandee T. A prospective blinded comparison of video capsule endoscopy versus computed tomography enterography in potential small bowel bleeding. J Clin Gastroenterol. 2017;51:611–8.
Wang Z, Chen J-Q, Liu J-L, Qin X-G, Huang Y. CT enterography in obscure gastrointestinal bleeding: a systematic review and meta-analysis. J Med Imag Radiat Oncol. 2013;57:263–73.
Yen H-H. Clinical impact of multidetector computed tomography before double-balloon enteroscopy for obscure gastrointestinal bleeding. World J Gastroenterol. 2012;18:692.
Chen SC, Lu DS, Hecht JR, et al. CT colonography: value of scanning in both the supine and prone positions. AJR Am J Roentgenol. 1999;172(3):595–9.
Hendrikus JM, van Leeuwen MS, Laheij RJ, Vleggaar FP. CT-colonography after incomplete colonoscopy. Dis Colon Rectum. 56(5):593–9.
Pickhardt PJ, Hassan C, Halligan S, Marmo R. Colorectal cancer: CT colonography and colonoscopy for detection – systematic review and meta-analysis. Radiology. 2011;259(2):393–405.
Plumb AA, Halligan S, Pendse DA, Taylor SA, Malett S. Sensitivity and specificity of CT colonography for the detection of colonic neoplasia after positive faecal occult blood testing: systematic review and meta-analysis. Eur Radiol. 2014 May;24(5):1049–58.
Wu L-M. Usefulness of CT angiography in diagnosing acute gastrointestinal bleeding: a meta-analysis. World J Gastroenterol. 2010;16:3957.
Kuhle WG, Sheiman RG. Detection of active colonic hemorrhage with use of helical CT: findings in a swine model. Radiology. 2003;228:743–52.
Wells ML, Hansel SL, Bruining DH, Fletcher JG, Froemming AT, Barlow JM, Fidler JL. CT for evaluation of acute gastrointestinal bleeding. Radiographics. 2018;38(4):1089–107.
Tseng C-M, Lin I-C, Chang C-Y, et al. Role of computed tomography angiography on the management of overt obscure gastrointestinal bleeding. PLoS One. 2017;12(3):1–9 OR e0172754. https://doi.org/10.1371/journal.pone.0172754.
Sun H, Xue HD, Wang YN, et al. Dual-source dual-energy computed tomography angiography for active gastrointestinal bleeding: a preliminary study. Clin Radiol. 2013 Feb;68(2):139–47.
Thomsen HS. Nephrogenic systemic fibrosis: a serious late adverse reaction to gadodiamide. Eur Radiol. 2006;16:2619–21.
Dillman JR, Smith EA, Khalatbari S, Strouse PJ. IV glucagon use in pediatric MR enterography: effect on image quality, length of examination, and patient tolerance. AJR Am J Roentgenol. 2013;201(1):185–9.
Masselli G, Di Tola M, Casciani E, Polettini E, Laghi F, Monti R, Giulia Bernieri M, Gualdi G. Diagnosis of small-bowel diseases: prospective comparison of multi-detector row CT Enterography with MR enterography. Radiology. 2015;279(2):420–31.
Huprich JE, Barlow JM, Hansel SL, Alexander JA, Fidler JL. Multiphase CT enterography evaluation of small-bowel vascular lesions. AJR Am J Roentgenol. 2013;201(1):65–72.
Amzallag-Bellenger E, Oudjit A, Ruiz A, Cadiot G, Soyer PA, Hoeffel CC. Effectiveness of MR enterography for the assessment of small-bowel diseases beyond crohn disease. Radiographics. 2012;32(5):1423–44.
Gerson LB, Fidler JL, Cave DR, Leighton JA. ACG clinical guideline: diagnosis and management of small bowel bleeding. Am J Gastroenterol. 2015;110:1265–87.
Morrison TC, Wells M, Fidler JL, Soto JA. Imaging workup of acute and occult lower gastrointestinal bleeding. Radiol Clin N Am. 2018;56:791–804.
Nolan D, Traill Z. The current role of the barium examination of the small intestine. Clin Radiol. 1997 Nov;52(11):809–20.
Chung SY, Park SH, Lee SS, Lee JH, Kim AY, Park SK, Han DJ, Ha HK. Comparison between CT colonography and double-contrast barium enema for colonic evaluation in patients with renal insufficiency. Korean J Radiol. 2012 May–Jun;13(3):290–9.
Bunker SR, Brown JM, McAuley RJ, et al. Detection of gastrointestinal bleeding sites: use of in vitro technetium Tc99m-labeled RBCs. JAMA. 1982;247:789–92.
Howarth DM. The role of nuclear medicine in the detection of acute gastrointestinal bleeding. Semin Nucl Med. 2006;36(2):133–46.
Thorne DA, Datz FL, Remley K, Christian PE. Bleeding rates necessary for detecting active gastrointestinal bleeding with Tc-99m labeled red blood cells in an experimental model. Clin Nucl Med. 1987;28(4):514–20.
Ziessman H, O’Malley J, Thrall J. Nuclear medicine: the requisites. 4th ed. Philadelphia: Elsevier Saunders; 2013. p. 307–21.
Bunker SR, Lull RJ, Tanasescu DE, et al. Scintigraphy of gastrointestinal hemorrhage: superiority of Tc-99m red blood cells over Tc-99m sulfur colloid. AJR. 1984;143:543–8.
Siddiqui AR, Schauwecker DS, Wellman HN, et al. Comparison of technetium-99m sulfur colloid and in vitro labeled technetium-99m RBCs in the detection of gastro-intestinal bleeding. Clin Nucl Med. 1985;10:546–9.
Dam HQ, Brandon DC, Graham VV, et al. The SNMMI procedure standard/ EANM practice guideline for gastrointestinal bleeding scintigraphy 2.0. J Nucl Med Technol. 2014;42:308–17.
Otomi Y, Otsuka H, Terazawa K, Yamanaka M, Obama Y, Arase M, et al. The diagnostic ability of SPECT/CT fusion imaging for gastrointestinal bleeding: a retrospective study. BMC Gastroenterol. 2018;18(1):183:1–7. https://doi.org/10.1186/s12876-018-0915-7.
Zahid A, Young CJ. Making decisions using radiology in lower GI hemorrhage. Int J Surg. 2016;31:100–3.
Zuckier LS. Acute gastrointestinal bleeding. Semin Nucl Med. 2003;33(4):297–311.
Singh PR, Russell CD, Dubovsky EV, et al. Technique of scanning for Meckel’s diverticulum. Clin Nucl Med. 1978;3:188–92.
Lin S, Suhocki PV, Ludwig KA, Shetzline MA. Gastrointestinal bleeding in adult patients with Meckel’s diverticulum: the role of technetium 99m pertechnetate scan. South Med J. 2002;95(11):1338–41.
Heyman S. Meckel’s diverticulum: possible detection by combining pentagastrin with histamine H2 receptor blocker. J Nucl Med. 1994;35:1656–8.
Treves S, Grand RJ, Eraklis AJ. Pentagastrin stimulation of technetium-99m uptake by ectopic gastric mucosa in a Meckel’s diverticulum. J Nucl Med. 1991;32:1422–4.
Chen Y, Tang Y, Hu C, Chen S. Bleeding meckel diverticulum. J Comput Assist Tomogr. 2019;43:220–7.
Platon A, Gervaz P, Becker CD, Morel P, Poletti PA. Computer tomography of complicated Meckel’s diverticulum in adults: a pictorial review. Insights Imaging. 2010 May;1(2):53–61.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Schuster, M.E., Jacobson, E.A., Sayegh, A.K., Becerra, V.N., Brooks, R.P.F., Kim, P.E. (2021). Radiologic Detection. In: Tadros, M., Wu, G.Y. (eds) Management of Occult GI Bleeding. Clinical Gastroenterology. Humana, Cham. https://doi.org/10.1007/978-3-030-71468-0_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-71468-0_4
Published:
Publisher Name: Humana, Cham
Print ISBN: 978-3-030-71467-3
Online ISBN: 978-3-030-71468-0
eBook Packages: MedicineMedicine (R0)