
Abstract
A three center randomized controlled crossover clinical trial of exoskeletal-assisted walking (EAW) compared to usual activity (UA) in people with chronic spinal cord injury (SCI) was performed. As secondary outcome measures, the effect of this intervention on bowel and bladder function was assessed using the 10Q Bowel function Survey, the Bristol Stool Form Scale (BFS) and the bowel and bladder components of the Spinal Cord Injury Quality of Life (SCI-QOL) instrument. Fifty subjects were completed the study, with bowel and bladder data available for 49. The amount of time needed for the bowel program on average was reduced in 24% of the participants after EAW. There was a trend toward normalization of stool form noted. There were no significant effects in patient reported outcomes for bowel or bladder function on the SCI-QOL components, although time since injury may have played a role.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


1 Introduction
Spinal cord injury (SCI) is well known to adversely affect bowel [1,2,3] and bladder function [4, 5]. Constipation related to slowed transit time and a sedentary lifestyle is a major issue as is incomplete bladder emptying related to positioning in non-ambulatory individuals. There are some suggestions that frequent upright posture [6] and locomotor training [7] could help bowel function in SCI, but the data is inconclusive [8]. Exoskeletal-assisted walking may be another intervention that could potentially improve bowel and bladder function in this population [9]. We therefore proposed a randomized clinical trial of the effects of 36 sessions of exoskeletal-assisted walking on bowel and bladder function in individuals with chronic non-ambulatory SCI.
2 Materials and Methods
We designed and implemented a three-center randomized crossover controlled clinical trial of exoskeletal-assisted walking (EAW) in non-ambulatory individuals with chronic SCI (>6 months post injury). As secondary outcome measures, we investigated whether this intervention would improve bowel and bladder function as compared to usual activity (UA).
Individuals were screened using a complete history and physical examination incorporating the following: the International Standards for Neurological Classification of SCI (ISNCSCI) examination to determine level and completeness of injury, range of motion at the hips, knees and ankles bilaterally, Ashworth spasticity examination in the lower extremities, standing orthostatic tolerance test, and bone mineral density (BMD) scanning of bilateral knees (proximal tibia and distal femur) and hips (femoral neck and total hip) by Dual Energy X-ray Absorptiometry (DXA).
Eligible participants were randomized within site to one of two groups for 12 weeks (three months): Group 1 received EAW first, three times per week for 12 weeks then crossover (UA) for a second 12 weeks; Group 2 received UA first for 12 weeks then crossover to EAW for 12 weeks of training.
Two powered exoskeleton devices were used in this study, namely the ReWalk 6.0® (ReWalk Robotics, Marlborough, MA) [10] and the Ekso GT® (Ekso Bionics, Richmond, CA) [11]. These powered exoskeletons were chosen because they were the only devices commercially available and FDA approved for use within rehabilitation centers at the time of study development.
Within the first two sessions, standing balance skills were practiced and achieved prior to progression to walking skills. Walking skills were then initiated utilizing a weight shifting pattern. Continuous walking resulted from serial performance of weight shifting. Participants were advanced in their degree of activity and number of steps based on individual progress as determined by the instructing trainer. Missed sessions were added to the end of the 12 weeks to achieve a 36-session total intervention.
The 10 Question Bowel Function Survey (10Q) and the Bristol Stool Form Scale (BFS) was administered before and after both interventions during the two arms of the study. The 10Q provided patient reported outcomes with regard to bowel program satisfaction including information about the time it took to perform a bowel program as well as the amount of assistance needed. The BFS provided information about stool firmness. The BFS rates stool consistency from 1 (hard to pass) to 7 (watery liquid), where 4 is the desired medium consistency [9]. The Bowel Management and the Bladder Management Difficulties item bank forms from the SCI-QOL instrument were performed three times: at baseline, at crossover, and after the second arm for both the EAW and UA arm interventions. The Bowel SCI-QOL instrument consisted of 26 questions (possible score range 25–130) and the Bladder SCI-QOL of 15 questions (possible score range 15–75). Lower scores indicated greater satisfaction with management.
3 Results
A total of 50 subjects completed the exoskeletal-assisted walking protocol including crossover. Of these, 49 individuals completed the bowel surveys and the BFS.
The 10Q Function survey results specifically related to external assistance needed and bowel evacuation times are presented in Table 1. In looking at the whole group (regardless of randomization order), a portion of patients reported a reduction by 12% in the need for external help and a reduction by 24% in evacuation time during each session and across a full week after the EAW three-month intervention.
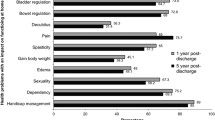
The BFS data suggested a slight qualitative improvement (i.e. trend to a medium consistency of 4) after EAW not seen in the UA group, although by chance the UA group tended to do better at baseline (Fig. 1).

Bristol Stool Form Scale Results. Frequency distribution of pre and post EAW and pre and Post UA. Top row represents pre and bottom row post data
Overall, for the whole group, there were no significant effects found for changes in patient-reported outcomes for the Bowel Management Difficulties SCI-QOL survey after EAW when compared to usual activity. This was also true of the Bladder Management Difficulties SCI-QOL survey.
We performed a post hoc sub-analyses based on time since injury, since it was noticed that the newer injured participants (< two years since injury) were often still learning to maximize their bowel management. Stratification by the duration of injury (DOI) sub-categories for outcomes of bowel function showed that those persons injured for more than two years demonstrated an improvement trend in the Bowel Management SCI-QOL survey after EAW (51.0 ± 9.5 pre versus 48.8 ± 10.2 post EAW, p = 0.1439). In contrast, the newer injured cohort (DOI <2 y) did not show improvement (48.3 ± 7.6 pre to 48.0 ± 8.3 post).
4 Discussion
EAW training had a positive effect on about one quarter of the participants for the patient-reported outcomes for bowel function and management. There were also trends towards normalization of stool form in the EAW group not seen in the UA group. The Bowel and Bladder SCI-QOL batteries were unable however to detect a significant improvement in patient’s perception of their evacuation management with the EAW intervention. Our time since injury sub-analysis suggested that those with newer SCI may still be adjusting and becoming competent with their bowel program, thus negating any potential positive effect from the EAW intervention.
5 Conclusion
A 36-session exoskeletal assisted walking program implemented over three months in non-ambulatory persons with spinal cord injury provided some, albeit limited improvement in several measures of bowel function when compared to a usual activity control group. Most notable improvement (i.e. reduction) was seen in average bowel evacuation time and in a trend to normalization of bowel form consistency. The degree of subjective improvement as determined by quality of life survey instruments may be in part related to the time since injury.
References
M.A. Korsten, N.R. Fajardo, A.S. Rosman, G.H. Creasey, A.M. Spungen, W.A. Bauman, Difficulty with evacuation after spinal cord injury: colonic motility during sleep and effects of abdominal wall stimulation. J. Rehabil. Res. Dev. 41(1), 95–100 (2004)
J.J. Adriaansen, F.W. van Asbeck, D. van Kuppevelt, G.J. Snoek, M.W. Post, Outcomes of neurogenic bowel management in individuals living with a spinal cord injury for at least 10 years. Arch. Phys. Med. Rehabil. 96(5), 905–912 (2015)
P.M. Faaborg, P. Christensen, N. Finnerup, S. Laurberg, K. Krogh, The pattern of colorectal dysfunction changes with time since spinal cord injury. Spinal Cord. 46(3), 234–238 (2008)
G. Savic, H.L. Frankel, M.A. Jamous, B.M. Soni, S. Charlifue, Long-term bladder and bowel management after spinal cord injury: a 20-year longitudinal study. Spinal Cord. 56(6), 575–581 (2018)
R. Hamid, M.A. Averbeck, H. Chiang, A. Garcia, R.T. Al Mousa, S.J. Oh et al., Epidemiology and pathophysiology of neurogenic bladder after spinal cord injury. World J. Urol. 36(10), 1517–1527 (2018)
J.J. Eng, S.M. Levins, A.F. Townson, D. Mah-Jones, J. Bremner, G. Huston, Use of prolonged standing for individuals with spinal cord injuries. Phys. Ther. 81(8), 1392–1399 (2001)
S.A. Morrison, D. Lorenz, C.P. Eskay, G.F. Forrest, D.M. Basso, Longitudinal recovery and reduced costs after 120 sessions of locomotor training for motor incomplete spinal cord injury. Arch. Phys. Med. Rehabil. 99(3), 555–562 (2018)
J.J. Wyndaele, Does regular standing improve bowel function in people with spinal cord injury? Spinal Cord. 53(1), 1 (2015)
D.B. Fineberg, M.A. Korsetn, P.K. Asselin, W.A. Bauman, N.Y. Harel, A. Spungen, Effect of robotic exoskeleton assisted ambulation on bowel function inpersons with paraplegia: one-month follow-up. J. Spinal Cord Med. 36, 533–534 (2013)
ReWalk [Available from: https://rewalk.com/]
Ekso Bionics [Available from: https://eksobionics.com/eksohealth/]
Acknowlegements
Supported by the Department of Defense/CDMRP SC130234 Award: W81XWH-14-2-0170 and National Center for the Medical Consequences of SCI (B9212-C, B2020-C) at the James J. Peters VA Medical Center.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this paper

Cite this paper
Gorman, P.H. et al. (2022). The Effect of Exoskeletal-Assisted Walking on Bowel and Bladder Function: Results from a Randomized Trial. In: Moreno, J.C., Masood, J., Schneider, U., Maufroy, C., Pons, J.L. (eds) Wearable Robotics: Challenges and Trends. WeRob 2020. Biosystems & Biorobotics, vol 27. Springer, Cham. https://doi.org/10.1007/978-3-030-69547-7_34
Download citation
DOI: https://doi.org/10.1007/978-3-030-69547-7_34
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-69546-0
Online ISBN: 978-3-030-69547-7
eBook Packages: EngineeringEngineering (R0)