
Abstract
The epidemiological trends of dermatophyte infections (dermatophytosis or Tinea) in Iran from 1960 to 2018 are characterized here. A thorough search in different literature databases was performed together with statistical analyses. Our findings stress that mycological and clinical aspects of dermatophytosis in Iran have notably been revolutionized over time. Tinea capitis has remained as the dominant Tinea infection in preschool and school-age children throughout the country though its occurrence has markedly subsided after 1980s. In adults, Tinea pedis (22%), Tinea corporis (19.6%), and Tinea cruris (18.4%) were the dominant forms of infection and currently a gradual increase in their incidence is of note. Some clinical types more frequently occurred in some age categories and were caused by some particular species. Tinea capitis more often affected patients under 20 years old, while other Tinea infections were more frequent in middle-aged and older adults. While Trichophyton schoenleinii and Trichophyton violaceum species accounted for a significant part of dermatophytic infections in the past, Epidermophyton floccosum, Trichophyton rubrum, Trichophyton tonsurans, and the Trichophyton mentagrophytes / Trichophyton interdigitale species group are currently predominating in Iran. A more striking mycological aspect of dermatophytosis, however, is the emergence of infection with less-known zoophilic species, e.g. Trichophyton benhamiae, Trichophyton eriotrephon, Trichophyton simii, and Microsporum ferrugineum, all of which having been identified by ITS-rDNA sequencing. Terbinafine, itraconazole, luliconazole, lanoconazole, and efinaconazole showed the best in vitro efficacy against dermatophyte isolates from Iran.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 Introduction
Dermatophytosis (also known as Tinea), which is a public health issue throughout the world, is principally superficial mycosis caused by a group of filamentous fungi known as “dermatophytes” [1, 2]. These fungi grow on the keratinized tissues of skin (in various body sites), nail and hair of human and animals, and spread in an eccentric pattern, leading to small to extended red circular lesions as rings and therefore termed as “ringworm.” Depending on the anatomical site of involved skin, the resulted infections are called Tinea corporis, Tinea cruris, Tinea pedis, and Tinea manuum. Infections of the skin and hair shafts of the beard and scalp areas are termed as Tinea barbae and Tinea capitis, respectively, while involvement of the nails is known as Tinea unguium [2, 3]. Based on the newest taxonomy of dermatophytes, this group contains more than 50 species distributed in seven genera: Trichophyton, Microsporum, Epidermophyton, Lophophyton, Paraphyton, Nannizzia, and Arthroderma [4]. Geographically, the distribution profiles of pathogenic dermatophytes and relevant infections are known to change over time due to immigration, tourism activities, socioeconomic and sanitary conditions [3, 5]. These infections are not life-threatening and, perhaps for this reason, they were more important in view of aesthetics in the past. But, during the last decade there have been reports highlighting the emergence and remarkable increase in the number of recalcitrant Tinea cases with therapeutic failure and repeated recurrences, hence the treatment of dermatophytoses and in vitro antifungal susceptibility testing on the causative fungi became of particular importance [6]. Such variation in the face of Tinea infections led to a real apprehension among dermatologists. Accordingly, regular and retrospective sequential surveys on dermatophytosis and relevant agents as well as in vitro testing of anti-dermatophyte drugs can provide keystones for the upcoming epidemiological investigations on these fungi, and appropriate decision for clinical management of relevant infections.
The first documented report on the prevalence and the etiologic agents of Tinea capitis in Iran returns to the work by Asgari et al. [7], during 1964–1966. But the first and the only critical review on the epidemiological aspects of dermatophytosis in Iran was conducted by Khosravi et al. [8] in 1994. In this study, a total of 12,150 cases of suspected dermatophytosis were investigated between 1986 and 1991 and the infection was confirmed by direct microscopy and culture in 9345 of the cases (76.9%). Since that time, multiple regional studies focused on the epidemiology and etiology of dermatophytosis in different parts of the country have been reported [8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113]. Herein, we aimed to restructure the epidemiological trends of dermatophytoses and antifungal susceptibility aspects of these infections by a comprehensive nationwide study during the time period of 1960 to 2018. An analysis of the frequency of all Tinea infections in regards to the causative species, location, and time period is reported.
2 Material and Methods
2.1 Data Collection Methods
A literature search was performed in the ISC, Google Scholar, Scopus, PubMed, and Web of science (ISI) databases by using the following key search terms: “Dermatophytosis,” “Tinea,” “Dermatophytes,” “Antifungal Susceptibility Testing” (AFST), and “Iran.” The key words were corroborated by the Mesh dictionary, by using the Boolean operator “AND” to link them. To recover the reports lost in our quest, we also scrutinized the references listed in the selected publications. All studies were checked out for information, e.g. place (province) and time of study (as decade), age, and gender of patients if specified, type of dermatophyte infection and the causative species. The extracted data were transferred to the IBM SPSS Statistics program (version 22). The period of analysis was designated from 1960 to 2018.
2.2 Inclusion Criteria
The eligible criteria designated for inclusion of the studies in the review were as follows: (1) publications in English or Persian (Farsi); (2) publications with enough mycological evidences for diagnosis of dermatophytosis and identification of dermatophyte agents including direct microscopy, culture, and morphological identification or sequencing of the internal transcribed spacer (ITS) regions of ribosomal DNA (rDNA). By contrast, a number of studies were excluded from the analysis due to some reasons: (1) studies conducted exclusively on dermatomycoses other than dermatophytosis or relying solely on dermatological findings; (2) studies in which the AFST was not performed according to the Clinical Laboratory Standards Institute (CLSI) M38-A2 guidelines [114] or the European Committee on Antimicrobial Susceptibility Testing (EUCAST) EDef 9.1 guidelines [115]; and (3) studies with discrepant or inexplicable results. In 2017, a new taxonomy for dermatophytes was proposed by De Hoog et al. [4] and we followed this taxonomy for dermatophytes species in this review.
2.3 Statistical Analysis
The differences in the distribution of some species between various infections and time periods of occurrence were compared by using chi-square (χ 2) test. Also, the distribution of each Tinea infection between various age groups was calculated by chi-square (χ 2) test. Two sides p value was calculated and the level of statistical significance was set at p < 0.05.
3 Results
The circumstance of data collection and entrance in this review was illustrated in Fig. 1. Of the 135 publications identified in this search, 106 studies from 24 provinces met our inclusion criteria and entered into the analysis among which a large part was performed in Tehran, the capital of Iran (33 studies), followed by East Azerbaijan (n = 11), Khuzestan (n = 9), Mazandaran (n = 9), and Isfahan (n = 8). In Fig. 2 the location of different provinces (cities) in the country and the provinces of realization in the studies was illustrated. Thirty eight studies were performed from 1960 to 1999 and 68 studies within 2000–2018. Altogether, of 162,799 suspected cases, 37,269 cases (22.9%) were confirmed for dermatophytosis by direct microscopic examination with 10% KOH and/or culture. In Table 1 the distribution of all dermatophytoses in Iran in regards to the time of occurrence was illustrated. Most cases of dermatophytic infections (n = 18,950; 50.8%) were reported within 2000–2009. Tinea pedis (22%) was the dominant form of dermatophytosis followed by Tinea capitis (20.3%), Tinea corporis (19.6%), Tinea cruris (18.4%), Tinea unguium (12.3%), Tinea manuum (7%), and Tinea barbae (0.4%). In 93 studies, the distribution of Tinea infections was correlated to the gender: 21089 individuals were males and 13,234 were females (M/F ratio = 1.59).

The flow diagram explaining the steps involved in collection and processing of data in this review

The location of different provinces in Iran. The yellow highlighted locations corresponding to provinces and cities with eligible studies included in this review
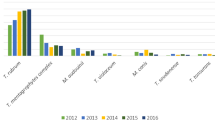
The evolution and frequency of pathogenic dermatophytes species in Iran during the last six decades are depicted in Table 2. A total of 31,485 isolates affiliated to 24 species were detected as causative agents of dermatophytoses in 103 reviewed studies which were, in decreasing order, Epidermophyton floccosum (n = 6098; 19.4%), Trichophyton rubrum (n = 5272), Trichophyton mentagrophytes / Trichophyton interdigitale species group (TMTISG) (n = 4896), Trichophyton verrucosum (n = 3610), Trichophyton tonsurans (n = 2871), T. interdigitale (n = 2459), Microsporum canis (n = 2365), Trichophyton violaceum (n = 1877), Trichophyton schoenleinii (n = 1532), Nannizzia gypsea (formerly Microsporum gypseum; n = 235), T. mentagrophytes (n = 78), Trichophyton erinacei (n = 64), Trichophyton benhamiae (n = 36), Lophophyton gallinae (formerly Trichophyton gallinae), Trichophyton soudanense and Microsporum audouinii (15 cases each one), Microsporum ferrugineum (n = 12), Trichophyton concentricum (n = 4), Arthroderma uncinatum (formerly Trichophyton ajelloi), Trichophyton eriotrephon, Trichophyton simii, Nannizzia fulva (formerly Microsporum fulvum), Nannizzia nana (formerly Microsporum nanum), and Nannizzia persicolor (formerly Microsporum persicolor), two cases each, and Nannizzia incurvata and Paraphyton cookei (formerly Microsporum cookei), one case each. A total of 22 isolates were reported as unknown species. Altogether, in 29,595 cases from 95 studies, the species causing dermatophytosis were correlated to the type of Tinea infection (Table 3). While TMTISG (n = 2117), T. rubrum (n = 1966), T. interdigitale (n = 876), and E. floccosum (n = 799) were respectively determined as the commonest species causing Tinea pedis, T. tonsurans (n = 1429), T. verrucosum (n = 1332), TMTISG (n = 845), M. canis (n = 714), E. floccosum (n = 710) and T. rubrum (n = 622) were the main species causing Tinea corporis. The species causing other Tinea infections and their frequencies are presented in Table 3. A statistically significant difference was found in distribution of some species including T. rubrum, T. interdigitale, T. schoenleinii, T. violaceum, T. tonsurans, T. benhamiae, T. verrucosum, M. canis, E. floccosum, and N. gypsea between different clinical conditions and time periods (p < 0.05). Concerning the correlation of each Tinea infection with the patients’ age, only a total of 17,188 Tinea cases from 25 out of the 106 reviewed publications could be sorted into six age groups (Table 4). Regarding AFST, only 10 publications were eligible for analysis.
4 Discussion
In this review, the epidemiological and mycological features of dermatophytosis in Iran were investigated according to the reports from 1960s to 2018. All reviewed studies were found to be descriptive (but not population based) investigations focused on outpatients attending the mycological laboratories in university-hospital clinics, or on skin, hair, and nail samples referred for direct examination and fungal culture. Except Tinea capitis which more often arose in the 1980s, the detection rates of Tinea infections were the highest in 2000–2009, likely because the vast majority of reviewed studies (n = 46) and then dermatophytic cases (n = 18,950) was from this period. It is known that dermatophytosis more often occurs in men [8]. Consistent with this fact, in almost all reports from Iran, the rate of infection was greater in males except for three studies from Guilan [57, 100] and Tehran [105] that found dermatophytosis affecting predominantly females. With regard to the age of patients, in 25 reviewed publications with the same age ranges, some clinical presentations were found to occur predominantly in some age categories and to be caused by some particular species. As shown in Table 4, Tinea capitis more often affected patients under 20 years old, whereas other infections affected more frequently middle-aged and older adults. The species causing infection in Iranian people during the last 58 years, e.g. E. floccosum, T. rubrum, TMTISG, T. verrucosum, M. canis, T. tonsurans, T. interdigitale, and T. violaceum, in fact are currently the main agents of dermatophytoses worldwide though their distribution pattern differs inside the country and also with other parts of the world. Herein, the evolution of human dermatophytoses and of dermatophytes species pertaining to the time of occurrence is discussed. To our knowledge, this review is the largest Iranian dataset on the epidemiological aspects of human dermatophytosis.
4.1 Tinea pedis
Tinea pedis (also known as athlete foot) is the fungal infection of the soles of the feet and interdigital spaces by a dermatophyte species that can lead to Tinea unguium in 50–60% of cases [116, 117]. The infection is also entitled with “pedal fungus reservoir” due to its extension to other body sites causing Tinea manuum, Tinea unguium, or even Tinea cruris [118]. Autoinoculation from Tinea pedis and onychomycosis is responsible for Tinea corporis, Tinea faciei, and rarely for Tinea capitis in the elderly. Besides, due to the long duration of treatment and the potential for recurrence of infection, Tinea pedis is yet postulated as a matter of concern for public health [119]. Because of health improvement in the mid-twentieth century, expansion of immigration and change in the human lifestyle, such as use of occlusive footwear, the incidence of Tinea pedis has increased. Unlike Tinea capitis or Tinea unguium, we found no worthwhile survey with regular intervals and specific focus on foot dermatophytosis as a distinct entity in Iran. However, integrated with other Tinea conditions, the epidemiological aspects of Tinea pedis were the matter of investigation in different geographical parts of Iran [27, 37]. In this review, Tinea pedis accounted for 22% of all dermatophytoses with an incidence peak in 2000–2009 (28% of all Tinea cases during this decade), and 64.9% of all cases of Tinea pedis also occurred in 2000s. Study of dermatophytosis among some military personnel in south of Iran was the first Iranian report addressing the mycological features of Tinea pedis [120]. In that study dermatophytosis was diagnosed in 145 out of 290 individuals who had lesions suggestive of dermatophytosis, and among them Tinea pedis was the major clinical form (n = 116). Though somewhat old, that study resonated that clinical manifestations of Tinea can vary depending on the occupation, and in certain occupational groups where the individuals have to stand or wear the boat (shoes) for a long time, dermatophytosis more often appears as Tinea pedis [120]. Tinea pedis was then found with a frequency of 11.9% in Isfahan from 1983 to 1984, with T. mentagrophytes as the main causative species [37]. In two later studies within 1983–1994, dermatophytosis of the feet accounted for 8.9% and 5% of all dermatophytoses in Isfahan and Hamadan, respectively [27, 72]. During 1986 to 1991, frequency of Tinea pedis in Iran increased to 15.2% in the study by Khosravi et al. [8], and it ranked the third among the different clinical presentations of dermatophytosis. Generally, before the new century Tinea pedis was a less frequent condition in Iran. At the beginning of the twenty-first century and parallel to infrequency of Tinea capitis, a meaningful upward shift in the prevalence of Tinea pedis occurred, especially in the north of the country. Similar to other Tinea infections, most Tinea pedis cases were recorded within 2000–2009 (Table 1). In Isfahan, the infection took a gradual rising trend after 2007 with an incidence peak in 2009 [31]. During 2000 to 2017, dermatophytic infection of the feet appeared as the dominant Tinea presentation in Tehran [19, 21, 46, 79, 121], Mazandaran [75] and Hamadan [55]. The frequency of infection increased from 20% [84] to 32.1% [75] in Mazandaran (North of Iran) from 2003 to 2014, and it reached 43.4% in Tehran during 2008–2010 [21] which is the highest incidence rate of Tinea pedis from Iran till now. Similarly, in the next investigations during 2010–2014, the infection remained as the most common presentation of dermatophytosis in this city [19, 79, 121]. In the only study performed in Qazvin, Tinea pedis was the third prevalent manifestation of dermatophytosis [30]. A review by Seebacher et al. [5] showed that Tinea pedis accompanied with toenail involvement accounts for more than 50% of Tinea infections in central Europe.
As for the pathogenic agents, Emami et al. [120] found T. mentagrophytes as the main species causing Tinea pedis in 1974. Likewise, T. mentagrophytes (51.7%) was the major causative species in Isfahan during 1983 to 1994 [37, 72], but at that time, T. interdigitale was not recognized as a distinct species. So it is very likely that majority of those T. mentagrophytes isolates actually were T. interdigitale. In the nationwide study by Khosravi et al. [8], T. mentagrophytes var. interdigitale (now called T. interdigitale) (40%), T. rubrum (32%) and E. floccosum (24%) were the leading causes of Tinea pedis in Iran between 1986 and 1991. In Qazvin, during 2004–2006, Tinea pedis was mainly caused by E. floccosum, T. rubrum, and T. mentagrophytes var. interdigitale [30]. In general, T. rubrum, T. interdigitale, and E. floccosum are the predominant species causing Tinea pedis worldwide [3, 5]. As concluded from Table 3, TMTISG, T. rubrum, T. interdigitale, and E. floccosum were the dominant pathogens causing foot infection during the last 58 years in Iran, a statistically notable finding and congruent with the global pattern. Recently, a thorough sequence-based study on the human clinical isolates morphologically identified as TMTISG indicated that Tinea pedis is mainly caused by T. interdigitale rather than T. mentagrophytes, and this finding was statistically significant [122]. Likewise, many isolates from foot clinical materials that were morphologically identified as T. mentagrophytes were, in fact, T. interdigitale in ITS sequencing. Members of the genera Microsporum, Arthroderma, Nannizzia, Lophophyton, and Paraphyton were less frequently reported as agents of Tinea pedis in Iran. Given the increase in the rate of host factors such as elderly population and predisposing diseases like diabetes, the growing incidence of foot infection is predicted.
4.2 Tinea capitis, an Everlasting Condition in Iran
Tinea capitis (scalp ringworm) is an infection of the hair, scalp, and annexes (eyebrows and eyelashes) caused by dermatophytes, mainly of the genera Trichophyton, Microsporum, and Nannizzia [123]. The most important concerns regarding dermatophytosis of the scalp are its high propensity for transmissibility and the long duration of the treatment even with new antifungals [124]. About five decades ago, Tinea capitis was known as “Tinea of elementary students” in Iran and the spectrum of dermatophyte species causing Tinea capitis encompassed all ecological categories of geophilic, zoophilic, and anthropophilic species [8, 37, 125]. In this review, Tinea capitis was found as the second most frequent form of dermatophytosis but nowadays scalp infection is clearly less common in Iran. As shown in Table 1, Tinea capitis was more prevalent in the twentieth century but, similar to the global trend, the incidence of scalp infection sharply decreased after 2010 through the country. This may be the result of improvement in child’s standards and of greater availability of oral antifungals such as terbinafine and itraconazole.
The oldest study regarding dermatophytosis in Iran, conducted by Asgari et al. [113], was a preliminary screening on the prevalence and etiological agents of Tinea capitis in 14 different cities of Iran during 1964 to 1966. In this study, three distinct geographic foci were identified: in decreasing order of importance, the Caspian Sea coast with 25%, the central plateau of Iran with 7.9% and the Persian Gulf coast with 2.4%. In February to March 1970, 1891 children aged 6 to 24 years from Bandar Abbas and Minab cities, South of Iran, were screened by Asgari et al. [7] to define the prevalence of Tinea capitis. They found a prevalence of 3.3% with dominance of endothrix-type Tinea capitis (95%), and neither ectothrix-type infection nor female infection was detected. Failure to diagnose infection among females was attributed to the fact that women and girls refused to be investigated for scalp infection due to cultural issues. Besides, infection was more common in age group ranging from 5 to 14 years. As inferred from Table 1, ringworm of the scalp had an increasing trend in prevalence between 1960 and 2000 with 52.5% of all Tinea capitis cases detected during 1980s and the highest rate of scalp infection in the 1990s (42.9% of all Tinea infections in this decade). Tinea capitis was reported as the most common type of dermatophytosis in studies performed in Hamadan, Isfahan and East Azerbaijan during 1971 to 2014 [27, 31, 37, 47, 48, 50, 72, 125] but also, with lower frequency, from all parts of Iran. In the nationwide study conducted by Khosravi et al. [8] between 1986 and 1991, Tinea capitis was also noted as the predominant type of dermatophyte infection (35.6%).
The prevalence rate of scalp ringworm in this reviewed series changed from 72% in a study in 1983 [37] to 0.8% 30 years later [21]. However, in spite of this considerable decrease in incidence, Tinea capitis remains as a never-ending problem in most parts of the country. In a recent study conducted in Mashhad Northern Iran, Tinea capitis accounted for 32.5% of all dermatophytosis [65], and among them, 53% were endothrix infections caused by T. violaceum and 28% favus due to T. schoenleinii. Regarding the age distribution, Tinea capitis is known to primarily, but not exclusively, affect prepubertal children [3, 123]. Consistent with this fact, the patients with scalp infection in Iran ranged from under one year old to more than 50 years old with majority of them in the age groups of 1–9 and 10–19 years.
Regarding the causal agents of Tinea capitis, they were not static over the time. While M. canis and M. audouinii were the predominant species in Europe and Mediterranean countries, T. tonsurans appeared in the Americas and is currently the most frequent species causing scalp infection worldwide [124, 126]. As shown in Table 3, spectrum of species causing scalp infection in Iran encompassed all seven genera of dermatophytes. Infection mostly occurred by M. canis, followed by T. violaceum, T. verrucosum, T. schoenleinii, and T. tonsurans. The earliest survey on the causative agents of scalp infection in Iran was conducted by Asgari and Sateri [7] in 1970. They found T. violaceum (80%), T. soudanense (15%), and T. tonsurans and T. schoenleinii (1.6% each) as agents of Tinea capitis in Bandar Abbas. In 1980s, T. verrucosum, T. schoenleinii, and T. violaceum were the dominant agents of Tinea capitis in Isfahan [37]. Till 1990s, T. verrucosum remained as the dominant agent of infection in Isfahan, but M. canis appeared as the second common species during this period [72]. In Hamadan during 1991–1992 T. schoenleinii and T. verrucosum were equally the most common agents of Tinea capitis [27] while in the new century, T. tonsurans appeared as the dominant agent of infection in this city and in Tehran as well [46, 55]. In the national study conducted by Khosravi et al. [8], M. canis was found as the most prevalent agent of Tinea capitis, followed by T. verrucosum and T. violaceum. Along with T. verrucosum, T. schoenleinii was endemic in the rural areas of Iran [8], but in the last decade, the rate of infection by this species decreased progressively and it is now eradicated from most parts of the country; the latest cases of T. schoenleinii infection were reported in 2017 by Salari et al. [34]. Generally, overview of the infection pattern shows that over the last decades, the dominant zoophilic species, e.g. M. canis and T. verrucosum, have been replaced by anthropophilic species, especially T. tonsurans [19]. The recent molecular-based studies from Northern and central cities, e.g. Sari, Rasht, and Arak, underlined this changing in the clinical-etiological profile of Tinea capitis with a gradual increase in the rate of endothrix-type Tinea capitis by T. tonsurans [57, 75, 78, 127]. On the other hand, in two recent similar studies from Southwestern cities like Ahvaz, Shiraz, and Yasuj, ectothrix-type scalp infections emerged with T. interdigitale (currently T. mentagrophytes) as the main causative agent [29, 109]. Until the last taxonomic changes from de Hoog et al. [4], all strains of the TMTISG were gathered under the term T. interdigitale which did not discriminate the zoophilic and anthropophilic variants of the species. However, based on the current taxonomy of dermatophytes, it is known that almost all of those Iranian strains causing Tinea capitis were in fact zoophilic species of T. mentagrophytes. Similar pictures were described from Tehran. The predominant species such as T. violaceum and M. canis causing Tinea capitis in the late 1990s and early 2000s [42, 46, 60] were gradually replaced by T. tonsurans and T. mentagrophytes [19, 79, 121]. Nannizzia gypsea was the most common geophilic species causing Tinea capitis, so that 38% of all infections by this species were scalp infections (Table 3). Generally, Tinea capitis was the most common dermatophytic condition before twenty-first century in Iran, but its occurrence decreased considerably during the last two decades. Additionally, the pattern of the causative species has progressively changed with a substantial increase in the incidence of T. tonsurans and T. mentagrophytes and a remarkable decline in the rate of infection by T. schoenleinii after 2000s (Table 3).
4.3 Tinea corporis
Tinea corporis is a worldwide distributed infection that affects the skin of trunk, arms, legs, and neck. In a recent review on human dermatophytosis, this type of infection was found as the predominant Tinea in African adults [126]. It was stated that Tinea corporis is the main clinical form of dermatophytosis in the Middle East [3]. Consistent with this, 65.6% of all Tinea corporis cases were detected in the twenty-first century (during 2000–2018). In this review, Tinea corporis was the third most common presentation of dermatophytic infections with the highest rate of incidence in 2010s. As it can be inferred from Table 1, 24.4% of all dermatophytosis cases between 2010 and 2018 were Tinea corporis. To our knowledge, the oldest retrieved data regarding Tinea corporis also came from the work of Emami et al. [120] in 1974. They found this type of dermatophytosis as the lowest frequent type (1.4%) among affected military personnel. In five distinct surveys from center and west of the country between 1983 and 2018, cases of Tinea corporis constituted the second most frequent type of dermatophytosis after scalp infection [27, 31, 37, 55, 72]. Likewise, in East Azerbaijan till early 1990s Tinea corporis ranked second among all forms of dermatophytosis after Tinea capitis but during 1997–98, it appeared as the main manifestation of dermatophytosis [128]. Similarly, Tinea corporis ranked the first in frequency (31.4%) among all Tinea forms over the period of 1999–2001 in Tehran [60]. The infection also appeared as the main Tinea infection in Khorasan [65], Khuzestan [109], and Kermanshah [18] with prevalence rates of 33%, 37.2, and 38.5%, respectively.
All dermatophytes from all ecological categories cause Tinea corporis, but the main species varies geographically. In Africa, the most prevalent causative species were found to be T. violaceum, T. rubrum, and M. canis [126]. In this review, T. verrucosum and TMTISG were respectively the dominant species involved in Tinea corporis in central provinces of Isfahan and Yazd during 1983–2015 [31, 37, 72, 104]. Likewise, in three different surveys from west of Iran between 1991 and 2015, T. verrucosum was reported as the species predominantly causing infection [18, 27, 55]. In different surveys from Tehran, E. floccosum [42, 60, 79], T. tonsurans [19, 46], T. interdigitale [21, 25], M. canis [129], and T. rubrum [121] were involved as the dominant species causing infection. In Northern provinces, the infection more often occurred by T. verrucosum [128], T. mentagrophytes [65, 84], and T. rubrum [57]. In South part of the country, TMTISG was found as the leading species [29, 82, 109]. Overall, as pointed out in Table 3, T. tonsurans (22.1%), T. verrucosum (20.6%), TMTISG (13.1%), M. canis (11.07%), and E. floccosum were the main species involved in Tinea corporis in Iran (p < 0.05).
4.4 Tinea cruris
The dermatophytic infection of the skin in genitals, inner tights, and buttocks is termed as Tinea cruris (also jock itch and Tinea inguinalis). The infection is globally distributed with different prevalence rates ranging from 2.5 to 52% [130]. It seems that the prevalence rate of Tinea cruris was low before the new century in most parts of Iran. To our knowledge, the first Iranian study addressing the mycological features of Tinea cruris was performed by Emami et al. [120]. They found Tinea cruris as the second type of Tinea among military personnel in some regions in the south of Iran. In Isfahan, during 1983 to 1984, a frequency of 7.3% was reported, with E. floccosum as the only causative agent [37]. Afterward, during 1983 to 1993 the infection ranked fourth among all clinical forms of dermatophyte infections (6.8%) [72]. In four investigations from North West of the country between 1985 and 1997, Tinea cruris rated 1.3–5.3% in term of frequency [48, 50, 110, 128]. In other studies over the period of 2001–2011, Tinea cruris was reported as the most prevalent Tinea with frequency up to 47% [30, 57, 58, 82, 84, 100]. As shown in Table 1, the highest rate of groin infection (57.4%) was from 2000–2009. But it should be stressed that such rate of infection was not solely the result of widespread occurrence of Tinea cruris during 2000s, but also due to a publication bias with multitude of studies focused on dermatophytosis in this decade (46 out of 106 reviewed publications). Tinea cruris is well known to be more common in adolescents and young adults [130]. Congruent with this, the highest rate of infection in Iran was described in 20–39 years old individuals (Table 4).
From a mycological perspective, the most common species causing Tinea cruris worldwide in 1970s were T. mentagrophytes and E. floccosum, but since the 1980s they have been replaced by T. rubrum and now this species is responsible for the majority of the cases [5, 130]. In Iran, however, E. floccosum has been settled as the main pathogen causing groin infection from the past till now [8, 37, 72, 109]. As shown in Table 3, 69.1% of all E. floccosum strains were isolated from groin infection and 72.2% of all Tinea cruris cases were caused by this species, and this finding was statistically significant (p < 0.05). Historically, in 1974 T. mentagrophytes and E. floccosum were reported as the most common cause of Tinea corporis among the personnel of military services in South of Iran [120]. Fourteen years later, Sadri et al. [59] found E. floccosum as the most frequent species causing Tinea cruris in patients referred to the Mycological Laboratory, Razi Hospital, in Tehran during a 3-month period. Between 1983 and 2014 E. floccosum, with notable difference, exceeded other species such as TMTISG, T. rubrum, and M. canis as the agent of groin infection in center, North East, and South of the country [30, 31, 37, 58, 65, 72, 82, 109]. In two different surveys in Hamadan, west of the country, T. verrucosum and E. floccosum were the main agents of jock itch between 1991 to 2016 with almost the same ratio [27, 55], whereas the dominant species causing infection were E. floccosum and T. rubrum in the north of Iran [57, 75, 84], and E. floccosum, T. rubrum and TMTISG in Tehran [19, 21, 25, 46, 60, 79]. Finally, when data regarding the age and gender of patients were available, the infection more often occurred in adults and males. Generally, Tinea cruris remains as a common Tinea infection in Iran with predominance of E. floccosum as the etiological agent.
4.5 Tinea unguium
The term Tinea unguium (or dermatophyte onychomycosis) encompasses any fungal infection of the finger and toe nails by dermatophytes [131, 132]. Tinea unguium together with nail infections by yeasts and non-dermatophyte molds is responsible for about half of all the nail abnormalities and it still remains as an unsolved and even rising problem in many parts of the world [117, 131, 133]. In Australia, the incidence of toenail dermatophytosis increased from 13.8% during 1961–64 to the striking rate of 54.8% in 1995–96 [134]. Though not life-threatening, onychomycosis still remains a serious global disease due to some negative social consequences [132]. Meanwhile, unlike to skin infections by dermatophytes and due to factors intrinsic to the nail, dermatophytosis of the nails is widely difficult to eradicate with antifungal therapy [117]. Today, seven decades after introduction of griseofulvin, Tinea unguium along with Tinea pedis and Tinea capitis remains a never-ending story in dermatology [5]. It is estimated that the global prevalence of Tinea unguium will increase as predisposing conditions such as diabetes, senility, and smoking are becoming more common [117]. Like in other parts of the world, Tinea unguium was found to be common in Iran, with a prevalence rate varying from 1.5% [27] to 21.3% [21]. The first report of Tinea unguium in Iran comes from the study of Ardehali [76] in 1973 with frequency rate of 38%. In the 1980s and early 1990s, Tinea unguium was the less common form of dermatophytosis in most parts of Iran. In Isfahan, Hamadan, and East Azerbaijan frequency of the infection during 1983 to 1998 varied from 1.3 to 2.6% [27, 37, 48, 72, 128]. In the nationwide study by Khosravi et al. [8] between 1986 and 1991, nail infection accounted for 2.6% of all dermatophytoses and it was the lowest common among all dermatophytic infections. Aghamirian and Ghiasian [28] investigated over a 4-year period (2004–2007) the prevalence of onychomycosis in Qazvin in 308 suspected patients and found a rate of 40.2%, with 50% of these infections caused by dermatophytes. In the unique investigation of dermatophytosis from Khorramabad, West of Iran (2007–2008), nail infection ranked second among all Tinea infections (25.5%) [35]. As concluded from Table 1, similar to Tinea cruris, Tinea unguium had a sinusoidal trend in prevalence during the last six decades. But except the report by Ardehali [76], review of the literature indicated that dermatophyte infection of the finger and toe nails was uncommon or less prevalent before 2000s and majority of Tinea unguium cases occurred during the period of 2000–2009 (Table 1). Compared to Tinea capitis which gradually diminished over the time, and similar to Tinea pedis, frequency of nails dermatophytosis has increased over the time, and with reference to the change in the lifestyle and to growth in the number of populations at greater risk for onychomycosis, such rising trend in the frequency was predictable. However, compared to the period of 2000 to 2009, frequency of the infection has decreased to 8.8% in 2009–2018 (Table 1). Although this may imply the improvement in social awareness of fungal nail infection, such frequency is yet remarkable due to its negative social outcomes.
The species most often isolated from Tinea unguium are T. rubrum, T. interdigitale and E. floccosum, worldwide [117]. Consistent with the global trend, T. rubrum and TMTISG constituted the major causative agents of Tinea unguium in this review (Table 3) and this finding was statistically significant. Surprisingly, in the oldest available report from Iran by Ardehali [76], T. schoenleinii was incriminated as the leading agent (63.1%) of onychomycosis. The other species in decreasing order were T. violaceum (15.8%), T. rubrum (10.5%), T. tonsurans, and T. verrucosum (5.3% each). In 93.6% of the cases due to T. schoenleinii and T. violaceum, an accompanying scalp infection was detected and the patients were mostly the peasants who had nail infection in left hands. Khosravi et al. [8] during 1980s showed that T. rubrum, with notable difference, was the leading cause of nail infection compared to T. interdigitale and E. floccosum. In another study by Khosravi and Mansouri [73], T. interdigitale, T. violaceum, and T. rubrum were found to be the foremost cause of Tinea unguium in Tehran from 1996 to 1997. In Isfahan, from 1983 to 2014, the causative agents were found to be TMTISG, E. floccosum and T. rubrum [31, 72, 107]. In Kerman, South of the country, Salari et al. [34] recently identified T. interdigitale as the main agent (64.7%) of nail infection. As illustrated in Table 3, nearly half of the cases of Tinea unguium in Iran were due to T. rubrum. Since 2000s, T. rubrum has remarkably overtaken the TMTISG as the agent of nail and foot mycoses, particularly in Tehran and Northern half of the country, e.g. Khorasan and Mazandaran [21, 46, 65, 75]. In Tehran, during two independent studies from 2000 to 2011, T. rubrum was isolated from 64–74% of all Tinea unguium cases [21, 46]. Similarly, in Qazvin, two different investigations between 2004 and 2007 demonstrated the predominance of T. rubrum followed by T. interdigitale and E. floccosum [28, 30]. Similar to the scenario for Tinea pedis, the recent comprehensive sequence-based study by Taghipour et al. [122], on the human clinical isolates of TMTISG revealed that Tinea unguium is also more commonly caused by T. interdigitale rather than T. mentagrophytes.
Recently, some mycological studies from Tehran, Isfahan, Kermanshah and Ahvaz demonstrated a shift in the etiology of onychomycosis from dermatophytes towards non-dermatophyte molds (NDMs) and yeasts [18, 80, 107, 135, 136]. The frequency of nail infections due to yeasts such as Candida species and NDMs in these investigations varied from 62 to 83.1%. It is known that Tinea unguium is a gender- and age-related infection and its prevalence peaked in males and elderly individuals. Furthermore, nail infection by dermatophytes is much more abundant in toe nails than in finger nails [117, 133]. In agreement with these facts, in 18 studies with retrievable data, we found that dermatophytic onychomycosis more often occurred in toe nails (54.7%) and male patients (M/F ratio: 1.1), aged of 50 years and above. Generally, the increase in life expectancy and in the number of diabetic individuals has resulted in an increased frequency of particular infections such as Tinea unguium and Tinea pedis [3].
4.6 Tinea manuum
Tinea manuum is the term applied for dermatophyte infection of the intertriginous web spaces, palmar and dorsum surfaces of the hands which typically occurs in adults. The infection may also be seen together with Tinea pedis and the so-called ‘two-feet-one-hand syndrome implies to the unilateral infection coexistent with bilateral plantar Tinea pedis [137]. But, compared to Tinea pedis, only a few investigations have been published regarding the clinical and mycological perspective of Tinea manuum. According to our dataset, the first study in Iran with information on the clinico-mycological features of Tinea manuum was performed by Chadeganipour et al. [72] in Isfahan between 1983 and 1993. In their study Tinea manuum accounted for only 2.6% of dermatophytosis cases. Subsequently, Omidynia et al. [27] during their survey of dermatophytosis in Hamadan between 1991 and 1992 found Tinea manuum as the third form of infection (10.4%) in term of abundance. After that, Khosravi et al. [8], in their nationwide study during 1986 to 1994, reported the frequency of Tinea manuum as 9.7% and T. interdigitale as the main causative species. In another surveillance, during 1991 to 1993 hand dermatophytosis accounted for 12% of all dermatophytosis in Tabriz, North West of Iran [48]. In different reports, the frequency of Tinea manuum varied from 2.1% to 18.7% in Tehran [21, 25, 46, 79, 129, 138] or from 4% to 16.4% in Mazandaran [75, 84], whereas it was of 17.5% in Mashhad [65]. But, the highest frequency of Tinea manuum throughout the country (35.5%) was reported from Kerman by Mosavi et al. [16] during 2007–2011. While the frequency of Tinea manuum in Iran was found to be 7% in this review, in different reports from Australia, Poland, China, and Syria, it ranged from 3.4 to 16% [134, 139,140,141]. On the whole, our data support the conclusion that Tinea manuum occurs uncommonly worldwide. Regarding its etiologic agents, Tinea manuum is known to be caused mainly by T. rubrum throughout the world [134, 137, 142], but the causative agents may vary geographically. The survey of all eligible reports from Iran shows that especially before 2000, T. verrucosum was the dominant species causing hand infection but after that T. interdigitale, T. rubrum, TMTISG and T. tonsurans emerged as the main involved species. But, given the marked reduction in the isolation rate of T. verrucosum after 2009 (Table 2), more occurrence of hand infection by human-adapted species like T. rubrum and T. interdigitale is expectable.
4.7 Tinea barbae
Tinea barbae, also called sycosis, is a dermatophytic infection of the skin and hairs of the beard and moustache in men [143,144,145]. Though rare, these disorders impose major complications and healthcare burdens. Besides, given that the clinical appearance of infection simulate to the folliculitis or pseudo-folliculitis barbae, misdiagnosis is highly usual [145]. Nevertheless, few investigations have rated the clinical and mycological features of this infection. Congruent with this view, our review also revealed that the infection has taken less attention in Iran, with only 12 studies reporting a total of 150 cases. This rarity among our dataset made it statistically difficult to take a comprehensive assessment on clinical and mycological aspects of the infection. In our dataset, the frequency of the infection regularly declined after its highest value (44%) in 1980–89, except the period of 2000–2009 where there was a publication bias as for other Tinea presentations. During 2010 to 2018 only six episodes of infection were detected. Notably, this finding was expected because such trend was observed in some recent reports from Iran [21, 25, 109]. Overall, dermatophytosis of the beard was formerly more common but after substantial progresses in lifestyle and sanitary habits of men, especially application of single-use razors, its occurrence took apparently a descending trend worldwide [109, 145]. Overview of the few available literature indicated that most cases of Tinea barbae cases were reported as small series and caused by zoophilic or anthropophilic species [143,144,145,146]. Bonifaz et al. [144] diagnosed 9 cases of Tinea barbae in Mexico over an 18-year retrospective study (1983–2001). Infection was more common in the 60s of life and mainly resulted from T. rubrum and M. canis. The most recent cross-sectional study on Tinea barbae was performed in a major Tertiary Dermatology Department in Lisbon, Portugal by Duarte et al. [145]. Overall, seven cases all of which caused by T. rubrum were detected over an 11-years period (2008 to 2018), with a 46% decrease in the frequency of Tinea barbae compared to similar survey performed in the past decade. A high rate of 43% misdiagnosis at the first clinical inspection by a dermatologist was reported which accentuates the role of mycological examinations for confirmation of the diagnosis. As to the etiology, T. verrucosum, M. canis, and T. mentagrophytes are the dominant zoophilic agents, while T. rubrum is the more common anthropophilic species [143,144,145]. The highest frequency of beard infection in Iran (6.4%) backs to a study in Lorestan, Southwest of Iran. Sepahvand et al. [35] in that scrutiny, found 11 cases of Tinea barbae among which a dermatophyte strain was isolated from culture in 5 cases, i.e. T. violaceum in 4 cases and E. floccosum in the last one. In Isfahan, during 1983–1993, 6 cases of beard infection by T. violaceum, M. canis, and T. verrucosum were detected [72]. Likewise, 6 cases of infection due to T. verrucosum and TMTISG were found over the period of 2004 to 2014 in Kerman [34]. Generally, in the few reported cases among our series, the most common dermatophytes involved were the zoophilic species T. verrucosum (64%), M. canis (18%), TMTISG (10.1%), followed by the anthropophilic species T. violaceum and T. interdigitale (one 2.2% each).
4.8 Trends of Change of Infectious Species
Analysis of the literature reveals that the spectrum of dermatophyte species can be altered throughout the time and may depend on the variation in clinical manifestation of dermatophytosis in the respective regions [5]. This was reflected in this review of dermatophytosis in Iran. As shown in Table 2, favus by T. schoenleinii was prevalent for 3–4 decades before 2000s, but afterward its occurrence strikingly decreased and it has almost disappeared today in Iran. This phenomenon may likely be due to the effectivity of griseofulvin in pediatric Tinea capitis and improvement in the sanitary condition of children during two recent decades. In some recent sequence-based investigations from cities like Tehran, Ahvaz, Shiraz and Yasuj, T. interdigitale was reported as the most common species causing Tinea infections [21, 25, 109, 147]. As indicated before, in those papers from 2013–2016, all anthropophilic and zoophilic strains of the current T. mentagrophytes/T. interdigitale complex were gathered under the term T. interdigitale. Given the recent taxonomy proposed by De Hoog et al. [4], differentiation of T. mentagrophytes and T. interdigitale can be accomplished by ITS sequencing. As stated by Taghipour et al. [122], due to the lack of sequence-based investigations in the past and to the taxonomic instability across dermatophytes species, the true estimation on the rate and spectrum of Tinea infections by either T. mentagrophytes or T. interdigitale in Iran is difficult. In limited number of studies with detailed morphological evaluation, T. mentagrophytes var. interdigitale (currently an invalid name) had predominantly been isolated from Tinea pedis and Tinea unguium while T. mentagrophytes var. mentagrophytes was mainly reported from Tinea corporis and Tinea capitis [8, 31]. The recent comprehensive survey on the GenBank entries accompanied with practical assessment by Taghipour et al. [122] indicated that T. mentagrophytes and T. interdigitale are associated with particular clinical manifestations and a great number of Iranian T. interdigitale strains, especially those isolated from infections other than foot and nail, should be reclassified as T. mentagrophytes. By contrast, majority of submitted T. mentagrophytes which had been isolated from Tinea unguium and Tinea pedis were, in fact, T. interdigitale. Then, estimation of the real incidence of foot and other infections by T. interdigitale and T. mentagrophytes in previous studies (whether from Iran or abroad) when there were no available ITS sequences connected to the isolates, is very difficult.
In terms of frequency of infectious species, E. floccosum was reported as the dominant agent of dermatophytosis in some parts of the country from the past till now [19, 30, 37, 57, 60, 79, 84] and now it is the most prevalent anthropophilic species in the South and West regions of Iran [18, 82, 109]. As a whole, it has also been found as the main species causing groin infection in Iran which was statistically significant [25, 30, 31, 37, 57, 60, 82, 109] and currently it is the third agent of Tinea pedis and Tinea unguium after T. interdigitale and T. rubrum [5]. Of note, the species very rarely invade the hair but four episodes of scalp infection by E. floccosum were found in our dataset. Surveillance of trend of infections by E. floccosum in this review supports the conclusion of Seebacher et al. [5] that contrary to some European countries like Germany, incidence of infection by this anthropophilic species in many Islamic countries is increasing.
The anthropophilic dermatophyte T. rubrum accounted as the second taxon causing dermatophytosis in Iran. Trichophyton rubrum, in general, is a complex comprising three taxa including T. rubrum, T. violaceum, and T. soudanense that despite their relative genetic similarity can be considered as separate species with distinct geographical distributions and clinical preferences [148]. Trichophyton rubrum has emerged since the twentieth century as a cause of chronic Tinea corporis from the endemic areas in South Asia. In the middle of the twentieth century, it has been the most incriminated species causing mainly Tinea pedis and Tinea unguium in Europe and currently it is the main entity causing dermatophytosis worldwide [149]. This species appeared in Iran in the late of the twentieth century, with a very low frequency [37, 76, 150]. For example, in 1973 it accounted for only 10.6% of Tinea unguium cases and its rarity was attributed to its non-indigenous nature [76]. In 1987 and 1996 the frequency of this species among clinical isolates of dermatophytosis in Hamadan and Isfahan was reported as zero and 1.75%, respectively [27, 37]. Between 1986 and 1991, T. rubrum constituted only 4.25% of all agents of dermatophytosis in Iran but it was the main anthropophilic species and the dominant agent of Tinea unguium [8]. After 1990s, its occurrence steadily increased and in many areas of the country it recently emerged as the main or the second most prevalent agent of dermatophytosis [18, 19, 21, 30, 55, 57]. In Central and North Europe, the high isolation rate of T. rubrum during last decades was noted to be connected with the growing incidence of Tinea pedis [5]. Likewise, in surveys conducted after 2000s, the increased frequency of T. rubrum in Iran was accompanied with an increased incidence of Tinea pedis [21, 25, 30, 46, 79, 121]. As illustrated in Table 3, this species was more frequently isolated from Tinea pedis and Tinea unguium. An update on dermatophytosis by Seebacher et al. [5] indicated that mycoses by T. rubrum, especially Tinea pedis and onychomycosis, have increased in central Europe. Generally, consistent with the universal trend, rising incidence of infections by T. rubrum is also predicted for Iran and some host and pathogen factors can impute to this rise. These include: (1) the higher capacity of some T. rubrum strains to spread [151]; (2) the expanded use of private baths which are the main source for vertical transmission of the species within families [152]; (3) use of occlusive shoes which develops humidity leading to Tinea pedis/Tinea unguium; and (4) expansion of social communications leading to greater tendency to the human-to-human than animal-to-human model of infection transmission.
The anthropophilic species T. schoenleinii and T. violaceum were once the most important agents of scalp and skin lesions in Iran [8, 37, 48, 50, 72], but in this review these two species ranked the second (21%) and the third (14.6%) most frequent agents of scalp infection after M. canis. From Table 3, it is figured out that great majority of T. schoenleinii infections was as scalp infection. However, in 1970s, it was even the dominant agent of Tinea unguium in Iran [76] and in 1980s it ranked the second most common agent of Tinea corporis in one study from Isfahan [37]. In East Azerbaijan, between 1985 and 1991, T. schoenleinii was demonstrated as the leading cause of dermatophytosis by Mohammadi [50] and Kazemi et al. [48]. The species even was described as the most common cause of dermatophytosis in Hamadan in the late 1990s [27]. In terms of timeframe, most cases of infection by T. schoenleinii (88.9.1%) occurred between 1980 and 1999 (Table 2). But, currently the elimination of T. schoenleinii and T. violaceum is a great variation in the spectrum of pathogenic dermatophytes species in most areas of Iran. Whereas some authors mentioned that Tinea capitis by T. schoenleinii (favus) is currently limited to some endemic regions like China and Iran [153], apparently no or rare episodes of infection by the species have been traced in the most recent surveys from Iran [21, 34, 109]. Now, it seems that infection by T. schoenleinii is only common in some African countries [5].
A similar story was revealed for T. violaceum in Iran. The highest rate of isolation for the species was during 1980 to 1999, afterward it decreased markedly in the current decade (Table 3). Trichophyton violaceum is a species with endemism confined to some North and East African countries that was imported from these regions to other parts of the world during the twentieth century. The taxon was reported as the most prominent species involved in Tinea capitis and Tinea corporis in most areas of Africa and currently it is a common cause of scalp infection in Africa and West Asia [148]. Additionally, the theory that T. violaceum (along with T. schoenleinii) has predilection to infect hair rather than skin [124] was confirmed statistically in this review where 76.3% of infections by this species in Iran were as Tinea capitis. The first documented report on human infection with this species in Iran was by Asgari and Sateri [7] from Bandar Abbas. In 1970 they found T. violaceum (80%) and T. soudanense (15%) as agents of endothrix Tinea capitis. Between 1986 and 1991, T. violaceum was reported as the second agent of scalp infection in Iran [8]. Currently, the disappearance of T. violaceum and T. schoenleinii along with reemergence of T. tonsurans and decline in the isolation rate of M. canis represent the most important alteration in the spectrum of dermatophytes causing Tinea capitis in Iran. There is no follow-up data regarding the efficacy of antifungal agents for treatment of dermatophytosis in Iran but, based on multicenter trial studies from Canada, Brazil and South Africa, one more likely explanation for the observed decrease in the isolation rate of T. violaceum (and T. schoenleinii) compared to the increase of T. tonsurans is the greater susceptibility of this species to routinely used antifungals compared to T. tonsurans [154]. There are also data supporting that scalp infection due to T. violaceum mostly occurs in children, rather than adults [155], and then gradual decrease of infection by the species in Iran can also be interpreted to as improvement in the sanitary standards for children.
As revealed in Tables 2 and 3, the cattle ringworm fungus T. verrucosum was one of the most common species causing dermatophytosis in Iran, especially Tinea corporis and scalp infection [27, 37, 72]. But, with the advent of sequence-based studies in the second decade of the twenty-first century in Iran, the validity of culture-based reports on the isolation of this zoophilic species from the past onwards was questioned [21, 25, 109]. At present, in Iran, it is known that part of the human isolates which personate the morphological characteristics of T. verrucosum are indeed a diverse range of dermatophyte species including T. mentagrophytes and T. verrucosum [21, 25, 57, 109]. Since 2008 till now, only six sequence-based proven cases of human T. verrucosum clinical isolates were detected in Khuzestan (n = 1) and Guilan (n = 5) of which four isolates were deposited in the Westerdijk Fungal Biodiversity Institute (CBS database, Utrecht, Netherlands) as T. verrucosum CBS 130944 to CBS 130947. Then, the true frequency of human dermatophytosis by T. verrucosum in Iran is much lower than those reported.
The human-adapted fungus T. tonsurans is a ubiquitous dermatophyte known as very contagious and hardly treatable species which can create epidemics especially among athletes in martial arts club [3, 156]. Infection with this taxon was uncommon in the past through the country. Within 1986–1991, it constituted 1.3% of all Tinea agents in Iran, and was exclusively isolated from Tinea capitis [8]. The considerable emergence of T. tonsurans as agent of dermatophytosis in Iran dates back to the late 1980s. This period was, in fact, concurrent with the highest rate of T. schoenleinii, T. violaceum, and M. canis isolation and with the sudden increase in the incidence of Tinea capitis and Tinea corporis. As shown in Table 2, majority of the T. tonsurans isolates (89.1%) were recovered after 2000. In addition, this species was predominantly isolated from cases of Tinea corporis (60%) and Tinea capitis (27.3%), findings which were statistically significant and in agreement with the global changes in the etiology of Tinea capitis towards by T. tonsurans [3]. In the last two decades, new presentations of Tinea corporis or Tinea capitis called Tinea corporis gladiatorum and Tinea capitis gladiatorum were described among sportsmen with extensive bodily contact, especially judoists and wrestlers, throughout the world [40, 69, 157,158,159]. Almost all studies pertaining to the mycological aspects of Tinea gladiatorum unanimously reported T. tonsurans as its most common causative agent. In three reports from Tehran, Qazvin and Sari cities between 2004 and 2008, frequency of this species as agent of Tinea gladiatorum ranged from 82.7 to 100% [40, 69, 157]. As a national sport, wrestling is very popular in Iran and many young individuals are involved in it through the country. Given the expansion of combat sports, especially wrestling, further incidence of both T. tonsurans and Tinea corporis gladiatorum/Tinea capitis gladiatorum in Iran may be expected.
Regarding T. simii, only two cases caused by this less-known species were reported from Yasuj and Ahvaz, among which only one was verified by ITS-rDNA sequencing of the isolate [53, 62]. Trichophyton simii is a rare dermatophyte pathogen that causes infection in a broad variety of animals and human with majorities of records regarding its isolation from India. Incidence of infection by this fungus, even in endemic area of Indian subcontinent, is little known [160]. Like other uncommon species, application of sequence-based procedures is needed to define the incidence rate of dermatophytosis by this fungus in Iran.
The species that is being identified recently in Iran is T. benhamiae (formerly Trichophyton species of Arthroderma benhamiae). It has been reported as an emerging zoonotic dermatophyte in some parts of Europe, especially Germany and Czech and has Guinea pig and some rodents as animal sources [161, 162]. Some strains of the species share mycological features with T. mentagrophytes and generally the definitive species identification relies on ITS-sequencing [161]. The epidemiological aspects of infection by this fungus in Iran is unknown. Until 2013, T. benhamiae has not been detected as agent of dermatophytosis in Iran, not as a result of infrequency, but because of misidentifications as other morphologically similar species. In 2013, it was reported for the first time from two cases of Tinea capitis and Tinea faciei in Tehran [21]. Since that time, the taxon has been isolated from cases of Tinea corporis, Tinea capitis, Tinea manuum, Tinea pedis, and Tinea unguium in Tehran, Ahvaz, Hamadan, Yasuj, and Shiraz [25, 29, 55, 109]. Among T. benhamiae isolates with demographic data in this review, 50% were from Tinea corporis and Tinea faciei which is consistent with the European trend of infection by the species [161]. Currently, the only explicit confirmation for T. benhamiae identification and its differentiation from the closely related species, e.g. T. erinacei and T. eriotrephon is ITS sequencing [161], thus the true incidence and epidemiologic trend of infection by this species in Iran remain to be determined.
Another recognized species with low frequency in this review was T. erinacei, a zoonotic species with hedgehogs as its primary and preferred host. The species causes infection in hedgehogs to a high rate of 20–47%, but it is a very uncommon pathogen for human [163, 164]. The first case of human dermatophytosis by T. erinacei was described from New Zealand in 1960 [165]. Since less than 50 cases of human infection by this zoophilic species have been reported worldwide, most of which go back to the twenty-first century and from Asian countries where the hedgehog is popular as pet, e.g. Japan, Korea, Thailand, and Taiwan [164, 166,167,168]. Surprisingly, Khosravi et al. [8] during their study of dermatophytosis in Iran reported 60 cases of human infection by T. erinacei, all of which originated from scalp infection. But, given the absence of molecular verification, validity of those isolations is questionable. To date, the only confirmed case of human dermatophytosis by T. erinacei comes from Rezaei-Matehkolaei et al. [21] in a study on dermatophytosis in Tehran. One explanation for such infrequency of infection by the species can be attributed to this fact that hedgehog is clearly not popular as pet in Iran. Similarly to T. benhamiae, the thorough identification of this less-known species relies on sequence-based procedures but, at the time of this review, in resource-limited countries such as Iran, the sequencing is relatively costly and difficult to establish in regular clinical diagnostics. Then, the incidence rate of human infection by T. erinacei should be considered with caution, but it is estimated to be less than that of T. benhamiae.
Trichophyton eriotrephon, which was detected from two cases of dermatophytosis in this review, is a pathogenic species closely related to T. benhamiae, T. erinacei, and T. concentricum. Up to now, there are only two published reports on the clinical isolation of the species worldwide, both of which originated from human dermatophytosis. The first one was in 1925 by Papegaay [169] from a case of Tinea corporis in Netherlands. Two other strains identified by ITS sequencing were isolated in Tehran, Iran, during 2008–2010 from two patients with Tinea capitis and Tinea faciei [21]. Recently, two additional ITS sequences from unpublished clinical isolates from Shiraz, South of Iran, were deposited in the GenBank under the accession numbers KP789415 and KP789416. The new isolates were recovered from cases of Tinea manuum and Tinea pedis. Considering the very low isolation rate of the species and that all the newly described isolates originated from human dermatophytosis in Iran, the epidemiological particularities of the infection by this mysterious species remain to be discovered. Additionally, similar to T. benhamiae and T. erinacei, sequencing is mandatory for identification of this species. Therefore, the actual abundance of the species within either Iranian or global dermatophytes population might be greater than what has been discovered so far.
Dermatophytosis due to Microsporum species, until 1970s, was uncommon in Iran [76]. Microsporum canis was reported as the main species causing Tinea corporis in Iran in 1978 [150] and Tinea capitis in 1994 [8]. According to Seebacher et al. [5], there was still in 2008 a predominance of M. canis among agents of Tinea capitis in Mediterranean countries of Europe such as Spain. Based on the new update on dermatophytosis by Coulibaly et al. [126], a number of reports highlighted the reemergence of the species in some Eastern and Northern African countries, especially in Tinea capitis. Here, the fungus was also found to be the most common species causing scalp infection in Iran, especially in 1980s. But, its isolation rate has decreased in the new era, most likely because of the decreased occurrence of scalp infection. As inferred from Tables 2 and 3, Tinea capitis and M. canis exhibited the highest incidence rates during 1980–1989, but they decreased markedly after 2000. Such synchronizations indicate a direct correlation between the presence of M. canis and Tinea capitis. Another attributable reason for the decline in M. canis isolation rate is the increased use of griseofulvin for treatment of Tinea capitis after 1980s since some recent investigations concluded that Microsporum species are more susceptible than Trichophyton species to griseofulvin which was used for treatment of Tinea capitis for many years [170]. Today, M. canis has been replaced by T. tonsurans as etiological agent of most Tinea infections including Tinea capitis/Tinea corporis. Microsporum ferrugineum, as one member of the former Arthroderma otae complex, was found as agent of 12 cases of dermatophytosis in Iran (Table 2). It has limited endemicity in the Balkans, some parts of Middle East, East Asia and Africa [2, 142]. The species is known for causing Tinea capitis but the epidemiological aspects of the infection by this non-indigenous species in Iran are unknown. In this review, 10 of 12 M. ferrugineum isolates were recovered from scalp infections but except two cases from Tehran [21] which were identified by ITS-rDNA sequencing, the identity of the other isolates is questionable. Conclusive differentiation of this species from M. canis and M. audouinii requires sequence-based strategies, e.g. ITS-RFLP or ITS sequencing [26]. Thus, given that in most mycological centers in Iran, the dermatophyte isolates are identified by conventional culture-based methods, the true incidence of this species remains incalculable. Likewise, the accuracy of the 15 reported cases of infection by M. audouinii in Iran could not be verified as this species is non-endemic of the country, and both reports on isolation of this fungus were solely based on the macroscopic and microscopic morphology of the colonies on cultures [23, 58].
In the present data set, Nannizzia gypsea was found as the dominant geophilic species causing dermatophytosis in Iran. Generally, prevalence of human dermatophytosis by N. gypsea compared to anthropophilic and zoophilic taxa is very low. In different reports the incidence of infection by the species ranged from 0.04 to 7% in Europe, 0.6 to 0.87% in the USA, and 0.1 to 6.5% in some Asian countries [171]. To the best of our knowledge, the highest rate (20.9%) was recently reported in one study from Egypt [172]. In Iran, the species contributed in less than 1% [21, 25, 46] to 7.5% [42] of the causative agents of dermatophytosis. Nannizzia gypsea is known to most frequently cause Tinea corporis but it was also responsible for other clinical conditions, especially Tinea capitis [171,172,173]. Concordance with this matter, 87.4% of all cases of dermatophytosis by N. gypsea in Iran had been correlated to Tinea corporis and Tinea capitis (Table 3).
Nannizzia fulva and N. incurvata were reported in only two cases of human dermatophytosis in Iran (1 case each), both of them after 2010 and identified by ITS sequencing [32, 174]. The two taxa are geophilic species morphologically and genetically very close to N. gypsea and very seldom engaged in human infections [174,175,176]. Recently, some sequence-based reports underline that N. fulva and N. incurvata can be overlooked due to misidentification with N. gypsea when identification is solely based on the classical morphological parameters, and thus the true prevalence of N. fulva and N. incurvata could have been underestimated [32, 174, 176, 177]. There were also some reports from the past to now, regarding the isolation of a few number of non-indigenous species, e.g. T. concentricum and T. soudanense, and also less common species, e.g. A. uncinatum, L. gallinae, N. nana, P. cookei, and N. persicolor, from cases of infections in Iran (Table 3). Of note, all studies citing the isolation of the above mentioned species solely used conventional morphological methods. Hence, it is a matter of discussion whether infections by these species are indeed rare or their true incidence underestimated.
4.9 Antifungal Susceptibility Studies on Dermatophytes
Compared to other fungal genera such as Candida, Aspergillus, and Malassezia, and also to the epidemiological aspects of dermatophyte infections, the in vitro antifungal susceptibility patterns of pathogenic dermatophyte species have less routinely been covered, worldwide. Likewise, the area of AFST against dermatophytes has no long history in Iran. We found limited number of studies relevant to this issue, most of which were from the new era and after 2010, and also geographically distributed to some limited provinces. The world’s oldest in vitro antifungal susceptibility assay on dermatophytes was documented in 1971 by Shadomy [178]. He evaluated the in vitro activity of clotrimazole against dermatophytes compared with nystatin, griseofulvin, and pyrrolnitrin and found that nystatin and griseofulvin were less active than clotrimazole against Trichophyton, Microsporum, and Epidermophyton species; however pyrrolnitrin and clotrimazole demonstrated approximately similar effects. After that, numerous studies have been focused on the in vitro / in vivo assessment of different classes of antifungal agents for treatment of dermatophytosis, but not in Iran. The first authentic study in Iran was carried out in 2004 by Chadeganipour et al. [22] in Isfahan, center of Iran, by using only griseofulvin. They found for all tested dermatophyte isolates a geometric mean of griseofulvin minimum inhibitory concentration (MIC) between 0.43 and 0.95 μg/mL. On that study, three strains (of M. canis, T. verrucosum and T. mentagrophytes) with high MIC values for griseofulvin were considered as resistant. However, one of the most comprehensive evaluation on drug susceptibility profile of dermatophytes was conducted by Adimi et al. [179] in 2012. Using CLSI broth microdilution method (M38-A), they analyzed the effects of 10 antifungal agents against a collection of 320 clinical isolates belonging to 15 different species of dermatophytes. Based on the obtained results, itraconazole demonstrated the lowest MIC value while fluconazole had the highest MICs for most tested dermatophytes. Moreover, on that report the most common pathogenic species in Iran, e.g. T. rubrum, TMTISG, E. floccosum, T. tonsurans and M. canis showed acceptable susceptibility to the principal drugs of choice for dermatophytosis, itraconazole and terbinafine. Also, the only data available so far regarding the AFST of the extremely rare species worldwide T. eriotrephon were provided on that study and all antifungals showed very low MICs against the two clinical isolates studied. Similarly, Afshari et al. [147] in Arak city found the lowest and the highest MIC values against tested dermatophytes for itraconazole and fluconazole, respectively. In 2016, the efficacy of six antifungals against a large collection of 316 clinical isolates representative of TMTISG, T. rubrum, M. canis, E. floccosum, T. tonsurans, and T. benhamiae from Ahvaz, Shiraz, and Yasuj was evaluated by Ansari et al. [29]. They found that terbinafine was the most effective antifungal agent against all examined species followed by itraconazole, griseofulvin, and fluconazole. By contrast, in another study from Mazandaran, Baghi et al. [180] evaluated the antifungal susceptibilities of 100 clinical dermatophyte isolates belonging to TMTISG, T. rubrum, T. tonsurans, E. floccosum, and M. canis species towards 12 antifungal agents. They found that luliconazole, anidulafungin, and caspofungin presented the most potent in vitro activities while fluconazole had the highest MIC values. The activity of the novel triazole, efinaconazole, compared with luliconazole, terbinafine, lanoconazole, itraconazole, and fluconazole against a collection of 120 T. interdigitale and T. rubrum clinical isolates was the matter of an in vitro assessment by Rezaei-Matehkolaei et al. [109]. Based on the geometric mean (GM) of the obtained MICs they concluded that efinaconazole (GM = 0.007 μg/mL), lanoconazole (GM = 0.002 μg/mL), and luliconazole (GM = 0.0005 μg/mL) are promising candidates for the treatment of onychomycosis due to T. interdigitale and T. rubrum. The in vitro activity of luliconazole against mentioned species was similar to that reported by Baghi et al. [180].
In 2018, Salehi et al. [181] for the first time in Iran searched for terbinafine resistance among clinical dermatophyte isolates. Out of 97 tested isolates belonging to four species, 5 isolates showed reduced susceptibility to terbinafine (MICs > 32 μg/mL), among which only two isolates of T. rubrum and T. tonsurans demonstrated Leu393Phe substitution in the squalene epoxidase protein. In the most recent study, Taghipour et al. [122] evaluated the in vitro terbinafine resistance in 140 isolates of TMTISG. They reported five terbinafine resistant isolates, all of which belonged to T. mentagrophytes genotype VIII (MICs ≥ 32 μg/mL). Allahdadi et al. [127] determined the antifungal susceptibility profile of dermatophytes originated from the scalp of asymptomatic carriers using four drugs, e.g. griseofulvin, terbinafine, itraconazole, and fluconazole. Fifteen isolates belonging to T. tonsurans, T. interdigitale, and T. rubrum species were highly susceptible to terbinafine (MIC90 = 0.064 μg/mL), followed by itraconazole (MIC90 = 0.125 μg/mL), while griseofulvin (MIC90 = 4 μg/mL) and fluconazole (MIC90 = 64 μg/mL) did not show proper in vitro activities. Finally, Ansari et al. [182] evaluated seven antifungal agents against a set of 40 clinical E. floccosum isolates from four cities (Tehran, Shiraz, Ahvaz, and Mashhad). The geometric mean across all isolates were, in increasing order, as follows: terbinafine (GM = 0.018 μg/mL), posaconazole (GM = 0.022 μg/mL), itraconazole (GM = 0.034 μg/mL), and voriconazole (GM = 0.045μg/mL), which exhibited low MICs against all tested strains, whereas caspofungin (GM = 0.22 μg/mL), ketoconazole (GM = 0.41 μg/mL), and griseofulvin (GM = 0.62 μg/mL) demonstrated higher MICs. Their study showed that terbinafine and posaconazole were the most potent antifungal drugs against E. floccosum strains.
5 Conclusion
During the past six decades, numerous investigations have been directed on dermatophytoses in Iran which markedly improved our knowledge on the epidemiological features of these infections. Within this period, the taxonomy of dermatophytes has widely changed but unfortunately, there have been very few researches that underpinned to the concept of dermatophytes species at the relevant times. Moreover, studies on tracking of dermatophytosis sources, routes of transmission, and risk factors predisposing the infections have been ignored or rare, and therefore research in these areas is still required. In conclusion, this review revealed important changes in the mycological and clinical aspects of dermatophytoses in Iran over time. They remained as dermatological problems among Iranian population though the rate of incidence and dynamic of the infectious agents have changed. Tinea capitis, in particular, is declining over the country and its anthropophilic agents T. schoenleinii and T. violaceum are being eliminated and replaced by another anthropophilic species T. tonsurans. On the contrary, Tinea pedis, Tinea unguium, and Tinea corporis are slowly increasing. The anthropophilic species E. floccosum, T. rubrum, T. tonsurans and T. interdigitale are currently responsible for the major part of dermatophytosis in Iran. A striking epidemiological feature is the emergence of infection with the less-known zoophilic species T. benhamiae with unknown reservoirs, which will be a significant challenge to control. Similar to the global trend, studies in Iran have also shown that terbinafine and itraconazole, among current antifungals, have still the best in vitro efficacy against dermatophytes. Furthermore, the recently FDA-approved azole drugs luliconazole, lanoconazole, and efinaconazole presented promising results compared to old antifungal agents for treatment of dermatophytoses.
References
Ameen M. Epidemiology of superficial fungal infections. Clin Dermatol. 2010;28(2):197–201.
Weitzman I, Summerbell RC. The dermatophytes. Clin Microbiol Rev. 1995;8(2):240–59.
Hayette M-P, Sacheli R. Dermatophytosis, trends in epidemiology and diagnostic approach. Curr Fungal Infect Rep. 2015;9(3):164–79.
De Hoog GS, Dukik K, Monod M, Packeu A, Stubbe D, Hendrickx M, et al. Toward a novel multilocus phylogenetic taxonomy for the dermatophytes. Mycopathologia. 2017;182(1–2):5–31.
Seebacher C, Bouchara J-P, Mignon B. Updates on the epidemiology of dermatophyte infections. Mycopathologia. 2008;166(5–6):335–52.
Dogra S, Shaw D, Rudramurthy SM. Antifungal drug susceptibility testing of dermatophytes: laboratory findings to clinical implications. Ind Derm Online J. 2019;10(3):225.
Asgari M, Sateri H. Cutaneous mycoses in santhern, Iran (scalp ringworm). Iran J Public Health. 1973:10–27.
Khosravi A, Aghamirian M, Mahmoudi M. Dermatophytoses in Iran. Mycoses. 1994;37(1–2):43–8.
Farnagh F, Rafiei M, Farivar Sadri M. The study of etiologic causes of dermatophyte in the location of foot and groin, and the possibility of association of dermatophytosis of these two locations together. Tehran Univ Med J. 2001;1:43–8.
Foladvand MA, Naeimi B. Superficial fungal infections of the skin in the fishermen port Bushehr. Iran South Med J. 1999;1.
Ghaednia B, Zaini F, Kordbacheh P, Hashemi SJ, Mehrabi MR, Mirbakhsh M. Fungal infections of people exposed to shrimp in Bushehr. Iran South Med J. 1999:1.
Asl Rahnamae Akbari N, Adibpour M, Salehpoor A, Noa Khahi A. Investigation of etiological agents of tinea capitis in children under twelve years dermatophytosis suspected infections admitted to the clinic No. 2 Tabriz University of Medical Sciences. Med J Tabriz Univ Med Sci Health Service. 2009;31(2).
Kazemi AH, Ghiasi S. Survey of otomycosis in north-western area of Iran (1447–2004). J Mazandaran Uni Med Sci. 2005;15(48):112–9.
Kordbacheh P, Moghadami M, Asadi MA. Survey of surface and cutaneous fungal diseases in schools and kindergartens in Mahallat and the suburbs. J School Pub Health Inst Publ Health Res. 1994;23(106):61–71.
Moghadami M, Emami M. Investigation causative agents of tinea cruris. J School Pub Health Inst Publ Health Res. 1987.
Mosavi A, Amin S, Safizadeh H, Hadizadeh S. Epidemiology of dermatophytosis in patients referred to the medical mycology laboratory of Afzalipoor Faculty of Medicine in Kerman in 2007–2011. J Dermatol Cosmet. 2012;3(2):114–23.
Hashemi SJ, Moheb Ali M, Zarehee Z. Epidemiology of tinea capitis in Meshkin Shahr primary schools. J Ardabil Univ Med Sci. 2005;5(3):278–81.
Mikaeili A, Mahmod A, Rezaei M, Ebrahimi A. The dermatophytes species frequency in referral patients to medical mycology lab of Kermanshah-2012. Med J Mashhad Univ Med Sci. 2015;57(9):956–61.
Zamani S, Sadeghi G, Yazdinia F, Moosa H, Pazooki A, Ghafarinia Z, et al. Epidemiological trends of dermatophytosis in Tehran, Iran: a five-year retrospective study. J Mycol Méd. 2016;26(4):351–8.
Sadeghi Tafti H, Falahati M, Kordbacheh P, Mahmoudi M, Safara M, Rashidian S, et al. A survey of the etiological agents of scalp and nail dermatophytosis in Yazd, Iran in 2014–2015. Curr Med Mycol. 2015;1(4):1–6.
Rezaei-Matehkolaei A, Makimura K, de Hoog S, Shidfar MR, Zaini F, Eshraghian M, et al. Molecular epidemiology of dermatophytosis in Tehran, Iran, a clinical and microbial survey. J Med Mycol. 2013;51(2):203–7.
Chadeganipour M, Nilipour S, Havaei A. In vitro evaluation of griseofulvin against clinical isolates of dermatophytes from Isfahan. Mycoses. 2004;47(11–12):503–7.
Sadeghi G, Abouei M, Alirezaee M, Tolouei R, Shams-Ghahfarokhi M, Mostafavi E, et al. A 4-year survey of dermatomycoses in Tehran from 2006 to 2009. J Mycol Méd. 2011;21(4):260–5.
Asadi AM, Dehghani R, Sharif Mohammad R. Epidemiologic study of onychomycosis and tinea pedis in Kashan, Iran. Jundishapur J Microbiol. 2009;2009(2):61–4.
Abastabar M, Rezaei-Matehkolaei A, Shidfar MR, Kordbacheh P, Mohammadi R, Shokoohi T, et al. A molecular epidemiological survey of clinically important dermatophytes in Iran based on specific RFLP profiles of beta-tubulin gene. Iran J Public Health. 2013;42(9):1049.
Rezaei-Matehkolaei A, Makimura K, de Hoog GS, Shidfar MR, Satoh K, Najafzadeh MJ, et al. Multilocus differentiation of the related dermatophytes Microsporum canis, Microsporum ferrugineum and Microsporum audouinii. J Med Microbiol. 2012;61(1):57–63.
Omidynia E, Farshchian M, Sadjjadi M, Zamanian A, Rashidpouraei R. A study of dermatophytoses in Hamadan, the governmentship of West Iran. Mycopathologia. 1996;133(1):9–13.
Aghamirian MR, Ghiasian SA. Onychomycosis in Iran: epidemiology, causative agents and clinical features. Nippon Ishinkin Gakkai Zasshi. 2010;51(1):23–9.
Ansari S, Hedayati MT, Zomorodian K, Pakshir K, Badali H, Rafiei A, et al. Molecular characterization and in vitro antifungal susceptibility of 316 clinical isolates of dermatophytes in Iran. Mycopathologia. 2016;181(1–2):89–95.
Aghamirian MR, Ghiasian SA. Dermatophytoses in outpatients attending the dermatology center of Avicenna Hospital in Qazvin, Iran. Mycoses. 2008;51(2):155–60.
Chadeganipour M, Mohammadi R, Shadzi S. A 10-year study of dermatophytoses in Isfahan, Iran. J Clin Lab Anal. 2016;30(2):103–7.
Nouripour-Sisakht S, Rezaei-Matehkolaei A, Abastabar M, Najafzadeh MJ, Satoh K, Ahmadi B, et al. Microsporum fulvum, an ignored pathogenic dermatophyte: a new clinical isolation from Iran. Mycopathologia. 2013;176(1–2):157–60.
Hashemi S, Gerami M, Zibafar E, Daei M, Moazeni M, Nasrollahi A. Onychomycosis in Tehran: mycological study of 504 patients. Mycoses. 2010;53(3):251–5.
Salari S, Mousavi SAA, Hadizadeh S, Izadi A. Epidemiology of dermatomycoses in Kerman province, southeast of Iran: a 10-years retrospective study (2004–2014). Microb Pathog. 2017;110:561–7.
Sepahvand A, Abdi J, Shirkhani Y, Fallahi S, Tarrahi M, Soleimannejad S. Dermatophytosis in western part of Iran, Khorramabad. Asian J Biol Sci. 2009;2(3):58–65.
Gerami Shoar M, Zomorodian K, Emami M, Tarazoei B, Saadat F. Study and identification of the etiological agents of onychomycosis in Tehran, capital of Iran. Iran J Public Health. 2002:100–4.
Chadegani M, Momeni A, Shadzi S, Javaheri MA. A study of dermatophytoses in Esfahan (Iran). Mycopathologia. 1987;98(2):101–4.
Pakshir K, Hashemi J. Dermatophytosis in Karaj, Iran. Ind J Dermatol. 2006;51(4):262.
Bassiri-Jahromi S, Khaksar AA. A etiological agents of tinea capitis in Tehran (Iran). Mycoses. 2006;49(1):65–7.
Aghamirian MR, Ghiasian SA. A clinico-epidemiological study on tinea gladiatorum in Iranian wrestlers and mat contamination by dermatophytes. Mycoses. 2011;54(3):248–53.
Moshir M, Tabatabai A, Poureslami M, Shamshiri A. Prevalence rate of different types of yeast infection in patients visiting the dermatology clinic of HAZRAT RASUL-E AKRAM hospital Razi. J Med Sci. 2002;8(26):466–7.
Rastegar Lari A, Akhlaghi L, Falahati M, Alaghehbandan R. Characteristics of dermatophytoses among children in an area south of Tehran, Iran. Mycoses. 2005;48(1):32–7.
Mirzahoseini H, Omidinia E, Shams-Ghahfarokhi M, Sadeghi G, Razzaghi-Abyaneh M. Application of PCR-RFLP to rapid identification of the main pathogenic dermatophytes from clinical specimens. Iran J Public Health. 2009;38(1):18–24.
Ghasemi Z, Falahati M, Zaini F, Ghaffarpour G-H, Ahmadi F, Eskandar S-E. Causative agents of tinea unguium in Razi Hospital, Tehran, Iran in 2010 and 2011. J Dermatol Cosmet. 2015;6(2):79–84.
Bassiri-Jahromi S, Sadeghi G, Asghari Paskiaee F. Evaluation of the association of superficial dermatophytosis and athletic activities with special reference to its prevention and control. Int J Dermatol. 2010;49(10):1159–64.
Bassiri-Jahromi S, Khaksari AA. Epidemiological survey of dermatophytosis in Tehran, Iran, from 2000 to 2005. Indian J Dermatol Venereol Leprol. 2009;75(2):142–7.
Mohamadi P, Masomi H. Prevalence of dermatophytosis in Shahrood. Med J Tabriz Univ Med Sci Health Service. 1995;27:81.
Kazemi A, Jamali R, Sinafar H, Noroozi A. Survey dermatophytosis in Shabestar (1991–3). Med J Tabriz Univ Med Sci Health Service. 1994;32.
Jamali R, Kazemi A, Lakestani A. Study of Tina capitis agents in Tabriz city. Urmia Med J. 1996;6.
Mohamadi P. Study of dermatophytosis in 1800 patients referring to Haft-e-Tir hospital in Tabriz University of Medical Sciences in 1364–1384. Med J Tabriz Univ Med Sci Health Service. 1988;27(9).
Razi A, Khoaeyani A, Mohamadi P, Sohrabi A, Nori M. Surface and cutaneous fungal infections in east Urmia villages in 1992–1997. Med J Tabriz Univ Med Sci Health Services. 1999;25.
Zaini F, Mahmoudi M, Mehbod A, Kordbacheh P, Safara M. Fungal nail infections in Tehran, Iran. Iran J Publ Health. 2009;38(3):46–53.
Zarei Mahmoudabadi A, Yaghoobi R. Tinea corporis due to Trichophyton simii—a first case from Iran. Sabouraudia. 2008;46(8):857–9.
Sheikhi N, Zaker Bostanabad S, Mirza AS. Comparison and evaluation of laboratory diagnostic method -smear, culture, molecular- in the fungal infection. New Cell Mol Biotechnol J. 2017;7(25):19–26.
Farokhipor S, Ghiasian S, Nazeri H, Kord M, Didehdar M. Characterizing the clinical isolates of dermatophytes in Hamadan city, central west of Iran, using PCR-RLFP method. J Mycol Méd. 2018;28(1):101–5.
Forghani F, Nasrollahi Omran A, Kouchaki M, Mirzaie A. Frequency of dermatophytosis in wrestling and bodybuilding halls in Challous, 2010. Med Lab J. 2013;7(3):31–7.
Fallahi AA, Rezaei-Matehkolaei A, Rezaei S. Epidemiological status of dermatophytosis in Guilan, north of Iran. Curr Med Mycol. 2017;3(1):20.
Mahboobi A, Baghestani S, Hamedi Y, Heidari M, Vahdani M. Epidemiology of dermatophytosis in Bandar Abbas, Iran 2003–2004. Bimonthly J Hormozgan Univ Med Sci. 2006;9(4):227–34.
Sadri MF, Farnaghi F, Danesh-Pazhooh M, Shokohi A. The frequency of tinea pedis in patients with tinea cruris in Tehran, Iran. Mycoses. 2000;43(1–2):41–4.
Falahati M, Akhlaghi L, Lari AR, Alaghehbandan R. Epidemiology of dermatophytoses in an area south of Tehran, Iran. Mycopathologia. 2003;156(4):279–87.
Kazemi A, Sadr Karimi A. Survey tinea unguium in northwest of Iran (1996–1999). Med J Mashhad Univ Med Sci. 2006;48(87).
Ansari S, Hedayati MT, Nouripour-Sisakht S, Rezaei-Matehkolaei A, Jannesar R, Mohammadi H, et al. A 9-month-old girl from Iran with extensive erythematous plaques due to Trichophyton simii, a zoophilic dermatophyte. Mycopathologia. 2016;181(5–6):451–5.
Soltanpoor A, Morovati H, Dehghan P, Rejali M. The epidemiology of dermatophytosis among elementary school children in Koohrang city, Iran, in 2014 and 2015. J Isfahan Med School. 2015;33(352):1–10.
Moghadami M, Shidfar MR. A study of onychomycosis in Tehran. Med J Islam Repub Iran. 1989;3(3):143–9.
Naseri A, Fata A, Najafzadeh MJ, Shokri H. Surveillance of dermatophytosis in northeast of Iran (Mashhad) and review of published studies. Mycopathologia. 2013;176(3–4):247–53.
Nikpoor N, Leppard BJ. Ringworm on the scalp due to Epidermophyton floccosum. Clin Exp Dermatol J. 1977;2:69–71.
Nikookhah F, Azamian A, Mahzounieh M. A study on fungal infection athlete’s foot among soccer players in the Esfahan city sport clubs. J Med Sci. 2007;7(5):913–5.
Hashemi S, Salami A, Hashemi S. An epidemiological study of human dermatophytosis in Karaj (2001). Arch Razi Inst. 2005;60:45–54.
Hedayati MT, Afshar P, Shokohi T, Aghili R. A study on tinea gladiatorum in young wrestlers and dermatophyte contamination of wrestling mats from sari, Iran. Br J Sports Med. 2007;41(5):332–4.
Behzadi Z, Parham S, Fata A, Najafzadeh MJ. The molecular identification of dermatophytes in patients suspected to dermatophytosis in Ghayen (South Khorasan province) in 2015–16: a short report. J Rafsanjan Univ Med Sci. 2018;16(10):983–90.
Diba K, Gheibi A, Deilami Z, Yekta Z, Hazrati KH. Use of the molecular and conventional methods for the identification of human dermatophytosis in Urmia lake’s peripheral area. J North Khorasan Univ Med Sci. 2012;6(3).
Chadeganipour M, Shadzi S, Dehghan P, Movahed M. Prevalence and aetiology of dermatophytoses in Isfahan, Iran. Mycoses. 1997;40(7–8):321–4.
Khosravi A, Mansouri P. Onychomycosis in Tehran, Iran: prevailing fungi and treatment with itraconazole. Mycopathologia. 2001;150(1):9–13.
Mahmoudabadi AZ. First case of Microsporum ferrugineum from Iran. Mycopathologia. 2006;161(5):337–9.
Didehdar M, Shokohi T, Khansarinejad B, Sefidgar SAA, Abastabar M, Haghani I, et al. Characterization of clinically important dermatophytes in north of Iran using PCR-RFLP on ITS region. J Mycol Méd. 2016;26(4):345–50.
Ardehali M. Dermatophytic agents of tinea unguium in Iran. Int J Dermatol. 1973;12(5):322–3.
Afshar P, Khodavaisy S, Kalhori S, Ghasemi M, Razavyoon T. Onychomycosis in north-east of Iran. Iran J Microbiol. 2014;6(2):98.
Afshar P, Vahedi L, Ghasemi M, Mardanshahi A. Epidemiology of tinea capitis in Northeast Iran: a retrospective analysis from 1998 to 2012. Int J Dermatol. 2016;55(6):640–4.
Ghojoghi A, Falahati M, Abastabar M, Ghasemi Z, Ansari S, Farahyar S, et al. Molecular identification and epidemiological aspects of dermatophytosis in Tehran, Iran. Res Mol Med. 2015;3(3):11–6.
Chadeganipour M, Nilipour S, Ahmadi G. Study of onychomycosis in Isfahan, Iran. Mycoses. 2010;53(2):153–7.
Hallaji Z, Sadri M, Dadvar F. Analysis of 58 cases of tinea capitis in Tehran Razi hospital. Acta Med Iran. 2001;39(2):109–12.
Mahmoudabadi AZ. A study of dermatophytosis in south west of Iran (Ahwaz). Mycopathologia. 2005;160(1):21–4.
Mahmoudabadi AZ, Yaghoobi R, Sadeghi B. A large outbreak of tinea capitis in a primary school. J Infect. 2007;54(6):e247–e8.
Rezvani SM, Sefidgar SAA, Hasanjani Roushan MR. Clinical patterns and etiology of dermatophytosis in 200 cases in Babol. North Iran Caspian J Intern Med. 2010;1(1):23–6.
Mahmoudabadi AZ, Izadi B. Prevalence of cutaneous mycoses among workers. Turk J Med Sci. 2011;41(2):291–4.
Asadi A, Davoodabadi A, Samei A. Prevalence of superficial and cutaneous fungal diseases in recreational center of addicts in Tehran during the year 1376. J Kashan Univ Med Sci Health Services. 1999;3(3):74–80.
Asadi MA, Houshyar H, Dehghani R, Ershadi A, Arbabi M, Doroudgar A, et al. Prevalence of skin and superficial mycoses in schools of the city of Kashan and its suburbs. Feyz J Kashan Univ Med Sci Health Services. 2001;4:41–7.
Zarrin M, Poosashkan M, Mahmoudabadi A, Mapar M. Prevalence of superficial fungal infection in primary school children in Ahvaz, Iran. Macedonian J Med Sci. 2011;4(1):89–92.
Asl Rahnamae Akbari N, Adibpour M, Salehpoor A, Kazemi A. Prevalence of nail fungal infections (onychomycosis). Med J Tabriz Univ Med Sci Health Service. 2004;27(2).
Amir Rajab N, Rafie A, Omidian M, Mapar M, Yaghobi R, Rasaei S, et al. Tinea capitis in Ahvaz. Iran J Infect Dis. 2007;37:71–5.
Ansarin H, Ghaffarpoor GH, Mehraban F. The survey of frequency and etiology of mycoses of the head and body among primary school students in Varamin. Iran J Med Sci. 2001;8(24).
Bassiri-Jahromi S, Khaksar AA. Study of onychomycosis in submitted patients to the Pasteur institute of Iran, 1993–1999. J Fac Med. 2002;60(5):364–70.
Bassiri-Jahromi S, Khaksar AA. Surveillance of dermatophytosis and the causative agents among children referred to Pasteur Institute of Iran from 2005 to 2006. Res Med. 2008;32(4):321–6.
Khaksar AA, Basiri-Jahromi S, Amirkhani A, Poorabdolahi A. Survey on the prevalence of tinea capitis in primary school children in coastline of Mazandaran province. Teb va Tazkiye Ministry Health Med Edu. 1996;25:18–22.
Zarei MA. A survey of 382 suspected patients with tinea capitis (AHWAZ). Jundishapur Sci Med J. 1997;22:45–52.
Zamanian A, Farshchian M, Nazeri H. The prevalence of tinea pedis in Sina hospital staff in Hamadan in 2000. Iran J Dermatol. 2003;6(4).
Zaini F, Ghagary A. Survey epidemiology and mycology tinea capitis in schools and kindergartens of the Chabahar port. Iran J Public Health. 1989;18:1–12.
Salehpoor A, Adibpour M, Attari M-A-A, Asl Rahnamae Akbari N. Investigating the incidence of thymus epithelium in patients referred to the Mycology Laboratory of Tabriz University of Medical Sciences. Med J Tabriz Univ Med Sci Health Service. 2004;38(62).
Shokohi T, Hajheidari Z, Haghani I, Khalilian A, Aghili SR, Miahi S. The study of 101 cases of onychomycosis and associate factors in patients referred to Boali Sina hospital and Toba dermatology outpatient clinics in sari. Mazandaran Univ Med Sci. 2009;19(71):33–43.
Alizadeh N, Sadr Eshkevari Sh, Golchei J, Falahi AA. A descriptive study of types of tinea in Gilan. Iran J Dermatol. 2004;7(4).
Alizadeh N, Sadr Eshkevari S, Golchaei J, Fallahi AA. Deep dermatophytosis in a patient with rheumatoid arthritis treated with immunosuppressive drugs: a case report. Iran J Dermatol. 2005;6(3):35–8.
Kazemi A. Tinea unguium in the north-west of Iran (1996–2004). Rev Iberoam Micol. 2007;24(2):113–7.
Bassiri-Jahromi S, Khaksar AA, Amirkhani A. Prevalence of fungal infections among wrestlers in Tehran. Pejouhesh dar Pezeshki (Res Med). 2006;30(3).
Rashidian S, Falahati M, Kordbacheh P, Mahmoudi M, Safara M, Sadeghi Tafti H, et al. A study on etiologic agents and clinical manifestations of dermatophytosis in Yazd, Iran. Curr Med Mycol. 2015;1(4):20–5.
Khaksar AA, Basiri-Jahromi S, Amirkhani A, Mortazavi R. Study of fungal infections in the physiological and mental disabled in Tehran. Teb va Tazkiye Ministry Health Med Edu. 1997;25.
Naseri A, Fata A, Khosravi AR. The first case of Microsporum persicolor infection in Iran. Jundishapur J Microbiol. 2012;5(1):362–4.
Chadeganipour M, Mohammadi R. Causative agents of onychomycosis: a 7-year study. J Clin Lab Anal. 2016;30(6):1013–20.
Yazdanfar A. Tinea capitis in primary school children in Hamedan (west of Iran). Int J Med Med Sci. 2010;2(2):029–33.
Rezaei-Matehkolaei A, Rafiei A, Makimura K, Gräser Y, Gharghani M, Sadeghi-Nejad B. Epidemiological aspects of dermatophytosis in Khuzestan, southwestern Iran, an update. Mycopathologia. 2016;181(7–8):547–53.
Mohamadi P, Babaei Sh, Rabiei H. Evaluation of dermatophytosis in children of primary school girls in Tabriz. Med J Tabriz Univ Med Sci Health Service. 2002;45.
Edalatkhah H, Golforoshan F, Azimi H, Mohammadi P, Razi A. Prevalence of various species of dermatophytes in patients referring to the dermatology clinic of Tabriz haft-e-Tir hospital. J Ardabil Univ Med Sci. 2006;6(1):47–52.
Emami M, Asgari M, Alilou M. Evaluation of dermatophytic contamination of garrisons in south of Iran. Iran J Publ Health. 1973;3(4).
Asgari M, Alilou M, Sheiban Z. Results of preliminary studies on prevalence and the etiologic agents of tinea capitis in Iran. Pahlavi Med J. 1971;2:422–34.
Wayne P. Clinical and Laboratory Standards Institute: Reference method for broth dilution antifungal susceptibility testing of yeasts; approved standard. In: CLSI document M27-A3 and Supplement S, vol. 3; 2008. p. 6–12.
Rodriguez-Tudela J, Arendrup M, Arikan S, Barchiesi F, Bille J, Chryssanthou E et al. EUCAST definitive document E. DEF 9.1: Method for the determination of broth dilution minimum inhibitory concentrations of antifungal agents for conidia forming moulds. Def. 2008;9:1–13.
Ogasawara Y, Hiruma M, Muto M, Ogawa H. Clinical and mycological study of occult tinea pedis and tinea unguium in dermatological patients from Tokyo. Mycoses. 2003;46(3–4):114–9.
Gupta AK, Versteeg SG, Shear NH. Onychomycosis in the 21st century: an update on diagnosis, epidemiology, and treatment. J Cutan Med Surg. 2017;21(6):525–39.
Daniel CR III, Jellinek NJ. The pedal fungus reservoir. Arch Dermatol. 2006;142(10):1344–6.
Toukabri N, Dhieb C, El Euch D, Rouissi M, Mokni M, Sadfi-Zouaoui N. Prevalence, etiology, and risk factors of tinea pedis and tinea unguium in Tunisia. Can J Infect Dis Med Microbiol. 2017;2017:6835725.
Emami M, Asgari M, Alilou M. Investigation of environmental pollution of dermatophytes in southern garrisons. Iran J Publ Health. 1974;3(4).
Hamedifard M, Hashemi SJ, Ghazvini RD, Zareei M, Hosseinpour L, Boroujeni ZB. Mycological study of superficial-cutaneous mycoses in Tehran, Iran. Infect Epidemiol Med. 2017;3(2):60–5.
Taghipour S, Pchelin IM, Zarei-Mahmoudabadi A, Ansari S, Katiraei F, Rafiei A, et al. Trichophyton mentagrophytes and T. interdigitale genotypes are associated with particular geographic areas and clinical manifestations. Mycoses. 2019;62(11):1084–91.
Tirado-Sánchez A, Bonifaz A. Tinea capitis: current review of the literature. Curr Fungal Infect Rep. 2018;12(3):120–6.
Hay R. Tinea capitis: current status. Mycopathologia. 2017;182(1–2):87–93.
Momtaz M. Distribution of skin diseases in Esfahan. Persian Med J. 1974;3:526–32.
Coulibaly O, L’Ollivier C, Piarroux R, Ranque S. Epidemiology of human dermatophytoses in Africa. Med Mycol. 2017;56(2):145–61.
Allahdadi M, Hajihossein R, Kord M, Rahmati E, Amanloo S, Didehdar M. Molecular characterization and antifungal susceptibility profile of dermatophytes isolated from scalp dermatophyte carriage in primary school children in Arak city, Center of Iran. J Mycol Méd. 2019;29(1):19–23.
Edalatkhah R, Samavati A. Prevalence of dermatophytes verities types in patient who referred to skin Clinic of Tabriz Haft-e-Tir hospital skin clinic 1997–8. J Ardabil Univ Med Sci. 2000;3(7):31–5.
Hassanzadeh Rad B, Hashemi SJ, Farasatinasab M, Atighi J. Epidemiological survey of human dermatophytosis due to zoophilic species in Tehran, Iran. Iran J Public Health. 2018;47(12):1930.
Shemer A, Babaev M. Fungal infections (onychomycosis, Tinea pedis, Tinea cruris, Tinea capitis, Tinea manuum, Tinea corporis, different Candida infections, and pityriasis versicolor) and mycological laboratory analyses. In: Tur E, Maibach HJ, editors. Gender and dermatology. Berlin: Springer; 2018. p. 235–42.
Elewski BE, Rich P, Tosti A, Pariser DM, Scher R, Daniel RC, et al. Onchomycosis: an overview. J Drugs Dermatol. 2013;12(7):s96–s103.
Elewski BE. Onychomycosis: pathogenesis, diagnosis, and management. Clin Microbiol Rev. 1998;11(3):415–29.
Piraccini BM, Alessandrini A. Onychomycosis: a review. J Fungi (Basel). 2015;1(1):30–43.
Coloe SV, Baird RW. Dermatophyte infections in Melbourne: trends from 1961/64 to 1995/96. Pathology. 1999;31(4):395–7.
Motamedi M, Ghasemi Z, Shidfar MR, Hosseinpour L, Khodadadi H, Zomorodian K, et al. Growing incidence of non-dermatophyte onychomycosis in Tehran, Iran. Jundishapur J Microbiol. 2016;9(8):e40543.
Fatahinia M, Jafarpour S, Rafiei A, Taghipour S, Makimura K, Rezaei-Matehkolaei A. Mycological aspects of onychomycosis in Khuzestan Province, Iran: a shift from dermatophytes towards yeasts. Curr Med Mycol. 2017;3(4):26–31.
Veraldi S, Schianchi R, Benzecry V, Gorani A. Tinea manuum: a report of 18 cases observed in the metropolitan area of Milan and review of the literature. Mycoses. 2019;62(7):604–8.
Moshir M, Tabatabaei A, Poureslami M, Shamshiri A. Evaluation of fungal infection in patient referred to dermatology clinic of Rasoul Akram. Razi J Med Sci. 2001;8(26):466–70.
Nowicki R. Dermatophytoses in the Gdansk area, Poland: a 12-year survey. Mycoses. 1996;39(9–10):399–402.
Tao-Xiang N, Zhi-Cheng L, Sao-Mao W, Wen-Zhu L. Analysis of dermatomycoses in Lanzhou district of northwestern China. Mycopathologia. 2005;160(4):281–4.
Ismail MT, Al-Kafri A. Epidemiological survey of dermatophytosis in Damascus, Syria, from 2008 to 2016. Curr Med Mycol. 2016;2(3):32.
Wisuthsarewong W, Chaiprasert A, Viravan S. Outbreak of tinea capitis caused by Microsporum ferrugineum in Thailand. Mycopathologia. 1996;135(3):157–61.
Sabota J, Brodell R, Rutecki GW, Hoppes WL. Severe tinea barbae due to Trichophyton verrucosum infection in dairy farmers. Clin Infect Dis. 1996;23(6):1308–10.
Bonifaz A, Ramírez-Tamayo T, Saúl A. Tinea barbae (tinea sycosis): experience with nine cases. J Dermatol. 2003;30(12):898–903.
Duarte B, Galhardas C, Cabete J. Adult tinea capitis and tinea barbae in a tertiary Portuguese hospital: a 11-year audit. Mycoses. 2019;62:1079–83.
Trotha R, Gräser Y, Platt J, Köster A, König B, König W, et al. Tinea barbae caused by a zoophilic strain of Trichophyton interdigitale. Mycoses. 2003;46(1–2):60–3.
Afshari MA, Shams-Ghahfarokhi M, Razzaghi-Abyaneh M. Antifungal susceptibility and virulence factors of clinically isolated dermatophytes in Tehran, Iran. Iran J Microbiol. 2016;8(1):36–46.
Su H, Packeu A, Ahmed SA, Al-Hatmi AM, Blechert O, İlkit M, et al. Species distinction in the Trichophyton rubrum complex. J Clin Microbiol. 2019;57(9):e00352–19.
Ilkit M, Durdu M. Tinea pedis: the etiology and global epidemiology of a common fungal infection. Crit Rev Microbiol. 2015;41(3):374–88.
Nikpoor N, Buxton M, Leppard B. Fungal diseases in shiraz. Pahlavi Med J. 1978;9(1):27–49.
Ghannoum M, Isham N. Fungal nail infections (onychomycosis): a never-ending story? PLoS Pathog. 2014;10(6):e1004105.
Nenoff P, Krüger C, Ginter-Hanselmayer G, Tietz HJ. Mycology–an update. Part 1: dermatomycoses: causative agents, epidemiology and pathogenesis. J Dtsch Dermatol Ges. 2014;12(3):188–210.
Ilkit M. Favus of the scalp: an overview and update. Mycopathologia. 2010;170(3):143–54.
Gupta A, Dlova N, Taborda P, Morar N, Taborda V, Lynde C, et al. Once weekly fluconazole is effective in children in the treatment of tinea capitis: a prospective, multicentre study. Br J Dermatol. 2000;142(5):965–8.
Grigoryan KV, Tollefson MM, Olson MA, Newman CC. Pediatric tinea capitis caused by Trichophyton violaceum and Trichophyton soudanense in Rochester, Minnesota, United States. Int J Dermatol. 2019;58(8):912–5.
El-Fari M, Gräser Y, Presber W, Titez HJ. An epidemic of tinea corporis caused by Trichophyton tonsurans among children (wrestlers) in Germany. Mycoses. 2000;43(5–6):191–6.
Bassiri-Jahromi S, Khaksar AA. Outbreak of tinea gladiatorum in wrestlers in Tehran (Iran). Ind J Dermatol. 2008;53(3):132–6.
Ilkit M, Ali Saracli M, Kurdak H, Turac-Bicer A, Yuksel T, Karakas M, et al. Clonal outbreak of Trichophyton tonsurans tinea capitis gladiatorum among wrestlers in Adana, Turkey. Med Mycol. 2010;48(3):480–5.
Hiruma J, Ogawa Y, Hiruma M. Trichophyton tonsurans infection in Japan: epidemiology, clinical features, diagnosis and infection control. J Dermatol. 2015;42(3):245–9.
Beguin H, Goens K, Hendrickx M, Planard C, Stubbe D, Detandt M. Is Trichophyton simii endemic to the Indian subcontinent? Med Mycol. 2013;51(4):444–8.
Nenoff P, Uhrlaß S, Krüger C, Erhard M, Hipler UC, Seyfarth F, et al. Trichophyton species of Arthroderma benhamiae–a new infectious agent in dermatology. J Dtsch Dermatol Ges. 2014;12(7):571–81.
Hubka V, Peano A, Cmokova A, Guillot J. Common and emerging dermatophytoses in animals: well-known and new threats. In: Seyedmousavi S, de Hoog GS, Guillot J, Verweij PE, editors. Emerging and epizootic fungal infections in animals. Berlin: Springer; 2018. p. 31–79.
Philpot CM, Bowen RG. Hazards from hedgehogs: two case reports with a survey of the epidemiology of hedgehog ringworm. Clin Exp Dermatol. 1992;17(3):156–8.
Phaitoonwattanakij S, Leeyaphan C, Bunyaratavej S, Chinhiran K. Trichophyton erinacei onychomycosis: the first to evidence a proximal subungual onychomycosis pattern. Case Rep Dermatol. 2019;11(2):198–203.
Marples MJ, Smith J. The hedgehog as a source of human ringworm. Nature. 1960;188(4753):867–8.
Kim J, Tsuchihashi H, Hiruma M, Kano R, Ikeda S. Tinea corporis due to Trichophyton erinacei probably transmitted from a hedgehog. Med Mycol J. 2018;59(4):E77–E9.
Rhee DY, Kim MS, Chang SE, Lee MW, Choi JH, Moon KC, et al. A case of tinea manuum caused by Trichophyton mentagrophytes var. erinacei: the first isolation in Korea. Mycoses. 2009;52(3):287–90.
Hsieh C-W, Sun P-L, Wu Y-H. Trichophyton erinacei infection from a hedgehog: a case report from Taiwan. Mycopathologia. 2010;170(6):417–21.
Papegaay J. About pathogenic fungi on human skin around Amsterdam. Neth J Med. 1925;69:879–90.
Gupta AK, Williams JV, Zaman M, Singh J. In vitro pharmacodynamic characteristics of griseofulvin against dermatophyte isolates of Trichophyton tonsurans from tinea capitis patients. Med Mycol. 2009;47(8):796–801.
Dolenc-Voljč M, Gasparič J. Human infections with Microsporum gypseum complex (Nannizzia gypsea) in Slovenia. Mycopathologia. 2017;182(11–12):1069–75.
Shalaby MFM, El-din AN, El-Hamd MA. Isolation, identification, and in vitro antifungal susceptibility testing of dermatophytes from clinical samples at Sohag University Hospital in Egypt. Electron Physician. 2016;8(6):2557–67.
Romano C, Massai L, Gallo A, Fimiani M. Microsporum gypseum infection in the Siena area in 2005–2006. Mycoses. 2009;52(1):67–71.
Rezaei-Matehkolaei A, Makimura K, Graser Y, Seyedmousavi S, Abastabar M, Rafiei A, et al. Dermatophytosis due to Microsporum incurvatum: notification and identification of a neglected pathogenic species. Mycopathologia. 2016;181(1–2):107–13.
Iwasawa MT, Togawa Y, Akita F, Kambe N, Matsue H, Yaguchi T, et al. Kerion celsi due to Arthroderma incurvatum infection in a Sri Lankan child: species identification and analysis of area-dependent genetic polymorphism. Med Mycol. 2012;50(7):690–8.
Do N-A, Nguyen T-D, Nguyen K-L, Le T-A. Distribution of species of dermatophyte among patients at a dermatology Centre of Nghean province, Vietnam, 2015–2016. Mycopathologia. 2017;182(11–12):1061–7.
Rezaei-Matehkolaei A, Jahangiri A, Mahmoudabadi AZ, Najafzadeh MJ, Nouripour-Sisakht S, Makimura K. Morpho-molecular characterization of soil inhabitant dermatophytes from Ahvaz, southwest of Iran, a high occurrence of Microsporum fulvum. Mycopathologia. 2017;182(7–8):691–9.
Shadomy S. In vitro antifungal activity of clotrimazole (Bay b 5097). Infect Immun. 1971;4(2):143–8.
Adimi P, Hashemi SJ, Mahmoudi M, Mirhendi H, Shidfar MR, Emmami M, et al. In-vitro activity of 10 antifungal agents against 320 dermatophyte strains using microdilution method in Tehran. Iran J Pharm Res. 2013;12(3):537–45.
Baghi N, Shokohi T, Badali H, Makimura K, Rezaei-Matehkolaei A, Abdollahi M, et al. In vitro activity of new azoles luliconazole and lanoconazole compared with ten other antifungal drugs against clinical dermatophyte isolates. Med Mycol. 2016;54(7):757–63.
Salehi Z, Shams-Ghahfarokhi M, Razzaghi-Abyaneh M. Antifungal drug susceptibility profile of clinically important dermatophytes and determination of point mutations in terbinafine-resistant isolates. Eur J Clin Microbiol Infect Dis. 2018;37(10):1841–6.
Ansari S, Ahmadi B, Norouzi M, Ansari Z, Afsarian MH, Lotfali E, et al. Epidermophyton floccosum: nucleotide sequence analysis and antifungal susceptibility testing of 40 clinical isolates. J Med Microbiol. 2019;68(11):1655–63.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Gharaghani, M. et al. (2021). Trends in Epidemiology of Dermatophytes in Iran. In: Bouchara, JP., Nenoff, P., Gupta, A.K., Chaturvedi, V. (eds) Dermatophytes and Dermatophytoses. Springer, Cham. https://doi.org/10.1007/978-3-030-67421-2_13
Download citation
DOI: https://doi.org/10.1007/978-3-030-67421-2_13
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-67420-5
Online ISBN: 978-3-030-67421-2
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)