
Abstract
Studies in adult humans and animals have demonstrated that sleep and body thermoregulation are closely linked. In a cool or warm environment, there is a functional conflict between the need for sleep and the maintenance of body homeothermia. This conflict might be especially harmful in infants.
This chapter reviews sleep-thermoregulation interactions in neonates and infants, together with the implications of these interactions: thermoregulatory responses can differ according to the sleep stage, and sleep can be deteriorated or improved by a non-thermoneutral environment or by slight manipulations of body temperatures.
In contrast to adults, the neonate’s thermoregulatory system is fully operational during rapid eye movement (REM) sleep, which protects him/her from long periods of poikilothermy. The lack of data on this aspect in older infants or adolescents means that we do not currently know when the switch from neonatal characteristics (greater thermoregulatory efficiency and a greater amount of REM sleep when exposed to a cool environment) to adult characteristics (i.e., poor thermoregulatory efficiency and partial REM sleep deprivation in cool or warm conditions) occurs.
In adults, sleep is regulated in parallel with the circadian rhythm in body temperatures. Similarly, distal skin vasodilation before sleep can be observed as a part of “sleep preparedness” in infants (from preterm neonates to older children). This vasodilation is observed despite age-related differences in sleep structure, rhythm and maturation, and thermoregulatory functions and centers.
These observations raise the question of whether thermal or nonthermal manipulation could improve infants’ sleep by inducing distal cutaneous vasodilation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Sleep
- Thermoregulation
- Body temperature
- Metabolism
- Neonate
- Child
- Rhythm
- Thermoneutrality
- Non-shivering thermogenesis
- Sweating
Introduction
Studies performed in animals have demonstrated that thermoregulatory responses are abolished during rapid eye movement (REM) sleep. In cats, Parmeggiani and Rabini [1] demonstrated that the body temperature change was not correlated with environmental temperatures in REM sleep—in contrast to the situation during non-REM (NREM) sleep. Similar results were obtained in kangaroo rats [2] and other mammals. These results suggest that a poikilothermic state operates during REM sleep—probably due to a transient, reversible inactivation of the central controller [3]. These observations led to several conclusions: (i) sleep and body thermoregulation are closely linked, (ii) the two processes interact, and (iii) REM sleep is characterized by a conflict between sleep needs and the maintenance of body homeothermia. As a result, partial or total REM sleep deprivation can be observed in animals sleeping in a cold or in a hot environment.
This functional conflict raises the question of whether thermoregulation during REM sleep is efficient in humans sleeping in a cool or warm environment. This question is of particular interest because of the longer duration of the REM episodes. This question was first addressed in adults and soon after in neonates. However, to the best of our knowledge, it has never been analyzed in older infants or adolescents. The studies performed in adults showed that in contrast to non-human mammals, thermoregulatory processes in REM sleep were depressed (but not abolished) in both cold [4] and warm environments [5].
This question is also of importance for the well-being of neonates, older babies, and infants when considering the paramount importance of sleep quantity and quality in neurodevelopment and good health in these more vulnerable populations. In the neonate, impaired thermoregulation during long episodes of REM sleep (lasting up to 1 hr) might be very harmful, since they can expose the child to significant, rapid heat exchanges with the environment at a time when the body’s thermoregulatory capabilities are not fully efficient. This also represents a challenge for babies and older infants, even though the latter’s thermoregulatory systems are more efficient. It is difficult to extrapolate the results obtained in adults to neonates or infants. Along with the difference in neural development, sleep and thermoregulation processes and rhythms develop progressively at these ages. In particular, there are marked differences between active sleep in neonates and REM sleep in adults. Moreover, because of the polyphasic nature of sleep (3- to 4-h sleep-wake cycles spread out across the 24-h period in neonates or with 1 or 2 daytime naps in babies and preschool infants), a single, long-lasting nighttime sleep period is not present yet, so that circadian processes and sleep pressure may act differently on sleep onset and maintenance than in adults.
This chapter reviews the functional interactions between sleep and thermoregulatory processes in neonates and infants, together with the implications of these interactions: thermoregulatory responses can differ according to the sleep stage, and sleep can be deteriorated or improved by a non-thermoneutral environment or by the manipulation of body temperatures.
Thermoregulation in Neonates and Infants
Basic Principles
Like adult humans, neonates and infants are homeotherms; they can maintain a constant body temperature despite changes in the surrounding environment. Homeothermia is achieved when the sum of metabolic heat production and heat loss from the body to the environment is nil.
Homeothermic organisms are able to control heat transfers and heat production through autonomic and behavioral responses in which the central nervous system has a leading role. The processes underlying these responses are not elicited in a specific range of air temperatures defined as the thermoneutral range , within which the body temperature (usually measured as the rectal temperature) is kept between 36.5 °C and 37.5 °C by merely changing the peripheral skin blood flow, and the metabolic heat production is minimal. In the adult, the thermoneutral range is defined by a narrow range of air temperatures (1–2 °C) and is also representative of the level of thermal comfort. In neonates, this temperature zone corresponds to optimal nursing conditions for vital functions and body growth. In premature neonates, the thermoneutral zone is narrower still; indeed, in very-low-birth-weight neonates, the width of the thermoneutral zone could be less than a single °C [6]. In infants, there is evidence that a narrow thermoneutral range is associated with delayed development of the central nervous system [7]. In neonates aged 3 months or less, the critical lower boundary of the thermoneutral zone varies greatly from one individual to another, and this variability is greater at the age of 3 months [8].
Above the upper boundary of the thermoneutral zone and below the latter’s lower boundary, thermoregulatory processes are the only means of preventing body temperature changes. Although several hypotheses for the functioning of the thermoregulatory system have been put forward [9], most models are based on the fact that internal and peripheral warm and cold receptors transmit afferent information to a central controller, which integrates the information and triggers thermal responses by effectors through efferent signals. The central controller (though to be mainly located in the preoptic area and anterior hypothalamus) has a major role in both sleep regulation and thermoregulation; consequently, it is especially involved in the functional interaction between the two [for a review, see 10]. Neuronal activity of the warm-sensitive neurons in the preoptic area and anterior hypothalamus increases at sleep onset and decreases prior to awakening and during wakefulness [11]. Changes in skin or core temperature modulate the firing rate of these warm-sensitive neurons. Boulant and Hardy [12] have shown that skin temperatures have a strong impact on the activity of warm-sensitive neurons; this might be a sleep-promoting signal.
The models of thermoregulation are adapted from control system theory and are based on hypothalamic sensitivity and the concept of a reference value (i.e., a set-point value). The central controller might asses the difference (signal error) between the set point and the controlled temperature levels measured by thermal sensors, in a negative feedback process. The most widely accepted model was developed by Hammel et al. [13]. According to these researchers, the set-point value can be adjusted as a function of several factors, including skin temperature levels, alertness, circadian rhythms, sleep, and fever. Thermal responses (changes in vasomotor tone, shivering, non-shivering thermogenesis, sweating as described below) are mediated according to the sign of the signal error, in order to keep the controlled temperature within a narrow range. The intensity of these responses (defined as a gain, i.e., the slope of the relationship between the thermal response and the controlled temperature) can be constant, since the responsiveness of the hypothalamic structures is only modified when changes in skin temperature reset the set-point value. Other studies describe the central controller’s contribution as an increase in the gain of the thermoregulatory function in response to skin temperature signals, without any change in the set-point temperature [5, 14, 15]. Although the validity of these various concepts of thermoregulation control is still subject to debate, they do explain a lot of observations.
As temperatures are not regulated uniformly from one body region to another, the concept of a single, regulated temperature of 36.5–37.5 °C remains questionable. This uniform temperature is not the overall body temperature. The body can be divided into two parts: a core including organs such as the lungs, heart, abdominal organs and brain (whose temperature is almost constant at between 36.5 and 37.5 °C) and a peripheral “shell” corresponding to skin layers (whose temperature is highly variable). In the adults, the skin can be divided into “hot” regions (above 36.5 °C) where the large arteries are close to the surface (such as the cheeks and the inguinal region), “warm” regions (above 33.5 °C, the skin of the limbs), and “cold” regions (below 33.5 °C, such as the extremities). Indeed, blood flow is controlled and regulated differentially in each body region. In preterm neonates (postnatal age: 28 days; body mass: 2300 g) nursed at thermoneutrality in a closed incubator, the regional thermal profile is less heterogeneous than in the adults. The highest skin temperatures are measured at the nape of the neck (37.05 °C), whereas the lowest values are recorded over the upper arms and feet (35.53 and 35.54 °C, respectively) [16]. The thermoregulatory system’s output results from the spatial integration of these various temperatures. Although this thermal heterogeneity generates variations in the afferent nervous information sent to the central controller, most models consider that the core or internal temperature (measured as the rectal, esophageal, axillary, or tympanic temperature) is the sole controlled variable.
In contrast to children and adults, neonates are particularly at risk of thermal stress . They have less efficient thermoregulatory responses, and relatively greater body heat losses to the environment—notably as a result of a high surface-area-to-body-volume ratio (0.8, 0.6 and 0.2 cm−1 in premature neonates, term neonates, and children weighing 20 kg, respectively) [17]. Neonates have less insulation from subcutaneous tissue, which increases thermal conductance and constitutes a further disadvantage when faced with cold. Moreover, the convective and evaporative heat transfer coefficients in neonates are greater than those in adults (promoting heat loss), as a result of the strong curvature of the body segments. The more immature the neonate, the larger the body heat losses. Comparing two mannequins representing small neonates of 900 and 1800 g, Elabbassi et al. [18] showed that the overall dry heat loss by convection, conduction, and radiation was 20.4% higher for the smaller mannequin.
Hence, neonates can become rapidly hypothermic; in addition to their disadvantageous physical characteristics, their thermoregulatory processes are not fully efficient and the energy available for maintaining body temperature is limited—increasing morbidity and mortality rates.
Thermoregulatory Parameters and Sleep Stage Effects in the Thermoneutral Range
The thermal responses controlled by hypothalamic structures differ from one sleep stage to another. This can be observed even within the thermoneutral range.
Oxygen consumption is greater in REM sleep than in NREM sleep in full-term neonates—at least during the first week of life [19,20,21], at 2 or 3 weeks of age [22], and 3–4 months of age [8, 23]. The situation for preterm neonates is subject to more debate, since the sleep stage difference in oxygen consumption was not always statistically significant—perhaps because the babies were more premature (33–35 weeks of gestation, studied between 3 and 17 days of age) [24].
In full-term babies aged 5 hr. to 7 days, skin blood flow (measured at the forehead) is greater (by 28%) during REM sleep than during NREM sleep (scored using behavioral criteria); this results (at least in part) from greater autonomic nervous system activity during REM sleep [25]. In full-term 3-day-old neonates, overall body heat loss was found to be greater during REM sleep; however, water loss did not differ significantly, except when specifically considering the transition from NREM sleep to REM sleep (it was higher in REM sleep) [20].
In a study of infants aged 2–26 weeks, nighttime body temperature patterns showed periodic ultradian oscillations with a period of approximately 1 hour; these oscillations might reflect alternating REM and NREM sleep stages [26]. The esophageal temperature is higher during REM sleep in preterm neonates reaching term [27]. A significant decrease in rectal temperature had already been observed during the REM-NREM transition in full-term neonates but not in preterm neonates reaching term [28]. With a larger sample size, the same group of researchers evidenced sleep stage differences in rectal and skin temperatures in both preterm and full-term neonates [29]. Richard [30] observed that the increase in axillary temperature due to mother–infant bed-sharing was mostly restricted to NREM sleep, and further suggested an explanation based on infant homeostasis, rather than passive body heating by mother heat-flux. In the study by Ammari et al. [31], however, skin temperatures and thermal gradients were similar in REM and NREM sleep stages.
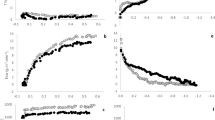
Body temperature patterns during a given episode of sleep also differ from one sleep stage to another. During NREM sleep, the esophageal temperature and the mean skin temperature both decrease over the course of the episode. In contrast, both temperatures increase significantly during REM sleep episodes. Oxygen uptake decreases during episodes of REM sleep but only when the latter is followed by an episode of NREM sleep [27]. This explains why the direction of the sleep state change (i.e., REM to NREM, or vice versa) may be relevant, and might explain also the discrepancies reported in the literature. The direction of the sleep state change has rarely been studied, however.
In preterm and term neonates, the variability of all the following thermoregulatory parameters is always greater in REM sleep: rectal but not skin thoracic temperatures [29], forehead blood flow [25], respiratory rate [32], metabolic activity [19]). This results from the predominant parasympathetic activity during NREM sleep (during REM sleep, parasympathetic activity decreases and sympathetic activity increases) [33].
Physiological Adjustments to Cold, and Sleep Stage Effects
When exposed to a cold environment, peripheral vasoconstriction occurs first, and directs venous blood from the peripheral skin layers to the deeper venous network. This process (which takes place within a few minutes) increases the insulating value of peripheral tissues, increases the internal-to-skin temperature difference, and decreases body heat losses (by convection, radiation, and conduction) to the surroundings. Distal skin regions contain arteriovenous anastomoses, which are primarily innervated by the sympathetic nervous system. As a result, vasoconstriction is more pronounced at the extremities than on the trunk; hence, the distal-to-proximal skin temperature gradient (DPG) increases. This difference is often considered to be an early marker of thermal stress [34, 35]. Lindqvist et al. [36] have observed that in neonates, vasomotricity is controlled more by the sympathetic system than by the parasympathetic system.
Brück et al. [37] reported that the thermoregulatory modulation of vascular tone is mature and functional in full-term neonates. In preterm neonates (weight <1000 g), this control is absent at birth but develops over the following 2–3 days [38]. However, there is evidence to show that the peripheral vasomotor responses of very premature infants are impaired during the first few hours after birth [39, 40], even though their arteriovenous anastomoses are functional [41]. Knobel et al. [40] pointed out that hypothermic small neonates (weighing 800 g) did not exhibit peripheral vasoconstriction during the first 12 hours of life. Taking into account Lyon et al.’s report [38] that peripheral vasoconstriction only occurred in neonates aged over 5 days, Knobel et al. [40] assumed that the increase in peripheral vasoconstriction capacity as a function of postnatal age was due to neuronal maturation. However, it has been observed that peripheral vasoconstriction can occur in body extremities (the hand, foot, and calf regions) in premature and term neonates [42]. Berg et al. showed that a fall in the air temperature of 4.5–8 °C decreased the peripheral blood flow by 36% [42]. In neonates with a gestational age of 33–36 weeks, peripheral vasoconstriction in the foot was combined with a release of vasomotor tone on the trunk [43], which limited the efficiency of this mechanism in response to cold exposure. The heat loss response to cold stress is age-dependent, since the rate of blood flow in the arteriovenous anastomoses begins to decrease during childhood [41]. Several studies have shown that in the cold, cutaneous vasoconstriction is greater in prepubertal infants than in adults [44,45,46]. A similar finding was reported by Tsuzuki et al. [47], who showed that the local skin temperatures at the hands and feet were greater in children (aged 15 months to 3 years) than in the mothers (aged 29 to 40 years), as a result of greater vasoconstriction.
Although the initial thermoregulatory response to cool exposure is peripheral skin vasoconstriction, there are few data on the effects of sleep stage on this process in a cool environment.
In a second response to cold exposure, metabolic heat production is increased through non-shivering thermogenesis (NST). This metabolism thermal response mainly involves the brown adipose tissue (BAT) . However, organs such as the liver or the brain (due to their high metabolic heat production) and tissues such as white adipose tissue also contribute to metabolic heat production. Given its large mass and relatively high oxygen consumption, the brain can warm the body. White adipose tissue not only provides free fatty acids to organs involved in thermogenesis but also produces heat directly. The metabolism in BAT is controlled by sympathetic innervations, and this tissue can produce a significant amount of heat. Most of the BAT is located in the thoracic, cervical, and paravertebral regions. The tissue’s location and ample blood supply mean that the generated heat warms the spinal cord, the heart, and the thorax as a whole—making it possible to increase cold resistance. At between 22 and 29 weeks of gestation, the BAT constitutes the majority of the neonate’s fat stores. At birth, a neonate weighing 3000 g has 40 g of BAT (about 11% of the body’s fat). However, the amount of BAT increases by a factor of 1.5 between the third and fifth weeks of life. Clarke et al. [48] have demonstrated that lambs delivered by cesarean section had a lower level of thermogenic activity (by 50%) in the BAT than those born vaginally; the level was similar to that of a fetus after 145 days of gestation. This was probably because the postpartum level of guanosine 5′-diphosphate (GDP) did not rise in these animals. Recent studies have suggested that BAT may have a key role in sleep promotion, and that this organ may be influenced by the interaction between sleep and body temperature [49].
Heat can also be generated through shivering thermogenesis . This thermal response to cold exposure appears progressively with age, and does not exist in the neonate—except when cold exposure is very strong [50]. Classically, shivering is induced by the cooling of the skin. However, a drop in the internal temperature drop can also induce shivering thermogenesis, even when the skin temperature is normal or elevated. Shivering thermogenesis involves two pathways. The first is muscle activity; this consists of rapid rhythmic, muscle contractions, starting in the scapular region. Synchronization with the antagonistic muscles makes it possible to combine the shivering with body movements. In neonates, shivering cannot be the major process in heat production, since the skeletal muscle system is not mature. The second pathway results from a transfer of energy chemical processes related to the stimulation of cellular metabolism by sympathetic activation and thyroid hormones.
As reported by several researchers [44, 45], metabolic heat production in response to cold exposure is greater in prepubertal infants than in adults. Combined with more efficient peripheral vasoconstriction, children can maintain similar [45] or higher body temperatures [44] than adults.
When exposed to a cool environment (an air temperature 3–5 °C below thermoneutrality), metabolic heat production increases in both 1-week- and 3-month-old infants [8]. Even premature infants (33–35 weeks old) were able to increase their oxygen consumption in all sleep stages [24]. All the literature data argue in favor of active, efficient thermoregulation during REM sleep in neonates.
Although the metabolic response to cooling varies widely from one neonate to another, it is usually assumed to be more intense during REM sleep than during NREM sleep in full-term neonates from the first week of life [20, 51] until the age of 3 months [8]. However, this difference is subject to debate [19, 24].
Since the thermal response during REM sleep is at least equivalent to (or more intense than) that recorded during NREM sleep, the sleep-stage-specific differences in oxygen consumption as observed at thermoneutrality are increased on cool exposure [52].
When the cool thermal load was prolonged (75 hr., thermoneutrality—2 °C, at 37 weeks of postconceptional age), the esophageal temperature difference between REM and NREM sleep disappeared, whereas oxygen consumption increased less in REM sleep (by 20%) than in NREM sleep (by 33%); furthermore, the inter-sleep stage difference was no longer present at the end of the cool exposure [53].
In individual neonates , we observed a negative correlation between oxygen consumption on the one hand and the esophageal and skin temperatures on the other hand when exposed to cool challenge [22]. In 5 of the 9 neonates, the metabolism increased when body temperatures decreased—demonstrating that closed-loop regulation (suggestive of a classical non-shivering thermogenesis response) is fully operative during REM sleep. Unfortunately, the small number of NREM sleep episodes prevented us from directly assessing this relationship in NREM sleep and thus probing potential sleep stage differences in the regression line’s slope (the gain of the response) and the intercept (the set point) [22].
Physiological Adjustments to Heat, and Sleep Stage Effects
In warm environments, the main heat loss responses are the release of the skin vasomotor tone and evaporative skin cooling (due to sweating).
There are few published data on the changes in peripheral blood flow in premature and low-birth-weight neonates exposed to hot environments—partly because the latter are less frequently encountered than cool conditions in nursing care. Likewise, sleep-stage effects on these responses have not—to the best of our knowledge—been analyzed in older infants. It is commonly accepted that the skin blood flow response to a rise in body temperature decreases with age [54, 55]. The higher peripheral blood flow and reduced cardiac output observed in young infants [56] increase the cardiovascular strain during heat exposure.
For preterm neonates, the heat loss by evaporation occurs by transcutaneous water loss . The skin is highly permeable because the epidermal barrier to water diffusion has not fully developed.
Active thermal sweating does not operate in the neonate before 37 weeks of gestational age [57], except when the body temperature is very high (i.e., rectal temperature ˃37.9 °C [58]. In mature neonates, thermal sweating occurs successively on the forehead, trunk, and limbs. Foster et al. [59] found that (i) the sweat gland density is higher in neonates than in adults but (ii) the maximum sweat output per gland in the neonate after intradermal injection of acetylcholine is only one-third that found in the adult. Likewise, the sweating rate response in prepubertal children is lower than in adults, despite a higher sweat gland density [60] and independently of the gender [61]. Lower sweating rates with ageing are mainly attributed to a decrease in sweat output per gland [62] and/or a higher threshold for sweating onset [63]. However, a possible age-related decrease in the hypothalamic set-point temperature for sweating (i.e., from premature infants to adults) cannot be ruled out [64].
When measuring water loss in neonates, it is difficult to discriminate between transcutaneous water loss and active sweating; this is especially problematic in preterm neonates. In a closed incubator, Okken et al. [65] reported a water loss rate of 1.04 ± 0.24 mL.kg−1.hr.−1 for preterm neonates (body mass: 1520 g; gestational age: 31 weeks; postnatal age 13 days) nursed under thermoneutral conditions. This water loss can lead to hypothermia and dehydration if appropriate preventive measures are not taken. Transcutaneous water loss decreases with postnatal age, as a consequence of the increase in the keratin content of the epidermis stratum corneum [66]. Thus, Wu et al. [67] showed that insensible water loss through the skin and respiratory tract in premature neonates can be four times that measured in term neonates. An old study performed on children aged from 5 months to 4 years found that the sweat rate was higher at sleep onset than during wakefulness [68]. Unfortunately, this work did not include a sleep stage analysis. Some recent studies [20] (but not others [8, 22]) have found a sleep stage effect on water loss at thermoneutrality.
In a slightly warm environment (thermoneutrality +2 °C, +0.23 °C for the esophageal temperature, and + 0.33 °C for the skin temperature), evaporative skin water loss in preterm neonates increased significantly (+66%) but there were no sleep state differences. Individual positive regressions between water loss and esophageal and skin temperatures measured during REM sleep episodes suggested that controlled, active process were operating—in line with what was observed in a cool environment [22].
Despite the differences in the thermoregulatory responses observed between adults and prepubertal infants, the respective body temperatures do not differ when they are exposed to heat stress [69, 70].
Behavioral Thermoregulation
As with autonomic regulation, behavioral regulation keeps the body temperature as constant as possible by acting on the external environment through various strategies. These involve the motor system and the creation of a microenvironment that protects the organism against fluctuations in the external thermal environment (i.e., avoidance reactions). Behavioral regulation precedes autonomic regulation and can be considered as an anticipatory avoidance reaction triggered by the peripheral perception of thermal stress. Indeed, behavioral regulation requires peripheral and internal temperature sensitivities and a central nervous component that partly overlaps with the autonomic regulation pathway. The motor effectors are different, however, and are stimulated via corticospinal and mesencephalic pathways. The mesencephalon is significantly involved in avoidance reactions. Thus, neonates can increase thermogenesis through muscle activity [22]. Body movements can also reflect discomfort upon cool exposure, interrupt sleep continuity, and induce sleep stage changes or awakenings. As expected, body activity increases when preterm neonates are exposed to a cool environment [71]; this often leads to the infant waking up [8]. Increased body activity is more pronounced in 1- to 3-month-old full-term babies than in younger ones, whatever the sleep stage [8, 51]. In preterm neonates, we have observed concomitant increases in the frequency and mean duration of body movements but only during REM sleep, which is already characterized at thermoneutrality by greater durations and frequencies of body movement. Four of the 9 neonates exhibited a positive individual correlation between oxygen consumption and internal temperature (but not skin temperature), which reflected greater body movements while sleeping in response to a lower internal temperature [22]. It is not clear how effective this process really is because the motor system is not well developed [72], and some studies have not observed this increase in body movement in response to cold [73].
When faced with cold or heat challenges, neonates can assume postures that change the skin surface area exchanging heat with the environment. Harpin et al. [58] showed that neonates were less active and adopted a relaxed “spread-eagle” position when exposed to a hot environment (an incubator air temperature of up to 39.9 °C). This behavioral thermoregulatory response is also observed in some immature infants (˃30 weeks of gestational age). Using a mannequin representing a neonate with a weight of 3300 g and a surface area of 0.23 m−2, Wheldon et al. [74] showed that the skin surface area for heat exchange increased from 0.48 for a fetal position (as observed in cold conditions) to 0.57 for a relaxed position and 0.76 for a spread-eagle position. The heat transfer coefficient for convective heat exchanges (promoting radiant and convective heat losses with the environment) respectively increased from 4.0 to 5.4 W.m−2.h−1.
With the exception of neonates nursed naked in an incubator (i.e., neonates requiring a highly controlled environment), clothing insulation is also a relevant component of behavioral thermoregulation. More mature infants usually sleep clothed, which considerably reduces heat loss but can increase the risk of body overheating. In sleeping adults wearing pajamas and covered by two cotton sheets and a single woolen blanket, Candas et al. [75] showed that the air temperature of the microclimate inside the bed was respectively 28.6, 29.6, and 29.7 °C for room temperatures of 16, 19, and 22 °C. The creation of an approximately thermoneutral microenvironment in the bed helps to protect the sleep stage structure [76].
Sleep Is Influenced by Non-thermoneutral Conditions
The impact of non-thermoneutral conditions on sleep has mainly been studied in neonates or older babies, given their greater vulnerability (especially regarding thermoregulation), the relevance of sleep for neurodevelopment, the risk of sudden infant death syndrome, and their relative inability to alert their parents when ambient conditions are harmful.
Sleeping in a Cool Environment
Although the disruption or continuation of the sleep cycle in neonates cannot strictly be described as an alternation between a homeothermic state and a poikilothermic state (in contrast to what is observed in adult animals and, partly, adult humans), sleep can be disturbed by cool exposure even when the latter does not elicit thermal responses.
The first impact concerns sleep duration and continuity . Cold exposure (by as much as 4 °C below thermoneutrality) increases the frequency of awakening in preterm neonates [43, 77]. Similarly, moderate cool challenges (1.5 °C below thermoneutrality) reduced the total sleep time (by a mean ± standard deviation of 20 ± 44 min) and the longest sustained sleep period, and increased intrasleep wakefulness [78]. These modifications were observed even though thermoregulation was only slightly elicited (vasodilation only, evidenced by a greater internal vs. skin temperature difference and no increase in oxygen consumption). Final spontaneous awakening was earlier (by 21 ± 41 min), and intrasleep wakefulness was longer [27].
Older infants (3- and 4-month-old) also woke up earlier when lightly clad in cool rooms, though their body temperatures were not low [8, 79]. However, 14-week-old Finnish infants slept longer (with an increase of 92 min during the daytime nap, as defined by behavioral criteria) outdoors in northern winter conditions (air temperature between −25.9 and 2.2 °C) than indoors (20.5–26.7 °C). Despite this observation, outdoor sleeping duration was shortened when the skin temperature cooling rate (but not the mean, maximal, or minimal value of any skin temperature) was large or when the outdoor air temperature was low. This apparent contradiction could be explained by the clothing and sleeping bag used in the prams, which restrained the infants’ movements. The researchers suggested that outdoor sleeping makes it possible to sleep swaddled without overheating. They concluded that sleeping outdoors is beneficial as long as the skin temperatures do not fall too much [80], in line with the studies cited below.
As regards sleep architecture , NREM sleep appears to be particularly sensitive to cool thermal stress; indeed, the latter can induce partial or even total NREM sleep deprivation [51]. Cool exposure reduces the total duration of NREM sleep and increases the total duration of REM sleep in full-term neonates [8, 51] and preterm neonates [22, 27, 78, 81,82,83,84]. In preterm neonates, NREM sleep episodes are less frequent, and the longest NREM sleep episode is shorter [82, 84]. Preferential switching from NREM sleep to REM sleep is observed [78]. Thus, neonates exposed to cool environment favor REM; this leads to greater expenditure of metabolic energy for thermoregulatory needs rather than energy conservation (which would be greater during NREM sleep but might compromise body homeothermia). This pattern is even observed for low-magnitude thermal stress.
Decrease of the ambient temperature or the core body temperature is associated with a greater amount of REM sleep [8, 22], which decreases the NREM/REM sleep ratio and/or the number of transitions from NREM sleep to REM sleep [19]. REM sleep episodes were more frequent but less frequently followed by an NREM sleep episode, and more frequently followed by wakefulness [27, 78]. It is noteworthy that the effects of cold exposure on REM sleep episodes differ according to an episode’s outcome: REM sleep episodes followed by NREM sleep were shortened (by 17 ± 28 min, on average) and less frequent, whereas REM sleep episodes followed by wakefulness were lengthened. The outcome of REM sleep in neonates is not related to a specific body temperature value at the time of the sleep stage transition. In contrast, a low esophageal temperature at the beginning of the REM sleep episode and/or a progressive rise in this temperature enhance the transition towards wakefulness [27].
This switching from NREM sleep to REM sleep is relevant from a thermoregulatory viewpoint. Interestingly, neonates exhibiting the greatest increase (by 41%) in metabolic heat production during NREM sleep did not switch into REM sleep [51]. Moreover, the modification of NREM sleep and REM sleep was less frequent in 3-month-old infants because most of them woke briefly at the beginning of the cooling procedure [8]. Consistently, the shorter NREM sleep episodes [51] and the longer REM sleep episodes observed in 1-week-old, full-term neonates [8] were not statistically significant in 3-week-old preterm neonates [27].
In another study, a 5 °C difference in the incubator air temperature between daytime and nighttime did not lead to sleep disturbances; however, this might have been due to a nycthemeral effect blunting the temperature effect and/or a small sample size [85].
During chronic cool exposure (75 hr., 2 °C below thermoneutrality, 37 weeks postconceptional age), the neonates’ sleep structure and duration did not improve (and continued to deteriorate, in fact) after thermal adaptation (as inferred by greater metabolic heat production during the last exposure than during the first cool exposure) [53]. Hence, protective mechanisms for maintaining body temperature do not interact with sleep mechanisms—in contrast to the situation in adults [86].
Sleeping in a Warm Environment
A warm environment (thermoneutrality +2 °C, +0.23 °C for esophageal temperature, and + 0.33 °C for skin temperature) did not induce any sleep differences in full-term neonates aged 2 or 3 weeks, although the sweating rate was increased (by 66%). Only the body movement frequency fell [22]. Franco et al. [87] did not observe any sleep differences between 11-week-old term infants sleeping at 28 °C and those sleeping at 24 °C, despite some intergroup differences in the body temperature pattern. Likewise, Brück et al. [81] did not observe any sleep modifications.
In a study performed in an earthquake shelter, school children (mean age: 11 years) claimed that heat was the most frequent cause of sleep disturbances. However, it is difficult to determine whether sleep disturbances (as assessed by actigraphy) are due to thermal discomfort and/or a sweaty feeling, rather than other factors (noise, stress, etc.) [88].
Impacts of Thermal Transients on Sleep
Neonates nursed in a closed incubator are often exposed to transient air temperature changes when the incubator door is opened or during a thermal overshoot after the door is closed. A decrease in the air temperature (from 24–27 °C to 18–21 °C over a 20 min period) during an episode of NREM sleep promotes the transition to REM sleep. This switch to a sleep stage associated with higher oxygen consumption was not observed when the latter had increased greatly during the preceding NREM sleep episode. When the air temperature decreased during an REM sleep episode, half of the neonates did not enter NREM sleep [51]. Few of the older (3-month-old) infants remained in the same sleep stage before and after transient cool exposure [8].
During progressive cooling, the REM sleep/NREM sleep ratio decreased in preterm neonates but increased in full-term neonates. Conversely, during a heating transient, the REM sleep/NREM sleep ratio decreased [89].
Sleeping at Thermoneutrality
The above-mentioned studies observed sleep disturbances in a non-thermoneutral environment. Sleep disturbances are observed as soon as (or sometimes even before) thermoregulatory processes are solicited. Indeed, sleep appears to be more sensitive to thermal stress than thermoregulatory parameters are. Kapas and Szentirmai [49] suggested that sleep duration is optimal when the organism does not need to invoke functions that require wakefulness. Thermoregulation is one of these functions, along with other activities related to energy metabolism (feeding, muscle activity, etc.). On the basis of studies of animals and adult humans, one can conclude that (i) sleep in general and REM sleep in particular are optimal within the thermoneutral range, and (ii) the REM sleep duration could be considered as a marker for thermoneutrality. In neonates, NREM sleep appears to be the most sensitive sleep stage, and is be reduced by exposure to a non-thermoneutral environment [27].
It has been observed that adults regulate sleep in phase with the circadian body temperature rhythm. Sleep occurs during the period where the core temperature is relatively low. In particular, increased sleepiness and habitual sleep onset occur when the core temperature is decreasing. Conversely, the likelihood of awakening increases as the core temperature increases in the morning. Distal (foot and hand) skin temperatures vary in the opposite way to the core temperature.
In 1938, Magnussen (cited in [90]) suggested that vegetative sleep preparedness starts around 100 min before sleep onset. The first step is skin vasodilation; this is particularly pronounced on the distal regions with the greatest vasomotricity (due to arteriovenous anastomoses [for a review, see 91]), which increases the heat losses to the environment and thus decreases the core body temperature. Bedtime and sleep onset usually occur just after or close to the most rapid decline in core temperature. However, the core body temperature decrease is probably a consequence of the distal skin heat loss, which initiates sleep per se [92]. In mechanistic terms, it is hypothesized that increased distal skin temperature stimulates the discharge of warm-sensitive neurons in the preoptic area and anterior hypothalamus. This induces a downwards shift of the set-point value for the vasomotor tone, and thus facilitates and improves sleep. Among various candidates (the core body temperature, the melatonin level, the heart rate, the subjective sleepiness rating…), the DPG (a marker of the vasomotor tone) is the best predictor of sleep onset [93].
As a result, many changes (including sympathovagal changes) occur at least 30 min before sleep onset [94]). These changes are linked to sleep per se (rather than to lights-off) and have a role in initiating sleep.
Interestingly, the relationship between simultaneous changes in sleep propensity and body temperature rhythms is causal relationship. Several studies in adults have shown that experimentally induced distal vasodilation promotes sleep (see below). This raises the question of whether the causal relationship also operates during development in infants, whose sleep is polyphasic and whose circadian rhythms are less tightly controlled.
Temperature Circadian Rhythm in Infants and Its Relationship to Sleep
Body temperature rhythm per se is one of the first circadian rhythms to appear in babies. According to Bueno and Menna-Barreto [95] the endogenous circadian system that regulates body temperature may be functional as early as 29 weeks of gestation. Longitudinal studies show that the temperature rhythm becomes more robust between birth and the age of 3 months [96], and that the rhythm at 6 months of age is already similar to that observed in young adults [97]. The rhythm increases in amplitude between 7 months and 7 years of age, and achieves an adult-like pattern at the age of 7 years [98].
Discrepancies in the literature data regarding the age at which the circadian body temperature rhythm appears can be attributed to high interindividual variability and the fact that the emergence of circadian rhythms depends on many environmental parameters (light levels, hospital vs. home differences, etc.), care-related parameters (the feeding schedule, etc.) and/or the mother and baby’s characteristics (maturation, intra-uterine growth, prematurity, etc.) [for a review, see 96]. These researchers concluded that sleep and circadian rhythms are already coupled in infants but that their time course of development is not necessarily comparable [96].
Body Temperature Rhythm According to Sleep
Even though Richard [30] has suggested (on the basis of anthropological data) that the “normal” sleep temperature profile (defined here as mother-baby co-sleeping) does not include a large drop in core temperatures at sleep, most researchers have demonstrated that the core temperature is higher when the baby is awake and falls with sleep [99]. In a study of 3–4-month-old babies sleeping at home, Wailoo et al. [100] observed that the rectal temperature (which was above 37 °C before the baby was put in its cot) fell by 0.8 °C over the following hour. The temperature then stabilized and rose slightly after 5 hr. Similarly, Tsogt et al. [101] observed a mature, diurnal temperature change pattern in 3-month-old infants: a fall in core temperature and an elevated peripheral temperature during the night, that is, probably after sleep onset (although sleep was not measured). The opposite pattern was observed later in the night, that is, probably before early awakening. This is observed by the age of 6 weeks, regardless of whether sleep occurs during the day or the night [102]. The older the baby, the greater the fall in rectal temperature after sleep onset [103].
In preterm infants aged 9 days, we observed similar results [104]. Foot and hand distal temperatures increased (by 0.38 °C and 0.15 °C, respectively) during the 20 min before nocturnal sleep onset (as determined by polysomnography), leading to a greater DPG (by 0.52 and + 0.30 °C/20 min, respectively). During the same period, the abdominal skin temperature (often considered as a marker of the core body temperature) did not vary significantly. In contrast to older infants and adults, the increase in distal temperature stopped after sleep onset. Differences in sleep between neonates, older infants, and adults might account for this specificity; in neonates, REM sleep appears first after sleep onset (and is characterized by an increase in sympathetic tone), whereas the autonomic balance in older infants and adults is in favor of parasympathetic tone and thus NREM sleep after sleep onset.
When considering the 30 min periods before and after sleep onset (as assessed by actigraphy) in 4-month-old term babies, the distal temperatures (but not the proximal temperatures) increased gradually until 10 min after sleep onset and then stabilized. The DPG rose by 0.075 °C/min during the 30 min before sleep onset. However, 7 of the 43 babies did not exhibit a similar pattern, and their distal temperature remains high for up to 45 min after sleep onset. Interestingly, the value of the DPG was correlated with the distal temperature rather than the proximal skin temperature—emphasizing the importance of the distal segments [91].
Abe and Kodama [91] found a lack of individual stability in the pre-sleep body temperature pattern in babies aged 4–9 months. In contrast, Lodemore et al. [105] observed that full-term babies developed mature temperature rhythms (defined here as the age at which the trough rectal temperature fell below 36.6 °C during the nighttime sleep) at a mean age of 11.1 ± 2.5 weeks. This change occurred abruptly (over 1 or 2 days) and was permanent—suggesting that the endogenous mechanism of temperature control was physiologically altered. Lodemore et al. demonstrated that the transition to mature temperature rhythms results from a complex interaction between intrinsic and extrinsic factors, including breast feeding, speed of weight gain, sex, and a supine sleeping position. The noticeable interindividual variability in the time needed to achieve a mature rhythm was associated with the appearance of longer nighttime sleep.
It is generally assumed that because a baby’s body temperature pattern does not depend on the ambient temperature or the thermal insulation (clothing or wrapping), it is internally driven and controlled. However, Franco et al. [87] demonstrated that the rectal temperature fell more rapidly and reached a lower trough value when 11-week-old term babies slept at 24 °C, relative to 28 °C. Moreover, the mature diurnal temperature pattern was not found in 3-month-old babies with traditional Mongolian swaddling, even though this higher degree of thermal insulation did not induce any thermal stress [101]. In contrast, Petersen et al.’s [99] study of 12- to 22-week-old babies did not report any significant effect of the thermal insulation used (which was probably lighter than Mongolian swaddling) on the core temperature level and rhythm—except for the combination of a prone position, heavy swaddling, and a warm room. In the latter situation, body temperatures tended to increase more rapidly at the end of the night but there was no impact on morning awakening. Interestingly, the decrease in core temperature was greater in babies not fed before sleep [106].
Wrist, shin, and foot temperatures show opposite trends (relative to the rectal temperature) [26] and have a one-hour phase advance [95]: these distal skin temperatures increase rapidly over the first hour after sleep onset, and decrease during or shortly before or after awakening. In contrast, the skin temperature measured on the abdomen only rose slightly or remained stable during the first part of the night in 3- to 4-month-old babies [100].
The fact that a baby’s body temperature pattern is in phase with its placement in a cot (and presumably sleep onset) rather than with time of the day, suggests that circadian rhythms do not have a major role at this age. However, a circadian influence is still present, as indicated by a lower fall in rectal temperature during a daytime sleep episode than during a nighttime sleep episode of similar duration [106].
Body Temperatures and Sleep Onset
In infants (5–12 years of age), Murphy et al. [107] observed that a distal (calf) skin temperature and a proximal (subclavicular region) skin temperature increased before bedtime. The distal temperature continued to increase after bedtime, whereas the proximal temperature began to fall slightly. In 6- to 12-year-old infants sleeping in their natural settings, McCabe et al. [108] reported increases in skin temperatures (on the back, neck, foot, and subclavicular region but not the forehead) from 1 hour before the reported bedtime to 2 hours afterwards. The changes were greater for the distal temperature than for the others, and all the changes were reproducible from one night to another. When considering the temperature change around sleep onset (as assessed by actigraphy), the DPG (Tfeet—Tsubclavicular) started to increase 1 hour before sleep onset and continued to do so until 90 minutes after sleep onset. However, the trend for a decrease in the core tympanic temperature from 1 hour before bedtime (the first measurement) to bedtime (the second measurement) did not reach statistical significance but was consistent with literature data in adults. Except for the abdominal temperature, none of the skin temperatures significantly varied before morning awakening.
In a study of preschool children (mean age: 4 years) and their mothers, Okamoto-Mizuno et al. [109] found that proximal temperatures might have a greater role than the foot distal skin temperature—probably as a result of more rapid redistribution of the blood to the proximal regions than to the distal regions at the wake-sleep transition. This discrepancy is unlikely to be due to age-related differences because studies performed in both younger and older populations have evidenced the major role of distal temperatures in prompting the core temperature decline before sleep onset.
Murphy et al. [107] reported that the DPG increased (i.e., distal temperatures rose towards proximal temperatures) before and after sleep onset in 5- to 12-year-old infants. These researchers defined a specific criterion (DPG0°) as the time at which the DPG first crossed 0 °C. In line with the literature data on adults, the study’s results showed that the shorter the time to reach DPG0°, the shorter the sleep onset latency. Interestingly, some of the infants in Murphy et al.’s study had pediatric bipolar disorder; these children displayed both thermoregulatory changes and sleep onset difficulties—suggesting that thermoregulation and emotion regulation share some neural circuits.
In contrast to the results in adults, the value of the DPG at sleep onset in 4- to 9-month-old infants was not correlated with rapid sleep onset and could therefore not accurately predict the sleep onset latency. For example, babies with a high DPG (getting close to 0) did not always fall asleep quickly, since the sleep onset latency ranged from 4 to 68 min. However, Abe and Kodama [91] observed that babies with a DPG value that remained low over the first 15 min after lights off were unlikely to fall asleep rapidly (i.e., within half an hour).
Since there are no easily measured, reliable markers of sleep propensity in neonates with polyphasic sleep, we sought to determine sleep propensity indirectly by studying the duration of the wakefulness episode [110]. This duration was analyzed as a function of body temperatures in 9-day-old preterm neonates. Our results showed that the duration of wakefulness was significantly shorter when distal (foot, hand, and thigh) temperatures measured at the end of the wakefulness episode were high. This was not the case for proximal skin temperatures at any time point or for both distal and proximal skin temperatures at the beginning of the wakefulness episode. Therefore, sleep onset was related to distal skin vasodilation during the wakefulness episode. Our study was also the first to find that regional skin temperature homogeneity (measured over the entire body, including distal and proximal parts of the body) promoted sleep onset: the more homogeneous the skin temperatures, the shorter the wakefulness episode.
Another aspect is sleep maintenance . In a study of babies during the first 6 months of life), Lodemore et al. [102] reported a negative correlation between the trough rectal temperature during the first 4 hours after bedtime and the time to first disturbance of the parents. Hence, the time to first disturbance was an indirect way of analyzing the duration of maintained sleep. The researchers suggested that body temperature and sleep rhythms were associated but could not determine whether the relationship was causal (i.e., whether temperature changes predisposed to longer sleep or vice versa, or whether the two rhythms matured simultaneously but independently).
Impacts of Thermal Manipulations Within the Circadian Body Temperature Range
In adults, the relationship between sleep and body temperature rhythms is causal, since experimentally modifying the body temperature influences sleep. Interestingly, several studies have shown that sleep can be promoted by slight manipulations of the body temperatures (i.e., those producing changes that remain within the everyday circadian range). These manipulations are designed to induce or strengthen skin vasodilation (especially distal vasodilation), increase heat loss, and to achieve a “completely relaxed, one-compartment body” state (i.e., when DPG = 0 °C, i.e., disappearance of the thermoregulatory shell [111] and homogenization of the skin temperatures, as already observed in preterm neonates [110]).
As a result, pre-sleep thermal manipulations capable of promoting distal vasodilation (a hot-water bottle [112], wearing a thermosuit [113], wearing socks [114], etc.) or nonthermal manipulations (lights off, lying down [115, 116], a spicy meal, physical exercise, cognitive and physical relaxation, etc.) were capable of (or might be capable of) increasing sleepiness, reducing sleep onset latency, and improving sleep maintenance [10, 117] in healthy men, older adults with insomnia [118], and adults with narcolepsy [119]. In particular, it has been proven that subtle skin warming—although perceived as slightly uncomfortable by the subject—reduces sleep onset latency [113]. Promoting pre-sleep relaxation and reducing anxiety when retiring for bed is also of value in decreasing sympathetic nervous system activity and, in turn, promoting skin vasodilation prior to sleep onset [120]. The same may hold for hypnotics (benzodiazepine [121] and temazepam: [122, 123]); the induced skin vasodilation might contribute to the drugs’ hypnotic effects. Likewise, melatonin secretion is the signal that induces selective vasodilation in the distal skin segments [93, 124].
In a Japanese study, Nakamura Ikada et al. [125] carefully analyzed the temperature and humidity values in the infant’s bed, as well as the infant’s skin temperatures. The researchers found differences according to the season and the environmental conditions (bedding, clothing, etc.). They recommended avoiding the use of waterproof sheets (especially during humid seasons), and bedding and coverings made for adults but that are not thermally appropriate for infants. Unfortunately, the study did not include an actigraphic analysis, and so the impact of these conditions on the infant’s sleep quality and quantity could not be assessed.
In a study that compared 4-year-old preschool children with their mothers, significant correlations were observed between sleep parameters and a proximal temperature (the chest) but not a distal temperature (the foot): the higher the proximal temperature, the lower the amount of wakefulness (the total duration and the episode duration) and the mean activity (measured using actigraphy) and the higher the sleep efficiency index. This was not observed in the mothers [109]. The major role of proximal temperature suggested by this study is not, however, in line with almost all the other studies performed in infants, whatever their age. It should be noted that in contrast to most studies in this field, Okamoto-Mizuno et al.’s study was performed in the absence of thermal constraints.
In babies aged 4–9 months, Abe and Kodama [91] suggested that interventions that decreased the DPG at lights off (e.g., a relatively low ambient temperature) could help to stabilize the DPG pattern from one night to another. It has also been found that increasing daytime exposure to light and maximizing the light-dark difference within a 24-hr period may promote circadian entrainment (and thus sleep) in 2- to 10-week-old babies [126]. In the same study, however, attempts to shorten the sleep onset latency (with lights off, and darkening the room during the night) did not exert a significant effect.
Lastly, the decrease in core temperature at sleep onset was found to be greater in babies not fed before sleep [106]. Therefore, lengthening the interval between the last feed and bedtime might shorten sleep latency.
To the best of our knowledge, and beyond the above-cited observational studies, the use of deliberate thermal manipulation within the circadian body temperature range (in order to improve sleep) has never been studied in neonates or older infants; this would be of great interest.
Conclusion
In contrast to adults, the neonate’s thermoregulatory system is fully operative during REM sleep in both cool and warm conditions—at least in the range of environmental temperatures usually studied. The maintenance of efficient thermoregulation in REM sleep protects the neonate from long periods of poikilothermy that would otherwise occur. This is of particular relevance, since REM sleep episodes can be long. Moreover, the thermoregulatory system not only helps to prevent REM sleep deprivation but also favors this sleep stage (i.e., preferential switching from NREM sleep to REM sleep, and a greater relative duration of REM sleep). As a result, REM sleep (of importance in neurodevelopment) appears to be a well-protected sleep stage.
The lack of data on thermoregulatory responses in older infants or adolescents prevents us from saying whether the transition from the neonatal thermoregulatory characteristics (greater efficiency, and a longer duration of REM sleep when exposed to a cool environment) to the adult thermoregulatory pattern (poor efficiency, and partial REM sleep deprivation in cool or warm environments) occurs at the same time as the transition to adult sleep characteristics and rhythms.
All the literature data indicate that distal skin vasodilation is part of “sleep preparedness” in infants (from preterm neonates to older children)—much as is observed in adults, and despite the many infant vs. adult differences in sleep structure, rhythm, neural maturation, thermoregulatory function, and thermoregulatory centers. It is important to note that distal skin vasodilation occurs even when most of the environmental and behavioral parameters that have been demonstrated to have a major role in the pre-sleep increase in vasodilation and sleepiness in adults (lying down, cognitive relaxation, body relaxation, reduced light intensity, etc.) cannot fully operate in babies and preterm neonates. This observation opens up interesting perspectives for further research, for example, whether it would be possible to improve sleep through thermal or nonthermal manipulations that induce distal skin vasodilation.
References
Parmeggiani PL, Rabini C. Sleep and environmental temperature. Arch Ital Biol. 1970;108:369–87.
Glotzbach SF, Heller HC. Central nervous regulation of body temperature during sleep. Science. 1976;194:537–9.
Parmeggiani PL. Thermoregulation during sleep from the view point of homeostasis. Clin Physiol Sleep Am Physiol Soc. 1988:159–69.
Haskell EH, Palca JW, Walker JM, Berger RJ, Heller HC. Metabolism and thermoregulation during stages of sleep in humans exposed to heat and cold. J Appl Physiol. 1981;51:948–54.
Libert JP, Candas V, Vogt JJ, Mairiaux PH. Central and peripheral inputs in sweating regulation during thermal transients. J Appl Physiol. 1982;52:1147–52.
Scopes JW, Ahmed I. Range of critical temperatures in sick and premature newborn infants. Arch Dis Child. 1966;41:417–9.
Satinoff E. Neural organization and evolution of thermal regulation in mammals. Science. 1978;201:16–22.
Azaz Y, Fleming PJ, Levine MR, McCabe R, Stewart A, Johnson P. The relationship between environmental temperature, metabolic rate, sleep state, and evaporative water loss in infants from birth to three months. Pediatr Res. 1992;32:417–23.
Libert JP, Tourneux P. The thermostatic control of body temperature. In: Singpost CKER, editor. Vegetatives functions and their interaction in the neonat. Kerala, India: Research Signpost; 2010. p. 45–75.
Van Someren EJW. More than a marker: interaction between the circadian regulation of temperature and sleep, age-related changes, and treatment possibilities. Chronobiol Int. 2000;17:313–54.
McGinty D, Szymusiak R. Brain structures and mechanisms involved in the generation of NREM sleep: focus on the preoptic hypothalamus. Sleep Med Rev. 2001;5:323–42.
Boulant JA, Hardy JD. The effect of spinal and skin temperatures on the firing rate and thermosensitivity of preoptic neurones. J Physiol. 1974;240:639–60.
Hammel HT, Jackson DC, Stolwijk JAJ, Hardy JD, Stromme SB. Temperature regulation by hypothalamic proportional control with an adjustable set-point. J Appl Physiol. 1963;18:1146–54.
Nadel ER, Bullard RW, Stolwijk JAJ. Importance of skin temperature in the regulation of sweating. J Appl Physiol. 1971;31:80–7.
Libert JP, Candas V, Vogt JJ. Effect of rate of change in skin temperature on local sweating rate. J Appl Physiol. 1979;47:306–11.
Libert JP, Bach V, Farges G. Neutral temperature range in incubators: performance of equipment in current use and new development. Crit Rev Biomed Eng. 1997;25:287–370.
Rein H, Schneider M. Physiology des Menschen: Auflage Springer; 1960. p. 13–4.
Elabbassi EB, Belghazi K, Delanaud S, Libert JP. Dry heat loss in incubator: comparison of two premature newborn sized manikins. Eur J Appl Physiol. 2004;92:679–82.
Stothers JK, Warner RM. Oxygen consumption and neonatal sleep states. J Physiol (London). 1978;278:435–40.
Stothers JK, Warner RM. Thermal balance and sleep state in the newborn. Early Hum Dev. 1984;9:313–22.
Dane HJ, Sauer PJ, Visser HK. Oxygen consumption and CO2 production of low-birth-weight infants in two sleep states. Biol Neonate. 1985;47:205–10.
Bach V, Bouferrache B, Kremp O, Maingourd Y, Libert JP. Regulation of sleep and body temperature in response to exposure to cool and warm environments in neonates. Pediatrics. 1994;93:789–96.
Butte NF, Jensen CL, Moon JK, Glaze DJ, Frost JD. Sleep organization and energy expenditure of breast-fed and formula-fed infants. Pediatr Res. 1992;32:514–9.
Darnall RA, Ariagno RL. The effect of sleep state on active thermoregulation in the premature infant. Pediatr Res. 1982;16:512–4.
Suichies HE, Aarnoudse JG, Okken A, Jentink HW, de Mul FF, Greve J. Forehead skin blood flow in normal neonates during active and quiet sleep, measured with a diode laser Doppler instrument. Acta Paediatr Scand. 1988;77:220–5.
Brown PJ, Dove RA, Tuffnell CS, Ford RP. Oscillations of body temperature at night. Arch Dis Child. 1992;67:1255–8.
Bach V, Telliez F, Leke A, Chiorri C, Libert JP. Interaction between body temperatures and the direction of sleep stage transition in neonates. Sleep Res Online. 2001;4:43–9.
Scher MS, Dokianakis SG, Sun M, Steppe DA, Guthrie RD, Sclabassi RJ. Rectal temperature changes during sleep state transitions in term and preterm neonates at postconceptional term ages. Pediatr Neurol. 1994;10:191–4.
Scher MS, Steppe DA, Salerno DG, Beggarly ME, Banks DL. Temperature differences during sleep between fullterm and preterm neonates at matched post-conceptional ages. Clin Neurophysiol. 2003;114:17–22.
Richard CA. Increased infant axillary temperatures in non-REM sleep during mother-infant bed-sharing. Early Hum Dev. 1999;55:103–11.
Ammari A, Schulze KF, Ohira-Kist K, Kashyap S, Fifer WP, Myers MM, et al. Effects of body position on thermal, cardiorespiratory and metabolic activity in low birth weight infants. Early Hum Dev. 2009;85:497–501.
Bolton DP, Herman S. Ventilation and sleep state in the newborn. J Physiol. 1974;240:67–77.
Trinder J, Kleiman J, Carrington M, Smith S, Breen S, Tan N, et al. Autonomic activity during human sleep as a function of time and sleep stage. J Sleep Res. 2001;10:253–64.
Rutter N, Hull D. Response of term babies to a warm environment. Arch Dis Child. 1979;54:178–83.
Lyon AJ, Freer Y. Goals and options in keeping preterm babies warm. Arch Dis Child Fetal Neonatal Ed. 2011;96:F71–4.
Lindqvist A, Oja R, Hellman O, VŠlimŠki I. Impact of thermal vasomotor control on the heart rate variability of newborn infants. Early Hum Dev. 1983;8:37–47.
Brück K. Temperature regulation in the newborn infant. Biol Neonat. 1961;3:65–119.
Lyon AJ, Pikaar ME, Badger P, McIntosh N. Temperature control in very low birthweight infants during first five days of life. Arch Dis Child Fetal Neonatal Ed. 1997;76:F47–50.
Kroth J, Weidlich K, Hiedl S, Nussbaum C, Christ F, Genzel-boroviczeny O. Functional vessel density in the first month of life in preterm neonates. Pediatr Res. 2008;64:567–71.
Knobel RB, Holditch-Davis D, Schwartz TA, Wimmer JE Jr. Extremely low birth weight preterm infants lack vasomotor response in relationship to cold body temperatures at birth. J Perinatol. 2009;29:814–21.
Midttun M. Blood flow rate in arteriovenous anastomoses: from the cradle to the grave. Clin Physiol. 2000;20:360–5.
Berg K, Celander O. Circulatory adaptation in the thermoregulation of fullterm and premature newborn infants. Acta Paediatr Scand. 1971;60:278–84.
Karlsson H, Olegard R, Nilsson K. Regional skin temperature, heat flow and conductance in preterm neonates nursed in low and in neutral environmental temperature. Acta Paediatr. 1996;85:81–7.
Wagner JA, Robinson S, Marino RP. Age and temperature regulation of humans in neutral and cold environments. J Appl Physiol. 1974;37:562–5.
Smolander J, Bar-Or O, Korhonen O, Ilmarinen J. Thermoregulation during rest and exercise in the cold in pre- and early pubescent boys and in young men. J Appl Physiol. 1992;72:1589–94.
Inoue Y, Nakamura S, Yonehiro K, Kuwahara T, Ueda H, Araki T. Regional differences in peripheral vasoconstriction of prepubertal boys. Eur J Appl Physiol. 2006;96:397–403.
Tsuzuki K, Tochihara Y, Ohnaka T. Comparison of thermal responses between young children (1- to 3-year-old) and mothers during cold exposure. Eur J Appl Physiol. 2008;103:697–705.
Clarke L, Darby CJ, Lomax MA, Symonds ME. Effect of ambient temperature during 1st day of life on thermoregulation in lambs delivered by cesarean section. J Appl Physiol. 1992;76:1481–8.
Kapas L, Szentirmai E. Brown adipose tissue at the intersection of sleep and temperature regulation. Temperature. 2014;1:16–7.
Adamsons KJ, Gandy GM, James LS. The influence of thermal factors upon oxygen consumption of the newborn human infant. J Pediatr. 1965;66:495–508.
Fleming PJ, Levine MR, Azaz Y, Johnson P. The effect of sleep state on the metabolic response to cold stress in newborn infants. In: Jones CT, editor. Fetal and neonatal development. Ithaca, New York: Perinatology Press; 1988. p. 635–9.
Stothers JK, Warner RM. Oxygen consumption of the newborn infant in a cool environment, measured with regard to sleep state. J Physiol (London). 1977;272:16–7.
Telliez F, Chardon K, Leke A, Cardot V, Tourneux P, Bach V. Thermal acclimation of neonates to prolonged cool exposure as regards sleep stages. J Sleep Res. 2004;13:337–43.
Kenney WL, Tankersley CG, Newswanger DL, Hyde DE, Puhl SM, Turner NL. Age and hypohydration independently influence the peripheral vascular response to heat stress. J Appl Physiol. 1990;68:1902–8.
Minson CT, Wladkowski SL, Cardell AF, Pawelczyk JA, Kenney WL. Age alters the cardiovascular response to direct passive heating. J Appl Physiol. 1998;84:1323–32.
Jokinen E, Valimaki I, Antila K, Seppanen A, Tuominen J. Children in sauna: cardiovascular adjustment. Pediatrics. 1990;86:282–8.
Harpin VA, Rutter N. Sweating in preterm babies. J Pediatr. 1982;100:614–9.
Harpin VA, Chellappah G, Rutter N. Responses of the newborn infant to overheating. Biol Neonate. 1983;44:65–75.
Foster KG, Hey EN, Katz G. The response of the sweat glands of the new-born baby to thermal stimuli and to intradermal acetylcholine. J Physiol (London). 1969;203:13–29.
Bar-Or O. Climate and the exercising child:a review. Int J Sports Med. 1980;1:53–65.
Drinkwater BL, Kupprat IC, Denton JE, Crist JL, Horvath SM. Response of prepubertal girls and college women to work in the heat. J Appl Physiol Respir Environ Exerc Physiol. 1977;43:1046–53.
Kenney WL, Fowler SR. Methylcholine-activated eccrine sweat gland density and output as a function of age. J Appl Physiol. 1988;65:1082–6.
Inoue Y, Ichinose-Kuwahara T, Nakamura S, Ueda H, Yasumatsu H, Kondo N, et al. Cutaneous vasodilation response to a linear increase in air temperature from 28 degrees C to 40 degrees C in prepubertal boys and young men. J Physiol Anthropol. 2009;28:137–44.
Sulyok E, Jéquier E, Prod'hom LS. Thermal balance of the newborn in a heat-gaining environment. Pediatr Res. 1973;7:888–900.
Okken A, Bligham G, Franz W, Bohn E. Effect of forced convection of heated air on sensible water loss and heat loss in premature infants in incubators. J Pediatr. 1982;101:108–12.
Hammarlund K, Sedin G, Stršmberg B. Transepidermal water loss in newborn infants. VII. Relation to post-natal age in very pre-term and full-term appropriate for gestational age infants. Acta Paediatr Scand. 1982;71:369–74.
Wu PYK, Hodgman JE. Insensible water loss in preterm infants: changes with postnatal development and non-ionizing radiant energy. Pediatrics. 1974;54:704–12.
Day R. Regulation of body temperature during sleep. Am J Dis Child. 1941;61:734–46.
Shibasaki M, Inoue Y, Kondo N. Mechanisms of underdeveloped sweating responses in prepubertal boys. Eur J Appl Physiol Occup Physiol. 1997;76:340–5.
Inoue Y, Kuwahara T, Araki T. Maturation- and aging-related changes in heat loss effector function. J Physiol Anthropol Appl Hum Sci. 2004;23:289–94.
Perlstein PH, Hersh C, Gyck CJ, Sutherland JM. Adaptation to cold in the first three days of life. Pediatrics. 1974;54:411–6.
Asakura H. Fetal and neonatal thermoregulation. J Nippon Med Sch = Nippon Ika Daigaku Zasshi. 2004;71:360–70.
Hey EN, O'Connell B. Oxygen consumption and heat balance in the cot-nursed baby. Arch Dis Child. 1970;45:335–43.
Wheldon AE. Energy balance in the newborn baby: use of a manikin to estimate radiant and convective heat loss. Phys Med Biol. 1982;27:285–96.
Candas V, Libert JP, Vogt JJ, Ehrhart J, Muzet A. Body temperatures during sleep under different thermal conditions. In: Fanger PO, Valbjorn O, editors. Indoor climate: effects on human comfort, performance, and health. Copenhagen: Danish building Research Institute; 1979. p. 763–78.
Muzet A, Ehrhart J, Candas V, Libert JP, Vogt JJ. REM sleep and ambient temperature in man. Int J Neurosci. 1983;18:117–26.
Karlsson H, Hamel SE, Nilsson K, Olagard R. Measurement of skin temperature and heat flow from skin in term newborn babies. Acta Paediatr. 1995;84:605–12.
Bach V, Telliez F, Leke A, Libert JP. Gender-related sleep differences in neonates in thermoneutral and cool environments. J Sleep Res. 2000;9:249–54.
Wailoo MP, Petersen SA, Whittaker H. Disturbed nights and 3-4 month old infants: the effects of feeding and thermal environment. Arch Dis Child. 1990;65:499–501.
Tourula M, Isola A, Hassi J, Bloigu R, Rintamaki H. Infants sleeping outdoors in a northern winter climate: skin temperature and duration of sleep. Acta Paediatr. 2010;99:1411–7.
Brück K, Parmelee AH, Brück M. Neutral temperature range and range of “thermal comfort” in premature infants. Biol Neonate. 1962;4:32–51.
Telliez F, Bach V, Krim G, Libert JP. Consequences of a small decrease of air temperature from thermal equilibrium on thermoregulation in sleeping neonates. Med Biol Eng Comput. 1997;35:516–20.
Telliez F, Bach V, Dewasmes G, Leke A, Libert JP. Sleep modifications during cool acclimation in human neonates. Neurosci Lett. 1998;245:25–8.
Bach V, Telliez F, Zoccoli G, Lenzi P, Leke A, Libert JP. Interindividual differences in the thermoregulatory response to cool exposure in sleeping neonates. Eur J Appl Physiol. 2000;81:455–62.
Orsi KC, Avena MJ, Lurdes de Cacia Pradella-Hallinan M, da Luz Goncalves Pedreira M, Tsunemi MH, Machado Avelar AF, et al. Effects of handling and environment on preterm newborns sleeping in incubators. J Obstet Gynecol Neonat Nurs. 2017;46:238–47.
Libert JP, Di Nisi J, Fukuda H, Muzet A, Ehrhart J, Amoros C. Effect of continuous heat exposure on sleep stages in humans. Sleep. 1988;11:195–209.
Franco P, Scaillet S, Valente F, Chabanski S, Groswasser J, Kahn A. Ambient temperature is associated with changes in infants' arousability from sleep. Sleep. 2001;24:325–9.
Okamoto-Mizuno K, Mizuno K, Tanabe M, Niwano K. Effects of the environment of a simulated shelter in a gymnasium on sleep in children. Int J Biometeorol. 2018;62:2015–23.
Tirosh E, Bader D, Hodgins H, Cohen A. Sleep architecture as related to temperature changes in neonates at term. Clin Physiol. 1996;16:603–8.
Van Den Heuvel CJ, Noone JT, Lushington K, Dawson D. Changes in sleepiness and body temperature precede nocturnal sleep onset: evidence from a polysomnographic study in young men. J Sleep Res. 1998;7:159–66.
Abe N, Kodama H. Distal-proximal skin temperature gradient prior to sleep onset in infants for clinical use. Pediatr Int. 2015;57:227–33.
Kräuchi K, Wirz-Justice A. Circadian clues to sleep onset mechanisms. Neuropsychopharmacology. 2001;25:S92–6.
Kräuchi K, Cajochen C, Werth E, Wirz-Justice A. Functional link between distal vasodilation and sleep-onset latency? Am J Physiol Regul Integr Comp Physiol. 2000;278:R741–8.
Okamoto Mizuno K, Yamashiro Y, Tanaka H, Komada Y, Mizuno K, Tamaki M, et al. Heart rate variability and body temperature during sleep onset. Sleep Biol Rhythms. 2008;6:42–9.
Bueno C, Menna-Barreto L. Development of sleep/wake, activity and temperature rhythms in newborns maintained in a neonatal intensive care unit and the impact of feeding schedules. Infant Behav Dev. 2016;44:21–8.
Mirmiran M, Maas YG, Ariagno RL. Development of fetal and neonatal sleep and circadian rhythms. Sleep Med Rev. 2003;7:321–34.
Zornoza-Moreno M, Fuentes-Hernandez S, Sanchez-Solis M, Rol MA, Larque E, Madrid JA. Assessment of circadian rhythms of both skin temperature and motor activity in infants during the first 6 months of life. Chronobiol Int. 2011;28:330–7.
Abe K, Sasaki H, Takebayashi K, Fukui S, Nambu H. The development of circadian rhythm of human body temperature. J Interdiscipl Cycle Res. 1978;9:211–6.
Petersen SA, Anderson ES, Lodemore M, Rawson D, Wailoo MP. Sleeping position and rectal temperature. Arch Dis Child. 1991;66:976–9.
Wailoo MP, Petersen SA, Whittaker H, Goodenoug H. Sleeping body temperatures in 3-4 month old infants. Arch Dis Child. 1989;64:596–9.
Tsogt B, Manaseki-Holland S, Pollock J, Blair PS, Fleming P. Thermoregulatory effects of swaddling in Mongolia: a randomised controlled study. Arch Dis Child. 2016;101:152–60.
Lodemore M, Petersen SA, Wailoo MP. Development of night time temperature rhythms over the first six months of life. Arch Dis Child. 1991;66:521–4.
Joseph D, Chong NW, Shanks ME, Rosato E, Taub NA, Petersen SA, et al. Getting rhythm: how do babies do it? Arch Dis Child Fetal Neonatal Ed. 2015;100:F50–4.
Bach V, Delanaud S, Barcat L, Bodin E, Tourneux P, Libert JP. Distal skin vasodilation in sleep preparedness, and its impact on thermal status in preterm neonates. Sleep Med. 2019;
Lodemore MR, Petersen SA, Wailoo MP. Factors affecting the development of night time temperature rhythms. Arch Dis Child. 1992;67:1259–61.
Anderson ES, Petersen SA, Wailoo MP. Factors influencing the body temperature of 3-4 month old infants at home during the day. Arch Dis Child. 1990;65:1308–10.
Murphy PJ, Frei MG, Papolos D. Alterations in skin temperature and sleep in the fear of harm phenotype of pediatric bipolar disorder. J Clin Med. 2014;3:959–71.
McCabe SM, Elliott C, Langdon K, Abbiss CR. Patterns and reliability of children's skin temperature prior to and during sleep in the home setting. Physiol Behav. 2018;194:292–301.
Okamoto-Mizuno K, Mizuno K, Shirakawa S. Sleep and skin temperature in preschool children and their mothers. Behav Sleep Med. 2016;16:64–78.
Barcat L, Decima P, Bodin E, Delanaud S, Stephan-Blanchard E, Leke A, et al. Distal skin vasodilation promotes rapid sleep onset in preterm neonates. J Sleep Res. 2017;26:572–7.
Kräuchi K, Deboer T. The interrelationship between sleep regulation and thermoregulation. Front Biosci. 2010;15:604–25.
Kräuchi K, Cajochen C, Werth E, Wirz-Justice A. Warm feet promote the rapid onset of sleep. Nature. 1999;401:36–7.
Raymann RJ, Swaab DF, Van Someren EJ. Cutaneous warming promotes sleep onset. Am J Physiol Regul Integr Comp Physiol. 2005;288:R1589–97.
Ko Y, Lee JY. Effects of feet warming using bed socks on sleep quality and thermoregulatory responses in a cool environment. J Physiol Anthropol. 2018;37:13.
Tikuisis P, Ducharme MB. The effect of postural changes on body temperatures and heat balance. Eur J Appl Physiol Occup Physiol. 1996;72:451–9.
Kräuchi K, Cajochen C, Wirz-Justice A. A relationship between heat loss and sleepiness: effects of postural change and melatonin administration. J Appl Physiol. 1997;83:134–9.
Liao WC. Effects of passive body heating on body temperature and sleep regulation in the elderly: a systematic review. Int J Nurs Stud. 2002;39:803–10.
Van Someren EJ, Raymann RJ, Scherder EJ, Daanen HA, Swaab DF. Circadian and age-related modulation of thermoreception and temperature regulation: mechanisms and functional implications. Ageing Res Rev. 2002;1:721–78.
Fronczek R, Raymann RJ, Overeem S, Romeijn N, van Dijk JG, Lammers GJ, et al. Manipulation of skin temperature improves nocturnal sleep in narcolepsy. J Neurol Neurosurg Psychiatry. 2008;79:1354–7.
Lack L, Gradisar M. Acute finger temperature changes preceding sleep onsets over a 45-h period. J Sleep Res. 2002;11:275–82.
Echizenya M, Mishima K, Satoh K, Kusanagi H, Sekine A, Ohkubo T, et al. Heat loss, sleepiness, and impaired performance after diazepam administration in humans. Neuropsychopharmacology. 2003;28:1198–206.
Gilbert SS, Burgess HJ, Kennaway DJ, Dawson D. Attenuation of sleep propensity, core hypothermia, and peripheral heat loss after temazepam tolerance. Am J Physiol Regul Integr Comp Physiol. 2000;279:R1980–7.
Libert JP, Weber LD, Amoros C, Muzet A, Ehrhart J, Follenius M. Influence of triazolam on thermal heat balnce in poor sleepers. Eur J Clin Pharmacol. 1984;27:173–9.
Kräuchi K, Cajochen C, Mori D, Graw P, Wirz-Justice A. Early evening melatonin and S-20098 advance circadian phase and nocturnal regulation of core body temperature. Am J Phys. 1997;272:R1178–88.
Nakamura Ikeda R, Fukai K, Okamoto MK. Infant's bed climate and bedding in the Japanese home. Midwifery. 2012;28:340–7.
Tsai SY, Thomas KA, Lentz MJ, Barnard KE. Light is beneficial for infant circadian entrainment: an actigraphic study. J Adv Nurs. 2012;68:1738–47.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Bach, V., Libert, JP. (2021). Thermoregulation and Metabolism. In: Gozal, D., Kheirandish-Gozal, L. (eds) Pediatric Sleep Medicine. Springer, Cham. https://doi.org/10.1007/978-3-030-65574-7_6
Download citation
DOI: https://doi.org/10.1007/978-3-030-65574-7_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-65573-0
Online ISBN: 978-3-030-65574-7
eBook Packages: MedicineMedicine (R0)